
Men’s Psychotherapy Use, Male Role Norms, and Male-Typical Depression Symptoms: Examining 716 Men and Women Experiencing Psychological Distress

 ,
, 
 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
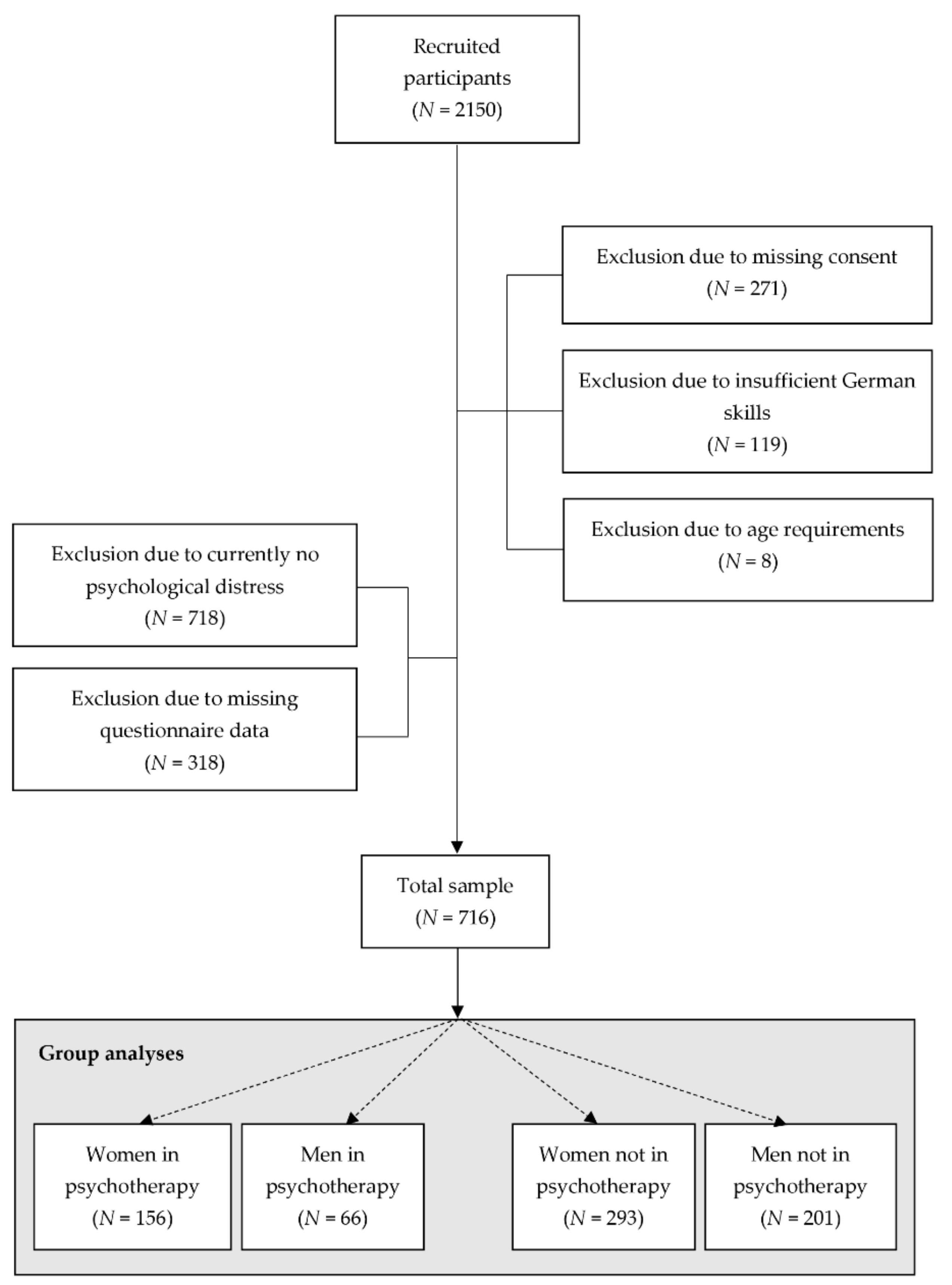
2.1. Procedure and Sample
2.2. Instruments
2.2.1. Sociodemographics, Self-Reported Psychological Distress and Psychotherapy Use
2.2.2. Patient Health Questionnaire-9
2.2.3. Male Depression Risk Scale-22
2.2.4. Generalized Anxiety Disorder-7
2.2.5. Bem Sex-Role Inventory
2.2.6. Male Role Norms Scale
2.3. Statistical Analysis
3. Results
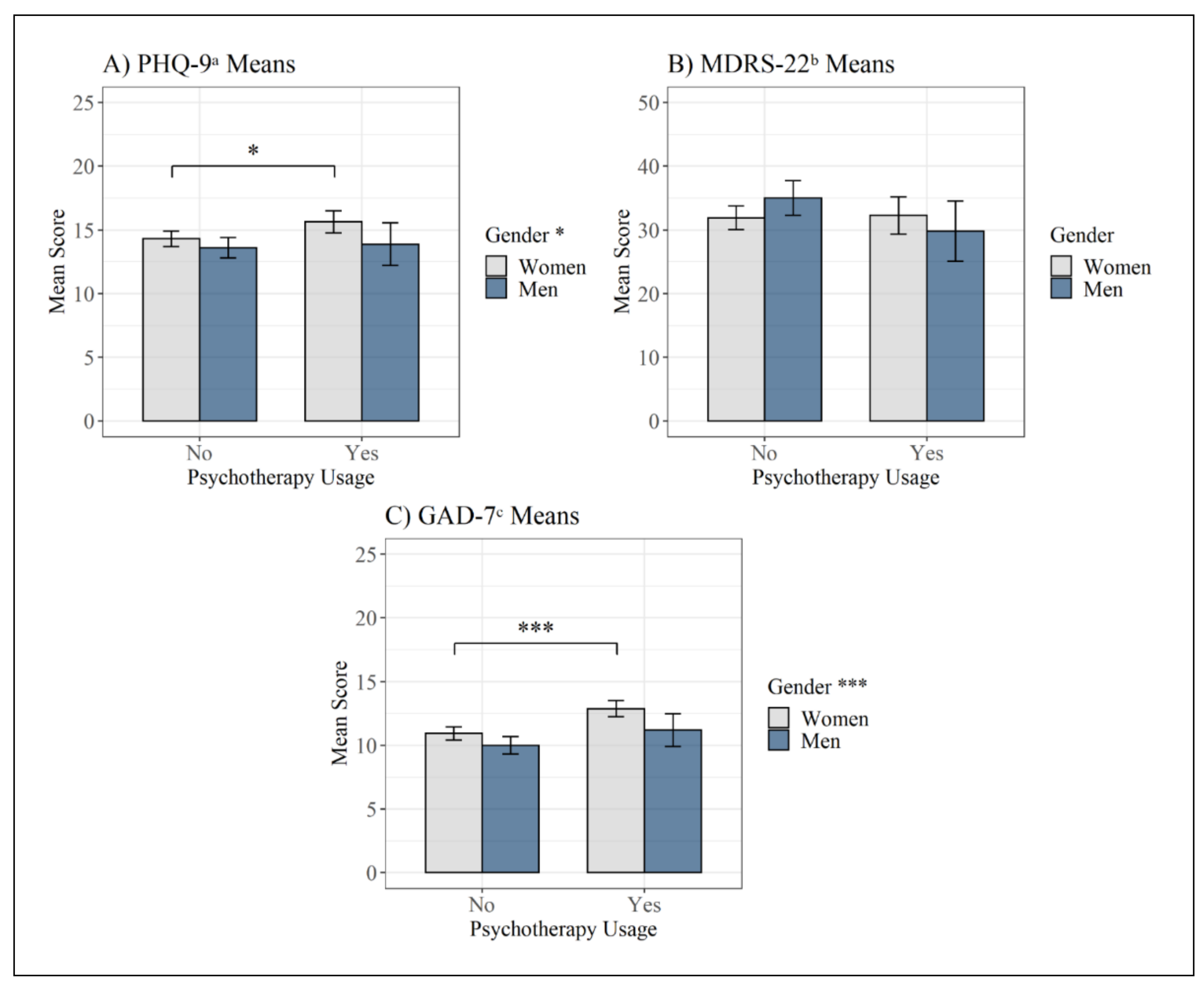
3.1. Descriptive Statistics and Group Differences in Mental Health Symptoms
3.2. Correlation Analysis Separated by Gender
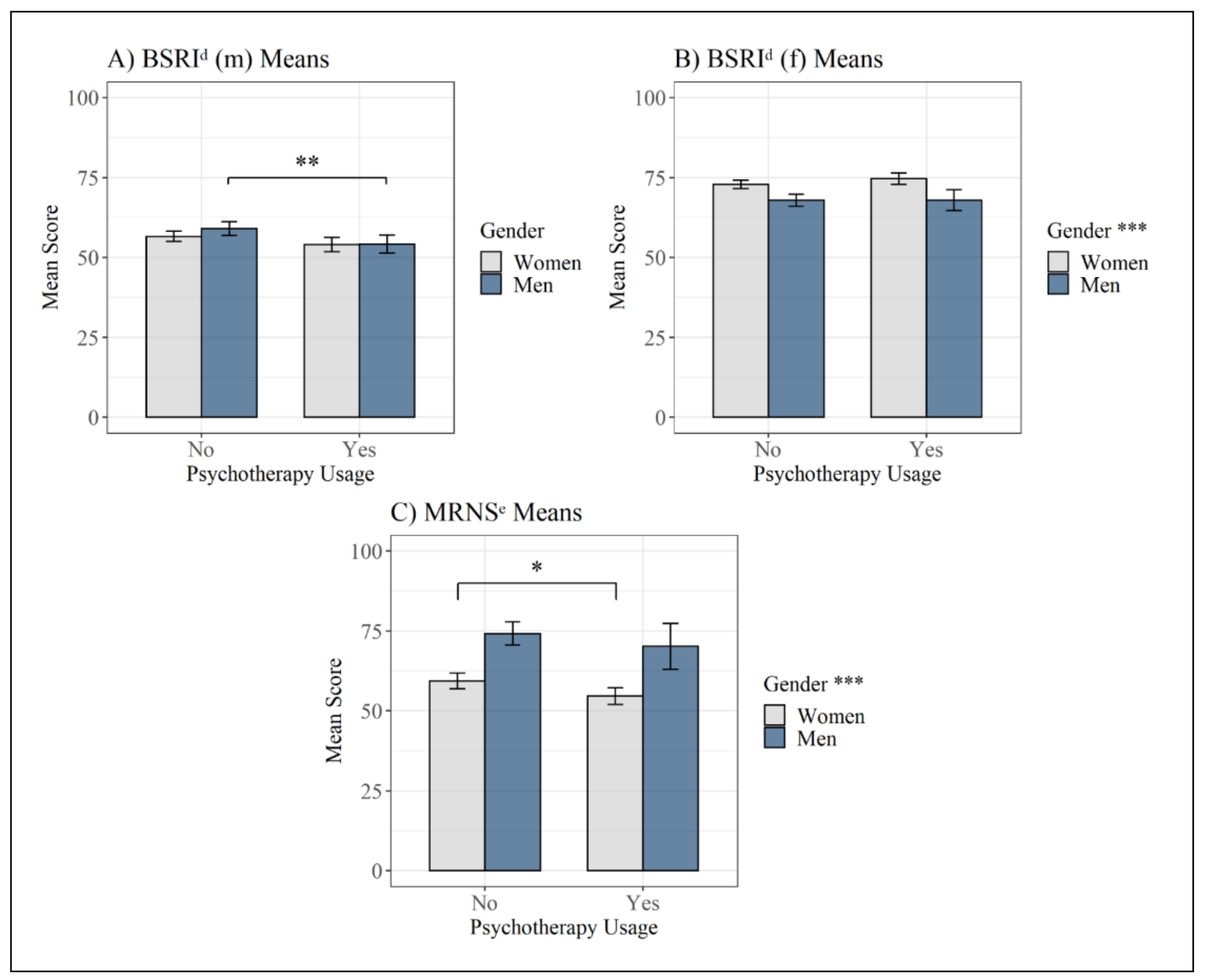
3.3. Group Comparisons Regarding Psychotherapy Use and Gender Roles
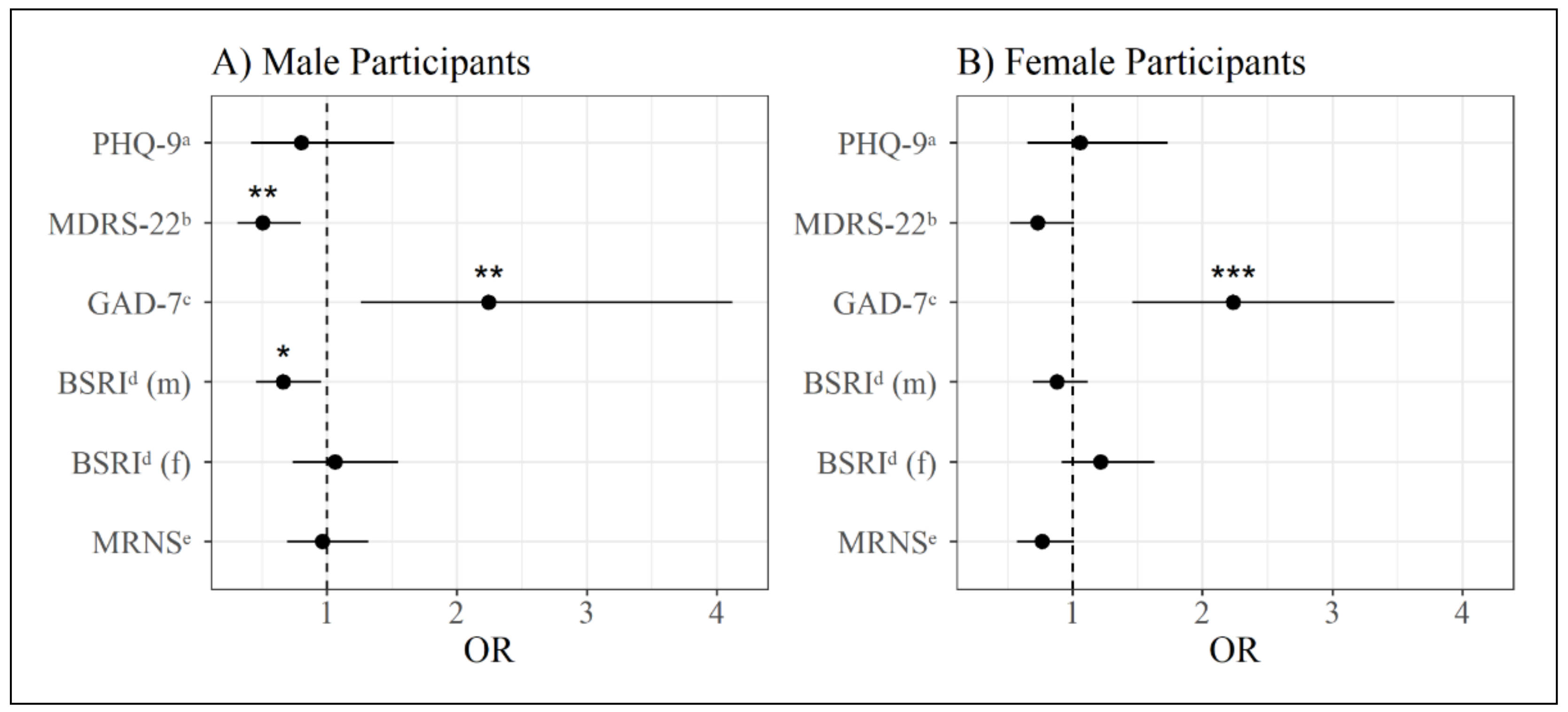
3.4. Binary Logistic Regression Analysis for the Prediction of Psychotherapy Use
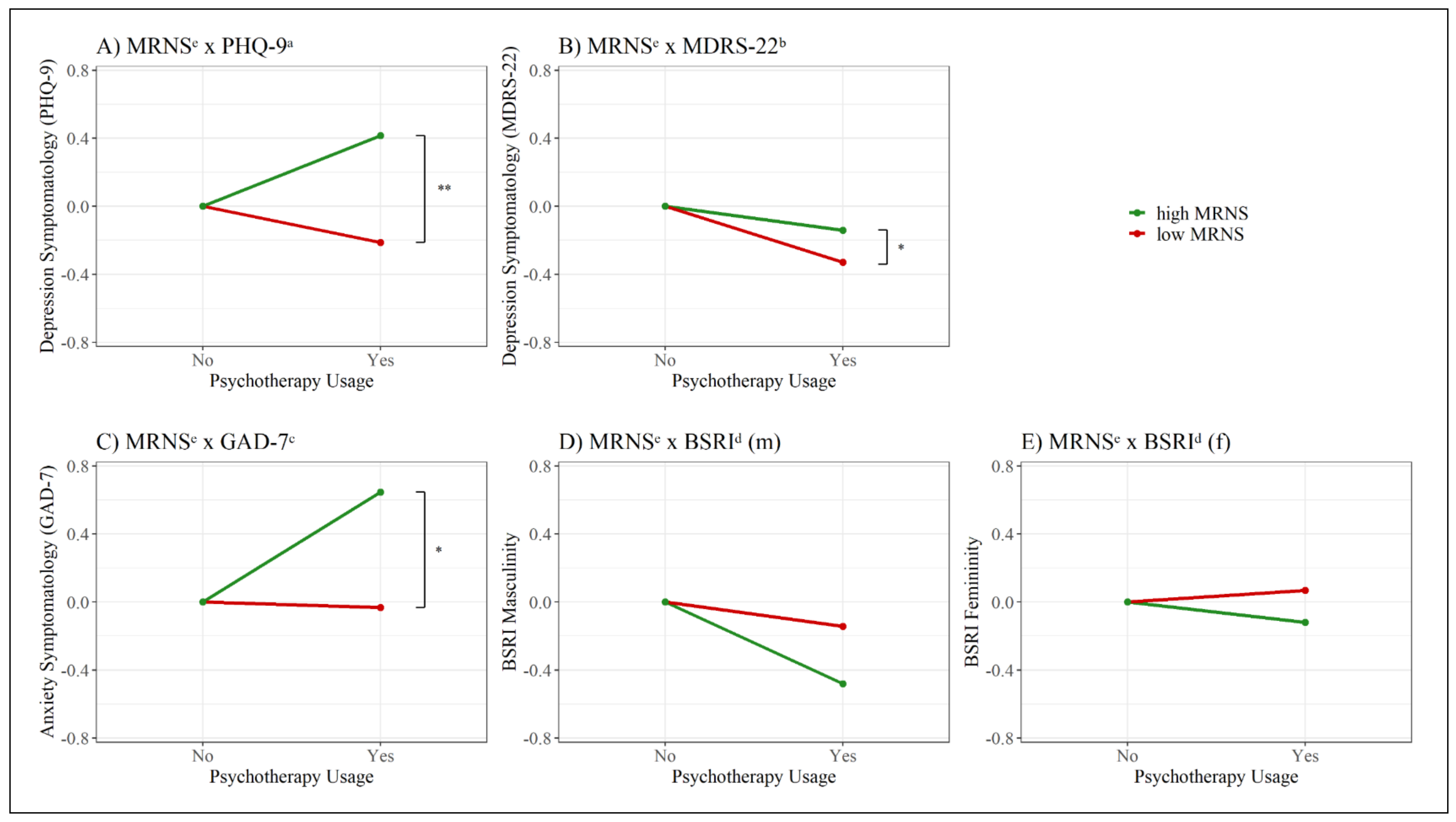
3.5. Interaction Analysis Examining Indirect Relations between Adherence to Traditional Male Role Norms and Psychotherapy Use
4. Discussion
4.1. Summary of Results
4.2. Integration of Findings
4.3. Limitations
4.4. Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Seidler, Z.E.; Dawes, A.J.; Rice, S.M.; Oliffe, J.L.; Dhillon, H.M. The role of masculinity in men’s help-seeking for depression: A systematic review. Clin. Psychol. Rev. 2016, 49, 106–118. [Google Scholar] [CrossRef] [PubMed]
- Walther, A.; Seidler, Z.E. Männliche Formen der Depression und deren Behandlung. PiD Psychother. Dialog. 2020, 21, 40–45. [Google Scholar] [CrossRef]
- Rommel, A.; Bretschneider, J.; Kroll, L.; Prütz, F.; Thom, J. Inanspruchnahme psychiatrischer und psychotherapeutischer Leistungen. Individuelle Determinanten und regionale Unterschiede. PPmP Psychother. Psychosom. Med. Psychol. 2018, 68, e31. [Google Scholar] [CrossRef]
- Larisch, A.; Heuft, G.; Engbrink, S.; Brähler, E.; Herzog, W.; Kruse, J. Behandlung psychischer und psychosomatischer Beschwerden—Inanspruchnahme, Erwartungen und Kenntnisse der Allgemeinbevölkerung in Deutschland. Z. Psychosom. Med. Psychother. 2013, 59, 153–169. [Google Scholar] [CrossRef] [PubMed]
- Strauss, B.; Hartung, J.; Kächele, H. Geschlechterspezifische Inanspruchnahme von Psychotherapie und Sozialer Arbeit. In Geschlecht, Gesundheit und Krankheit; Hurrelmann, K., Kolip, P., Eds.; Hogrefe: Göttingen, Germany, 2002; pp. 533–547. Available online: https://www.researchgate.net/profile/Horst_Kaechele/publication/215984847_Geschlechtsspezifische_Inanspruchnahme_von_Psychotherapie_und_Sozialer_Arbeit/links/554912a00cf205bce7ac0143/Geschlechtsspezifische-Inanspruchnahme-von-Psychotherapie-und-Sozialer-Arbeit.pdf (accessed on 10 February 2021).
- Harris, M.G.; Diminic, S.; Reavley, N.; Baxter, A.; Pirkis, J.; A Whiteford, H. Males’ mental health disadvantage: An estimation of gender-specific changes in service utilisation for mental and substance use disorders in Australia. Aust. N. Z. J. Psychiatry 2015, 49, 821–832. [Google Scholar] [CrossRef]
- Brandstetter, S.; Dodoo-Schittko, F.; Speerforck, S.; Apfelbacher, C.; Grabe, H.-J.; Jacobi, F.; Hapke, U.; Schomerus, G.; Baumeister, S.E. Trends in non-help-seeking for mental disorders in Germany between 1997–1999 and 2009–2012: A repeated cross-sectional study. Soc. Psychiatry Psychiatr. Epidemio. 2017, 52, 1005–1013. [Google Scholar] [CrossRef] [PubMed]
- Hasin, D.S.; Sarvet, A.L.; Meyers, J.L.; Saha, T.D.; Ruan, W.J.; Stohl, M.; Grant, B.F. Epidemiology of Adult DSM-5 Major Depressive Disorder and Its Specifiers in the United States. JAMA Psychiatry 2018, 75, 336–346. [Google Scholar] [CrossRef]
- Salk, R.H.; Hyde, J.S.; Abramson, L.Y. Gender differences in depression in representative national samples: Meta-analyses of diagnoses and symptoms. Psychol. Bull. 2017, 143, 783–822. [Google Scholar] [CrossRef] [PubMed]
- Bandelow, B.; Michaelis, S. Epidemiology of anxiety disorders in the 21st century. Dialog Clin. Neurosci. 2015, 17, 327–335. [Google Scholar] [CrossRef]
- Altemus, M.; Sarvaiya, N.; Epperson, C.N. Sex differences in anxiety and depression clinical perspectives. Front. Neuroendocr. 2014, 35, 320–330. [Google Scholar] [CrossRef]
- Fiacco, S.; Walther, A.; Ehlert, U. Steroid secretion in healthy aging. Psychoneuroendocrinology 2019, 105, 64–78. [Google Scholar] [CrossRef]
- Schiller, C.; Johnson, S.L.; Abate, A.C.; Schmidt, P.J.; Rubinow, D.R. Reproductive Steroid Regulation of Mood and Behavior. Compr. Physiol. 2016, 6, 1135–1160. [Google Scholar] [CrossRef] [PubMed]
- Walther, A.; Wasielewska, J.M.; Leiter, O. The antidepressant effect of testosterone: An effect of neuroplasticity? Neurol. Psychiatry Brain Res. 2019, 32, 104–110. [Google Scholar] [CrossRef]
- Walther, A.; Rice, T.; Kufert, Y.; Ehlert, U. Neuroendocrinology of a Male-Specific Pattern for Depression Linked to Alcohol Use Disorder and Suicidal Behavior. Front. Psychiatry 2017, 7, 206. [Google Scholar] [CrossRef]
- Martin, L.A.; Neighbors, H.W.; Griffith, D. The Experience of Symptoms of Depression in Men vs Women. JAMA Psychiatry 2013, 70, 1100–1106. [Google Scholar] [CrossRef] [PubMed]
- Cavanagh, A.; Wilson, C.J.; Kavanagh, D.J.; Caputi, P. Differences in the Expression of Symptoms in Men Versus Women with Depression: A Systematic Review and Meta-analysis. Harv. Rev. Psychiatry 2017, 25, 29–38. [Google Scholar] [CrossRef]
- Walther, A.; Grub, J.; Ehlert, U.; Wehrli, S.; Rice, S.; Seidler, Z.; Debelak, R. Male depression risk, psychological distress, and psychotherapy uptake: Validation of the German version of the male depression risk scale. J. Affect. Disord. Rep. 2021, 4, 100107. [Google Scholar] [CrossRef]
- Rutz, W.; Wålinder, J.; Von Knorring, L.; Rihmer, Z.; Pihlgren, H. Prevention of depression and suicide by education and medication: Impact on male suicidality. An update from the Gotland study. Int. J. Psychiatry Clin. Pr. 1997, 1, 39–46. [Google Scholar] [CrossRef]
- Rice, S.M.; Oliffe, J.L.; Kelly, M.T.; Cormie, P.; Chambers, S.; Ogrodniczuk, J.S.; Kealy, D. Depression and Prostate Cancer: Examining Comorbidity and Male-Specific Symptoms. Am. J. Mens Health 2018, 12, 1864–1872. [Google Scholar] [CrossRef] [PubMed]
- Zajac, I.T.; Rice, S.; Proeve, M.; Kealy, D.; Oliffe, J.L.; Ogrodniczuk, J.S. Suicide risk, psychological distress and treatment preferences in men presenting with prototypical, externalising and mixed depressive symptomology. J. Ment. Health 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Fields, A.J.; Cochran, S.V. Men and Depression: Current Perspectives for Health Care Professionals. Am. J. Lifestyle Med. 2010, 5, 92–100. [Google Scholar] [CrossRef]
- O’Neil, J.M. Gender Role Conflict Research 30 Years Later: An Evidence-Based Diagnostic Schema to Assess Boys and Men in Counseling. J. Couns. Dev. 2013, 91, 490–498. [Google Scholar] [CrossRef]
- Rutz, W. Preventing suicide and premature death by education and treatment. J. Affect. Disord. 2001, 62, 123–129. [Google Scholar] [CrossRef]
- Rochlen, A.B.; Paterniti, D.A.; Epstein, R.M.; Duberstein, P.; Willeford, L.; Kravitz, R.L. Barriers in Diagnosing and Treating Men With Depression: A Focus Group Report. Am. J. Men’s Health 2010, 4, 167–175. [Google Scholar] [CrossRef]
- Addis, M.E.; Mahalik, J.R. Men, masculinity, and the contexts of help seeking. Am. Psychol. 2003, 58, 5–14. [Google Scholar] [CrossRef]
- Courtenay, W.H. Constructions of masculinity and their influence on men’s well-being: A theory of gender and health. Soc. Sci. Med. 2000, 50, 1385–1401. [Google Scholar] [CrossRef]
- Pleck, J.H. The gender role strain paradigm: An update. In A new Psychology of Men; Levant, F.R., Pollack, S.W., Eds.; Basic Books/Hachette Book Group: New York, NY, USA, 1995; pp. 11–32. [Google Scholar]
- Thomas, R.M. Recent Theories of Human Development; SAGE Publications: SAGE Business Cases Originals:: Thousand Oaks, CA, USA, 2001. [Google Scholar]
- Long, V.O. Relationship of masculinity to self-esteem and self-acceptance in female professionals, college students, clients, and victims of domestic violence. J. Consult. Clin. Psychol. 1986, 54, 323–327. [Google Scholar] [CrossRef]
- O’Heron, C.A.; Orlofsky, J.L. Stereotypic and nonstereotypic sex role trait and behavior orientations, gender identity, and psychological adjustment. J. Pers. Soc. Psychol. 1990, 58, 134–143. [Google Scholar] [CrossRef]
- Johnson, W.; McCoy, N. Self-Confidence, Self-Esteem, and Assumption of Sex Role in Young Men and Women. Percept. Mot. Ski. 2000, 90, 751–756. [Google Scholar] [CrossRef] [PubMed]
- McCusker, M.G.; Galupo, M.P. The impact of men seeking help for depression on perceptions of masculine and feminine characteristics. Psychol. Men Masc. 2011, 12, 275–284. [Google Scholar] [CrossRef]
- Pleck, J.H. The Myth of Masculinity; Vol. second printing; Massachusetts Institute of Technology: Cambridge, MA, USA, 1982. [Google Scholar]
- Thompson, E.H.; Pleck, J.H. The Structure of Male Role Norms. Am. Behav. Sci. 1986, 29, 531–543. [Google Scholar] [CrossRef]
- Levant, R.F. The new psychology of men. Prof. Psychol. Res. Pr. 1996, 27, 259–265. [Google Scholar] [CrossRef]
- Wong, Y.J.; Ho, M.-H.R.; Wang, S.-Y.; Miller, I.S.K. Meta-analyses of the relationship between conformity to masculine norms and mental health-related outcomes. J. Couns. Psychol. 2017, 64, 80–93. [Google Scholar] [CrossRef] [PubMed]
- Yousaf, O.; Popat, A.; Hunter, M.S. An investigation of masculinity attitudes, gender, and attitudes toward psychological help-seeking. Psychol. Men Masc. 2015, 16, 234–237. [Google Scholar] [CrossRef]
- Levant, R.F.; Hirsch, L.S.; Celentano, E.; Cozza, T.M.; Hill, S.; MacEachern, M.; Marty, N.; Schnedeker, J. Male Role Norms Inventory. PsycTESTS Dataset 1992, 9, 179. [Google Scholar] [CrossRef]
- Smith, J.P.; Tran, G.Q.; Thompson, R.D. Can the theory of planned behavior help explain men’s psychological help-seeking? Evidence for a mediation effect and clinical implications. Psychol. Men Masc. 2008, 9, 179. [Google Scholar] [CrossRef]
- Berger, J.L.; Addis, M.E.; Green, J.D.; Mackowiak, C.; Goldberg, V. Men’s reactions to mental health labels, forms of help-seeking, and sources of help-seeking advice. Psychol. Men Masc. 2013, 14, 433–443. [Google Scholar] [CrossRef]
- Sileo, K.M.; Kershaw, T.S. Dimensions of Masculine Norms, Depression, and Mental Health Service Utilization: Results From a Prospective Cohort Study Among Emerging Adult Men in the United States. Am. J. Mens Health 2020, 14. [Google Scholar] [CrossRef] [PubMed]
- Rice, S.M.; Fallon, B.J.; Aucote, H.M.; Möller-Leimkühler, A.M. Development and preliminary validation of the male depression risk scale: Furthering the assessment of depression in men. J. Affect. Disord. 2013, 151, 950–958. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, S.; Zepf, S. Effectiveness of Psychotherapy in Germany: A Replication of the Consumer Report Study. Psychother. Res. 2003, 13, 235–242. [Google Scholar] [CrossRef]
- Rice, S.M.; Oliffe, J.L.; Kealy, D.; Ogrodniczuk, J.S. Male depression subtypes and suicidality: Latent profile analysis of internalizing and externalizing symptoms in a representative Canadian sample. J. Nerv. Mental Dis. 2018, 206, 169–172. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 2006. [Google Scholar]
- Levis, B.; Benedetti, A.; Ioannidis, J.P.; Sun, Y.; Negeri, Z.; He, C.; Wu, Y.; Krishnan, A.; Bhandari, P.M.; Neupane, D.; et al. Patient Health Questionnaire-9 scores do not accurately estimate depression prevalence: Individual participant data meta-analysis. J. Clin. Epidemiol. 2020, 122, 115–128. [Google Scholar] [CrossRef]
- Martin, A.; Rief, W.; Klaiberg, A.; Braehler, E. Validity of the Brief Patient Health Questionnaire Mood Scale (PHQ-9) in the general population. Gen. Hosp. Psychiatry 2006, 28, 71–77. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Löwe, B.; Decker, O.; Müller, S.; Brähler, E.; Schellberg, D.; Herzog, W.; Herzberg, P.Y. Validation and Standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the General Population. Med. Care 2008, 46, 266–274. [Google Scholar] [CrossRef]
- Hinz, A.; Klein, A.M.; Brähler, E.; Glaesmer, H.; Luck, T.; Riedel-Heller, S.G.; Wirkner, K.; Hilbert, A. Psychometric evaluation of the Generalized Anxiety Disorder Screener GAD-7, based on a large German general population sample. J. Affect. Disord. 2017, 210, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Bem, S.L. The measurement of psychological androgyny. J. Consult. Clin. Psychol. 1974, 42, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Troche, S.J.; Rammsayer, T.H. Eine Revision des deutschsprachigen Bem Sex-Role Inventory. Klin. Diagn. Eval. 2011, 4, 262–283. Available online: https://www.researchgate.net/profile/Stefan_Troche/publication/316842202_Eine_Revision_des_deutschsprachigen_Bem_Sex-Role_Inventory/links/5913358fa6fdcc963e7ed77e/Eine-Revision-des-deutschsprachigen-Bem-Sex-Role-Inventory.pdf (accessed on 23 March 2020).
- Bem, S.L. Bem Sex Role Inventory. PsycTESTS Dataset 2011. [Google Scholar] [CrossRef]
- Sinn, J.S. The Predictive and Discriminant Validity of Masculinity Ideology. J. Res. Pers. 1997, 31, 117–135. [Google Scholar] [CrossRef]
- Revelle, W. Psych: Procedures for Personality and Psychological Research (2.1.3); Northwestern University: Evanston, IL, USA, 2020; Available online: https://cran.r-project.org/package=psych (accessed on 5 May 2021).
- Mangiafico, S. Rcompanion: Functions to Support Extension Education Program Evaluation (2.4.0). 2021. Available online: https://CRAN.R-project.org/package=rcompanion (accessed on 5 May 2021).
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016; Available online: https://ggplot2.tidyverse.org (accessed on 10 September 2020).
- Zimmerman, D.W.; Zumbo, B.D. Rank transformations and the power of the Student t test and Welch t’ test for non-normal populations with unequal variances. Can. J. Exp. Psychol. 1993, 47, 523–539. [Google Scholar] [CrossRef]
- Parent, M.C.; Moradi, B.; Rummell, C.M.; Tokar, D.M. Evidence of construct distinctiveness for conformity to masculine norms. Psychol. Men Masc. 2011, 12, 354–367. [Google Scholar] [CrossRef]
- Levant, R.F.; Richmond, K. The gender role strain paradigm and masculinity ideologies. In APA Handbook of Men and Masculinities; American Psychological Association (APA): Washington, DC, USA, 2016; pp. 23–49. [Google Scholar]
- Coleman, D.; Feigelman, W.; Rosen, Z. Association of High Traditional Masculinity and Risk of Suicide Death. JAMA Psychiatry 2020, 77, 435. [Google Scholar] [CrossRef]
- Cramer, K.M. Psychological antecedents to help-seeking behavior: A reanalysis using path modeling structures. J. Couns. Psychol. 1999, 46, 381–387. [Google Scholar] [CrossRef]
- Gulliver, A.; Griffiths, K.M.; Christensen, H.; Brewer, J.L. A systematic review of help-seeking interventions for depression, anxiety and general psychological distress. BMC Psychiatry 2012, 12, 81. [Google Scholar] [CrossRef] [PubMed]
- Levant, R.F.; Wimer, D.J.; Williams, C.M.; Smalley, K.B.; Noronha, D. The Relationships between Masculinity Variables, Health Risk Behaviors and Attitudes toward Seeking Psychological Help. Int. J. Mens Health 2009, 8, 3–21. [Google Scholar] [CrossRef]
- Kelleher, C. Minority stress and health: Implications for lesbian, gay, bisexual, transgender, and questioning (LGBTQ) young people. Couns. Psychol. Q. 2009, 22, 373–379. [Google Scholar] [CrossRef]
- Timmins, L.E.; Rimes, K.A.; Rahman, Q. Minority stressors and psychological distress in transgender individuals. Psychol. Sex. Orientat. Gend. Divers. 2017, 4, 328–340. [Google Scholar] [CrossRef]
- McDermott, R.C.; Wolfe, G.; Levant, R.F.; Alshabani, N.; Richmond, K. Measurement invariance of three gender ideology scales across cis, trans, and nonbinary gender identities. Psychol. Men Masc. 2021, 22, 331–344. [Google Scholar] [CrossRef]
- O’Neil, J.M.; Helms, B.J.; Gable, R.K.; David, L.; Wrightsman, L.S. Gender-role conflict scale: College men’s fear of femininity. Sex Roles 1986, 14, 335–350. [Google Scholar] [CrossRef]
- Komlenac, N.; Siller, H.; Bliem, H.R.; Hochleitner, M. Validation of the Internal Structure of a German-Language Version of the Gender Role Conflict Scale—Short Form. Front. Psychol. 2018, 9, 1161. [Google Scholar] [CrossRef]
- Liddon, L.; Kingerlee, R.; Barry, J.A. Gender differences in preferences for psychological treatment, coping strategies, and triggers to help-seeking. Br. J. Clin. Psychol. 2017, 57, 42–58. [Google Scholar] [CrossRef] [PubMed]
- Swift, J.K.; Callahan, J.L.; Ivanovic, M.; Kominiak, N. Further examination of the psychotherapy preference effect: A meta-regression analysis. J. Psychother. Integr. 2013, 23, 134–145. [Google Scholar] [CrossRef]
- Vogel, D.L.; Wade, N.G.; Haake, S. Measuring the self-stigma associated with seeking psychological help. J. Couns. Psychol. 2006, 53, 325–337. [Google Scholar] [CrossRef]
- Eisenberg, D.; Downs, M.F.; Golberstein, E.; Zivin, K. Stigma and Help Seeking for Mental Health among College Students. Med. Care Res. Rev. 2009, 66, 522–541. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total (N = 716) | In PT (N = 222) | Not in PT (N = 494) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| N (%) | M (SD) | N (%) | M (SD) | N (%) | M (SD) | t (df) | χ2 (df) | p | |
| Age | 32.7 (12.2) | 31.9 (11.7) | 33.1 (12.4) | −1.25 (449.71) | 0.212 | ||||
| Gender | 7.40 (1) | 0.006 ** | |||||||
| Men | 267 (37.3) | 66 (29.7) | 201 (40.7) | ||||||
| Women | 449 (62.7) | 156 (70.3) | 293 (59.3) | ||||||
| Education | 6.20 (3) | 0.102 | |||||||
| None completed | 7 (1.0) | 5 (2.3) | 2 (0.4) | 3.66 (1) | 0.033 * | ||||
| Secondary education | 389 (54.3) | 115 (51.8) | 274 (55.5) | 0.69 (1) | 0.407 | ||||
| Tertiary education | 287 (40.1) | 93 (41.9) | 194 (39.3) | 0.34 (1) | 0.562 | ||||
| Other | 33 (4.6) | 11 (5.0) | 16 (3.2) | 0.08 (1) | 0.778 | ||||
| Relationship status | 0.75 (2) | 0.686 | |||||||
| Single | 334 (46.6) | 101 (45.5) | 233 (47.2) | 0.11 (1) | 0.739 | ||||
| In a relationship | 327 (45.7) | 106 (47.7) | 221 (44.7) | 0.44 (1) | 0.505 | ||||
| Single after a permanent relationship | 55 (7.7) | 15 (6.8) | 40 (8.1) | 0.22 (1) | 0.638 | ||||
| Sexual orientation | 4.33 (4) | 0.364 | |||||||
| Heterosexual-identified | 467 (65.2) | 135 (60.8) | 332 (67.2) | 2.49 (1) | 0.115 | ||||
| Gay/Lesbian-identified | 52 (7.3) | 20 (9.0) | 32 (6.5) | 1.11 (1) | 0.293 | ||||
| Bisexual-identified | 144 (20.1) | 49 (22.1) | 95 (19.2) | 0.60 (1) | 0.438 | ||||
| Asexual-identified | 26 (3.6) | 7 (3.2) | 19 (3.8) | 0.06 (1) | 0.808 | ||||
| Other | 27 (3.8) | 11 (5.0) | 16 (3.2) | 0.82 (1) | 0.367 | ||||
| PHQ-9 a | 14.4 (5.6) | 15.1 (5.9) | 14.0 (5.5) | 2.41 (714) | 0.016 * | ||||
| MDRS-22 b | 32.7 (18.1) | 31.5 (18.7) | 33.2 (17.8) | −1.12 (714) | 0.265 | ||||
| GAD-7 c | 11.1 (4.7) | 12.4 (4.7) | 10.5 (4.7) | 4.86 (714) | <0.001 *** | ||||
| BSRI d (m) | 56.6 (14.3) | 54.1 (13.5) | 57.6 (14.5) | −3.04 (714) | 0.002 ** | ||||
| BSRI d (f) | 71.4 (12.4) | 72.6 (12.1) | 70.8 (12.5) | 1.81 (714) | 0.070 | ||||
| MRNS e | 63.5 (24.0) | 59.2 (22.2) | 65.4 (24.5) | −3.17 (714) | 0.002 ** | ||||
| (A) Male participants | |||||||
| Variable | M | SE | PHQ-9 a | MDRS-22 b | GAD-7 c | BSRI d (m) | BSRI d (f) |
| PHQ-9 a | 13.7 | 6.0 | |||||
| MDRS-22 b | 33.7 | 19.7 | 0.55 *** | ||||
| GAD-7 c | 10.3 | 5.0 | 0.68 *** | 0.54 *** | |||
| BSRI d (m) | 57.8 | 14.7 | −0.37 *** | −0.17 * | −0.26 *** | ||
| BSRI d (f) | 67.9 | 13.3 | −0.12 | −0.16 * | −0.05 | 0.33 *** | |
| MRNS e | 73.2 | 26.7 | 0.07 | 0.28 *** | 0.11 | 0.13 | −0.21 ** |
| (B) Female participants | |||||||
| PHQ-9 a | 14.8 | 5.4 | |||||
| MDRS-22 b | 32.0 | 17.1 | 0.57 *** | ||||
| GAD-7 c | 11.6 | 4.5 | 0.64 *** | 0.47 *** | |||
| BSRI d (m) | 55.7 | 14.0 | −0.34 *** | −0.15 * | −0.25 *** | ||
| BSRI d (f) | 73.4 | 11.3 | −0.09 | −0.03 | 0.04 | 0.26 *** | |
| MRNS e | 57.7 | 20.1 | −0.04 | 0.06 | −0.04 | 0.04 | −0.13 * |
| No Interaction | MRNS x PHQ-9 | MRNS x MDRS-22 | MRNS x GAD-7 | MRNS x BSRI (m) | MRNS x BSRI (f) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Predictor | β (SE) | p | β (SE) | p | β (SE) | p | β (SE) | p | β (SE) | p | β (SE) | p |
| Intercept | 0.36 (1.14) | 0.750 | −1.62 (1.04) | 0.119 | −1.58 (1.02) | 0.122 | −1.24 (1.00) | 0.212 | −1.27 (0.99) | 0.198 | −1.33 (0.99) | 0.181 |
| PHQ-9 a | −0.22 (0.33) | 0.499 | −0.28 (0.22) | 0.198 | −0.11 (0.21) | 0.610 | −0.09 (0.21) | 0.685 | −0.15 (0.21) | 0.479 | −0.12 (0.21) | 0.556 |
| MDRS-22 b | −0.68 (0.24) | 0.005 ** | −0.59 (0.20) | 0.003 ** | −0.80 (0.22) | <0.001 *** | −0.54 (0.19) | 0.007 ** | −0.56 (0.20) | 0.005 ** | −0.58 (0.20) | 0.004 ** |
| GAD-7 c | 0.81 (0.30) | 0.007 ** | 0.96 (0.31) | 0.002 ** | 0.96 (0.32) | 0.002 ** | 0.67 (0.32) | 0.034 * | 0.79 (0.30) | 0.010 ** | 0.80 (0.30) | 0.008 ** |
| BSRI d (m) | −0.41 (0.19) | 0.029 * | −0.35 (0.20) | 0.077 | −0.39 (0.19) | 0.039 * | −0.35 (0.19) | 0.063 | −0.34 (0.19) | 0.082 | −0.42 (0.18) | 0.024 * |
| BSRI d (f) | 0.06 (0.19) | 0.743 | 0.05 (0.19) | 0.803 | 0.08 (0.19) | 0.681 | 0.08 (0.19) | 0.667 | 0.05 (0.19) | 0.795 | 0.12 (0.19) | 0.544 |
| MRNS e | −0.04 (0.16) | 0.818 | −0.08 (0.16) | 0.611 | −0.13 (0.16) | 0.413 | −0.11 (0.16) | 0.506 | 0.90 (0.55) | 0.102 | 1.01 (0.62) | 0.105 |
| Interaction | 0.52 (0.17) | 0.002 ** | 0.35 (0.14) | 0.011* | 0.35 (0.15) | 0.016 * | −0.26 (0.15) | 0.084 | −0.25 (0.15) | 0.087 | ||
| Omnibus statistics | ||||||||||||
| χ2 (df) | 20.20 (6) | 31.54 (7) | 27.61 (7) | 26.14 (7) | 23.42 (7) | 23.10 (7) | ||||||
| p (omnibus) | 0.003 ** | <0.001 *** | <0.001 *** | <0.001 *** | 0.001 ** | 0.002 ** | ||||||
| Pseudo R2 (Nagelkerke) | 0.108 | 0.165 | 0.146 | 0.139 | 0.125 | 0.123 | ||||||
| No Interaction | MRNS x PHQ-9 | MRNS x MDRS-22 | MRNS x GAD-7 | MRNS x BSRI (m) | MRNS x BSRI (f) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Predictor | β (SE) | p | β (SE) | p | β (SE) | p | β (SE) | p | β (SE) | p | β (SE) | p |
| Intercept | −2.56 (0.81) | 0.002** | −2.53 (0.81) | 0.002 ** | −2.59 (0.81) | 0.001 ** | −2.69 (0.83) | 0.001 ** | −2.40 (0.83) | 0.004 ** | −2.49 (0.83) | 0.003 ** |
| PHQ-9 a | 0.04 (0.16) | 0.817 | −0.01 (0.17) | 0.948 | 0.03 (0.16) | 0.833 | 0.04 (0.16) | 0.792 | 0.03 (0.16) | 0.868 | 0.04 (0.16) | 0.811 |
| MDRS-22 b | −0.26 (0.14) | 0.060 | −0.26 (0.14) | 0.061 | −0.33 (0.15) | 0.028* | −0.26 (0.14) | 0.063 | −0.25 (0.14) | 0.067 | −0.26 (0.14) | 0.064 |
| GAD-7 c | 0.81 (0.22) | <0.001 *** | 0.82 (0.22) | <0.001 *** | 0.81 (0.22) | <0.001 *** | 0.84 (0.23) | <0.001 *** | 0.80 (0.22) | <0.001 *** | 0.79 (0.22) | <0.001 *** |
| BSRI d (m) | −0.13 (0.12) | 0.286 | −0.14 (0.12) | 0.259 | −0.13 (0.12) | 0.276 | −0.13 (0.12) | 0.293 | −0.17 (0.13) | 0.184 | −0.13 (0.12) | 0.280 |
| BSRI d (f) | 0.19 (0.15) | 0.188 | 0.19 (0.15) | 0.196 | 0.20 (0.15) | 0.175 | 0.21 (0.15) | 0.163 | 0.20 (0.15) | 0.186 | 0.18 (0.15) | 0.217 |
| MRNS e | −0.25 (0.13) | 0.064 | −0.24 (0.14) | 0.081 | −0.25 (0.14) | 0.068 | −0.28 (0.14) | 0.049 * | 0.24 (0.53) | 0.652 | 0.04 (0.75) | 0.961 |
| Interaction | −0.13 (0.14) | 0.374 | −0.23 (0.16) | 0.153 | 0.11 (0.15) | 0.457 | −0.14 (0.14) | 0.347 | −0.06 (0.15) | 0.700 | ||
| Omnibus statistics | ||||||||||||
| χ2 (df) | 31.41 (6) | 32.21 (7) | 33.56 (7) | 31.97 (7) | 32.29 (7) | 31.55 (7) | ||||||
| p (omnibus) | <0.001 *** | <0.001 *** | <0.001 *** | <0.001 *** | <0.001 *** | <0.001 *** | ||||||
| pseudo R2 (Nagelkerke) | 0.093 | 0.095 | 0.099 | 0.095 | 0.096 | 0.094 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eggenberger, L.; Fordschmid, C.; Ludwig, C.; Weber, S.; Grub, J.; Komlenac, N.; Walther, A. Men’s Psychotherapy Use, Male Role Norms, and Male-Typical Depression Symptoms: Examining 716 Men and Women Experiencing Psychological Distress. Behav. Sci. 2021, 11, 83. https://doi.org/10.3390/bs11060083
Eggenberger L, Fordschmid C, Ludwig C, Weber S, Grub J, Komlenac N, Walther A. Men’s Psychotherapy Use, Male Role Norms, and Male-Typical Depression Symptoms: Examining 716 Men and Women Experiencing Psychological Distress. Behavioral Sciences. 2021; 11(6):83. https://doi.org/10.3390/bs11060083
Chicago/Turabian StyleEggenberger, Lukas, Callia Fordschmid, Claudio Ludwig, Seraina Weber, Jessica Grub, Nikola Komlenac, and Andreas Walther. 2021. "Men’s Psychotherapy Use, Male Role Norms, and Male-Typical Depression Symptoms: Examining 716 Men and Women Experiencing Psychological Distress" Behavioral Sciences 11, no. 6: 83. https://doi.org/10.3390/bs11060083
APA StyleEggenberger, L., Fordschmid, C., Ludwig, C., Weber, S., Grub, J., Komlenac, N., & Walther, A. (2021). Men’s Psychotherapy Use, Male Role Norms, and Male-Typical Depression Symptoms: Examining 716 Men and Women Experiencing Psychological Distress. Behavioral Sciences, 11(6), 83. https://doi.org/10.3390/bs11060083