
Chemsex and Psychosis: A Systematic Review

Abstract
1. Introduction
Aims
2. Materials and Methods
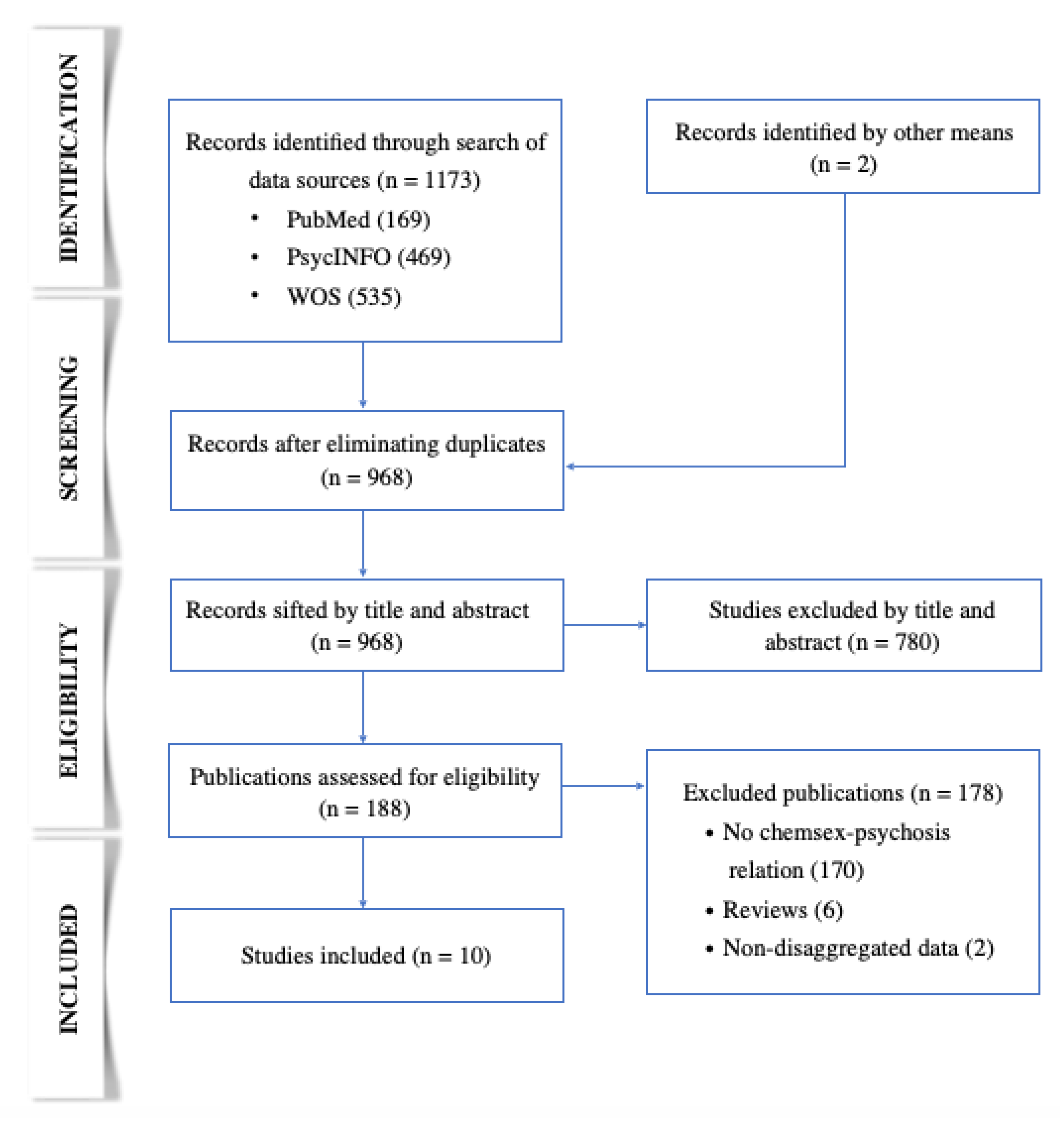
2.1. Information Sources and Search Strategy

{kind=link}
{kind=link}
| Population | Risk Factor | Result |
|---|---|---|
| MSM, trans | Chemsex | Psychosis |
2.2. Study Selection Process

2.3. Eligibility Criteria
2.4. Data Extraction Process
2.5. Risk of Bias Assessment of Individual Studies
2.6. Synthesis Methods
| Author and Year of Publication | Type of Study | Country | Population | Drugs |
|---|---|---|---|---|
| Bourne et al. (2015) [29] | Qualitative | United Kingdom | MSM N = 30 Mean age = 36 years | Mephedrone 90% (66.7% with GHB/GBL) and methamphetamine 33% (normally with GHB/GBL) |
| Dolengevich et al. (2016) [30] | Case Report | Spain | MSM aged 25 | Mephedrone |
| Gavín et al. (2021) [31] | Retrospective longitudinal descriptive | Spain | MSM from an addiction unit N = 53 Mean age = 37.7 years | As main drug: methamphetamine 81.1%, GHB 9.4%, cocaine 3.8%, mephedrone 1.9%, speed 1.9%, and ketamine 1.9% Other substances: alcohol, cannabis, Viagra, poppers, and benzodiazepines |
| Dolengevich et al. (2020) [32] | Cross-sectional descriptive | Spain | MSM N = 138 Mean age = 37.46 years | From the 62 referred to psychiatry: mephedrone 64.3%, poppers 54.8%, GHB 48.3%, erectile dysfunction drugs 35.4%, methamphetamine 32.2%, cocaine 19.3%, and ketamine 4.8% |
| Ballesteros et al. (2017) [33] | Cross-sectional descriptive | Spain | MSM with mephedrone use disorder N = 15 Median age = 40 years | Mephedrone 100%, cocaine 66.7%, GHB 66.7%, methamphetamine 60%, ketamine 23%, and other substances (including drugs for erectile dysfunction) 25% |
| Batisse et al. (2016) [34] | Cross-sectional | France | MSM N = 51 Mean age = 40 years | Slamsex: mephedrone 51%, cocaine 3.9% and MDMA 2%. Non-slamsex: cocaine 33%, GHB/GBL 13%, poppers 11%, cannabis 11%, methamphetamine 8%, ketamine 8%, MDMA 6%, benzodiazepines 6%, LSD 2%, ethyl chloride 2%, and drugs for erectile dysfunction |
| Schreck et al. (2020) [35] | Cross-sectional | France | MSM who practiced slamsex N = 34 Median age = 38 years | Cathinones 100%, GBL 32.4%, poppers 14.8%, GHB 14.7%, cocaine 11.8%, cannabis 8.8%, methamphetamine 5.9%, MDMA 2.9%, ketamine 2.9%, and alcohol 2.9% |
| Bohn et al. (2020) [36] | Cross-sectional | Germany | MSM and trans (N = 3) N = 280 Mean age = 40.22 years | Poppers 87.9%, erectile dysfunction drugs 76.1%, GHB/GBL 73.6%, alcohol 72.1%, MDMA 59.6%, amphetamines 57.5%, ketamine 55.7%, methamphetamine 46.4%, cannabis 53.2%, cocaine 43.6%, mephedrone 35%, opioid analgesics 5.4%, and heroin 1.1% |
| Hibbert et al. (2021) [37] | Qualitative | United Kingdom | MSM N = 13 Median age = 34 years | Mephedrone 38%, poppers 38%, methamphetamine 31%, GHB/GBL 31%, cocaine 23%, and LSD 8% |
| Dolengevich et al. (2019) [38] | Cross-sectional descriptive | Spain | HIV+ MSM N = 216 Median age = 38 years | Cocaine 79.1%, poppers 78.7%, GHB 71.7%, cathinones 69.4%, MDMA 48.6%, ketamine 36.1%, and methamphetamine 29.6% |
3. Results
3.1. Sociodemographic Profile
| Study | Foreign/Ethnic Minority Status | Under Employment | Salary >1000 €/month | Higher Education | Stable Relationship * |
|---|---|---|---|---|---|
| Bourne et al. (2015) [29] | 46.7% | - | - | - | - |
| Gavín et al. (2021) [31] | 69.8% | - | - | - | - |
| Dolengevich et al. (2020) [30] | - | - | - | - | - |
| Ballesteros et al. (2016) [33] | - | 73.0% | - | 60.0% | - |
| Batisse et al. (2016) [34] | - | 85.0% | - | - | - |
| Schreck et al. (2020) [35] | - | 62.0% | - | - | 62.0% |
| Bohn et al. (2020) [36] | 17.6% | 77.8% | 87.2% | 77.7% | 57.4% |
| Hibbert et al. (2021) [37] | 23.0% | 77.0% | - | - | 46.0% |
| Dolengevich et al. (2019) [38] | 28.7% | - | 70.0% | 63.9% | 42.0% |
3.2. Psychotic Symptomatology and Disorders
| Study | Psychiatric Pathology | Psychosis | Substance Abuse/ Dependence | Anxiety | Depression | Suicidal Ideation | Suicide Attempt | ADHD |
|---|---|---|---|---|---|---|---|---|
| Bourne et al. (2015) [29] | 16.7% a | - | - | - | - | - | - | - |
| Gavín et al. (2021) [31] | 72.1% b | 37.2% * | 100.0% d | 4.7% * | 20.9% * | - | - | - |
| Dolengevich et al. (2020) [32] | 46.3% | 10.1% | 46.3% | 3.5% | 13.7% | - | - | 3.1% |
| Ballesteros et al. (2016) [33] | 60.0% b | 6.7% | 100.0%d | 6.7% | 13.3% | - | 13.3% | 5.7% |
| Batisse et al. (2016) [34] | 50.0% c | 31.4% * | 31.4% | - | - | - | - | - |
| Schreck et al. (2020) [35] | 26.0% | - | 88.2% | 8.8% * | - | 2.9% | - | - |
| Bohn et al. (2020) [36] | - | 13.2% * | - | 8.3% | 11.9% | 12.7% | 9.6% | - |
| Hibbert et al. (2021) [37] | - | 7.7% * | - | - | - | - | - | - |
| Dolengevich et al. (2019) [38] | - | 15.3% * | 19.0% | 26.9% | 33.3% | 15.3% | 13.8% | - |
3.3. Trauma
3.4. Psychological and Social Motivations
3.5. Drugs
| Study | Slamsex | Polydrug Use |
|---|---|---|
| Bourne et al. (2015) [29] | 33.3% | - |
| Gavín et al. (2021) [31] | - | 73.6% |
| Dolengevich et al. (2020) [32] | 40.0% | - |
| Ballesteros et al. (2016) [33] | 53.3% | 100.0% |
| Batisse et al. (2016) [34] | 60.8% | 62.0% |
| Schreck et al. (2020) [35] | - | 85.0% |
| Bohn et al. (2020) [36] | 30.0% | - |
| Dolengevich et al. (2019) [38] | 15.7% | 45.4% |
3.6. STIs and Infections Due to Intravenous Drug Use
3.7. Sexual Abuse
3.8. Professional and Personal Impact
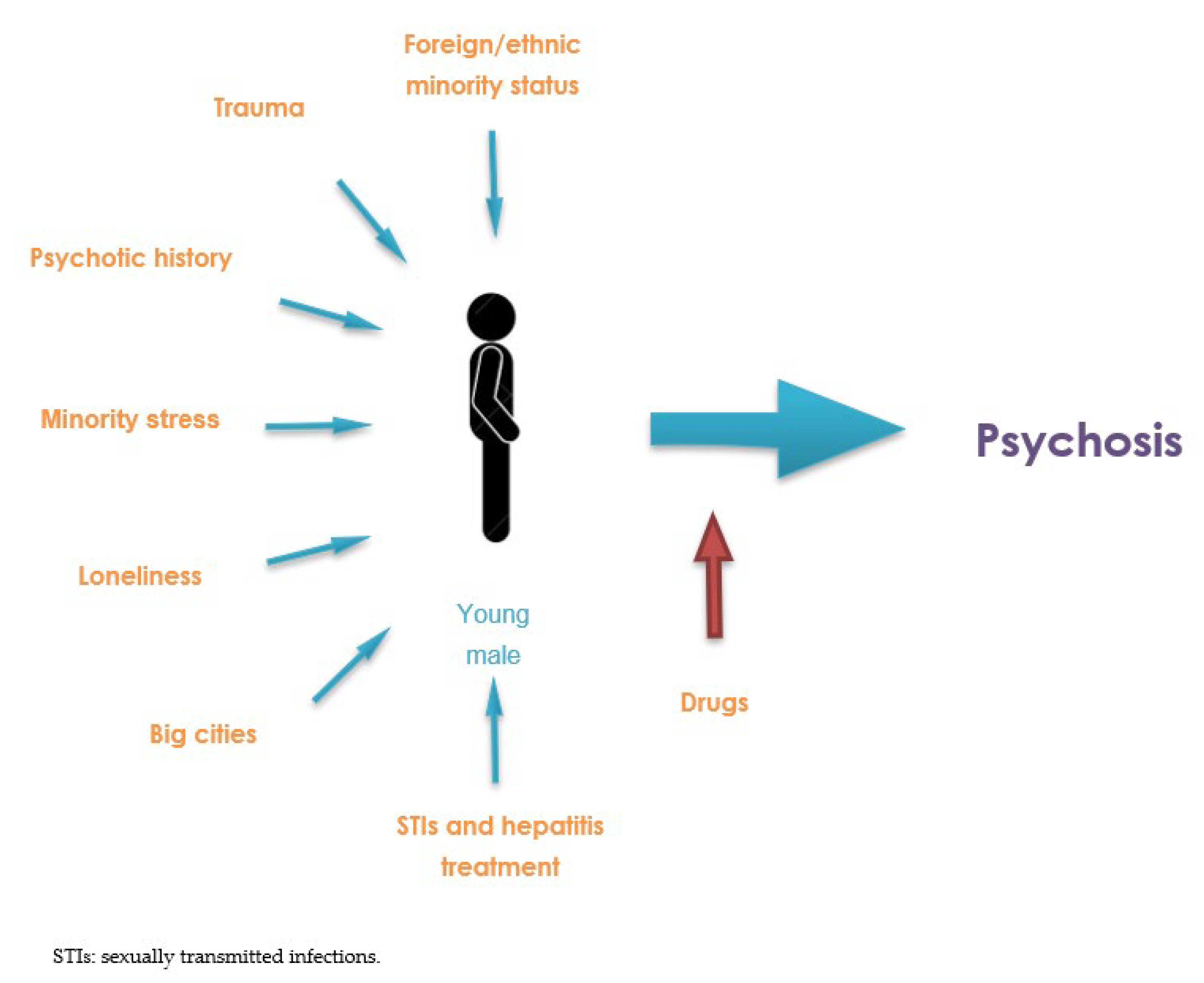
4. Discussion
- -
- Bohn et al. (2020) [36] identified that 33.6% of those who used chemsex had missed work or had worked while still under the influence of drugs.
- -
- Schreck et al. (2020) [35] described that 55% of men had social problems, with 44% experiencing separation and 24% missing work.
- -
- In the study by Dolengevich et al. (2019) [38], up to 31.5% of men reported interference with work, social, or family life, with a greater impact on the slamsex group (64.7%) compared to the chemsex group without slamsex (25.3%).

4.1. Limitations and Strengths
4.2. Future Lines of Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- PubMed:
- PsycINFO:
- WOS:
- #8 AND #34 AND #45
- 8: #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7
- 1: TS = (Homosexual*)
- 2: TS = (Gay$)
- 3: TS = (“Men who have sex with men”)
- 4: TS = (MSM)
- 5: TS = (Bisexual*)
- 6: TS = (Trans$exual*)
- 7: TS = (Transgender*)
- 34: #27 OR #33
- 27: #13 AND #26
- 13: #9 OR #10 OR #11 OR #12
- 9:TS = (“Sexual behavio*”)
- 10: TS = (“Sexual health”)
- 11: TS = (“Sexual risk”)
- 12: TS = (“Unsafe sex”)
- 26: #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 OR #24 OR #25
- 14: TS = (“Illicit drug*”)
- 15: TS = (*amphetamine)
- 16: TS = (MDMA)
- 17: TS = (Ecstasy)
- 18: TS = (Mephedrone)
- 19: TS = (GHB)
- 20: TS = (GBL)
- 21: TS = (Ketamine)
- 22: TS = (Cocaine)
- 23: TS = (Poppers)24: TS = (Viagra)
- 25: TS = (Cannabis)
- 33: #28 OR #29 OR #30 OR #31 OR #32
- 28: TS = (Chemsex)
- 29: TS = (Slamsex)
- 30: TS = (“Sexuali?ed drug*”)
- 31: TS = (“Party and play”)
- 32: TS = (“Intensive sex partying”)
- 45: #35 OR #36 OR #37 OR #38 OR #39 OR #40 OR #41 OR #42 OR #43 OR #44
- 35: TS = (“Mental health”)
- 36: TS = (“Mental disorder*”)
- 37: TS = (Psychosis)
- 38: TS = (Psychotic)
- 39: TS = (Schizo*)
- 40: TS = (Paranoi*)
- 41: TS = (Delusion*)
- 42: TS = (Hallucination*)
- 43: TS = (“Negative symptom*”)
- 44: TS = (Catatoni*)
References
- Chemsex Forum Organisation Comittee. 3rd European Chemsex Forum Paris. 2019. Available online: https://idpc.net/publications/2020/04/european-chemsex-forum-report (accessed on 3 September 2022).
- Bolmont, M.; Tshikung, O.N.; Trellu, L.T. Chemsex, a Contemporary Challenge for Public Health. J. Sex Med. 2022, 19, 1210–1213. [Google Scholar] [CrossRef] [PubMed]
- McCall, H.; Adams, N.; Mason, D.; Willis, J. What is chemsex and why does it matter? BMJ 2015, 35, h5790. [Google Scholar] [CrossRef] [PubMed]
- Dolengevich-Segal, H.; Rodríguez-Salgado, B.; Bellesteros-López, J.; Molina-Prado, R. Chemsex. Un fenómeno emergente. Adicciones 2017, 29, 207–209. [Google Scholar] [CrossRef]
- Drevin, G.; Rossi, L.H.; Férec, S.; Briet, M.; Abbara, C. Chemsex/slamsex-related intoxications: A case report involving gamma-hydroxybutyrate (GHB) and 3-methylmethcathinone (3-MMC) and a review of the literature. Forensic Sci. Int. 2021, 321, 110743. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Mo, P.K.H.; Ip, M.; Fang, Y.; Lau, J.T.F. Uptake and willingness to use PrEP among Chinese gay, bisexual and other men who have sex with men with experience of sexualized drug use in the past year. BMC Infect. Dis. 2020, 20, 299. [Google Scholar] [CrossRef]
- Guerras, J.M.; Hoyos, J.; Donat, M.; de la Fuente, L.; Palma Díaz, D.; Ayerdi, O.; García-Pérez, J.N.; García de Olalla, P.; Belza, M.J. Sexualized drug use among men who have sex with men in Madrid and Barcelona: The gateway to new drug use? Front. Public Health 2022, 10, 997730. [Google Scholar] [CrossRef] [PubMed]
- Stuart, D. A chemsex crucible: The context and the controversy. J. Fam. Plann. Reprod. Health Care 2016, 42, 295–296. [Google Scholar] [CrossRef]
- Weatherburn, P.; Hickson, F.; Reid, D.; Torres-Rueda, S.; Bourne, A. Motivations and values associated with combining sex and illicit drugs (‘chemsex’) among gay men in South London: Findings from a qualitative study. Sex Transm. Infect 2017, 93, 203–206. [Google Scholar] [CrossRef]
- Tomkins, A.; George, R.; Kliner, M. Sexualised drug taking among men who have sex with men: A systematic review. Perspect. Public Health 2019, 139, 23–33. [Google Scholar] [CrossRef]
- Íncera-Fernández, D.; Gámez-Guadix, M.; Moreno-Guillén, S. Mental Health Symptoms Associated with Sexualized Drug Use (Chemsex) among Men Who Have Sex with Men: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 13299. [Google Scholar] [CrossRef]
- Ramachandran, P.S.; Baird, R.W.; Markey, P.; Singleton, S.; Lowe, M.; Currie, B.J.; Burrow, J.N.; Price, R.N. Neurosyphilis: Still prevalent and overlooked in an at risk population. PLoS ONE 2020, 15, e0238617. [Google Scholar] [CrossRef]
- Pakianathan, M.; Whittaker, W.; Lee, M.J.; Avery, J.; Green, S.; Nathan, B.; Hegazi, A. Chemsex and new HIV diagnosis in gay, bisexual and other men who have sex with men attending sexual health clinics. HIV Med. 2018, 19, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Lafortune, D.; Blais, M.; Miller, G.; Dion, L.; Lalonde, F.; Dargis, L. Psychological and Interpersonal Factors Associated with Sexualized Drug Use Among Men Who Have Sex with Men: A Mixed-Methods Systematic Review. Arch. Sex Behav. 2021, 50, 427–460. [Google Scholar] [CrossRef] [PubMed]
- Mittal, V.A.; Walker, E.F. Advances in the neurobiology of stress and psychosis. Schizophr. Res. 2019, 213, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Heriot-Maitland, C.; Wykes, T.; Peters, E. Trauma and Social Pathways to Psychosis, and Where the Two Paths Meet. Front. Psychiatry 2022, 12, 804971. [Google Scholar] [CrossRef]
- Tan, R.K.J.; Phua, K.; Tan, A.; Gan, D.C.J.; Ho, L.P.P.; Ong, E.J.; See, M.Y. Exploring the role of trauma in underpinning sexualised drug use (‘chemsex’) among gay, bisexual and other men who have sex with men in Singapore. Int. J. Drug Policy 2021, 97, 103333. [Google Scholar] [CrossRef]
- Wilkerson, J.M.; Di Paola, A.; Nieto, D.; Schick, V.; Latini, D.M.; Braun-Harvey, D.; Zoschke, I.N.; McCurdy, S. Sexual Violence and Chemsex among Substance-Using Sexual and Gender Minorities in Texas. Subst. Use Misuse 2021, 56, 2141–2150. [Google Scholar] [CrossRef]
- Yates, K.; Lång, U.; Peters, E.M.; Wigman, J.T.; McNicholas, F.; Cannon, M.; DeVylder, J.; Oh, H.; Kelleher, I. Sexual assault and psychosis in two large general population samples: Is childhood and adolescence a developmental window of sensitivity? Schizophr. Res. 2022, 241, 78–82. [Google Scholar] [CrossRef]
- Chau, A.K.C.; Zhu, C.; So, S.H.W. Loneliness and the psychosis continuum: A meta-analysis on positive psychotic experiences and a meta-analysis on negative psychotic experiences. Int. Rev. Psychiatry 2019, 31, 471–490. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. Declaración PRISMA 2020: Una guía actualizada para la publicación de revisiones sistemáticas. Rev. Esp. Cardiol. 2021, 74, 790–799. Available online: https://www.revespcardiol.org/es-declaracion-prisma-2020-una-guia-articulo-S0300893221002748 (accessed on 3 September 2022). [CrossRef]
- Vassar, M.; Yerokhin, V.; Sinnett, P.M.; Weiher, M.; Muckelrath, H.; Carr, B.; Varney, L.; Cook, G. Database selection in systematic reviews: An insight through clinical neurology. Health Info. Libr. J. 2017, 34, 156–164. [Google Scholar] [CrossRef]
- Da Costa Santos, C.M.; de Mattos Pimenta, C.A.; Nobre, M.R.C. The PICO strategy for the research question construction and evidence search. Rev. Lat. Am. Enfermagem. 2007, 15, 508–511. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Pub.: Washington DC, USA, 2013. [Google Scholar] [CrossRef]
- Critical Skills Appraisal Programme. CASP Checklists. Available online: https://casp-uk.net/ (accessed on 3 September 2022).
- Long, H.; French, D.; Brooks, J. Optimising the value of the critical appraisal skills programme (CASP) tool for quality appraisal in qualitative evidence synthesis. Methods Med. Health Serv. 2020, 1, 31–42. [Google Scholar] [CrossRef]
- Hannes, K.; Bennett, S. Evidence-Based Practice across the Health Professions, 3rd ed.; Elsevier: Chatswood, NSW, Australia, 2017; pp. 226–247. [Google Scholar]
- Popay, J.; Roberts, H.; Sowden, A.; Petticrew, M.; Arai, L.; Rodgers, M.; Brittenl, N.; Roen, K.; Duffy, S. Guidance on the conduct of narrative synthesis in systematic reviews. Prod. ESRC Methods Programme Version 2006, 15, 47–71. [Google Scholar] [CrossRef]
- Bourne, A.; Reid, D.; Hickson, F.; Torres-Rueda, S.; Steinberg, P.; Weatherburn, P. “Chemsex” and harm reduction need among gay men in South London. Int. J. Drug Policy 2015, 26, 1171–1176. [Google Scholar] [CrossRef]
- Dolengevich-Segal, H.; Rodríguez-Salgado, B.; Gómez-Arnau, J.; Sánchez-Mateos, D. Severe Psychosis, Drug Dependence, and Hepatitis C Related to Slamming Mephedrone. Case Rep. Psychiatry 2016, e8379562. [Google Scholar] [CrossRef]
- Gavin, P.; Arbelo, N.; Monras, M.; Nuno, L.; Bruguera, P.; De la Mora, L.; Martínez-Rebollar, M.; Miquel, L.; Blanch, J.; Miquel, L. Methamphetamine use in chemsex and its consequences on mental health: A descriptive study. Rev. Esp. Salud Publica 2021, 95, e202108108. [Google Scholar]
- Dolengevich, H.; Curto Ramos, J.; Ibarguchi, L.; Barrio Fernandez, P.; Garcia, A.; Gonzalez Baeza, A. Chemsex, psychopathology and multidisciplinary intervention in Madrid. «sex, drugs and you» program. NGO apoyo positivo. Eur. Psychiat. 2020, 63, S47–S48. Available online: https://hdl.handle.net/20.500.12530/55992 (accessed on 3 September 2022).
- Ballesteros-López, J.; Molina, R.; Rodriguez Salgado, B.; Martin-Herrero, J.; Dolengevich-Segal, H. Mephedrone and chemsex. A descriptive analysis of a sample of patients in Madrid. Rev. Esp. De Drogodependencias 2017, 41, 47–61. [Google Scholar]
- Batisse, A.; Peyriere, H.; Eiden, C.; Courne, M.A.; Djezzar, S. Use of psychostimulants in a sexual context: Analysis of cases reported to the French network of Addictovigilance Centers. Therapie 2016, 71, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Schreck, B.; Guerlais, M.; Laforgue, E.; Bichon, C.; Grall-Bronnec, M.; Victorri-Vigneau, C. Cathinone Use Disorder in the Context of Slam Practice: New Pharmacological and Clinical Challenges. Front. Psychiatry 2020, 11, 705. [Google Scholar] [CrossRef] [PubMed]
- Bohn, A.; Sander, D.; Köhler, T.; Hees, N.; Oswald, F.; Scherbaum, N.; Deimel, D.; Schecke, H. Chemsex and Mental Health of Men Who Have Sex with Men in Germany. Front. Psychiatry 2020, 11, 542301. [Google Scholar] [CrossRef] [PubMed]
- Hibbert, M.P.; Germain, J.S.; Brett, C.E.; Van Hout, M.C.; Hope, V.D.; Porcellato, L.A. Service provision and barriers to care for men who have sex with men engaging in chemsex and sexualised drug use in England. Int. J. Drug Policy 2021, 92, 103090. [Google Scholar] [CrossRef] [PubMed]
- Dolengevich-Segal, H.; Gonzalez-Baeza, A.; Valencia, J.; Valencia-Ortega, E.; Cabello, A.; Tellez-Molina, M.J.; Perez-Elias, M.J.; Serrano, R.; Perez-Latorre, L.; Martin-Carbonero, L.; et al. Drug-related and psychopathological symptoms in HIV-positive men who have sex with men who inject drugs during sex (slamsex): Data from the U-SEX GESIDA 9416 Study. PLoS ONE 2019, 14, e0220272. [Google Scholar] [CrossRef]
- Van Os, J.; Linscott, R.J.; Myin-Germeys, I.; Delespaul, P.; Krabbendam, L. A systematic review and meta-analysis of the psychosis continuum: Evidence for a psychosis proneness-persistence-impairment model of psychotic disorder. Psychol. Med. 2009, 39, 179–195. [Google Scholar] [CrossRef]
- Fiorentini, A.; Cantù, F.; Crisanti, C.; Cereda, G.; Oldani, L.; Brambilla, P. Substance-Induced Psychoses: An Updated Literature Review. Front. Psychiatry 2021, 12, 694863. [Google Scholar] [CrossRef]
- Jongsma, H.E.; Gayer-Anderson, C.; Lasalvia, A.; Quattrone, D.; Mulè, A.; Szöke, A.; Selten, J.-P.; Turner, C.; Arango, C.; Tarricone, I.; et al. Treated Incidence of Psychotic Disorders in the Multinational EU-GEI Study. JAMA Psychiatry 2018, 75, 36–46. [Google Scholar] [CrossRef]
- Radua, J.; Ramella-Cravaro, V.; Ioannidis, J.P.; Reichenberg, A.; Phiphopthatsanee, N.; Amir, T.; Thoo, H.Y.; Oliver, D.; Davies, C.; Morgan, C.; et al. What causes psychosis? An umbrella review of risk and protective factors. World Psychiatry 2018, 17, 49–66. [Google Scholar] [CrossRef]
- Stilo, S.A.; Murray, R.M. Non-Genetic Factors in Schizophrenia. Curr. Psychiatry Rep. 2019, 21, 100. [Google Scholar] [CrossRef]
- Kennedy, R.; Murira, J.; Foster, K.; Heinsbroek, E.; Keane, F.; Pal, N.; Chalmers, L.; Sinka, K. Sexualized drug use and specialist service experience among MSM attending urban and rural sexual health clinics in England and Scotland. Int. J. STD AIDS 2021, 32, 1338–1346. [Google Scholar] [CrossRef]
- González-Baeza, A.; Barrio-Fernández, P.; Curto-Ramos, J.; Ibarguchi, L.; Dolengevich-Segal, H.; Cano-Smith, J.; Rúa-Cebrián, G.; García-Carrillo de Albornoz, A.; Kessel, D. Understanding Attachment, Emotional Regulation, and Childhood Adversity and Their Link to Chemsex. Subst. Use Misuse 2022, 24, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Jaspal, R. Chemsex, Identity and Sexual Health among Gay and Bisexual Men. Int. J. Environ. Res. Public Health 2022, 19, 12124. [Google Scholar] [CrossRef] [PubMed]
- Meyer, I.H. Prejudice, Social Stress, and Mental Health in Lesbian, Gay, and Bisexual Populations: Conceptual Issues and Research Evidence. Psychol. Bull. 2003, 129, 674–697. [Google Scholar] [CrossRef] [PubMed]
- Sattler, F.A.; Wagner, U.; Christiansen, H. Effects of Minority Stress, Group-Level Coping, and Social Support on Mental Health of German Gay Men. PLoS ONE 2016, 11, e0150562. [Google Scholar] [CrossRef] [PubMed]
- Gevonden, M.J.; Selten, J.P.; Myin-Germeys, I.; De Graaf, R.; Have, M.T.; Van Dorsselaer, S.; Van Os, J.; Veling, W. Sexual minority status and psychotic symptoms: Findings from the Netherlands Mental Health Survey and Incidence Studies (NEMESIS). Psychol. Med. 2014, 44, 421–433. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017; Available online: https://apps.who.int/iris/handle/10665/254610 (accessed on 3 September 2022).
- Andreu-Bernabeu, Á.; Díaz-Caneja, C.M.; Costas, J.; De Hoyos, L.; Stella, C.; Gurriarán, X.; Alloza, C.; Fañanás, L.; Bobes, J.; González-Pinto, A.; et al. Polygenic contribution to the relationship of loneliness and social isolation with schizophrenia. Nat. Commun. 2022, 13, 51. [Google Scholar] [CrossRef]
- Sánchez-Fernández, M.D.; Tomateo-Torvisco, D. Síndromes psiquiátricos en personas infectadas con el Virus de la Inmunodeficiencia Humana: Una revisión breve. Rev. De Neuro-Psiquiatr. 2014, 77, 70–77. [Google Scholar] [CrossRef]
- Román Avezuela, N.; Esteve Díaz, N.; Martín, M.d.V.; Domarco Manrique, L.; Domínguez Longás, A.; García Cabeza, I. Tratamiento de hepatitis C y psicosis: A propósito de dos casos clínicos. Rev. De La Asoc. Española De Neuropsiquiatría 2014, 34, 135–141. [Google Scholar] [CrossRef][Green Version]
- Jalil, E.M.; Torres, T.S.; Pereira, C.C.d.A.; Farias, A.; Brito, J.D.U.; Lacerda, M.; da Silva, D.A.R.; Wallys, N.; Ribeiro, G.; Gomes, J.; et al. High Rates of Sexualized Drug Use or Chemsex among Brazilian Transgender Women and Young Sexual and Gender Minorities. Int. J. Environ. Res. Public Health 2022, 19, 1704. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moreno-Gámez, L.; Hernández-Huerta, D.; Lahera, G. Chemsex and Psychosis: A Systematic Review. Behav. Sci. 2022, 12, 516. https://doi.org/10.3390/bs12120516
Moreno-Gámez L, Hernández-Huerta D, Lahera G. Chemsex and Psychosis: A Systematic Review. Behavioral Sciences. 2022; 12(12):516. https://doi.org/10.3390/bs12120516
Chicago/Turabian StyleMoreno-Gámez, Lucía, Daniel Hernández-Huerta, and Guillermo Lahera. 2022. "Chemsex and Psychosis: A Systematic Review" Behavioral Sciences 12, no. 12: 516. https://doi.org/10.3390/bs12120516
APA StyleMoreno-Gámez, L., Hernández-Huerta, D., & Lahera, G. (2022). Chemsex and Psychosis: A Systematic Review. Behavioral Sciences, 12(12), 516. https://doi.org/10.3390/bs12120516