Exploring Language Learning as a Potential Tool against Cognitive Impairment in Late-Life Depression: Two Meta-Analyses and Suggestions for Future Research

 ,
,  ,
,  , and
, and
Abstract
1. Introduction
2. Aims and Objectives
3. Methods
3.1. Inclusion and Exclusion Criteria
- Participants were ≥55 years old (Studies on LLD used various cut-off points for a minimum age of inclusion ranging from 45 [75] to 65 [76]. 55 was chosen as a middle ground that primarily identified studies where participants had a mean age of 65 or higher and resulted in more included studies to meet the current investigation’s aims)
- The study was published in English.
3.2. Search Strategies
3.3. Study Selection
3.4. Data Collection Process & Data Items
3.5. Risk of Bias in Individual Studies
3.6. Summary Measures & Synthesis of Results
4. Results
4.1. Study Selection
4.2. Summary of Study Characteristics Late-Life Depression
4.2.1. Demographic Information
4.2.2. Types of Tasks Used
4.2.3. Operationalization of Late-Life Depression
4.3. Study Characteristics of Studies on Bilingualism and Aging
4.3.1. Demographic Information
4.3.2. Type of Tasks Used
4.3.3. Operationalization of Bilingualism
4.4. Risk of Bias in Individual Studies
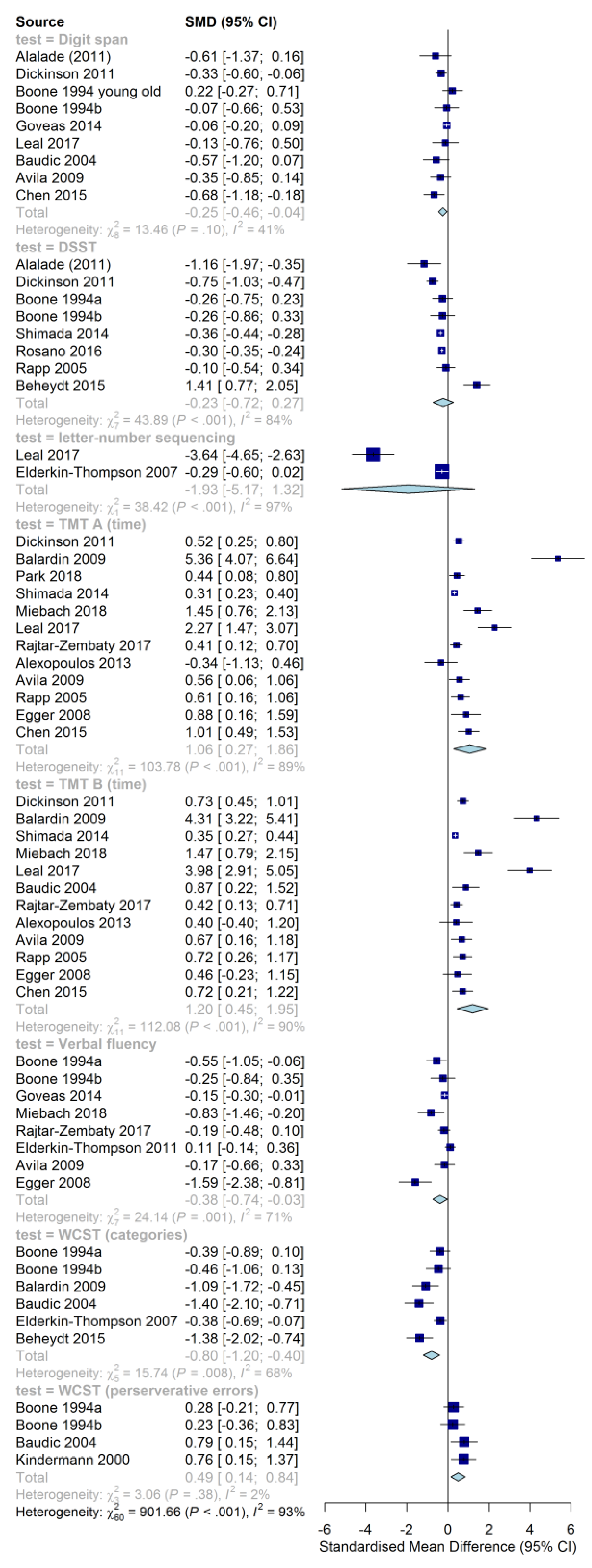
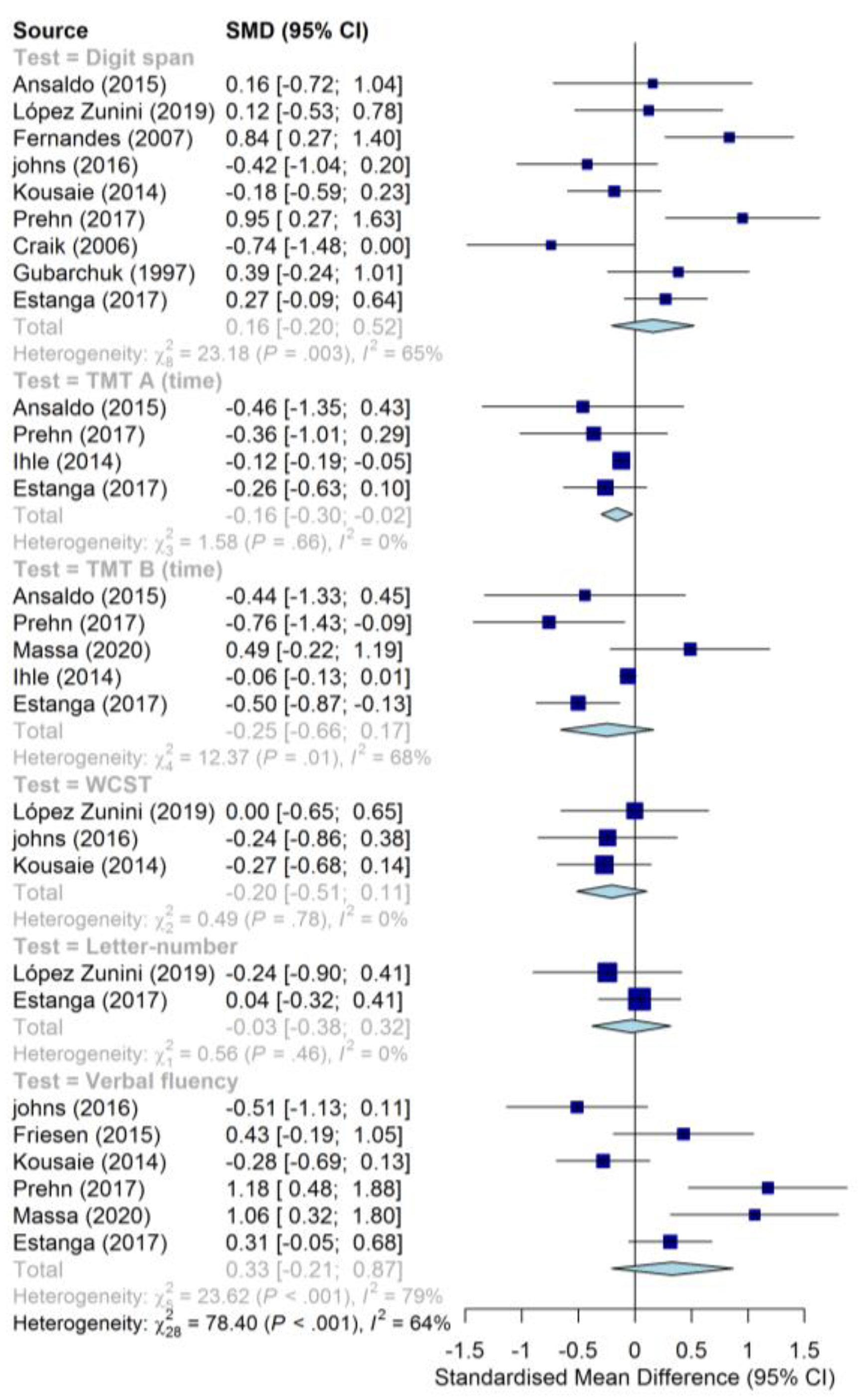
4.5. Cognitive Functioning in LLD and Bilingualism
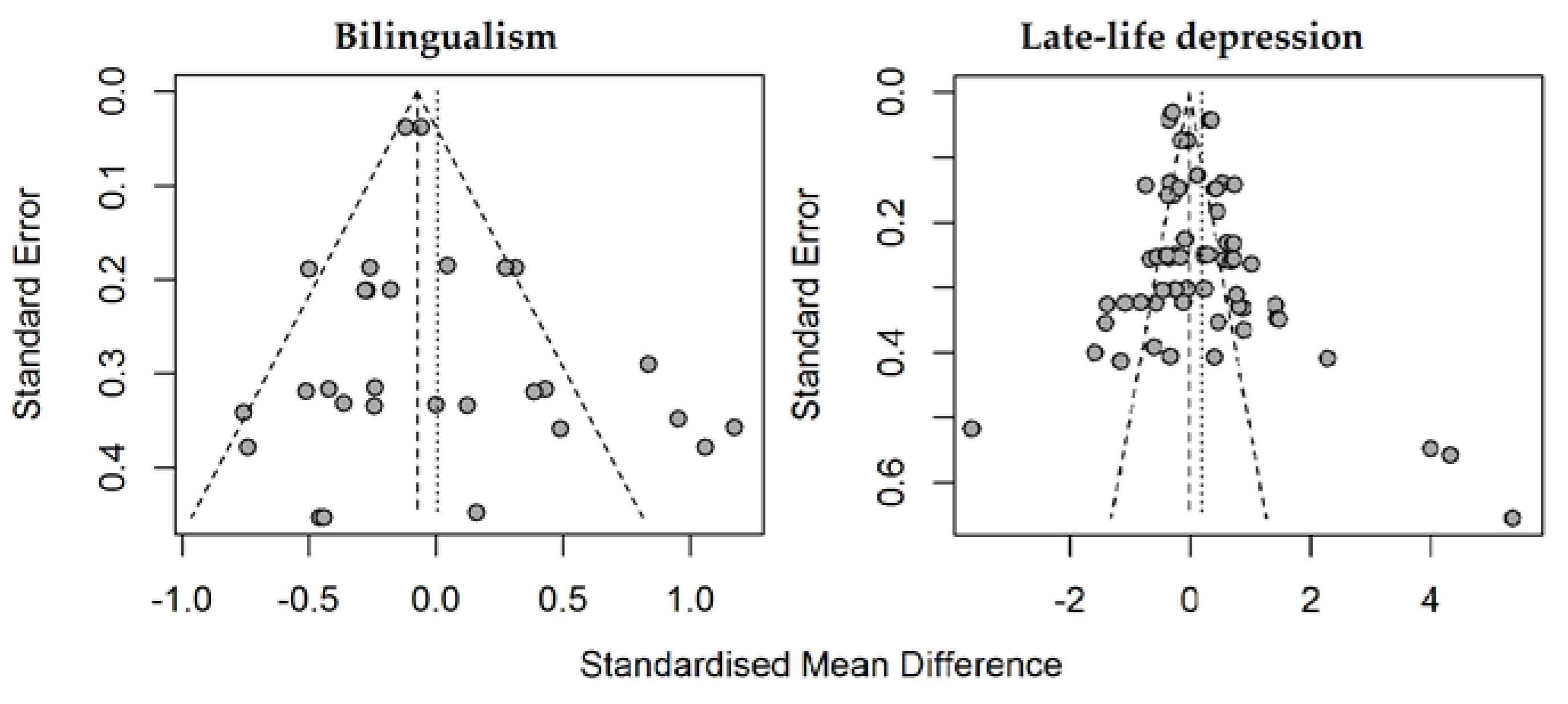
4.6. Risk of Bias Across Studies
5. Discussion
5.1. Cognitive Function in LLD
5.2. Cognitive Function in Bilinguals
5.3. Issues in Defining Bilingualism
5.4. Issues Pertaining to Older Populations Specifically
6. Directions for Future Research
6.1. Language Learning Interventions
6.2. Lifelong Bilinguals Versus Lifelong Monolinguals
6.3. General Methodological Improvements
7. Strengths and Limitations
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kangas, O. One hundred years of money, welfare and death: Mortality, economic growth and the development of the welfare state in 17 OECD countries 1900–2000. Int. J. Soc. Welf. 2010, 19, S42–S59. [Google Scholar] [CrossRef]
- Meerding, W.J.; Bonneux, L.; Polder, J.J.; Koopmanschap, M.A.; van der Maas, P.J. Demographic and epidemiological determinants of healthcare costs in Netherlands: Cost of illness study. BMJ 1998, 317, 111–115. [Google Scholar] [CrossRef]
- 2020 Alzheimer’s disease facts and figures. Alzheimer’s Dement. 2020, 16, 391–460. [CrossRef] [PubMed]
- Hebert, L.E.; Weuve, J.; Scherr, P.A.; Evans, D.A. Alzheimer disease in the United States (2010–2050) estimated using the 2010 census. Neurology 2013, 80, 1778–1783. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders 1; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar] [CrossRef]
- Blazer, D.G. Depression in Late Life: Review and Commentary. Focus (Madison) 2009, 7, 118–136. [Google Scholar] [CrossRef]
- Djernes, J.K. Prevalence and predictors of depression in populations of elderly: A review. Acta Psychiatr. Scand. 2006, 113, 372–387. [Google Scholar] [CrossRef]
- Guerra, M.; Prina, A.M.; Ferri, C.P.; Acosta, D.; Gallardo, S.; Huang, Y.; Jacob, K.S.; Jimenez-Velazquez, I.Z.; Llibre Rodriguez, J.J.; Liu, Z.; et al. A comparative cross-cultural study of the prevalence of late life depression in low and middle income countries. J. Affect. Disord. 2016, 190, 362–368. [Google Scholar] [CrossRef]
- Wagenaar, D.B.; Mickus, M.A.; Gaumer, K.A.; Colenda, C.C. Late-Life Depression and Mental Health Services in Primary Care. J. Geriatr. Psychiatry Neurol. 2002, 15, 134–140. [Google Scholar] [CrossRef]
- Hinton, L.; Zweifach, M.; Tang, L.; Unützer, J.; Oishi, S. Gender Disparities in the Treatment of Late-Life Depression: Qualitative and Quantitative Findings From the IMPACT Trial. Am. J. Geriatr. Psychiatry 2006, 14, 884–892. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Rao, S.; Vaze, A. Do primary care physicians have particular difficulty identifying late-life depression? A meta-analysis stratified by age. Psychother. Psychosom. 2010, 79, 285–294. [Google Scholar] [CrossRef]
- Conwell, Y.; Van Orden, K.; Caine, E.D. Suicide in older adults. Psychiatr. Clin. N. Am. 2011, 34, 451–468. [Google Scholar] [CrossRef] [PubMed]
- Covey, L.S.; Glassman, A.H.; Stetner, F. Cigarette smoking and major depression. J. Addict. Dis. 1998, 17, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Brière, F.N.; Rohde, P.; Seeley, J.R.; Klein, D.; Lewinsohn, P.M. Comorbidity between major depression and alcohol use disorder from adolescence to adulthood. Compr. Psychiatry 2014, 55, 526–533. [Google Scholar] [CrossRef]
- Kim, J.-M.; Stewart, R.; Shin, I.-S.; Yoon, J.-S.; Lee, H.-Y. Lifetime urban/rural residence, social support and late-life depression in Korea. Int. J. Geriatr. Psychiatry 2004, 19, 843–851. [Google Scholar] [CrossRef]
- Koenig, A.M.; Bhalla, R.K.; Butters, M.A. Cognitive functioning and late-life depression. J. Int. Neuropsychol. Soc. 2014, 20, 461–467. [Google Scholar] [CrossRef]
- Rajtar, A.; Sałakowski, A.; Rajtar-Zembaty, J.; Starowicz-Filip, A. Executive dysfunction in late-life depression. Psychiatr. Pol. 2017, 51, 705–718. [Google Scholar] [CrossRef]
- Diniz, B.S.; Butters, M.A.; Albert, S.M.; Dew, M.A.; Reynolds, C.F. Late-life depression and risk of vascular dementia and Alzheimer’s disease: Systematic review and meta-analysis of community-based cohort studies. Br. J. Psychiatry 2013, 202, 329–335. [Google Scholar] [CrossRef]
- Zanetti, M.; Ballabio, C.; Abbate, C.; Cutaia, C.; Vergani, C.; Bergamaschini, L. Mild cognitive impairment subtypes and vascular dementia in community-dwelling elderly people: A 3-year follow-up study. J. Am. Geriatr. Soc. 2006, 54, 580–586. [Google Scholar] [CrossRef]
- Panza, F.; Frisardi, V.; Capurso, C.; D’Introno, A.; Colacicco, A.M.; Imbimbo, B.P.; Santamato, A.; Vendemiale, G.; Seripa, D.; Pilotto, A.; et al. Late-Life depression, mild cognitive impairment, and dementia: Possible continuum? Am. J. Geriatr. Psychiatry 2010, 18, 98–116. [Google Scholar] [CrossRef]
- Butters, M.A.; Young, J.B.; Lopez, O.; Aizenstein, H.J.; Mulsant, B.H.; Reynolds, C.F.; DeKosky, S.T.; Becker, J.T. Pathways linking late-life depression to persistent cognitive impairment and dementia. Dialogues Clin. Neurosci. 2008, 10, 345–357. [Google Scholar]
- Crocco, E.A.; Castro, K.; Loewenstein, D.A. How late-life depression affects cognition: Neural mechanisms. Curr. Psychiatry Rep. 2010, 12, 34–38. [Google Scholar] [CrossRef]
- Blazer, D.G.; Hybels, C.F. Origins of depression in later life. Psychol. Med. 2005, 35, 1241–1252. [Google Scholar] [CrossRef]
- Chang, S.-C.; Pan, A.; Kawachi, I.; Okereke, O.I. Risk factors for late-life depression: A prospective cohort study among older women. Prev. Med. 2016, 91, 144–151. [Google Scholar] [CrossRef]
- Hays, J.C.; Landerman, L.R.; George, L.K.; Flint, E.P.; Koenig, H.G.; Land, K.C.; Blazer, D.G. Social correlates of the dimensions of depression in the elderly. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 1998, 53B, P31–P39. [Google Scholar] [CrossRef]
- Lue, B.-H.; Chen, L.-J.; Wu, S.-C. Health, financial stresses, and life satisfaction affecting late-life depression among older adults: A nationwide, longitudinal survey in Taiwan. Arch. Gerontol. Geriatr. 2010, 50, S34–S38. [Google Scholar] [CrossRef]
- Kurlowicz, L.H. Social factors and depression in late life. Arch. Psychiatr. Nurs. 1993, 7, 30–36. [Google Scholar] [CrossRef]
- Kim, J.-M.; Shin, I.-S.; Yoon, J.-S.; Stewart, R. Prevalence and correlates of late-life depression compared between urban and rural populations in Korea. Int. J. Geriatr. Psychiatry 2002, 17, 409–415. [Google Scholar] [CrossRef]
- Stern, Y. Cognitive reserve. Neuropsychologia 2009, 47, 2015–2028. [Google Scholar] [CrossRef]
- Scarmeas, N.; Stern, Y. Cognitive reserve and lifestyle. J. Clin. Exp. Neuropsychol. 2003, 25, 625–633. [Google Scholar] [CrossRef]
- Leles da Costa Dias, F.; Teixeira, A.L.; Cerqueira Guimarães, H.; Borges Santos, A.P.; Rios Fonseca Ritter, S.; Barbosa Machado, J.C.; Tonidandel Barbosa, M.; Caramelli, P. Prevalence of late-life depression and its correlates in a community-dwelling low-educated population aged 75+ years: The Pietà study. J. Affect. Disord. 2019, 242, 173–179. [Google Scholar] [CrossRef]
- Gertner, A.K.; Domino, M.E.; Dow, W.H. Risk factors for late-life depression and correlates of antidepressant use in Costa Rica: Results from a nationally-representative longitudinal survey of older adults. J. Affect. Disord. 2017, 208, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Pollock, B.G. The pharmacokinetic imperative in late-life depression. J. Clin. Psychopharmacol. 2005, 25, S19–S23. [Google Scholar] [CrossRef] [PubMed]
- Solai, L.K.K.; Mulsant, B.H.; Pollock, B.G. Selective serotonin reuptake inhibitors for late-life depression: A comparative review. Drugs Aging 2001, 18, 355–368. [Google Scholar] [CrossRef] [PubMed]
- Rapaport, M.H.; Schneider, L.S.; Dunner, D.L.; Davies, J.T.; Pitts, C.D. Efficacy of controlled-release paroxetine in the treatment of late-life depression. J. Clin. Psychiatry 2003, 64, 1065–1074. [Google Scholar] [CrossRef]
- Schneider, L.S.; Nelson, J.C.; Clary, C.M.; Newhouse, P.; Krishnan, K.R.R.; Shiovitz, T.; Weihs, K. An 8-Week Multicenter, Parallel-Group, Double-Blind, Placebo-controlled study of sertraline in elderly outpatients with major depression. Am. J. Psychiatry 2003, 160, 1277–1285. [Google Scholar] [CrossRef]
- Tedeschini, E.; Levkovitz, Y.; Iovieno, N.; Ameral, V.E.; Nelson, J.C.; Papakostas, G.I. Efficacy of antidepressants for late-life depression. J. Clin. Psychiatry 2011, 72, 1660–1668. [Google Scholar] [CrossRef]
- Bohlmeijer, E.; Smit, F.; Cuijpers, P. Effects of reminiscence and life review on late-life depression: A meta-analysis. Int. J. Geriatr. Psychiatry 2003, 18, 1088–1094. [Google Scholar] [CrossRef]
- Cuijpers, P.; van Straten, A.; Smit, F. Psychological treatment of late-life depression: A meta-analysis of randomized controlled trials. Int. J. Geriatr. Psychiatry 2006, 21, 1139–1149. [Google Scholar] [CrossRef]
- Bhalla, R.K.; Butters, M.A.; Mulsant, B.H.; Begley, A.E.; Zmuda, M.D.; Schoderbek, B.; Pollock, B.G.; Reynolds, C.F.; Becker, J.T. Persistence of neuropsychologic deficits in the remitted state of late-life depression. Am. J. Geriatr. Psychiatry 2006, 14, 419–427. [Google Scholar] [CrossRef]
- Koenig, A.M.; Delozier, I.J.; Zmuda, M.D.; Marron, M.M.; Begley, A.E.; Anderson, S.J.; Reynolds, C.F.; Arnold, S.E.; Becker, J.T.; Butters, M.A. Neuropsychological functioning in the acute and remitted states of late-life depression. J. Alzheimer’s Dis. 2015, 45, 175–185. [Google Scholar] [CrossRef]
- Liao, W.; Zhang, X.; Shu, H.; Wang, Z.; Liu, D.; Zhang, Z. The characteristic of cognitive dysfunction in remitted late life depression and amnestic mild cognitive impairment. Psychiatry Res. 2017, 251, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Ramscar, M.; Hendrix, P.; Love, B.; Baayen, H. Learning is not decline. Ment. Lex. 2014, 8, 450–481. [Google Scholar] [CrossRef]
- Ramscar, M.; Hendrix, P.; Shaoul, C.; Milin, P.; Baayen, H. The Myth of cognitive decline: Non-linear dynamics of lifelong learning. Top. Cogn. Sci. 2014, 6, 5–42. [Google Scholar] [CrossRef]
- Formosa, M. Education and older adults at the university of the third age. Educ. Gerontol. 2012, 38, 114–126. [Google Scholar] [CrossRef]
- Kelly, M.E.; Loughrey, D.; Lawlor, B.A.; Robertson, I.H.; Walsh, C.; Brennan, S. The impact of cognitive training and mental stimulation on cognitive and everyday functioning of healthy older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2014, 15, 28–43. [Google Scholar] [CrossRef] [PubMed]
- Kueider, A.M.; Parisi, J.M.; Gross, A.L.; Rebok, G.W. Computerized cognitive training with older adults: A systematic review. PLoS ONE 2012, 7, e40588. [Google Scholar] [CrossRef] [PubMed]
- Anguera, J.A.; Gunning, F.M.; Areán, P.A. Improving late life depression and cognitive control through the use of therapeutic video game technology: A proof-of-concept randomized trial. Depress. Anxiety 2017, 34, 508–517. [Google Scholar] [CrossRef]
- Morimoto, S.S.; Wexler, B.E.; Liu, J.; Hu, W.; Seirup, J.; Alexopoulos, G.S. Neuroplasticity-based computerized cognitive remediation for treatment-resistant geriatric depression. Nat. Commun. 2014, 5, 4579. [Google Scholar] [CrossRef] [PubMed]
- Motter, J.N.; Pimontel, M.A.; Rindskopf, D.; Devanand, D.P.; Doraiswamy, P.M.; Sneed, J.R. Computerized cognitive training and functional recovery in major depressive disorder: A meta-analysis. J. Affect. Disord. 2016, 189, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Seitz, A.R. A New framework of design and continuous evaluation to improve brain training. J. Cogn. Enhanc. 2018, 2, 78–87. [Google Scholar] [CrossRef]
- Olfers, K.J.F.; Band, G.P.H.; Colzato, L.S.; Hommel, B. The Case of the Leiden “Lifestyle 2030” Study. In Theory-Driven Approaches to Cognitive Enhancement; Colzato, L.S., Ed.; Springer International Publishing: Cham, Germany, 2017; pp. 305–317. [Google Scholar]
- Kaushanskaya, M.; Marian, V. The bilingual advantage in novel word learning. Psychon. Bull. Rev. 2009, 16, 705–710. [Google Scholar] [CrossRef]
- Costa, A.; Hernández, M.; Costa-Faidella, J.; Sebastián-Gallés, N. On the bilingual advantage in conflict processing: Now you see it, now you don’t. Cognition 2009, 113, 135–149. [Google Scholar] [CrossRef]
- Bialystok, E. Bilingualism Research: Visions For The Future. Available online: https://www.youtube.com/watch?v=Asyf1my3RP4&t=14m26 (accessed on 27 August 2020).
- Bialystok, E.; Craik, F.I.M. Cognitive and linguistic processing in the bilingual mind. Curr. Dir. Psychol. Sci. 2010, 19, 19–23. [Google Scholar] [CrossRef]
- Lehtonen, M.; Soveri, A.; Laine, A.; Järvenpää, J.; de Bruin, A.; Antfolk, J. Is bilingualism associated with enhanced executive functioning in adults? A meta-analytic review. Psychol. Bull. 2018, 144, 394–425. [Google Scholar] [CrossRef]
- Nichols, E.S.; Wild, C.J.; Stojanoski, B.; Battista, M.E.; Owen, A.M. Bilingualism affords No general cognitive advantages: A population study of executive function in 11,000 people. Psychol. Sci. 2020, 31, 548–567. [Google Scholar] [CrossRef]
- Laine, M.; Lehtonen, M. Cognitive consequences of bilingualism: Where to go from here? Lang. Cogn. Neurosci. 2018, 33, 1205–1212. [Google Scholar] [CrossRef]
- Alladi, S.; Bak, T.H.; Duggirala, V.; Surampudi, B.; Shailaja, M.; Shukla, A.K.; Chaudhuri, J.R.; Kaul, S. Bilingualism delays age at onset of dementia, independent of education and immigration status. Neurology 2013, 81, 1938–1944. [Google Scholar] [CrossRef]
- Bialystok, E.; Craik, F.I.M.; Freedman, M. Delaying the Onset of Alzheimer Disease. Neurology 2010, 75, 1726–1729. [Google Scholar]
- Woumans, E.; Santens, P.; Sieben, A.; Versijpt, J.; Stevens, M.; Duyck, W. Bilingualism Delays Clinical Manifestation of Alzheimer’s Disease. Bilingualism 2015, 18, 568–574. [Google Scholar] [CrossRef]
- Bialystok, E.; Craik, F.I.M.; Freedman, M. Bilingualism as a Protection against the Onset of Symptoms of Dementia. Neuropsychologia 2007, 45, 459–464. [Google Scholar] [CrossRef]
- Schweizer, T.A.; Ware, J.; Fischer, C.E.; Craik, F.I.M.; Bialystok, E. Bilingualism as a Contributor to Cognitive Reserve: Evidence from Brain Atrophy in Alzheimer’s Disease. Cortex 2012, 48, 991–996. [Google Scholar] [CrossRef]
- Poarch, G.J.; van Hell, J.G. Cross-Language Activation in Children’s Speech Production: Evidence from Second Language Learners, Bilinguals, and Trilinguals. J. Exp. Child Psychol. 2012, 11, 419–438. [Google Scholar] [CrossRef]
- Antoniou, M.; Gunasekera, G.M.; Wong, P.C.M. Foreign Language Training as Cognitive Therapy for Age-Related Cognitive Decline: A Hypothesis for Future Research. Neurosci. Biobehav. Rev. 2013, 37, 2689–2698. [Google Scholar] [CrossRef]
- Van der ploeg, M.; Keijzer, M.; Lowie, W. Methodological Concerns and Their Solutions in Third-Age Language Learning Studies. Dutch J. Appl. Psycholinguist. 2020, in press. [Google Scholar]
- Wechsler, D. WAIS-IV: Wechsler Adult Intelligence Scale. San Antonio, TX Psychol. Corp. 2008, 36, 3245–3252. [Google Scholar]
- Partington, J.E.; Leiter, G.R. Partington’s Pathways Test. Psychol. Serv. Cebter J. 1949, 1, 11–20. [Google Scholar]
- Grant, D.A.; Berg, E. A Behavioral Analysis of Degree of Reinforcement and Ease of Shifting to New Responses in a Weigl-Type Card-Sorting Problem. J. Exp. Psychol. 1948, 38, 404–411. [Google Scholar] [CrossRef]
- Prior, A.; Macwhinney, B. A Bilingual Advantage in Task Switching. Bilingualism 2010, 13, 253–262. [Google Scholar] [CrossRef]
- Hallett, P.E. Primary and Secondary Saccades to Goals Defined by Instructions. Vision Res. 1978, 18, 1279–1296. [Google Scholar] [CrossRef]
- Meyer, S.R.A.; de Jonghe, J.F.M.; Schmand, B.; Ponds, R.W.H.M. The Visual Association Test-Extended: A Cross-Sectional Study of the Performance Validity Measures. Clin. Neuropsychol. 2017, 31, 798–813. [Google Scholar] [CrossRef]
- Bowie, C.R.; Harvey, P.D. Administration and interpretation of the Trail Making Test. Nat. Protoc. 2006, 1, 2277–2281. [Google Scholar] [CrossRef] [PubMed]
- Naismith, S.L.; Rogers, N.L.; Lewis, S.J.G.; Terpening, Z.; Ip, T.; Diamond, K.; Norrie, L.; Hickie, I.B. Sleep Disturbance Relates to Neuropsychological Functioning in Late-Life Depression. J. Affect. Disord. 2011, 132, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Morin, R.T.; Gonzales, M.M.; Bickford, D.; Catalinotto, D.; Nelson, C.; Mackin, R.S. Impaired Financial Capacity in Late-Life Depression: Revisiting Associations with Cognitive Functioning. J. Int. Neuropsychol. Soc. 2019, 25, 1088–1093. [Google Scholar] [CrossRef]
- Lamers, F.; Van Oppen, P.; Comijs, H.C.; Smit, J.H.; Spinhoven, P.; Van Balkom, A.J.L.M.; Nolen, W.A.; Zitman, F.G.; Beekman, A.T.F.; Penninx, B.W.J.H. Comorbidity Patterns of Anxiety and Depressive Disorders in a Large Cohort Study: The Netherlands Study of Depression and Anxiety (NESDA). J. Clin. Psychiatry 2011, 72, 342–348. [Google Scholar] [CrossRef]
- Hugo, J.; Ganguli, M. Dementia and Cognitive Impairment. Epidemiology, Diagnosis, and Treatment. Clin. Geriatr. Med. 2014, 30, 421–442. [Google Scholar] [CrossRef]
- Riedel, O.; Klotsche, J.; Spottke, A.; Deuschl, G.; Förstl, H.; Henn, F.; Heuser, I.; Oertel, W.; Reichmann, H.; Riederer, P.; et al. Cognitive Impairment in 873 Patients with Idiopathic Parkinson’s Disease: Results from the German Study on Epidemiology of Parkinson’s Disease with Dementia (GEPAD). J. Neurol. 2008, 255, 255–264. [Google Scholar] [CrossRef]
- Kist, N.; Sandjojo, J.; Kok, R.M.; Van Den Berg, J.F. Cognitive Functioning in Older Adults with Early, Late, and Very Late Onset Alcohol Dependence. Int. Psychogeriatrics 2014, 26, 1863–1869. [Google Scholar] [CrossRef]
- Barker, M.J.; Greenwood, K.M.; Jackson, M.; Crowe, S.F. Cognitive Effects of Long-Term Benzodiazepine Use: A Meta-Analysis. CNS Drugs 2004, 18, 37–48. [Google Scholar] [CrossRef]
- Drayer, D.E. Lipophilicity, Hydrophilicity, and the Central Nervous System Side Effects of Beta Blockers. Pharmacother. J. Hum. Pharmacol. Drug Ther. 1987, 7, 87–91. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”. A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- National Heart, Lung, and Blood Institute. Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 27 August 2020).
- National Institutes of Health. Quality Assessment of Controlled Intervention Studies–NHLBI, NIH. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 27 August 2020).
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley & Sons, Ltd.: New York, NY, USA, 2009. [Google Scholar]
- Combs, J.G.; Ketchen, D.J.; Crook, T.R.; Roth, P.L. Assessing Cumulative Evidence within “Macro” Research: Why Meta-Analysis Should Be Preferred Over Vote Counting. J. Manag. Stud. 2011, 48, 178–197. [Google Scholar] [CrossRef]
- Friedman, L. Why Vote-Count Reviews Don’t Count (Multiple Letters). Biol. Psychiatry 2001, 49, 161–162. [Google Scholar] [CrossRef]
- R Development Core Team. R: A Language and Environment for Statistical Computing; Foundation for Statistical Computing: Vienna, Austria, 2020; ISBN 3-900051-07-0. [Google Scholar]
- Lüdecke, D. Esc: Effect size computation for meta analysis. Zenodo 2018. [Google Scholar] [CrossRef]
- Schwarzer, G. Package “Meta”. In Proceedings of the 2014 IEEE/ACM 7th International Conference on Utility and Cloud Computing (UCC 2014), London, UK, 8–11 December 2014. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, 1–34. [Google Scholar] [CrossRef]
- Smoski, M.J.; LaBar, K.S.; Steffens, D.C. Relative Effectiveness of Reappraisal and Distraction in Regulating Emotion in Late-Life Depression. Am. J. Geriatr. Psychiatry 2014, 22, 898–907. [Google Scholar] [CrossRef]
- Nelson, H.E. A Modified Card Sorting Test Sensitive to Frontal Lobe Defects. Cortex 1976, 12, 313–324. [Google Scholar] [CrossRef]
- Alalade, E.; Denny, K.; Potter, G.; Steffens, D.; Wang, L. Altered Cerebellar-Cerebral Functional Connectivity in Geriatric Depression. PLoS One 2011, 6, e20035. [Google Scholar] [CrossRef]
- Alexopoulos, G.S.; Hoptman, M.J.; Yuen, G.; Kanellopoulos, D.; Seirup, J.K.; Lim, K.O.; Gunning, F.M. Functional Connectivity in Apathy of Late-Life Depression: A Preliminary Study. J. Affect. Disord. 2013, 149, 398–405. [Google Scholar] [CrossRef]
- Avila, R.; Moscoso, M.A.A.A.; Ribeiz, S.; Arrais, J.; Jaluul, O.; Bottino, C.M.C.C. Influence of Education and Depressive Symptoms on Cognitive Function in the Elderly. Int. Psychogeriatrics 2009, 21, 560–567. [Google Scholar] [CrossRef]
- Balardin, J.B.; Vedana, G.; Ludwig, A.; de Lima, D.B.; Argimon, I.; Schneider, R.; Luz, C.; Schröder, N.; Bromberg, E. Contextual Memory and Encoding Strategies in Young and Older Adults with and without Depressive Symptoms. Aging Ment. Health 2009, 13, 313–318. [Google Scholar] [CrossRef]
- Baudic, S.; Tzortzis, C.; Dalla Barba, G.; Traykov, L. Executive Deficits in Elderly Patients With Major Unipolar Depression. J. Geriatr. Psychiatry Neurol. 2004, 17, 195–201. [Google Scholar] [CrossRef]
- Beheydt, L.L.; Schrijvers, D.; Docx, L.; Bouckaert, F.; Hulstijn, W.; Sabbe, B. Cognitive and Psychomotor Effects of Three Months of Escitalopram Treatment in Elderly Patients with Major Depressive Disorder. J. Affect. Disord. 2015, 188, 47–52. [Google Scholar] [CrossRef]
- Boone, K.B.; Lesser, I.; Miller, B.; Wohl, M.; Berman, N.; Lee, A.; Palmer, B. Cognitive Functioning in a Mildly to Moderately Depressed Geriatric Sample: Relationship to Chronological Age. J. Neuropsychiatry Clin. Neurosci. 1994, 6, 267–272. [Google Scholar]
- Chen, Z.; Lan, G.; Shen, X.; Pan, X.; Chen, X.; LI, J. Relationship of Changes in Cognitive and Depressive Symptoms during Antidepressant Treatment of Individuals with Geriatric Depression and Their Relationship to the APOE Epsilon 4 Allele. Shanghai Arch. Psychiatry 2013, 25, 99–106. [Google Scholar]
- Dickinson, W.J.; Potter, G.G.; Hybels, C.F.; McQuoid, D.R.; Steffens, D.C. Change in Stress and Social Support as Predictors of Cognitive Decline in Older Adults with and without Depression. Int. J. Geriatr. Psychiatry 2011, 26, 1267–1274. [Google Scholar] [CrossRef] [PubMed]
- Egger, K.; Schocke, M.; Weiss, E.; Auffinger, S.; Esterhammer, R.; Goebel, G.; Walch, T.; Mechtcheriakov, S.; Marksteiner, J. Pattern of Brain Atrophy in Elderly Patients with Depression Revealed by Voxel-Based Morphometry. Psychiatry Res. Neuroimaging 2008, 164, 237–244. [Google Scholar] [CrossRef]
- Elderkin-Thompson, V.; Mintz, J.; Haroon, E.; Lavretsky, H.; Kumar, A. Executive Dysfunction and Memory in Older Patients with Major and Minor Depression. Arch. Clin. Neuropsychol. 2007, 22, 261–270. [Google Scholar] [CrossRef]
- Elderkin-Thompson, V.; Moody, T.; Knowlton, B.; Hellemann, G.; Kumar, A. Explicit and Implicit Memory in Late-Life Depression. Am. J. Geriatr. Psychiatry 2011, 19, 364–373. [Google Scholar] [CrossRef] [PubMed]
- Goveas, J.S.; Espeland, M.A.; Hogan, P.E.; Tindle, H.A.; Shih, R.A.; Kotchen, J.M.; Robinson, J.G.; Barnes, D.E.; Resnick, S.M. Depressive Symptoms and Longitudinal Changes in Cognition: Women’s Health Initiative Study of Cognitive Aging. J. Geriatr. Psychiatry Neurol. 2014, 27, 94–102. [Google Scholar] [CrossRef]
- Kindermann, S.S.; Kalayam, B.; Brown, G.G.; Burdick, K.E.; Alexopoulos, G.S. Executive Functions and P300 Latency in Elderly Depressed Patients and Control Subjects. Am. J. Geriatr. Psychiatry 2000, 8, 57–65. [Google Scholar] [CrossRef]
- Leal, S.L.; Noche, J.A.; Murray, E.A.; Yassa, M.A. Disruption of Amygdala–Entorhinal–Hippocampal Network in Late-life Depression. Hippocampus 2017, 27, 464–476. [Google Scholar] [CrossRef] [PubMed]
- Miebach, L.; Wolfsgruber, S.; Frommann, I.; Buckley, R.; Wagner, M. Different Cognitive Complaint Profiles in Memory Clinic and Depressive Patients. Am. J. Geriatr. Psychiatry 2018, 26, 463–475. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Lee, S.B.; Lee, J.J.; Yoon, J.C.; Han, J.W.; Kim, T.H.; Jeong, H.-G.G.; Newhouse, P.A.; Taylor, W.D.; Kim, J.H.; et al. Depression Plays a Moderating Role in the Cognitive Decline Associated With Changes of Brain White Matter Hyperintensities. J. Clin. Psychiatry 2018, 79, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Rapp, M.A.; Dahlman, K.; Sano, M.; Grossman, H.T.; Haroutunian, V.; Gorman, J.M. Neuropsychological Differences Between Late-Onset and Recurrent Geriatric Major Depression. Am. J. Psychiatry 2005, 162, 691–698. [Google Scholar] [CrossRef] [PubMed]
- Rosano, C.; Perera, S.; Inzitari, M.; Newman, A.B.; Longstreth, W.T.; Studenski, S. Digit Symbol Substitution Test and Future Clinical and Subclinical Disorders of Cognition, Mobility and Mood in Older Adults. Age Ageing 2016, 45, 687–694. [Google Scholar] [CrossRef]
- Shimada, H.; Park, H.; Makizako, H.; Doi, T.; Lee, S.; Suzuki, T. Depressive Symptoms and Cognitive Performance in Older Adults. J. Psychiatr. Res. 2014, 57, 149–156. [Google Scholar] [CrossRef]
- Steffens, D.C.; Wagner, H.R.; Levy, R.M.; Horn, K.A.; Krishnan, K.R. Performance Feedback Deficit in Geriatric Depression. Biol. Psychiatry 2001, 50, 358–363. [Google Scholar] [CrossRef]
- Ramos, S.; Fernández García, Y.; Antón, E.; Casaponsa, A.; Duñabeitia, J.A. Does Learning a Language in the Elderly Enhance Switching Ability? J. Neurolinguistics 2017, 43, 39–48. [Google Scholar] [CrossRef]
- Wong, P.C.M.; Ou, J.; Pang, C.W.Y.; Zhang, L.; Tse, C.S.; Lam, L.C.W.; Antoniou, M. Language Training Leads to Global Cognitive Improvement in Older Adults: A Preliminary Study. J. Speech Lang. Hear. Res. 2019, 62, 2411–2424. [Google Scholar] [CrossRef]
- Massa, E.; Köpke, B.; El Yagoubi, R. Age-Related Effect on Language Control and Executive Control in Bilingual and Monolingual Speakers: Behavioral and Electrophysiological Evidence. Neuropsychologia 2020, 138, 107336. [Google Scholar] [CrossRef]
- Little, D. Common European Framework of Reference for Languages. In The TESOL Encyclopedia of English Language Teaching; Wiley: Hoboken, NJ, USA, 2018; pp. 1–6. [Google Scholar]
- Ansaldo, A.I.; Ghazi-Saidi, L.; Adrover-Roig, D. Interference Control in Elderly Bilinguals: Appearances Can Be Misleading. J. Clin. Exp. Neuropsychol. 2015, 37, 455–470. [Google Scholar] [CrossRef]
- Marian, V.; Blumenfeld, H.K.; Kaushanskaya, M. The Language Experience and Proficiency Questionnaire (LEAP-Q): Assessing Language Profiles in Bilinguals and Multilinguals. J. Speech, Lang. Hear. Res. 2007, 50, 940–967. [Google Scholar] [CrossRef]
- Craik, F.I.M.; Bialystok, E. Planning and Task Management in Older Adults: Cooking Breakfast. Mem. Cogn. 2006, 34, 1236–1249. [Google Scholar] [CrossRef]
- Estanga, A.; Ecay-Torres, M.; Ibañez, A.; Izagirre, A.; Villanua, J.; Garcia-Sebastian, M.; Iglesias Gaspar, M.T.; Otaegui-Arrazola, A.; Iriondo, A.; Clerigue, M.; et al. Beneficial Effect of Bilingualism on Alzheimer’s Disease CSF Biomarkers and Cognition. Neurobiol. Aging 2017, 50, 144–151. [Google Scholar] [CrossRef]
- COERLL University of Texas at Austin. Bilingual Language Profile: An Easy-to-Use Instrument to Assess Bilingualism (Spanish-English). Available online: http://sites.la.utexas.edu/bilingual (accessed on 27 August 2020).
- Fernandes, M.A.; Craik, F.; Bialystok, E.; Kreuger, S. Effects of Bilingualism, Aging, and Semantic Relatedness on Memory under Divided Attention. Can. J. Exp. Psychol. 2007, 61, 128–141. [Google Scholar] [CrossRef]
- Friesen, D.C.; Luo, L.; Luk, G.; Bialystok, E. Proficiency and Control in Verbal Fluency Performance across the Lifespan for Monolinguals and Bilinguals. Lang. Cogn. Neurosci. 2015, 30, 238–250. [Google Scholar] [CrossRef]
- Anderson, J.A.E.; Mak, L.; Keyvani Chahi, A.; Bialystok, E. The Language and Social Background Questionnaire: Assessing Degree of Bilingualism in a Diverse Population. Behav. Res. Methods 2018, 50, 250–263. [Google Scholar] [CrossRef]
- Gubarchuk, I.; Kemper, S. Effects of Aging on the Production of Russian. Discourse Process. 1997, 23, 63–82. [Google Scholar] [CrossRef]
- Ihle, A.; Oris, M.; Fagot, D.; Kliegel, M. The Relation of the Number of Languages Spoken to Performance in Different Cognitive Abilities in Old Age. J. Clin. Exp. Neuropsychol. 2016, 38, 1103–1114. [Google Scholar] [CrossRef] [PubMed]
- Johns, B.T.; Sheppard, C.L.; Jones, M.N.; Taler, V. The Role of Semantic Diversity in Word Recognition across Aging and Bilingualism. Front. Psychol. 2016, 7, 1–11. [Google Scholar] [CrossRef]
- Kousaie, S.; Sheppard, C.; Lemieux, M.; Monetta, L.; Taler, V. Executive Function and Bilingualism in Young and Older Adults. Front. Behav. Neurosci. 2014, 8, 1–12. [Google Scholar] [CrossRef] [PubMed]
- López Zunini, R.A.; Morrison, C.; Kousaie, S.; Taler, V. Task Switching and Bilingualism in Young and Older Adults: A Behavioral and Electrophysiological Investigation. Neuropsychologia 2019, 133, 107186. [Google Scholar] [CrossRef]
- Prehn, K.; Taud, B.; Reifergeste, J.; Clahsen, H.; Flöel, A. Neural Correlates of Grammatical Inflection in Older Native and Second-Language Speakers. Bilingualism 2017, 21, 1–12. [Google Scholar] [CrossRef]
- Zhang, Z.; Xu, X.; Ni, H. Small Studies May Overestimate the Effect Sizes in Critical Care Meta-Analyses: A Meta-Epidemiological Study. Crit. Care 2013, 17, R2. [Google Scholar] [CrossRef] [PubMed]
- Ioannidis, J.P.A. Interpretation of Tests of Heterogeneity and Bias in Meta-Analysis. J. Eval. Clin. Pract. 2008, 14, 951–957. [Google Scholar] [CrossRef]
- Field, A.P. Meta-Analysis of Correlation Coefficients: A Monte Carlo Comparison of Fixed- and Random-Effects Methods. Psychol. Methods 2001, 6, 161–180. [Google Scholar] [CrossRef]
- Pfenninger, S.E.; Polz, S. Foreign Language Learning in the Third Age: A Pilot Feasibility Study on Cognitive, Socio-Affective and Linguistic Drivers and Benefits in Relation to Previous Bilingualism of the Learner. J. Eur. Second Lang. Assoc. 2018, 2, 1. [Google Scholar] [CrossRef]
- Bak, T.H.; Long, M.R.; Vega-Mendoza, M.; Sorace, A. Novelty, Challenge, and Practice: The Impact of Intensive Language Learning on Attentional Functions. PLoS One 2016, 11, 1–11. [Google Scholar] [CrossRef]
- Chu, L.W.; Chiu, K.C.; Hui, S.L.; Yu, G.K.K.; Tsui, W.J.C.; Lee, P.W.H. The Reliability and Validity of the Alzheimer’s Disease Assessment Scale Cognitive Subscale (ADAS-Cog) among the Elderly Chinese in Hong Kong. Ann. Acad. Med. Singap. 2000, 29, 474–485. [Google Scholar] [CrossRef]
- Almeida, O.P.; Almeida, S.A. Short Versions of the Geriatric Depression Scale: A Study of Their Validity for the Diagnosis of a Major Depressive Episode According to ICD-10 and DSM-IV. Int. J. Geriatr. Psychiatry 1999, 14, 858–865. [Google Scholar] [CrossRef]
- Reynolds, W.M.; Kobak, K.A. Reliability and Validity of the Hamilton Depression Inventory: A Paper-and-Pencil Version of the Hamilton Depression Rating Scale Clinical Interview. Psychol. Assess. 1995, 7, 472–483. [Google Scholar] [CrossRef]
- Surrain, S.; Luk, G. Describing Bilinguals: A Systematic Review of Labels and Descriptions Used in the Literature between 2005–2015. Bilingualism 2019, 1–15. [Google Scholar] [CrossRef]
- Landreat, M.G.; Vigneau, C.V.; Hardouin, J.B.; Bronnec, M.G.; Marais, M.; Venisse, J.L.; Jolliet, P. Can We Say That Seniors Are Addicted to Benzodiazepines. Subst. Use Misuse 2010, 45, 1988–1999. [Google Scholar] [CrossRef]
- Ramírez Gómez, D. Language Teaching and the Older Adult: The Significance of Experience; Channel View Books: Bristol, UK, 2016. [Google Scholar]
- Mewborn, C.M.; Lindbergh, C.A.; Stephen Miller, L. Cognitive Interventions for Cognitively Healthy, Mildly Impaired, and Mixed Samples of Older Adults: A Systematic Review and Meta-Analysis of Randomized-Controlled Trials. Neuropsychol. Rev. 2017, 27, 403–439. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Legault, J.; Litcofsky, K.A. Neuroplasticity as a Function of Second Language Learning: Anatomical Changes in the Human Brain. Cortex 2014, 58, 301–324. [Google Scholar] [CrossRef]
- Matsumoto, D. Exploring Third-Age Foreign Language Learning from the Well-Being Perspective: Work in Progress. Stud. Self-Access Learn. J. 2019, 10, 111–116. [Google Scholar] [CrossRef]
- Gullifer, J.W.; Titone, D. Characterizing the Social Diversity of Bilingualism Using Language Entropy. Bilingualism 2020, 23, 283–294. [Google Scholar] [CrossRef]
- Bialystok, E.; Craik, F.I.M.; Ryan, J. Executive Control in a Modified Antisaccade Task: Effects of Aging and Bilingualism. J. Exp. Psychol. Learn. Mem. Cogn. 2006, 32, 1341–1354. [Google Scholar] [CrossRef]
- Avorn, J.; Everitt, D.E.; Weiss, S. Increased Antidepressant Use in Patients Prescribed β-Blockers. JAMA J. Am. Med. Assoc. 1986, 255, 357–360. [Google Scholar] [CrossRef]
- Verbeek, D.E.P.; Van Riezen, J.; De Boer, R.A.; Van Melle, J.P.; De Jonge, P. A Review on the Putative Association Between Beta-Blockers and Depression. Heart Fail. Clin. 2011, 7, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Pliatsikas, C. Understanding Structural Plasticity in the Bilingual Brain: The Dynamic Restructuring Model. Biling. Lang. Cogn. 2019, 23, 459–471. [Google Scholar] [CrossRef]
- Kroll, J.F.; Dussias, P.E.; Bice, K.; Perrotti, L. Bilingualism, Mind, and Brain. Annu. Rev. Linguist. 2015, 1, 377–394. [Google Scholar] [CrossRef] [PubMed]
- Bialystok, E.; Abutalebi, J.; Bak, T.H.; Burke, D.M.; Kroll, J.F. Aging in Two Languages: Implications for Public Health. Ageing Res. Rev. 2016, 27, 56–60. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Date | Database | Search String |
|---|---|---|
| 23 January 2020 | PubMed, EBSCOhost | (“late-life depress*” OR “geriatric depress*”) AND (“Trail making t*” OR “TMT” OR “color-shape switch t*” OR “colour-shape switch t*” OR “phonemic verbal fluency” OR “Visual association t*” OR “Vat-E” OR “wisconsin card sorting t*” OR “WCST” OR “modified wisconsin card sorting t*” OR “mwcst” OR “digit-span” OR “digit span” OR “letter number sequencing” OR “letter-number sequencing” OR “symbol coding t*” OR “symbol-coding t*” OR “digit substitution t*” OR “DSST” OR “antisaccade” OR “anti-saccade”) |
| 17 March 2020 | PubMed, EBSCOhost | (“senior*” OR “older adul*” OR “third-age” OR “third age” OR “65*” OR “aged” OR “elder*” OR “pension*”) AND (“lifelong bilingualism” OR “bilingualism” OR “language course” OR “language learning” OR “language training” OR “language acquisition” OR “multilingualism” OR “foreign language” OR “language teaching”) AND (“Trail making t*” OR “TMT” OR “color-shape switch t*” OR “colour-shape switch t*” OR “phonemic verbal fluency” OR “Visual association t*” OR “Vat-E” OR “wisconsin card sorting t*” OR “WCST” OR “modified wisconsin card sorting t*” OR “mwcst” OR “digit-span” OR “digit span” OR “letter number sequencing” OR “letter-number sequencing” OR “symbol coding t*” OR “symbol-coding t*” OR “digit substitution t*” OR “DSST” OR “antisaccade” OR “anti-saccade”) |
| First Author (year) | Country | Group | N (fem.) | Age (SD) | Education (SD) | MMSE (SD) | Operationalization of LLD | Notes |
|---|---|---|---|---|---|---|---|---|
| Alalade (2011) [96] | USA | LLD | 11 (10) | 64.9 (4.5) | 14.4 (3.1) | 28.9 (1.7) | DSM-IV criteria + at least some depressive symptoms as measured with MADRS (≥8) | On average early onset 33.5 (18.5) |
| HC | 18 (11) | 71.2 (6.6) | 15.8 (2.3) | 29.2 (1.2) | ||||
| Alexopoulos (2013) [97] | USA | LLD | 16 (n/a) | 69.0 (5.5) | 17.2 (2.3) | 29.1 (0.9) | DSM-IV criteria + MADRS ≥ 18 | |
| HC | 10 (n/a) | 68.6 (7.0) | 16.3 (3.8) | 28.5 (1.0) | ||||
| Avila (2009) [98] | Brazil | LLD | 30 (22) | 69.5 (7.5) | 11.9 (3.3) | 27.4 (2.4) | DSM-IV criteria + (HAM-D + MADRS. No minimum for inclusion) | Only the high education group was used here since low education group had only approx. 3 years of schooling |
| HC | 33 (26) | 68.0 (7.1) | 11.9 (3.3) | 28.4 (1.7) | ||||
| Balardin (2009) [99] | Brazil | LLD | 22 (9) | 69.4 (1.1) | 7.1 (0.9) | 27.4 (0.4) | ≥5 on the 15 –item Geriatric Depression Scale (GDS) | |
| HC | 22 (16) | 67.8 (1.4) | 9.6 (0.6) | 27.7 (0.3) | ||||
| Baudic (2004) [100] | France | LLD | 21 (n/a) | 71.8 (8.8) | 9.6 (3.3) | 28.1 (1.4) | DSM-IV criteria + MADRS > 20 | |
| HC | 19 (n/a) | 73.6 (7.7) | 13.5 (5.6) | 29.7 (0.6) | ||||
| Beheydt (2015) [101] | Switzer land | LLD | 28 (24) | 74.7 (7.6) | n/a | 25.5 (3.8) | DSM-IV-TR criteria + 30-item GDS score ≥11 | Participants matched on y/of education; MMSE scores in LLD group significantly lower |
| HC | 20 (15) | 72.0 (5.1) | n/a | 28.3 (1.4) | ||||
| Boone (1994) young-old [102] | USA | LLD | 23 (n/a) | 64.4 (2.8) | 15.6 (2.6) | n/a | DSM-III-R criteria measured with SCID interview + (Ham-D. No minimum for inclusion) | Young-old and old-old presented in the same study |
| HC | 54 (n/a) | 64.4 (2.7)) | 14.5 (2.4) | n/a | ||||
| Boone (1994) old-old [102] | USA | LLD | 14 (n/a) | 75.5 (5.1) | 15.3 (2.8) | n/a | DSM-III-R criteria measured with SCID interview + (Ham-D. No minimum for inclusion) | Gender distribution overall is balanced (53% female) |
| HC | 51 (n/a) | 74.7 (4.1) | 14.3 (2.8) | n/a | ||||
| Chen (2013) [103] | China | LLD | 64 (47) | 67.5 (6.0) | 8.9 (4.2) | 29.9 (0.2) | Chinese Classification of Mental Disorder (CCMD-3) + 30-item GDS score ≥ 11 | |
| HC | 31 (18) | 68.2 (8.6) | 9.0 (4.0) | 29.9 (0.2) | ||||
| Dickinson (2011) [104] | USA | LLD | 112 (63) | 68.7 (6.3) | 14.2 (2.5) | 27.8 (2.4) | Not mentioned (Ham-D + MADRS used to measure depression severity) | |
| HC | 101 (73) | 70.5 (5.7) | 15.4 (1.8) | 28.9 (1.3) | ||||
| Egger (2008) [105] | Austria | LLD | 14 (10) | 71.4 (7.5) | 9.4 (2.2) | 27.2 (1.0) | DSM-IV criteria + 30-item GDS score ≥ 15 | |
| HC | 20 (13) | 72.3 (7.7) | 10.8 (2.7) | 28.6 (0.8) | ||||
| Elderkin-Thompson (2007) [106] | USA | LLD | 95 (63) | 70.0 (7.9) | 14.9 (2.7) | 29.0 (1.3) | DSM-IV criteria + 17-item Ham-D ≥ 8 (minor LLD) + 17-item Ham-D ≥ 15 | Combined minor and major depression |
| HC | 71 (42) | 71.5 (7.6) | 14.9 (2.7) | 29.4 (1.1) | ||||
| Elderkin-Thompson (2011) [107] | USA | LLD | 112 (77) | 69.0 (7.9) | 15.6 (2.7) | 29.0 (1.1) | DSM-IV criteria measured with SCID interview + 17-item Ham-D ≥ 15 | |
| HC | 138 (86) | 71.0 (7.7) | 15.5 (2.7) | 29.3 (1.0) | ||||
| Goveas (2014) [108] | USA | LLD | 204 (204) | ≅70 | ≅65% attended or completed college | Modif. MMSE 96.0 (3.5) | ≥5 on the 15 –item Geriatric Depression Scale (GDS) | Women’s health cohort study |
| HC | 2017 (2017) | ≅70 | ≅ 75% attended or completed college | Modif. MMSE 97.0 (2.7) | ||||
| Kindermann (2000) [109] | USA | LLD | 25 (16) | 73.4 (6.0) | 13.3 (2.5) | 28.4 (1.8) | Research Diagnostic Criteria + 21-item Ham-D ≥ 17 | |
| HC | 20 (12) | 71.2 (6.2) | 13.8 (2.5) | 29.2 (1.0) | ||||
| Leal (2017) [110] | USA | LLD | 15 (9) | 67.9 (6.9) | 13.9 (2.2) | 28.1 (0.5) | ≥4 on 15-item GDS + ≥ 8 on 21-item Beck’s Depression Inventory II | |
| HC | 27 (18) | 72.2 (7.6) | 16.7 (2.2) | 28.9 (0.2) | ||||
| Miebach (2018) [111] | Germany | LLD | 21 (14) | 69.4 (8.0) | 12.6 (2.8) | 27.6 (2.1) | ICD-10 criteria + (15-item GDS. No minimum for inclusion) | |
| HC | 21 (12) | 67.5 (7.2) | 15.1 (3.1) | 29.0 (1.2) | ||||
| Park (2018) [112] | South-Korea | LLD | 63 (46) | 71.2 (5.1) | 7.3 (5.5) | 23.6 (4.4) | DSM-IV criteria + (15-item Korean GDS. No minimum for inclusion) | LLD group includes major depression, minor depression, dysthymia, and subsyndromal depression |
| HC | 59 (29) | 70.3 (4.7) | 10.2 (5.8) | 26.3 (3.5) | ||||
| Rajtar-Zembaty (2017) [17] | Poland | LLD | 87 (57) | 68.1 (6.0) | 13.6 (3.3) | n/a | DSM-V criteria + ≥ 7 on 15-item GDS + no depressive episode before age 60 | |
| HC | 100 (61) | 66.8 (4.8) | 14.6 (3.0) | n/a | ||||
| Rapp (2005) [113] | USA | LLD | 40 (25) | 83.3 (8.6) | 10.2 (2.1) | 23.1 (4.7) | DSM-III-R or DSM-IV + ≥ 11 on 30-item GDS | Combined early and late-onset LLD |
| HC | 39 (21) | 84.1 (6.8) | 9.8 (2.0) | 26.0 (3.5) | ||||
| Rosano (2016) [114] | USA | LLD | 2545 (1633) | 74.8 (5.3) | 33.3% less than high school | n/a | ≥5 on 20-item CES-D (subclinical depression) + ≥11 on CES-D (clinical depression) | Combined subclinical and clinical depression |
| HC | 2146 (1179) | 74.6 (5.4) | 23.7% less than high school | n/a | ||||
| Shimada (2014) [115] | Japan | LLD | 657 (245) | 71.4 (4.4) | 44.6% < 10 years | 26.2 (2.5) | ≥6 on 15-item GDS or a diagnosis of depression | Combined depressive complaints group with depressed group |
| HC | 3695 (1921) | 71.5 (5.2) | 33.3% < 10 years | 26.5 (2.4) | ||||
| Smoski (2014) [94] | USA | LLD | 30 (n/a) | 68.3 (6.3) | n/a | >26 | DSM-IV criteria measured with SCID interview + (CES-D. No minimum for inclusion) | |
| HC | 40 (n/a) | 70.8 (7.1) | n/a | >26 | ||||
| Steffens (2001) [116] | USA | LLD | 117 (80) | 70.3 (7.2) | 14.0 (3.6) | ≥24 in 90% | DSM-IV criteria + (HAM-D + MADRS + DDES. No minimum for inclusion) | |
| HC | 142 (103) | 70.2 (6.0) | 15.8 (2.6) | ≥24 in 90% |
| First Author (Year) | Country | Group | N (fem.) | Age (SD) | Education (SD) | MOCA/MMSE (SD) | Bil. Lang. | Operationali-zation of Bilingualism | Other Language Tests | Notes |
|---|---|---|---|---|---|---|---|---|---|---|
| Ansaldo (2015) [121] | Canada | Bi | 10 (n/a) | 74.2 (7.4) | 17.2 (3.1) | MOCA 27.2 (1.6) | French-English | LEAP-Q [122]; ≥30% L2 usage | Bilingual aphasia test part C | |
| Mono | 10 (n/a) | 74.5 (7.1) | 16.1 (3.28) | MOCA 27.7 (1.1) | ||||||
| Craik (2006) [123] | Canada | Bi | 15 (n/a) | 68.8 (6.1) | 15.3 (3.7) | n/a | Varied | Speaking two languages daily from childhood (≤10 years) | Context of acquisition; frequency of L2 usage | |
| Mono | 15 (n/a) | 70.3 (4.3) | 16.1 (3.5) | n/a | ||||||
| Estanga (2017) [124] | Spain | Bi | 88 (46) | 60.5 (4.3) | 14 (4) | MMSE 28.7 (1.23) | Basque-Spanish | Speaking two languages regularly and fluently | Semi-structured interview; Bilingual Language Profile questionnaire [125] | Authors sent a subset of dataset that adhered to inclusion criteria |
| Mono | 43 (25) | 60.8 (4.4) | 12 (2) | MMSE 28.4 (1.31) | ||||||
| Fernandes (2007) [126] | Canada | Bi | 26 (n/a) | 69.7 (0.8) | 16.3 (0.5) | n/a | Varied | Speaking two languages regularly from adolescence (≤12 years) | Self-rating reading, speaking, listening, writing (1–10); AoA; frequency of L2 usage; language preference | |
| Mono | 16 (n/a) | 74.1 (7.5) | 15.5 (0.5) | n/a | ||||||
| Friesen (2015) [127] | Canada | Bi | 21 (n/a) | 71.1 (3.8) | n/a | MMSE >26 | Varied | Speaking two languages fluently on a daily basis | Language and Social Background Questionnaire [128]; self-rated prof.; frequency of language usage; context of language use | |
| Mono | 20 (n/a) | 70.9 (2.6) | n/a | MMSE >26 | ||||||
| Gubar-chuk (1997) [129] | USA + Russia | Bi | 20 (11) | 70.0 (6.6) | 13.7 (4) | n/a | Russian-English | n/a | Self-rating of overall English proficiency (1–4) | Data from two experiments in the same study combined |
| Mono | 20 (10) | 68.2 (7.5) | 12.0 (0) | n/a | ||||||
| Ihle (2016) [130] | Switzer-land | Bi | 928 (n/a) | ≥65 | n/a | n/a | Varied | Speaking ≥ 2 languages regularly (regardless of proficiency) | Dialects did not count as languages | |
| Mono | 1884 (n/a) | ≥65 | n/a | n/a | ||||||
| Johns (2016) [131] | Canada | Bi | 28 (7) | 70.6 (5.7) | 16.1 (1.27) | MOCA 27.7 (1.3) | French-English | Reaching high proficiency in L2 in early adolescence (≤13 years) | Self-rating reading, speaking, listening, writing (1–5) | |
| Mono | 16 (10) | 74.1 (7.5) | 15.1 (3.3) | MOCA 27.1 (1.9) | ||||||
| Kousaie (2014) [132] | Canada | Bi | 36 (17) | 70.7 (5.9) | 16.1 (2.9) | MOCA 27.5 (1.6) | French-English & English-French | Reaching high proficiency in L2 in early adolescence (≤ 13 years) | Self-rating reading, speaking, listening, writing (1–5) | Combined two monolingual groups for our analysis |
| Mono | 61 (23) | 72.4 (6.5) | 15.7 (2.7) | MOCA 27.5 (1.5) | ||||||
| López Zunini (2019) [133] | Canada | Bi | 18 (10) | 71.4 (4.0) | 16 (2.6) | 27.6 (1.6) | French-English | Highly proficient in both languages; no functional knowledge of other languages | Self-rating reading, speaking, listening, writing (1–5) | |
| Mono | 18 (11) | 71.7 (3.5) | 15.6 (2.7) | 27.8 (1.3) | ||||||
| Massa (2020) [119] | France | Bi | 16 (n/a) | 72.3 (5.0) | 16.0 (2.7) | MMSE 29.5 (0.8) | French-Italian/Italian-French | Bilinguals were all dominant in French | Sociolinguistic questionnaire regarding frequency/context of usage | |
| Mono | 16 (n/a) | 71.1 (5.9) | 15.1 (2.4) | MMSE 28.9 (1.6) | ||||||
| Prehn (2017) [134] | Germany | Bi | 19 (n/a) | >55 | Most ≥ Undergraduate | MMSE 29.7 (0.5) | English-German & Russian-German | ≥ B2 on CEFR measured with Goethe Institute Placement Test | German vocabulary and grammar test using cloze test | |
| Mono | 18 (n/a) | >55 | Most ≥ Undergraduate | MMSE 29.3 (0.9) | ||||||
| First author | Country | Group | N (fem.) | Age (SD) | Education | Global cogn. | Language learnt? | Intervention | ||
| Ramos (2017) [117] | Spain | Lang | 26 (12) | 67.4 | 92% ≥ secondary education | MMSE 28.4 | Basque | 8-month language course by an education center for adults | ||
| Ctrl | 17 (9) | 69.2 | 71% ≥ secondary education | MMSE 28.5 | ||||||
| Wong (2019) [118] | China | Lang. | 53 (43) | 70.8 (6.0) | Most < high school graduate | ADAS-Cog 8.3 (4.6) | English | 5 h per week 2 to 3 days a week for 6 months in senior center (130 h max) | ||
| Game | 51 (44) | 71.1 (6.5) | Most < high school graduate | ADAS-Cog 9.1 (5.4) | ||||||
| Music | 49 (43) | 71.1 (6.1) | Most < high school graduate | ADAS-Cog 9.1 (5.6) |
| Author | Group | Test | Hedges’ g | Conclusion |
|---|---|---|---|---|
| Wong (2019) [118] | Language learning | Digit-span (forward) | 0.09 (very small) language vs. gaming 0.04 (very small) language vs. music | No significant differences between language/music/gaming groups after completing the intervention |
| Wong (2019) [118] | Language learning | Digit-span (backward) | −0.26 Language vs. games (small) −0.58 language vs. music (medium) | Significant gains in digit-span performance in language learning intervention, but not in the music or gaming interventions |
| Ramos (2017) [117] | Language-learning | Color-shape switch (RTs to switch trials) | 0.1 (small) | Decrease in RTs on switch trials was slightly larger in language learning group than in controls, but this was not significant |
| Massa (2020) [119] | Lifelong biling. | Antisaccade (% correct) | −0.50 (medium) | Bilinguals made slightly more mistakes than monolinguals, but this was not significant |
| Massa (2020) [119] | Lifelong biling. | Antisaccade (congruent –incongruent) | 0.18 (small) | Bilinguals had slightly shorter response times than monolinguals, but this was not significant |
| Ansaldo (2015) [121] | Lifelong biling. | TMT A errors | −0.73 (medium) | Bilinguals made fewer errors than monolinguals |
| Ansaldo (2015) [121] | Lifelong biling. | TMT B errors | −0.33 (small) | Bilinguals made fewer errors than monolinguals |
| Smoski (2014) [94] | LLD | TMT A (percentile) | −0.09 (small) | LLD took slightly longer to complete TMT A than HC, but this was not significant |
| Smoski (2014) [94] | LLD | TMT B (percentile) | −0.47 (medium) | LLD took longer to complete TMT B than HC, but this was not significant |
| Steffens (2001) [116] | LLD | TMT B (% perseveration errors) | 0.27 (small) | LLD group made significantly more perseveration errors than HC |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brouwer, J.; van den Berg, F.; Knooihuizen, R.; Loerts, H.; Keijzer, M. Exploring Language Learning as a Potential Tool against Cognitive Impairment in Late-Life Depression: Two Meta-Analyses and Suggestions for Future Research. Behav. Sci. 2020, 10, 132. https://doi.org/10.3390/bs10090132
Brouwer J, van den Berg F, Knooihuizen R, Loerts H, Keijzer M. Exploring Language Learning as a Potential Tool against Cognitive Impairment in Late-Life Depression: Two Meta-Analyses and Suggestions for Future Research. Behavioral Sciences. 2020; 10(9):132. https://doi.org/10.3390/bs10090132
Chicago/Turabian StyleBrouwer, Jelle, Floor van den Berg, Remco Knooihuizen, Hanneke Loerts, and Merel Keijzer. 2020. "Exploring Language Learning as a Potential Tool against Cognitive Impairment in Late-Life Depression: Two Meta-Analyses and Suggestions for Future Research" Behavioral Sciences 10, no. 9: 132. https://doi.org/10.3390/bs10090132
APA StyleBrouwer, J., van den Berg, F., Knooihuizen, R., Loerts, H., & Keijzer, M. (2020). Exploring Language Learning as a Potential Tool against Cognitive Impairment in Late-Life Depression: Two Meta-Analyses and Suggestions for Future Research. Behavioral Sciences, 10(9), 132. https://doi.org/10.3390/bs10090132