
Social and Mental Health Impact of Nuclear Disaster in Survivors: A Narrative Review



Abstract
:1. Introduction
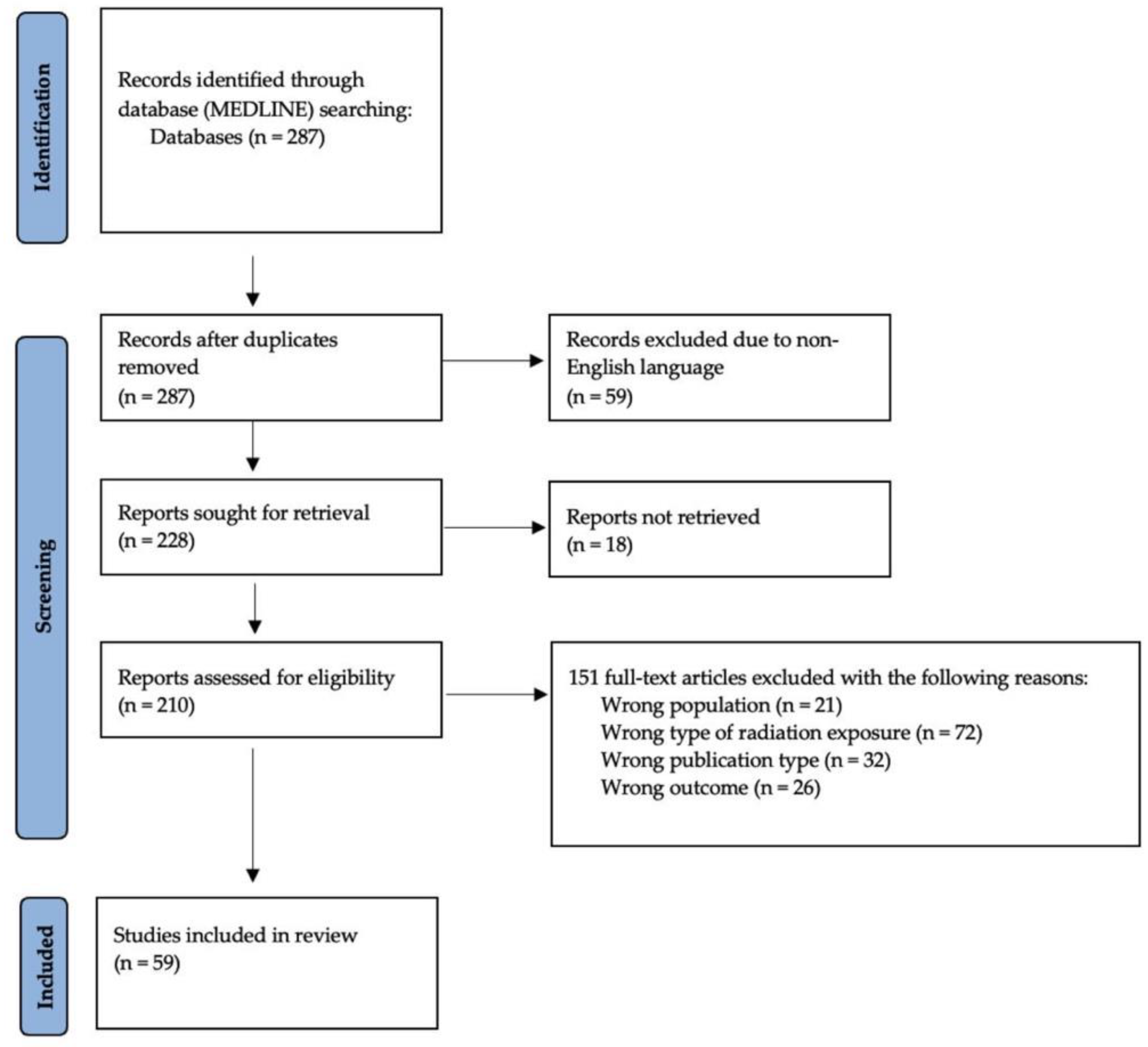
2. Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
3. Results
4. Discussion
5. Key Mental Health Disorders and Associated Risk Factors
5.1. Post-Traumatic Stress Disorder (PTSD)
5.2. Depression and Suicidality
5.3. Anxiety Disorders
6. Protective Factors and Vulnerable Populations
7. Comparison of Three Nuclear Disasters
8. Individual-Level Interventions Aimed at Mitigating Psychological Distress
9. Population-Based Interventions, Public Policy, and Practice Interventions
9.1. Trust in Experts and Sources of Information
9.2. Radiation Countermeasures
9.3. Technology-Based Population Supports
10. Limitations
11. Conclusions and Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Davidson, L.M.; Baum, A. Chronic stress and posttraumatic stress disorders. J. Consult. Clin. Psychol. 1986, 54, 303–308. [Google Scholar] [CrossRef]
- Baum, A.; Gatchel, R.J.; Schaeffer, M.A. Emotional, behavioral, and physiological effects of chronic stress at Three Mile Island. J. Consult. Clin. Psychol. 1983, 51, 565–572. [Google Scholar] [CrossRef]
- Bromet, E.; Schulberg, H.C.; Dunn, L. Reactions of psychiatric patients to the Three Mile Island nuclear accident. Arch. Gen. Psychiatry 1982, 39, 725–730. [Google Scholar] [CrossRef] [PubMed]
- Dew, M.A.; Bromet, E.J.; Schulberg, H.C. A comparative analysis of two community stressors’ long-term mental health effects. Am. J. Community Psychol. 1987, 15, 167–184. [Google Scholar] [CrossRef] [PubMed]
- Prince-Embury, S.; Rooney, J.F. Psychological adaptation among residents following restart of Three Mile Island. J. Trauma. Stress 1995, 8, 47–59. [Google Scholar] [CrossRef] [PubMed]
- Prince-Embury, S.; Rooney, J.F. Psychological symptoms of residents in the aftermath of the Three Mile Island nuclear accident and restart. J. Soc. Psychol. 1988, 128, 779–790. [Google Scholar] [CrossRef]
- Solomon, Z. Stress, social support and affective disorders in mothers of pre-school children—a test of the stress-buffering effect of social support. Soc. Psychiatry 1985, 20, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Steinhauser, G.; Brandl, A.; Johnson, T.E. Comparison of the Chernobyl and Fukushima nuclear accidents: A review of the environmental impacts. Sci. Total Environ. 2014, 470, 800–817. [Google Scholar] [CrossRef]
- Hasegawa, A.; Tanigawa, K.; Ohtsuru, A.; Yabe, H.; Maeda, M.; Shigemura, J.; Ohira, T.; Tominaga, T.; Akashi, M.; Hirohashi, N.; et al. Health effects of radiation and other health problems in the aftermath of nuclear accidents, with an emphasis on Fukushima. Lancet 2015, 386, 479–488. [Google Scholar] [CrossRef]
- Shigemura, J.; Terayama, T.; Kurosawa, M.; Kobayashi, Y.; Toda, H.; Nagamine, M.; Yoshino, A. Mental health consequences for survivors of the 2011 Fukushima nuclear disaster: A systematic review. Part 1: Psychological consequences. CNS Spectr. 2020, 26, 14–29. [Google Scholar] [CrossRef]
- Terayama, T.; Shigemura, J.; Kobayashi, Y.; Kurosawa, M.; Nagamine, M.; Toda, H.; Yoshino, A. Mental health consequences for survivors of the 2011 Fukushima nuclear disaster: A systematic review. Part 2: Emotional and behavioral consequences. CNS Spectr. 2020, 26, 30–42. [Google Scholar] [CrossRef] [PubMed]
- Takebayashi, Y.; Lyamzina, Y.; Suzuki, Y.; Murakami, M. Risk Perception and Anxiety Regarding Radiation after the 2011 Fukushima Nuclear Power Plant Accident: A Systematic Qualitative Review. Int. J. Environ. Res. Public Health 2017, 14, 1306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuroda, Y.; Iwasa, H.; Orui, M.; Moriyama, N.; Nakayama, C.; Yasumura, S. Association between Health Literacy and Radiation Anxiety among Residents after a Nuclear Accident: Comparison between Evacuated and Non-Evacuated Areas. Int. J. Environ. Res. Public Health 2018, 15, 1463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murakami, M.; Harada, S.; Oki, T. Decontamination Reduces Radiation Anxiety and Improves Subjective Well-Being after the Fukushima Accident. Tohoku J. Exp. Med. 2017, 241, 103–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakayama, C.; Sato, O.; Sugita, M.; Nakayama, T.; Kuroda, Y.; Orui, M.; Iwasa, H.; Yasumura, S.; Rudd, R.E. Lingering health-related anxiety about radiation among Fukushima residents as correlated with media information following the accident at Fukushima Daiichi Nuclear Power Plant. PLoS ONE 2019, 14, e0217285. [Google Scholar] [CrossRef]
- Orui, M.; Nakayama, C.; Kuroda, Y.; Moriyama, N.; Iwasa, H.; Horiuchi, T.; Nakayama, T.; Sugita, M.; Yasumura, S. The Association between Utilization of Media Information and Current Health Anxiety Among the Fukushima Daiichi Nuclear Disaster Evacuees. Int. J. Environ. Res. Public Health 2020, 17, 3921. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, A.; Nomura, S.; Tsubokura, M.; Matsumura, T.; Muto, K.; Sato, M.; Gilmour, S. The relationship between media consumption and health-related anxieties after the Fukushima Daiichi nuclear disaster. PLoS ONE 2013, 8, e65331. [Google Scholar] [CrossRef] [Green Version]
- Page, M.A.-O.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Abramenko, I.V.; Bilous, N.I.; Chumak, S.A.; Loganovsky, K.M. Influence of polymorphic variants of the SLC6A4 gene on the frequency of detection of depressive states in the group of the clean up workers of consequences of Chornobyl accident in the remote period after the Chornobyl catastrophe. Probl. Radiac. Med. Ta Radiobiol. 2017, 22, 282–291. [Google Scholar] [CrossRef] [Green Version]
- Adams, R.E.; Guey, L.T.; Gluzman, S.F.; Bromet, E.J. Psychological well-being and risk perceptions of mothers in Kyiv, Ukraine, 19 years after the Chornobyl disaster. Int. J. Soc. Psychiatry 2011, 57, 637–645. [Google Scholar] [CrossRef]
- Bromet, E.J.; Gluzman, S.; Schwartz, J.E.; Goldgaber, D. Somatic symptoms in women 11 years after the Chornobyl accident: Prevalence and risk factors. Environ. Health Perspect. 2002, 110, 625–629. [Google Scholar] [CrossRef] [Green Version]
- Cwikel, J.; Abdelgani, A.; Goldsmith, J.R.; Quastel, M.; Yevelson, I.I. Two-year follow up study of stress-related disorders among immigrants to Israel from the Chernobyl area. Environ. Health Perspect. 1997, 105, 1545–1550. [Google Scholar]
- Cwikel, J.; Rozovski, U. Coping with the stress of immigration among new immigrants to Israel from Commonwealth of Independent States (CIS) who were exposed to Chernobyl: The effect of age. Int. J. Aging Hum. Dev. 1998, 46, 305–318. [Google Scholar] [CrossRef] [PubMed]
- Foster, R.P. The long-term mental health effects of nuclear trauma in recent Russian immigrants in the United States. Am. J. Orthopsychiatry 2002, 72, 492–504. [Google Scholar] [CrossRef]
- Loganovsky, K.; Havenaar, J.M.; Tintle, N.L.; Guey, L.T.; Kotov, R.; Bromet, E.J. The mental health of clean-up workers 18 years after the Chernobyl accident. Psychol. Med. 2008, 38, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Loganovsky, K.N.; Zdanevich, N.A. Cerebral basis of posttraumatic stress disorder following the Chernobyl disaster. CNS Spectr. 2013, 18, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Rahu, K.; Rahu, M.; Tekkel, M.; Bromet, E. Suicide risk among Chernobyl cleanup workers in Estonia still increased: An updated cohort study. Ann. Epidemiol. 2006, 16, 917–919. [Google Scholar] [CrossRef]
- Anderson, D.; Prioleau, P.; Taku, K.; Naruse, Y.; Sekine, H.; Maeda, M.; Yabe, H.; Katz, C.; Yanagisawa, R. Post-traumatic Stress and Growth Among Medical Student Volunteers After the March 2011 Disaster in Fukushima, Japan: Implications for Student Involvement with Future Disasters. Psychiatr. Q. 2016, 87, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Aoki, Y.; Okada, M.; Inokuchi, R.; Matsumoto, A.; Kumada, Y.; Yokoyama, H.; Ishida, T.; Saito, I.; Ito, H.; Sato, H.; et al. Time-related changes in suicide attempts after the nuclear accident in Fukushima. Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 1911–1918. [Google Scholar] [CrossRef]
- Cavanagh, S.R.; Fitzgerald, E.J.; Urry, H.L. Emotion reactivity and regulation are associated with psychological functioning following the 2011 earthquake, tsunami, and nuclear crisis in Japan. Emotion 2014, 14, 235–240. [Google Scholar] [CrossRef]
- Goto, A.; Bromet, E.J.; Fujimori, K. Pregnancy and Birth Survey Group of Fukushima Health Management Survey. Immediate effects of the Fukushima nuclear power plant disaster on depressive symptoms among mothers with infants: A prefectural-wide cross-sectional study from the Fukushima Health Management Survey. BMC Psychiatry 2015, 15, 59. [Google Scholar]
- Goto, A.; Bromet, E.J.; Ota, M.; Ohtsuru, A.; Yasumura, S.; Fujimori, K. Pregnancy and Birth Survey Group of the Fukushima Health Management Survey. The Fukushima Nuclear Accident Affected Mothers’ Depression but Not Maternal Confidence. Asia-Pac. J. Public Health 2017, 29, 139S–150S. [Google Scholar] [CrossRef] [Green Version]
- Hidaka, T.; Kakamu, T.; Hayakawa, T.; Kumagai, T.; Jinnouchi, T.; Sato, S.; Tsuji, M.; Nakano, S.; Koyama, K.; Fukushima, T. Effect of age and social connection on perceived anxiety over radiation exposure among decontamination workers in Fukushima Prefecture, Japan. J. Occup. Health 2016, 58, 186–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hori, A.; Hoshino, H.; Miura, I.; Hisamura, M.; Wada, A.; Itagaki, S.; Kunii, Y.; Matsumoto, J.; Mashiko, H.; Katz, C.L.; et al. Psychiatric Outpatients After the 3.11 Complex Disaster in Fukushima, Japan. Ann. Glob. Health 2016, 82, 798–805. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, A.; Tanigawa, T.; Charvat, H.; Wada, H.; Shigemura, J.; Kawachi, I. Longitudinal effects of disaster-related experiences on mental health among Fukushima nuclear plant workers: The Fukushima NEWS Project Study. Psychol. Med. 2017, 47, 1936–1946. [Google Scholar] [CrossRef] [PubMed]
- Imamura, K.; Sekiya, Y.; Asai, Y.; Umeda, M.; Horikoshi, N.; Yasumura, S.; Yabe, H.; Akiyama, T.; Kawakami, N. The effect of a behavioral activation program on improving mental and physical health complaints associated with radiation stress among mothers in Fukushima: A randomized controlled trial. BMC Public Health 2016, 16, 1144. [Google Scholar] [CrossRef] [Green Version]
- Ishii, K.; Goto, A.; Ota, M.; Yasumura, S.; Fujimori, K. Pregnancy and Birth Survey of the Fukushima Health Management Survey. Asia-Pac. J. Public Health 2017, 29, 56S–62S. [Google Scholar] [CrossRef] [Green Version]
- Ishikawa, S.-i.; Motoya, R.; Sasagawa, S.; Takahashi, T.; Okajima, I.; Takeishi, Y.; Essau, C.A. Mental Health Problems among Undergraduates in Fukushima, Tokyo, and Kyoto after the March 11 Tohoku Earthquake. Tohoku J. Exp. Med. 2015, 236, 115–122. [Google Scholar] [CrossRef] [Green Version]
- Ito, S.; Sasaki, M.; Okabe, S.; Konno, N.; Goto, A. Depressive Symptoms and Associated Factors in Female Students in Fukushima Four Years after the Fukushima Nuclear Power Plant Disaster. Int. J. Environ. Res. Public Health 2018, 15, 2411. [Google Scholar] [CrossRef] [Green Version]
- Kakamu, T.; Hidaka, T.; Kumagai, T.; Jinnouchi, T.; Sato, S.; Masuishi, Y.; Endo, S.; Nakano, S.; Koyama, K.; Fukushima, T. Characteristics of anxiety and the factors associated with presence or absence of each anxiety among radiation decontamination workers in Fukushima. Ind. Health 2019, 57, 580–587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kashiwazaki, Y.; Takebayashi, Y.; Murakami, M. Relationships between radiation risk perception and health anxiety, and contribution of mindfulness to alleviating psychological distress after the Fukushima accident: Cross-sectional study using a path model. PLoS ONE 2020, 15, e0235517. [Google Scholar] [CrossRef]
- Kawakami, N.; Fukasawa, M.; Sakata, K.; Suzuki, R.; Tomita, H.; Nemoto, H.; Yasumura, S.; Yabe, H.; Horikoshi, N.; Umeda, M.; et al. Onset and remission of common mental disorders among adults living in temporary housing for three years after the triple disaster in Northeast Japan: Comparisons with the general population. BMC Public Health 2020, 20, 1271. [Google Scholar] [CrossRef]
- Kohzaki, M.; Ootsuyama, A.; Moritake, T.; Abe, T.; Kubo, T.; Okazaki, R. What have we learned from a questionnaire survey of citizens and doctors both inside and outside Fukushima?: Survey comparison between 2011 and 2013. J. Radiol. Prot. 2015, 35, N1. [Google Scholar] [CrossRef] [Green Version]
- Kukihara, H.; Yamawaki, N.; Uchiyama, K.; Arai, S.; Horikawa, E. Trauma, depression, and resilience of earthquake/tsunami/nuclear disaster survivors of Hirono, Fukushima, Japan. Psychiatry Clin. Neurosci. 2014, 68, 524–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuroda, Y.; Iwasa, H.; Goto, A.; Yoshida, K.; Matsuda, K.; Iwamitsu, Y.; Yasumura, S. Occurrence of depressive tendency and associated social factors among elderly persons forced by the Great East Japan Earthquake and nuclear disaster to live as long-term evacuees: A prospective cohort study. BMJ Open 2017, 7, e014339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kusama, T.; Aida, J.; Tsuboya, T.; Sugiyama, K.; Yamamoto, T.; Igarashi, A.; Osaka, K. The association between socioeconomic status and reactions to radiation exposure: A cross-sectional study after the Fukushima Daiichi nuclear power station accident. PLoS ONE 2018, 13, e0205531. [Google Scholar] [CrossRef] [PubMed]
- Lebowitz, A.J. Cross-Sectional Data Within 1 Year of the Fukushima Meltdown: Effect-Size of Predictors for Depression. Community Ment. Health J. 2016, 52, 94–101. [Google Scholar] [CrossRef]
- Lebowitz, A.J. Relational Satisfaction from Providing and Receiving Support is Associated with Reduced Post-Disaster Depression: Data From Within One Year of the 2011 Japan Triple Disaster. Community Ment. Health J. 2017, 53, 202–214. [Google Scholar] [CrossRef]
- Maeda, M.; Ueda, Y.; Nagai, M.; Fujii, S.; Oe, M. Diagnostic interview study of the prevalence of depression among public employees engaged in long-term relief work in Fukushima. Psychiatry Clin. Neurosci. 2016, 70, 413–420. [Google Scholar] [CrossRef] [Green Version]
- Murakami, M.; Hirosaki, M.; Suzuki, Y.; Maeda, M.; Yabe, H.; Yasumura, S.; Ohira, T. Reduction of radiation-related anxiety promoted wellbeing after the 2011 disaster: ’Fukushima Health Management Survey’. J. Radiol. Prot. 2018, 38, 1428–1440. [Google Scholar] [CrossRef] [PubMed]
- Murakami, M.; Takebayashi, Y.; Takeda, Y.; Sato, A.; Igarashi, Y.; Sano, K.; Yasutaka, T.; Naito, W.; Hirota, S.; Goto, A.; et al. Effect of Radiological Countermeasures on Subjective Well-Being and Radiation Anxiety after the 2011 Disaster: The Fukushima Health Management Survey. Int. J. Environ. Res. Public Health 2018, 15, 124. [Google Scholar] [CrossRef] [Green Version]
- Nagamine, M.; Yamamoto, T.; Shigemura, J.; Tanichi, M.; Yoshino, A.; Suzuki, G.; Takahashi, Y.; Miyazaki, M.; Uwabe, Y.; Harada, N.; et al. The Psychological Impact of the Great East Japan Earthquake on Japan Ground Self-Defense Force Personnel: A Three-Wave, One-Year Longitudinal Study. Psychiatry 2018, 81, 288–296. [Google Scholar] [CrossRef] [PubMed]
- Oe, M.; Fujii, S.; Maeda, M.; Nagai, M.; Harigane, M.; Miura, I.; Yabe, H.; Ohira, T.; Takahashi, H.; Suzuki, Y.; et al. Three-year trend survey of psychological distress, post-traumatic stress, and problem drinking among residents in the evacuation zone after the Fukushima Daiichi Nuclear Power Plant accident [The Fukushima Health Management Survey]. Psychiatry Clin. Neurosci. 2016, 70, 245–252. [Google Scholar] [CrossRef]
- Oe, M.; Maeda, M.; Nagai, M.; Yasumura, S.; Yabe, H.; Suzuki, Y.; Harigane, M.; Ohira, T.; Abe, M. Predictors of severe psychological distress trajectory after nuclear disaster: Evidence from the Fukushima Health Management Survey. BMJ Open 2016, 6, e013400. [Google Scholar] [CrossRef]
- Oe, M.; Takahashi, H.; Maeda, M.; Harigane, M.; Fujii, S.; Miura, I.; Nagai, M.; Yabe, H.; Ohira, T.; Suzuki, Y.; et al. Changes of Posttraumatic Stress Responses in Evacuated Residents and Their Related Factors. Asia-Pac. J. Public Health 2017, 29, 182S–192S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orui, M.; Suzuki, Y.; Maeda, M.; Yasumura, S. Suicide Rates in Evacuation Areas After the Fukushima Daiichi Nuclear Disaster. Crisis J. Crisis Interv. Suicide 2018, 39, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Rubin, G.J.; Amlot, R.; Wessely, S.; Greenberg, N. Anxiety, distress and anger among British nationals in Japan following the Fukushima nuclear accident. Br. J. Psychiatry 2012, 201, 400–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shigemura, J.; Someda, H.; Tokuno, S.; Nagamine, M.; Tanichi, M.; Araki, Y.; Nagakawa, S.; Saito, T.; Tsumatori, G.; Itabashi, J.; et al. Disaster Victim Identification: Psychological Distress and Posttraumatic Stress in Dentists After the 2011 Fukushima Disaster. Psychiatry 2018, 81, 85–92. [Google Scholar] [CrossRef]
- Shigemura, J.; Tanigawa, T.; Nishi, D.; Matsuoka, Y.; Nomura, S.; Yoshino, A. Associations between disaster exposures, peritraumatic distress, and posttraumatic stress responses in Fukushima nuclear plant workers following the 2011 nuclear accident: The Fukushima NEWS Project study. PLoS ONE 2014, 9, e87516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanisho, Y.; Shigemura, J.; Kubota, K.; Tanigawa, T.; Bromet, E.J.; Takahashi, S.; Matsuoka, Y.; Nishi, D.; Nagamine, M.; Harada, N.; et al. The longitudinal mental health impact of Fukushima nuclear disaster exposures and public criticism among power plant workers: The Fukushima NEWS Project study. Psychol. Med. 2016, 46, 3117–3125. [Google Scholar] [CrossRef] [Green Version]
- Tsubokura, M.; Hara, K.; Matsumura, T.; Sugimoto, A.; Nomura, S.; Hinata, M.; Shibuya, K.; Kami, M. The immediate physical and mental health crisis in residents proximal to the evacuation zone after Japan’s nuclear disaster: An observational pilot study. Disaster Med. Public Health Prep. 2014, 8, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Tsujiuchi, T.; Yamaguchi, M.; Masuda, K.; Tsuchida, M.; Inomata, T.; Kumano, H.; Kikuchi, Y.; Augusterfer, E.F.; Mollica, R.F. High Prevalence of Post-Traumatic Stress Symptoms in Relation to Social Factors in Affected Population One Year after the Fukushima Nuclear Disaster. PLoS ONE 2016, 11, e0151807. [Google Scholar] [CrossRef]
- Agyapong, V. Coronavirus Disease 2019 Pandemic: Health System and Community Response to a Text Message (Text4Hope) Program Supporting Mental Health in Alberta. Disaster Med. Public Health Prep. 2020, 14, e5–e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agyapong, V.; Hrabok, M.; Shalaby, R.; Vuong, W.; Noble, J.; Gusnowski, A.; Mrklas, K.; Li, D.; Urichuck, L.; Snaterse, M.; et al. Text4Hope: Receiving Daily Supportive Text Messages for 3 Months During the COVID-19 Pandemic Reduces Stress, Anxiety, and Depression. Disaster Med. Public Health Prep. 2021, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Agyapong, V.; Hrabok, M.; Vuong, W.; Gusnowski, A.; Shalaby, R.; Mrklas, K.; Li, D.; Urichuk, L.; Snaterse, M.; Surood, S.; et al. Closing the Psychological Treatment Gap During the COVID-19 Pandemic With a Supportive Text Messaging Program: Protocol for Implementation and Evaluation. JMIR Res. Protoc. 2020, 9, e19292. [Google Scholar] [CrossRef]
- Agyapong, V.; Shalaby, R.; Hrabok, M.; Vuong, W.; Noble, J.; Gusnowski, A.; Mrklas, K.; Li, D.; Snaterse, M.; Surood, S.; et al. Mental Health Outreach via Supportive Text Messages during the COVID-19 Pandemic: Improved Mental Health and Reduced Suicidal Ideation after Six Weeks in Subscribers of Text4Hope Compared to a Control Population. Int. J. Environ. Res. Public Health 2021, 18, 2157. [Google Scholar] [CrossRef]
- Agyapong, V.; Ahern, S.; McLoughlin, D.; Farren, C.K. Supportive text messaging for depression and comorbid alcohol use disorder: Single-blind randomised trial. J. Affect. Disord. 2012, 141, 168–176. [Google Scholar] [CrossRef]
- Agyapong, V.; Mrklas, K.; Juhás, M.; Omeje, J.; Ohinmaa, A.; Dursun, S.; Greenshaw, A. Cross-sectional survey evaluating Text4Mood: Mobile health program to reduce psychological treatment gap in mental healthcare in Alberta through daily supportive text messages. BMC Psychiatry 2016, 16, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Agyapong, V.; Juhás, M.; Ohinmaa, A.; Omeje, J.; Mrklas, K.; Suen, V.; Dursun, S.; Greenshaw, A. Randomized controlled pilot trial of supportive text messages for patients with depression. BMC Psychiatry 2017, 17, 1–10. [Google Scholar] [CrossRef] [Green Version]
- O’Reilly, H.; Hagerty, A.; O’Donnell, S.; Farrell, A.; Hartnett, D.; Murphy, E.; Kehoe, E.; Agyapong, V.; McLoughlin, D.; Farren, C. Alcohol Use Disorder and Comorbid Depression: A Randomized Controlled Trial Investigating the Effectiveness of Supportive Text Messages in Aiding Recovery. Alcohol Alcholism 2019, 54, 551–558. [Google Scholar] [CrossRef]
- Shalaby, R.; Vuong, W.; Hrabok, M.; Gusnowski, A.; Mrklas, K.; Li, D.; Snaterse, M.; Surood, S.; Cao, B.; Li, X.; et al. Gender Differences in Satisfaction With a Text Messaging Program (Text4Hope) and Anticipated Receptivity to Technology-Based Health Support During the COVID-19 Pandemic: Cross-sectional Survey Study. JMIR MHealth UHealth 2021, 9, e24184. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Reference/ Nuclear Disaster | Sample | Final Sample Size | Study Period | Outcomes | Key Findings |
|---|---|---|---|---|---|
| Baum et al. (1983) [2] | Residents of Three Mile Island and three control groups | 121 (38 in TMI group, 32 in undamaged nuclear plant group, 24 in coal plant group, 27 in no plant group) | August 1980 | Stress (psychological, behavioural, and biochemical measures) | Residents of TMI exhibited more symptoms of stress (self-report, performance, and catecholamine levels) than the other three groups. |
| Bromet et al. (1982) [3] | Psychiatric patients treated in the six months prior to the Three Mile Island accident | 215 (151 from Three Mile Island, 64 from comparison area) | December 1979–January 1980, March–April 1980 | Mental health diagnoses (SADS-L), general psychological distress (GSI) | Rates of psychiatric conditions did not increase after the TMI accident. Greater psychological distress was associated with lower social support and perceiving the reactor as dangerous. |
| Davidson and Baum (1986) [1] | Residents living within 5 miles of Three Mile Island and a control group of residents living at least 80 miles from TMI | 87 (52 in TMI group, 35 in control group) | January 1984 | Stress (psychological, behavioral, and biochemical measures), PTSS (IES) | Residents of TMI exhibited more symptoms of stress (self-report, performance, and catecholamine levels) and greater PTSS. |
| Dew et al. (1987) [4] | Married women who delivered a child between January 1978 and March 1979 who experienced a community-wide stressor | 361 (257 who lived within 10 miles of the TMI facility, 104 who lived near a plant that experienced widespread layoffs) | December 1979, March 1980, September 1981, September 1982, September 1983 (layoff group only) | Subclinical psychological symptomatology (SCL-90) | Levels of psychological symptoms were similar between groups at all timepoints. Presence of a pre-existing psychiatric diagnosis predicted enduring distress in both groups. |
| Prince-Embury and Rooney (1988) [5] | Residents of Three Mile Island at the time of the reactor restart in 1985 | 108 | November 1985 | Psychological symptoms (SCL-90-R) | Psychological symptoms were chronically elevated for residents who remained at TMI after the 1979 accident. |
| Prince-Embury and Rooney (1995) [6] | Residents of Three Mile Island at the time of the reactor restart in 1985 still living in the area in 1989 | 64 | November 1985, June 1989 | Psychological symptoms (SCL-90-R) | A lowering of psychological symptoms occurred between 1985 and 1989 despite increased lack of control, less faith in experts, and increased fear of developing cancer. |
| Solomon (1985) [7] | Mothers from two semi-rural regions of Pennsylvania (TMI and control) | 436 (312 from Three Mile Island, 124 from the control area) | March–April 1980 | Psychiatric disorder (SADS-L) | Women with worse social support were more likely to develop a psychiatric disorder following the TMI nuclear accident. |
| Reference/ Nuclear Disaster | Sample | Final Sample Size | Study Period | Outcomes | Key Findings |
|---|---|---|---|---|---|
| Abramenko et al. (2017) [19] | Male clean-up workers | 59 | 1986 | Depressive symptoms | Workers who experienced ARS reported more depressive symptoms than those who did not. |
| Adams et al. (2011) [20] | Mothers with small children in Kyiv, Ukraine | 797 (254 evacuees, 239 neighborhood controls, 203 population-based controls) | 2005–2006 | PTSD (IES-R), MDE (CIDI), general psychological distress (SCL-90) | Evacuees reported more negative risk perceptions and poorer overall well-being than the two control groups. |
| Bromet et al. (2002) [21] | Mothers with small children in Kyiv, Ukraine | 600 (300 evacuees, 300 controls) | February–May 1997 | Perceived health, Chernobyl-related stress, PTSD (IES) | Evacuees had worse health, more Chernobyl-related illness, higher Chernobyl-related stress, and greater rates of PTSD (18% of evacuees vs. 9.7% of controls). |
| Cwikel et al. (1997) [22] | Immigrants from the Commonwealth of Independent States (CIS) living in Israel | 520 (87 from high-exposure areas, 217 from low-exposure areas, and 216 from comparison areas) | 1993–1996 | PTSS (IES), depression (CES-D), somatization (SCL-90), anxiety (SCL-90 | At eight years after the accident, the exposure group had higher rates of PTSS, depressive symptoms, somatization, and anxiety than the comparison group. |
| Cwikel and Rozovski (1998) [23] | Immigrants from the Commonwealth ofIndependent States (CIS) living in Israel | 520 (87 from high-exposure areas, 217 from low-exposure areas, and 216 from comparison areas) | 1993–1996 | PTSS (IES), depressive symptoms (CES-D), somatization (SCL-90), anxiety (SCL-90 | Rates of somatization, depressive symptoms, and PTSS symptoms improved at a slower rate for immigrants who were 55 and older compared to younger immigrants. |
| Foster (2002) [24] | Russian immigrants residing in New York City | 261 | 2001 | Depression (BDI), anxiety (BAI), PTSS (MISS PTSD) | Participants who lived closer to the reactor had higher levels of anxiety and PTSS 15 years after the accident than those who lived further away. |
| Loganovsky et al. (2008) [25] | Male clean-up workers sent to Chernobyl between 1986 and 1990 and geographically matched controls | 692 (295 clean-up workers, 397 geographically matched controls) | March–December 2002, December 2003–June 2004 | Depressive disorders, anxiety disorders, alcohol abuse, and intermittent explosive disorder (CIDI), PTSD (IES), somatization (SCL-90), suicidal ideation | Clean-up workers were more likely than controls to experience depression (18.0% vs. 13.1%) and suicidal ideation (9.2% vs. 4.1%) after the Chernobyl accident. Eighteen years after the accident, rates of depression and PTSD were still elevated in the clean-up workers compared to the control group. |
| Loganovsky et al. (2013) [26] | Patients with PTSD and population controls | 241 (34 Chernobyl clean-up workers with PTSD and ARS, 81 Chernobyl clean-up workers with PTSD without ARS, 76 Chernobyl evacuees with PTSD, 28 Afghanistan war veterans with PTSD, and 22 healthy controls without PTSD) | 2011–2012 | Radiation PTSD, neurological deficits, cognitive functions, neurophysiologic studies (EEG and carotid and cerebral ultrasounds) | Radiation PTSD includes “flashforward” phenomena, somatoform disorders, and neurocognitive deficits. Structural brain changes were demonstrated in Chernobyl clean-up workers, and changes in bioelectrical brain activity were demonstrated in Chernobyl survivors with PTSD. |
| Rahu et al. (2006) [27] | Men from Estonia who participated in the Chernobyl clean-up between 1986 and 1991 | 4786 | 1992–2002 | Mortality | Compared to population rates, clean-up workers had increased risk of suicide, but no elevated mortality risk. |
| Reference/ Nuclear Disaster | Sample | Final Sample Size | Study Period | Outcomes | Key Findings |
|---|---|---|---|---|---|
| Anderson et al. (2016) [28] | Fukushima Medical University students | 494 (132 volunteers, 362 non-volunteers) | July 2014 | Post-traumatic growth, psychological distress (confusion, anger, and sadness) | Higher post-traumatic growth in volunteers than non-volunteers, but no difference in distressing symptoms. |
| Aoki et al. (2014) [29] | Clinical records of all patients who visited the Ohta Nishinouchi medical center in the study period | 981 (493 in control year, 488 in study year) | March 2010–March 2011, March 2011–March 2012 | Non-fatal suicide attempts | The risk of suicide attempt by high-mortality means was elevated for four months after the disaster. There was no change in rates of low lethality attempts. |
| Cavanagh et al. (2014) [30] | Members of the U.S. Embassy in Tokyo | 120 | July 2011 | Psychological functioning (PTSS, depressive symptoms, and life satisfaction) | Self-reported use of cognitive reappraisal was not related to psychological functioning, but demonstrated success using cognitive reappraisal techniques was associated with fewer symptoms of depression and PTSS. |
| Goto et al. (2015) [31] | Women living in Fukushima who registered their pregnancies in a one-year period | 8196 | August 2010–July 2011 | Depressive symptoms (two-item screening measure) | 28% of women reported depressive symptoms. Living close to the reactor was associated with greater depressive symptoms. |
| Goto et al. (2017) [32] | Women living in Fukushima who registered their pregnancies in a two-year period | 13,109 (6686 in 2012, 6423 in 2013) | August 2011–July 2012, August 2012–July 2013 | Depressive symptoms (two-item screening measure) | 25% of mothers reported depressive symptoms in 2012, and 24% reported depressive symptoms in 2013. Higher radiation concern was associated with depressive symptoms. |
| Hidaka et al. (2016) [33] | Fukushima decontamination workers | 512 | August–October 2013 | Radiation anxiety | 44.7% of decontamination workers reported radiation anxiety. Socially isolated workers reported more anxiety over radiation exposure. |
| Hori et al. (2016) [34] | New patients in Fukushima outpatient psychiatry clinics in a three-month period | 2504 (771 in 2010, 1000 in 2011, 733 in 2012) | March–June 2010, March–June 2011, March–June 2012 | Diagnosis of ASD, PTSD, adjustment disorder and depression (ICD-10) | Increased incidence of new patients with ASD and PTSD in 2011 and decreased incidence of new patients with depression. These results returned to pre-disaster levels in 2012. |
| Ikeda et al. (2017) [35] | Fukushima nuclear power plant workers at TEPCO Daiichi (affected reactor) and Daini (intact reactor) | 1417 (1053 from Daiichi, 707 from Daini) | May–June 2011, May–June 2012, November 2013,November 2014 | Psychological Distress (K6), PTSS (IES-R) | Post-traumatic stress response symptoms decreased over time but remained elevated three years after the nuclear disaster. |
| Imamura et al. (2016) [36] | Mothers with preschool children in Fukushima city and surrounding areas | 37 (18 in behavioural activation intervention group, 19 in control group) | August 2014, September 2014, November 2014 | Psychological distress (K6), physical symptoms (BJSQ), radiation anxiety, positive well-being (liveliness and life satisfaction) | Behavioural activation was associated with lower psychological distress and less physical symptoms at the one-month follow-up, but not at three months. Behavioural activation was associated with higher life satisfaction and increased liveliness at the three-month follow-up. |
| Ishii et al. (2017) [37] | Women who received Maternal and Child Health Handbooks from municipal offices in Fukushima from 2011 to 2014 | 60,860 (16,001 in 2011, 14,516 in 2011, 15,218 in 2013, 14,516 in 2014) | 2011–2014 | Depressive symptoms (two-item screening measure) | 27% of mothers reported depressive symptoms in 2011, 26% in 2012, 25% in 2013, and 23% in 2014. |
| Ishikawa at al. (2015) [38] | Undergraduates from universities in Fukushima, Tokyo, and Kyoto | 435 (106 from Fukushima, 176 from Tokyo, 153 from Kyoto) | September–December 2013 | Trauma response (IES-R), depressive symptoms (CES-D), anger (STAXI), anxiety (SEA) | Tokyo undergraduates had the most significant traumatic response immediately after the earthquake. Fukushima undergraduates had the highest levels of anger. Kyoto undergraduates had more anxiety and depressive symptoms 2.5 years after the nuclear disaster than immediately after the accident. |
| Ito et al. (2018) [39] | Female college students | 288 | December 2015 | Depressive symptoms (WHO-5), radiation risk perception | 46.5% of female college students reported depressive symptoms. Higher radiation risk perception predicted reduced reproductive confidence, which was ultimately associated with increased depressive symptoms. |
| Kakamu et al. (2019) [40] | Radiation decontamination workers | 531 | August–October 2013 | Type of anxiety | 91.6% of decontamination workers reported at least one type of anxiety. Job security was the most common type of anxiety (41.8%) and working hours was the least common (6.0%). |
| Kashiwazaki et al. (2020) [41] | Residents of Fukushima and Tokyo aged 20–59 years | 832 (416 from Fukushima, 416 on Tokyo) | August 2018 | Health anxiety (HAI), psychological distress (K6) | Greater health anxiety was associated with more psychological distress. Mindfulness was associated with lower health anxiety and less psychological distress. |
| Kawakami et al. (2020) [42] | Adults living in temporary housing for three years after the nuclear disaster and a control group of residents from non-disaster areas of East Japan | 1941 (1089 in shelter group, 852 in control group) | June–August 2014 | MDE, manic or hypomanic episode, GAD, panic disorder, PTSD, and alcohol use disorder (CIDI) | The shelter group had a higher incidence of new mood and anxiety disorders in the first year after the disaster, but not in subsequent years. The remission rate for mood and anxiety disorders was lower in the shelter group. |
| Kohzaki et al. (2015) [43] | Citizens, doctors, and medical students inside and outside Fukushima | 2487 (1557 in 2011, 930 in 2013) | September–October 2011; August–November 2013 | Radiation anxiety | Citizens living in Fukushima were more anxious than those living outside Fukushima. Medical students who recently studied radiation biology were less anxious than the other groups. All three groups reported dissatisfaction with the government and TEPCO after the nuclear accident. |
| Kukihara et al. (2014) [44] | Evacuees from Hirono Town | 241 (116 men, 125 women) | December 2011 | PTSS (IES-R), depressive symptoms (ZSDS), resilience (CD-RISC) | 53.5% reported symptoms of PTSD, and 66.8% reported symptoms of depression. Resilience was shown to be a protective factor for PTSD, depression, and general health. |
| Kuroda et al. (2017) [45] | Elderly evacuees without a baseline depressive tendency | 438 | May 2010, May 2013 | Depressive tendency (BCL) | In elderly evacuees who did not report a depressive tendency at baseline, 37.2% had a depressive tendency at the second survey. Depressive tendency was associated with female sex, older age, and less engagement in social activities. |
| Kuroda, Iwasa, Orui, Moriyama, Nakayama, and Yasumura (2018) [13] | Fukushima residents | 777 (606 from non-evacuation areas, 171 from evacuation areas) | August–October 2016 | Radiation anxiety, discrimination and prejudice based on radiation exposure | Higher health literacy was associated with lower radiation anxiety in both areas and associated with lower discrimination and prejudice in the evacuation areas. |
| Kusama et al. (2018) [46] | Residents of Japan | 10,000 | March 2012 | Anxiety, radiation risk-averse behaviours | 23.0% of participants reported anxiety and 12.0% engaged in radiation risk-averse behaviours. Those with higher socioeconomic status felt less anxious, but engaged in more risk-averse behaviours than those with lower socioeconomic status. |
| Lebowitz (2016) [47] | Residents from Hirakata, Japan, and Otsu, Japan | 466 (351 female, 115 male) | December 2011–March 2012 | Depression (CES-D) | 23% of female participants and 17% of male participants met criteria for depression. The strongest predictors of depression were property damage and younger age. |
| Lebowitz (2017) [48] | Residents from Hirakata, Japan, and Otsu, Japan | 466 (351 female, 115 male) | December 2011–March 2012 | Depression (CES-D) | Relational satisfaction from both providing and receiving social support buffers against depression. |
| Maeda et al. (2016) [49] | Fukushima public employees working in two coastal towns that were initially evacuated | 168 (92 from Town A where evacuation restrictions were lifted several months after the accident, 76 from Town B where evacuation orders remained at time of study) | March–October 2013 | Depression, PTSD, and suicide risk (MINI) | 17.9% of public employees met criteria for depression, and 4.8% met criteria for PTSD. 8.9% screened positive for suicide risk. |
| Murakami et al. (2017) [14] | Residents of Marumori Town, Japan | 174 | March 2015 | Radiation anxiety, perceptions of radiation risk, well-being | Higher evaluation of the town’s decontamination efforts was associated with a reduction in radiation anxiety. |
| Murakami, Hirosaki et al. (2018) [50] | Fukushima evacuees | 34.312 | 2011–2012 | Frequency of laughter, mental health distress (K6), radiation anxiety | Laughing more frequently was associated with lower radiation anxiety in the absence of mental health distress, but not in the presence of mental health distress. |
| Murakami, Takebayashi et al. (2018) [51] | Fukushimaresidents | 1023 | August 2016 | Radiation anxiety, well-being | Certain radiation countermeasures were associated with lower well-being (thyroid exam, food inspection, explanatory meetings), but the basic survey was associated with greater well-being. The thyroid exam is associated with less radiation anxiety. |
| Nagamine et al. (2018) [52] | Japan Ground Self-Defense Force personnel deployed to the Great East Japan Earthquake | 56,753 | 1, 6, and 12 months post-mission completion of deployment | PTSS (IES-R), psychological distress (K10) | Duties with radiation exposure risk were not associated with PTSS or psychological distress. |
| Nakayama et al. (2019) [15] | Fukushima residents | 868 | August 2016 | Radiation anxiety | Radiation anxiety was higher for people who utilized internet sources for information about the nuclear disaster and lower for people who utilized local broadcast TV. Radiation anxiety was lower for people who trusted government sources of information and higher for people who trusted citizen groups. |
| Oe, Fujii et al. (2016) [53] | Fukushima residents living in evacuation zones | 169,175 (71,100 in January 2012, 53,162 in January 2013, 44,913 in February 2014) | January 2012, January 2013, February 2014 | Psychological distress (K6), PTSS (PCL) | Prevalence of PTSS for men was 18.6% in 2012, 16.3% in 2013, and 15.0% in 2013. Prevalence of PTSS for women was 24.9% in 2012, 19.9% in 2013, and 18.1% in 2014. |
| Oe, Maeda et al. (2016) [54] | Fukushima residents living in areas that were considered complete evacuation zones for three years after the disaster | 12,371 | 2011, 2012, 2013 | Psychological distress (K6), radiation risk perception | Higher psychological distress was associated with greater radiation risk perception and poor social support. |
| Oe et al. (2017) [55] | Fukushima residents living in areas that were considered complete evacuation zones for three years after the disaster | 12,371 | 2011, 2012, 2013 | PTSS (PCL), radiation risk perception | Four trajectories of PTSS were demonstrated: PTSS trajectories: chronic (8.1%), resistant (54.9%), recovered (19.3%), and non-recovered (17.7%). |
| Orui et al. (2020) [16] | Fukushima residents | 225 (156 forced evacuees, 69 voluntary evacuees) | August–October 2016 | Radiation anxiety | Use of public relations information from local government was associated with lower anxiety for forced evacuees, but not voluntary evacuees. |
| Orui et al. (2018) [56] | Vital statistics from the Ministry of Health, Labour, and Welfare on suicide rates in Japan during the study period | n/a | March 2009–December 2015 | Monthly suicide rate | Male suicide rates in evacuation areas increased immediately after the nuclear disaster, then increased again four years after the disaster. Overall, suicide rates decreased for males 50–69 years, but increased for males younger than 30 and 70 and older. Female suicide rates declined during the first year and then increased over the next three years. |
| Rubin et al. (2012) [57] | British nationals in Japan | 284 | December 2011 | Psychological distress (GHQ-12), anger (STAXI-2), anxiety (STAI) | 16% reported psychological distress, 29.7% reported anxiety, and 30.4% reported anger. Utilizing low credibility sources was associated with greater distress, anger, and anxiety. |
| Shigemura et al. (2018) [58] | Male dentists who conducted disaster victim identification (DVI) in Fukushima after the 2011 disaster | 49 | September-December 2011 | Psychological distress (GHQ-12), PTSS (IES-R) | Greater psychological distress was associated with younger age and property loss. PTSS was associated with extensive property loss. |
| Shigemura et al. (2014) [59] | Fukushima nuclear power plant workers at TEPCO Daiichi (affected reactor) and Daini (intact reactor) | 1411 (831 from Daiichi, 580 from Daini) | May–June 2011 | PTSS (IES-R) | For both plants, PTSS was highly associated with peritraumatic distress. Experiencing discrimination and the presence of a pre-existing illness were also associated with PTSS. |
| Shigemura et al. (2020) [10] | Systematic review of studies on the psychological consequences of the Fukushima disaster | 79 studies | August 2019 | Psychological distress, PTSS, anxiety | Rates of psychological distress ranged from 8.3 to 65.1%. Rates of depressive symptoms ranged from 12 to 52.0%. Rates of PTSS ranged from 10.5 to 62.6%. |
| Sugimoto et al. (2013) [17] | Fukushima residents | 969 | June–July 2011 | Radiation anxiety | Utilizing rumours as a source of information about the disaster increased radiation anxiety. Attending a seminar on radiation reduced radiation anxiety. |
| Takebayashi et al. (2017) [12] | Systematic review of studies on risk perception and anxiety regarding radiation among people living in Japan after the 2011 Fukushima nuclear disaster | 24 studies | May 2017 | Radiation anxiety | Radiation anxiety is associated with demographics, disaster-related stressors, trusted information, and radiation-related stressors. |
| Tanisho et al. (2016) [60] | Fukushima nuclear power plant workers at TEPCO Daiichi (affected reactor) and Daini (intact reactor) | 968 (571 from Daiichi, 397 from Daini) | May–June 2011, May–June 2012 | Psychological distress (K6), PTSS (IES-R) | Experiencing discrimination at time one predicted higher psychological distress and PTSS at time two. Higher PTSS at time one predicted higher PTSS at time two. PTSS was associated with older age. |
| Terayama et al. (2020) [11] | Systematic review of studies on the emotional and behavioural consequences of the 2011 Fukushima nuclear disaster | 61 studies | August 2019 | Emotional and behavioural consequences of the Fukushima nuclear disaster | Radiation risk perception was associated with immediate health effects and fear of future health effects. Survivors of nuclear disasters experience lower well-being, greater discrimination, and have an increased rate of suicide. |
| Tsubokura et al. (2014) [61] | Fukushima residents of Iitate village and Soma city who underwent annual health evaluations in the year before and the year after the disaster | 564 | May 2011 | Depressive symptoms (PHQ-9) | 12% of participants met criteria for depression. |
| Tsujiuchi et al. (2016) [62] | Fukushima evacuees living in Saitama prefecture | 350 | March–April 2012 | PTSS (IES-R) | 59.4% of participants had symptoms consistent with a diagnosis of PTSD. Predictors of PTSD included chronic physical and mental illness, lost jobs, and limited social support. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Longmuir, C.; Agyapong, V.I.O. Social and Mental Health Impact of Nuclear Disaster in Survivors: A Narrative Review. Behav. Sci. 2021, 11, 113. https://doi.org/10.3390/bs11080113
Longmuir C, Agyapong VIO. Social and Mental Health Impact of Nuclear Disaster in Survivors: A Narrative Review. Behavioral Sciences. 2021; 11(8):113. https://doi.org/10.3390/bs11080113
Chicago/Turabian StyleLongmuir, Caley, and Vincent I. O. Agyapong. 2021. "Social and Mental Health Impact of Nuclear Disaster in Survivors: A Narrative Review" Behavioral Sciences 11, no. 8: 113. https://doi.org/10.3390/bs11080113
APA StyleLongmuir, C., & Agyapong, V. I. O. (2021). Social and Mental Health Impact of Nuclear Disaster in Survivors: A Narrative Review. Behavioral Sciences, 11(8), 113. https://doi.org/10.3390/bs11080113