Innovative Self-Confidence Webinar Intervention for Depression in the Workplace: A Focus Group Study and Systematic Development

Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Theme 1: Practicality and Barriers on a Personal Level
3.1.1. Subtheme: Content
“Content if it’s relevant to you or your job, or your life at some point then, you know it could be however long you want because people will always engage with the topic.” (R2)
“So I think I want to have a really clear in my mind the structure and what actually they are going to talk about, what I learn before I would sign up to that, but I would not rule it out completely if it is not something really I wanted to do.” (R5)
“It’s about learning to develop some work-related skills; it was a training tool rather than a discussion tool.” (R9)
“So, the really good ones, particularly I mean most I have done, have been around software, to practically going through a tool online rather than they come to the office and show it to us that takes too long.” (R2)
“Actually I would do a lot on well-being, workplace well-being just because that’s what I’m interested in, and that can be implemented in the office.” (R4)
“Something that is useful to me and my personal life and maybe I have an issue with. So I think I would probably would be more motivated to do that more so hmm than work.” (R6)
3.1.2. Subtheme: Time and Duration Preference
“Yeah they schedule kind of like pre-lunch time at 11, so you can have a good time to get all your first priorities out of the way. Then you can join the webinar and in that way it’s quite useful.” (R6)
“I’ve got a view that early afternoon until 3 o’clock is quite a good time in terms of you have had your lunch, you have come back to your desk, and sort of you might have some time after that. You need to carry on with work, so it should not be the first thing of the day and not at the end of the day obviously.” (R5)
“Morning, well I think I definitely would give it all of my time in the morning, when I have got the whole day ahead of me and then, you know when it comes to 3, you obviously have a bit more crunch at that time.” (R10)
“It can be quite hard to keep engaged and keep focused on something if it’s more than 30 or 45 min. I reckon two hours will be quite a big ask especially when you spend a day like staring at the screen.” (R6)
“I always feel like half an hour and 15 min of questions and answers is good. So if you were really busy, you can just watch the first half hour, because not everyone wants to ask questions, yeah.” (R1)
“Another thing, the length would make a difference to me, if it was anything 45 min to an hour max, I just don’t think I can pay attention.” (R9)
“It is based on how interesting the last one is, then I will turn to the next one kind of thing.” (R4)
“I think would be better to have it 30 min in a number of days, one day a week rather than having the whole two-hour session in one day, so you can set aside some time for each day in a week.” (R5)
“Yeah there’s another thing about the thought that you can’t just disappear for half an hour, for every reason you need to be at your place somehow.” (R7)
“I think it depends because the ones I did were work-related, so in terms of people around me it’s actually fine for me to do it at my desk during working hours. But something like well-being training might not be received the same way by my colleagues, where I will be doing something that’s not directly related to work, so I think maybe that could be something that needs to be considered.” (R5)
3.1.3. Subtheme: Features of Webinar
“I think if you want to have a screen there must be something there, if it’s just a voice coming out, I think I would move away. Even if it’s a video of someone talking, there has to be something or if it’s like a 30-s animation or something like that, that would keep your attention.” (R5)
“Yeah I think diverse range of visual content and interactive content and that will do, so yeah.” (R1)
“People you know might be more interested with the nice spread designs, with nice soothing colors. I don’t know, sometimes you look at a website or attend a webinar and literally the layout designs make you like it.” (R4)
“If it’s a mix with some visual stuff, a group conversation and yeah some kind of interactive talking on the headset or typing stuff in mm I think that’s more likely to keep people’s attention. Yeah.” (R8)
“If you would provide some links to potential relevant information such as about mindfulness, that would be one aspect people would refer to or if there’s a work sheet attached that is about something. So they don’t have to do it but compliments what they talked about. Or maybe a link to an app that does the same thing, or reminder for mindfulness for next week or something.” (R4)
“I would like it to be hmm…some resources where I can reflect back. So that would be good, or emails.” (R7)
“And that made me remind of what was in the session that you’ve just done, because when you are engaged in the webinar, it comes to a point when you can’t remember. So if you could find some of the things that have been talked about, after the session, maybe that would be good.” (R6)
“Yeah there might be something or resources that were in the background or something that you don’t have the chance to write down, so it might just be useful to have that captured somewhere.” (R5)
“Yeah I agree sometimes when you have technical problems in linking up, it can just put you off the whole idea. Or if it’s too complicated to join and if it seems too much of a hassle.” (R6)
“Sometimes you have to add, download a little program to run in your desktop and I think, with something like this it would be better to have it in the browser so that if you are working with laptops that isn’t yours or somewhere within the workplace you don’t have to bring it on to the system, yeah.” (R6)
“So just a kind of thing where you just need to go to a web page and log in with some pre-login details, nothing more complicated than that.” (R8)
“Yes that’s true actually, yeah, once you have started you need some kind of support system in case some people are struggling.” (R9)
“Yeah my attention span on the pre-recorded ones was not very good because I knew that was no danger of me missing something. It was pre-recorded so I can just skip up or I can watch the whole thing again. I think ultimately I was paying less attention to it rather than the live one. And I would have felt less bad about kicking out completely with that to be honest.” (R6)
“I think obviously the nature of the discussion is that people are just more naturally engaging when in live, or when you’re presenting something, very straight to the point whereas when you have live discussion, it can be more engaging, and encourage people to get involve with the conversation as well rather than just listening to for half an hour completely.” (R5)
“Hmm we probably learn less with the recorded format, but if you were really busy and can’t get anywhere so you can watch it in your own time, yeah.” (R8)
3.1.4. Subtheme: Level of Participation
“I think the thing I just said, I mean where people feel like they might be forced to participate, that might put people off so I think it’s good to have the option but to make it clear that you don’t have to engage if you don’t want to, you could just listen.” (R9)
“Something interactive, like talking on the headset or typing stuff, hmm I think that would be more likely to keep people’s attention.” (R8)
3.1.5. Subtheme: Personalization
“I think quite personalized maybe in a way, which you don’t always get with webinars because they sort of aim it at delivering information to save amount of time, I don’t know but maybe something a bit more about you rather than just things in general, I suppose.” (R6)
“Yeah I think personalized is important if someone to be confident about themselves and also I would believe, it’s not just giving me some general stuff, I think it has to be completely tailored to why and how a person feels, that would be better.” (R7)
“I’m going to say something like testing or sort of questionnaire you can fill up beforehand, I know it’s quite difficult because so many people are involved in a session but you need to sort of have an understanding of what the person’s problems are, and probably want to find out before you can really engage with them, I think.” (R5)
3.2. Theme 2: Practicality and Barriers on an Interpersonal Level
3.2.1. Subtheme: Stigma from Others
“Hmm especially if it was, hmm, yeah something like mental health, you either want to be able to type or being in another room with different environment, not general office environment. Hmm, yeah.” (R3)
“Also the culture in terms of how people accept things, hmm, well-being and stuff, things as quite important, it’s like thinking being able to do it but also nothing judged when doing it.” (R6)
“Like if it turns out the guy next to you was doing it, you would have no way of not identifying him.” (R4)
“I think it depends ’cause the one I did were work-related, so in terms of people around me it’s actually fine for me to do it at my desk during working hours, but something like your suggestion or the other examples it might not be received the same way by my colleagues, where I will be doing something that’s not directly related to work, so I think maybe that could be something that needs to be considered.” (R5)
3.2.2. Subtheme: Level of Engagement with Presenter/Participants
“I think I do want to know who they were because, for example there will be about 10 people who will be listening to the same thing. You want to at least to know a little bit about them, I want to at least know roughly who they were, hmm, even if we have, I don’t know, nicknames or something. It has to have a sense of sort of personal link with them I think.” (R5)
“I’m interested to see what they got to say, but I don’t want to get into a discussion with them directly.” (R9)
“Honestly I think, again, it comes out to content, what topic it is. Because if it’s just to tell you some information then doesn’t really matter how many people around, but if the purpose of it is to interact with it, I think a smaller number may be better because particularly we are talking about personal topic sort of thing, you don’t want to broadcast that (laugh).” (R2)
“It all depends on the program but I would say not more than 20.” (R5)
“Although before signing up I might be more interested to know who they are. So actually, the point of signing up, if it says a bit about who the presenter is, why they are qualified and why they might be interesting, hmmm, that might make a difference signing up in the first place.” (R9)
“I mean, not to have a mental health doctor for the next six weeks, that’s being a bit extreme, yeah, but just being aware that they have background in this field and they are knowledgeable about it, is enough for me.” (R5)
“The worst thing is when we have someone who is, obviously that’s not their fault, but is a bit nervous, and kept saying ‘that was really interesting, thank you’, I’ve already heard that 40 times so I guess just being concise and very eloquent and informative.” (R10)
3.2.3. Subtheme: Moderated Interaction
“So you can just type in a question and then the moderator of the webinar will receive the questions in like a big feed, and then at some point during or after the presentation they will answer those questions. So you can kind of interact with other people but you are not interrupting the session, which is really good.” (R2)
“Basically I don’t want a person just reading it, but I want that they have control over our interactions, not just one person consistently talking.” (R10)
“So I want to see if someone else is asking a question and what the responses are. I guess if you got something to say, you can say, but it’s all being filtered to the presenter and they decide whether your opinion is valid. Well because otherwise, I don’t know I mean, but you could have people being rude or inappropriate.” (R9)
3.3. Theme 3: Practicality and Barriers on an Organizational Level
3.3.1. Subtheme: Endorsement from Management
“If it was something been mentioned by line management, to say that, you know, ‘this is a really good system, why not try it’, etcetera, and they will help you sort of, not manage your diary, but just you know, for them to be aware where are you going while attending the webinar, so it’s not that you just disappear for half an hour.” (R1)
“Yeah I think if it came from the general management, about this well-being thing, or if it came from the team leaders, ‘I welcome you to do this’, I would do it.” (R7)
“Yeah I think that would make a difference to me if someone said, or my boss said, she said, ‘Yes I’ve done this and I found it positive’, it would make me more likely to take it up.” (R9)
“And yeah, I think if any line managers specifically talk and say they have done it, that would put me on. And also knowing your participation is not going to be logged in some way.” (R9)
“And I think, I think it would be better to hmm…work on the assumption that people who are going to attend somehow got the OK from their boss, rather than checking that it’s alright. I mean I wouldn’t sign up to a webinar without telling at least that I would be doing that at some point during my week. So hmm, yeah, I’ll check if I sign up to something and then rather than getting the message ‘A has sign up for this webinar on Thursday morning…’, it would be weird. I don’t think the management will find this useful.” (R8)
3.3.2. Subtheme: Work Demands
“The level of work, I think that’s the main thing. Yeah I think when you listen to the webinar, without doing your job, yeah I just think however good people’s intentions are to do it, it’s a lot for people to get involved with.” (R1)
“Work. If your boss or your team wants you to do something important, so, that would definitely put me off from doing it I think.” (R6)
4. Discussion
4.1. Principal Findings
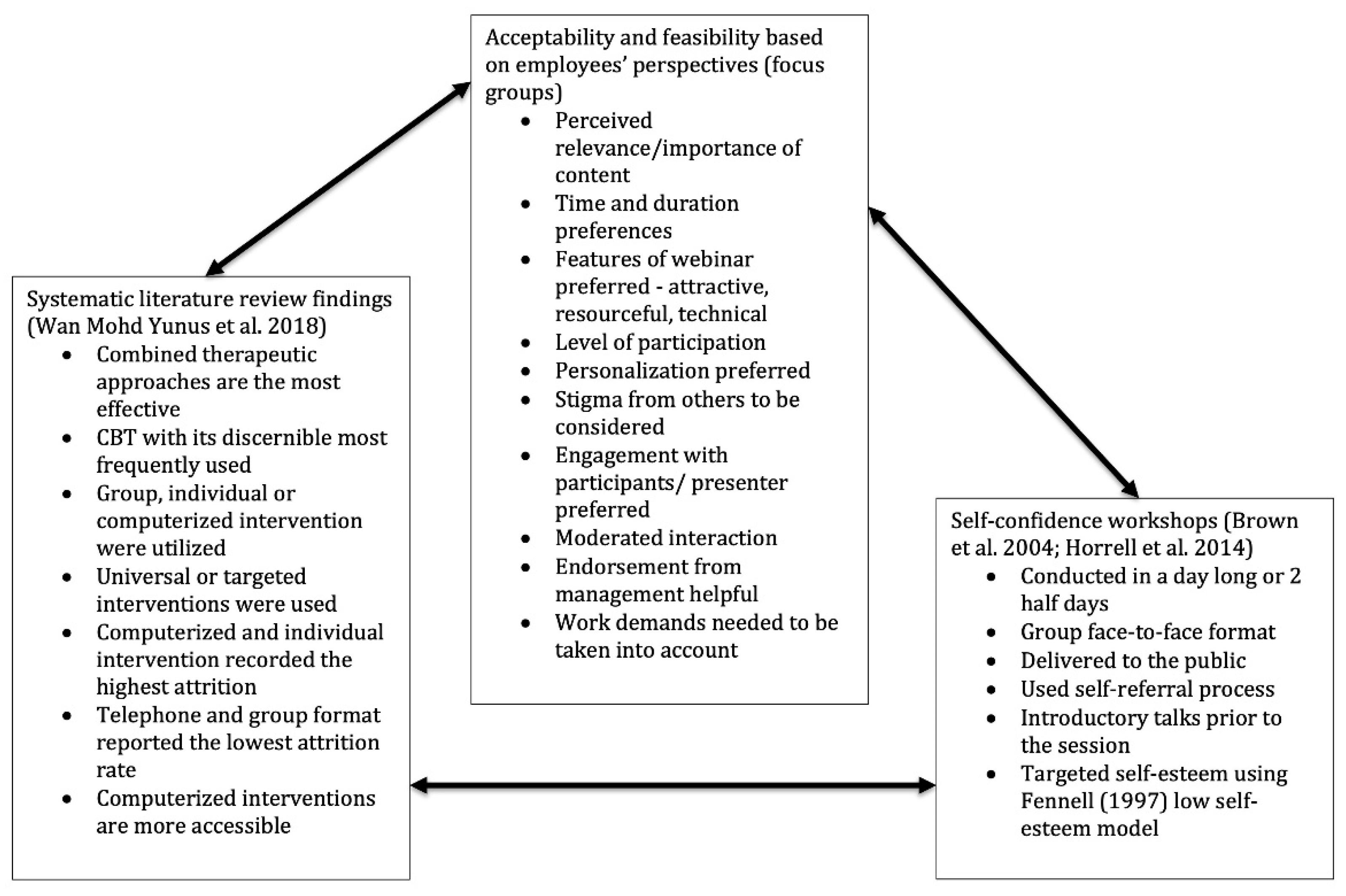
4.2. Intervention Development Process
4.2.1. Combined Therapeutic Approach
4.2.2. Duration and Number of Sessions
4.2.3. Universal or Targeted Intervention
4.2.4. Group or Individual Intervention?
4.2.5. The Importance of having Initial Face-to-Face Contact
4.2.6. The Need for a Moderator
4.3. Webinar Intervention Form and Structure
4.3.1. PowerPoint Presentations
4.3.2. Comics
4.3.3. Animation Videos
4.3.4. The “Interactive Zones”
- Panels were made available mostly during the “Interactive Zones” slides, when the responses from participants regarding a specific topic assigned by the webinar presenter were solicited.
- The responses by all participants were filtered and managed by the moderator and only credible responses were exhibited on the whiteboard.
- Participants were constantly prompted to maintain their concentration on the discussion theme.
4.3.5. Webcam
4.3.6. Homework and Post-Session Enquiries
4.4. Intervention Content
4.4.1. Introductory Meeting
4.4.2. Theoretical Basis of the Webinar Intervention
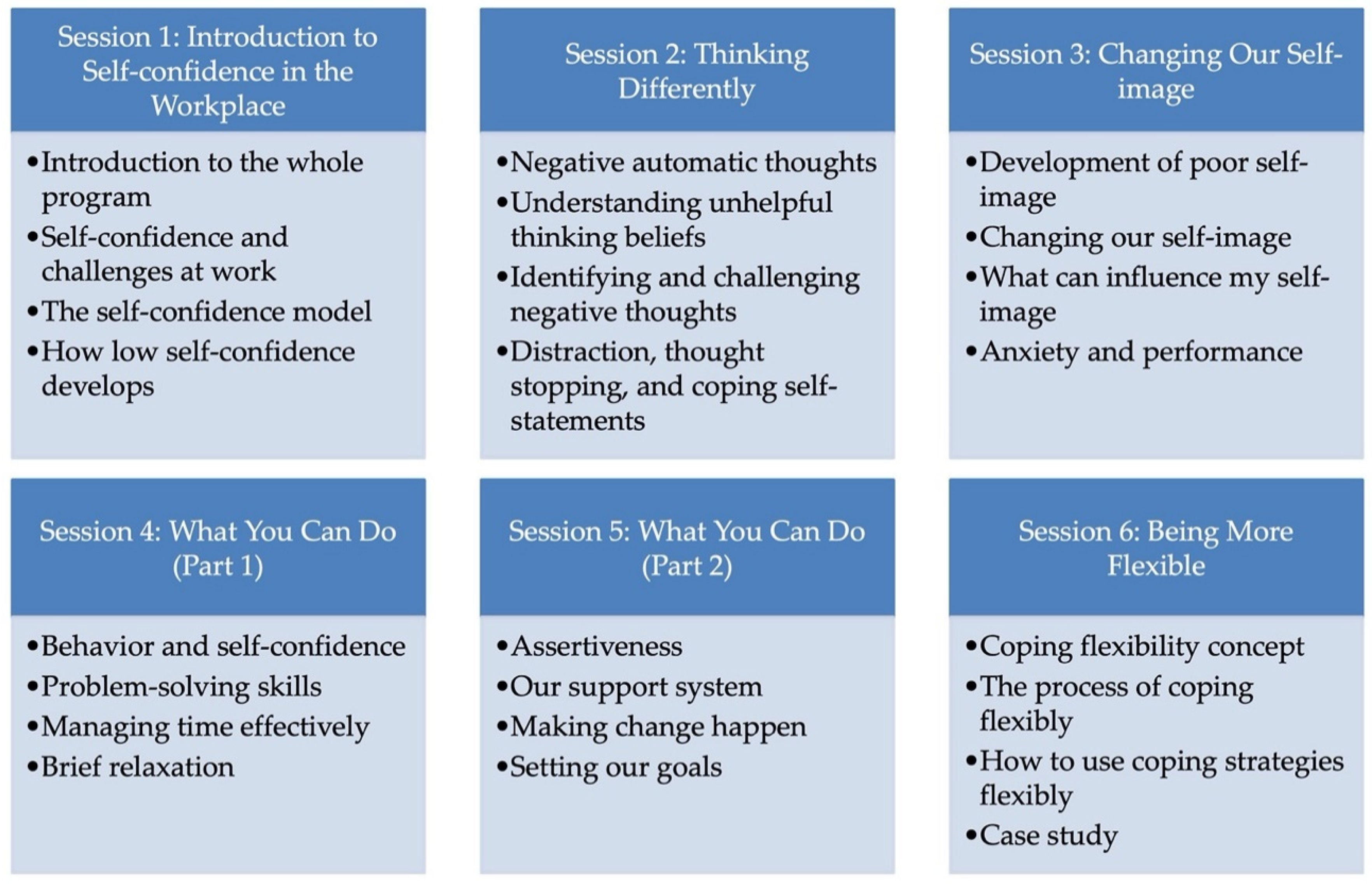
4.4.3. Intervention Sessions Summary
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Brown, J.S.L.; Cochrane, R.; Hancox, T. Large-scale health promotion stress workshops for the general public: A controlled evaluation. Behav. Cogn. Psychother. 2000, 28, 139–151. [Google Scholar] [CrossRef]
- Watkins, E.; Elliott, S.; Button, J.; Williams, R.; Brown, J.; Stanhope, N. Meeting the needs for psychological treatment of people with common mental disorders: An exploratory study. J. Ment. Health 2000, 9, 445–456. [Google Scholar] [CrossRef]
- Beck, A.T.; Rush, A.J.; Shaw, B.F.; Emery, G. Cognitive Therapy of Depression; The Guilford Press: New York, NY, USA, 1979. [Google Scholar]
- Brown, J.S.L.; Elliott, S.A.; Boardman, J.; Ferns, J.; Morrison, J. Meeting the unmet need for depression services with psycho-educational self-confidence workshops: Preliminary report. Br. J. Psychiatry 2004, 185, 511–515. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.S.L.; Elliott, S.A.; Boardman, J.; Andiappan, M.; Landau, S.; Howay, E. Can the effects of a 1-day CBT psychoeducational workshop on self-confidence be maintained after 2 years? A naturalistic study. Depress. Anxiety 2008, 25, 632–640. [Google Scholar] [CrossRef] [PubMed]
- Horrell, L.; Goldsmith, K.A.; Tylee, A.T.; Schmidt, U.H.; Murphy, C.L.; Bonin, E.M.; Beecham, J.; Kelly, J.; Raikundalia, S.; Brown, J.S.L. One-day cognitive-behavioural therapy self-confidence workshops for people with depression: Randomised controlled trial. Br. J. Psychiatry 2014, 204, 222–233. [Google Scholar] [CrossRef]
- Brown, J.S.L.; Boardman, J.; Elliott, S.A.; Howay, E.; Morrison, J. Are self-referrers just the worried well? Soc. Psychiatry Psychiatr. Epidemiol. 2005, 40, 396–401. [Google Scholar] [CrossRef]
- Campbell, M.; Fitzpatrick, R.; Haines, A.; Kinmonth, A.L.; Sandercock, P.; Spiegelhalter, D.; Tyrer, P. Framework for design and evaluation of complex interventions to improve health. BMJ 2000, 321, 694–696. [Google Scholar] [CrossRef]
- Craig, P.; Dieppe, P.; Macintyre, S.; Mitchie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337, 979–983. [Google Scholar] [CrossRef]
- Wan Mohd Yunus, W.M.A.; Musiat, P.; Brown, J.S.L. Systematic review of universal and targeted workplace interventions for depression. Occup. Environ. Med. 2018, 75, 66–75. [Google Scholar] [CrossRef]
- Moore, G.F.; Audrey, S.; Barker, M.; Bond, L.; Bonell, C.; Hardeman, W.; Moore, L.; O’Cathain, A.; Tinati, T.; Wight, D.; et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ Br. Med. J. 2015, 350, h1258. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Wilhide, C.; Hayes, J.R.; Farah, J.R. The use and influence of employee incentives on participation and throughput in a telephonic disease management program. Popul. Health Manag. 2008, 11, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.; Issakidis, C.; Hunt, C. Delay to seek treatment for anxiety and mood disorders in an Australian clinical sample. Behav. Chang. 2008, 25, 71–84. [Google Scholar] [CrossRef]
- Brouwer, W.; Oenema, A.; Crutzen, R.; de Nooijer, J.; de Vries, N.K.; Brug, J. What makes people decide to visit and use an internet-delivered behavior-change intervention?: A qualitative study among adults. Health Educ. 2009, 109, 460–473. [Google Scholar] [CrossRef]
- Petty, R.E.; Cacioppo, J.T.; Goldman, R. Personal Involvement as a Determinant of Argument-Based Persuasion. J. Personal. Soc. Psychol. 1981, 41, 847–855. [Google Scholar] [CrossRef]
- Office for National Statistics. UK Labour Market; Office for National Statistics: London, UK, 2016.
- Shain, M.; Suurvali, H. Investing in Comprehensive Workplace Health Promotion; Centre for Addiction and Mental Health (CAMH); The National Quality Institute (NQI): Toronto, ON, Canada, 2001. [Google Scholar]
- Danaher, B.G.; Jazdzewski, S.A.; McKay, H.G.; Hudson, C.R. Bandwidth constraints to using video and other rich media in behavior change websites. J. Med. Internet Res. 2005, 7. [Google Scholar] [CrossRef] [PubMed]
- Donker, T.; Griffiths, K.M.; Cuijpers, P.; Christensen, H. Psychoeducation for depression, anxiety and psychological distress: A meta-analysis. BMC Med. 2009, 7. [Google Scholar] [CrossRef]
- Nöhammer, E.; Schusterschitz, C.; Stummer, H. Determinants of employee participation in workplace health promotion. Int. J. Workplace Health Manag. 2010, 3, 97–110. [Google Scholar] [CrossRef]
- Johansson, R.; Sjöberg, E.; Sjögren, M.; Johnsson, E.; Carlbring, P.; Andersson, T.; Rousseau, A.; Andersson, G. Tailored vs. Standardized internet-based cognitive behavior therapy for depression and comorbid symptoms: A randomized controlled trial. PLoS ONE 2012, 7. [Google Scholar] [CrossRef]
- Brohan, E.; Thornicroft, G. Stigma and discrimination of mental health problems: Workplace implications. Occup. Med. 2010, 60, 414–415. [Google Scholar] [CrossRef]
- Haslam, C.; Brown, S.; Hastings, S.; Haslam, R. Effects of Prescribed Medication on Performance in the Working Population; Health and Safety Executive: London, UK, 2003.
- Kim, P.Y.; Thomas, J.L.; Wilk, J.E.; Castro, C.A.; Hoge, C.W. Stigma, Barriers to Care, and Use of Mental Health Services among Active Duty and National Guard Soldiers after Combat. Psychiatr. Serv. 2010, 61, 582–588. [Google Scholar] [CrossRef] [PubMed]
- Pendry, L.F.; Salvatore, J. Individual and social benefits of online discussion forums. Comput. Hum. Behav. 2015, 50, 211–220. [Google Scholar] [CrossRef]
- Davison, K.P.; Pennebaker, J.W.; Dickerson, S.S. Who talks? The social psychology of illness support groups. Am. Psychol. 2000, 55, 205–217. [Google Scholar] [CrossRef] [PubMed]
- Bargh, J.A.; McKenna, K.Y.A. The Internet and social life. Annu. Rev. Psychol. 2004, 55, 573–590. [Google Scholar] [CrossRef]
- Bargh, J.A.; McKenna, K.Y.A.; Fitzsimons, G.M. Can you see the real me? Activation and expression of the “true self” on the internet. J. Soc. Issues 2002, 58, 33–48. [Google Scholar] [CrossRef]
- White, M.; Dorman, S.M. Receiving social support online: Implications for health education. Health Educ. Res. 2001, 16, 693–707. [Google Scholar] [CrossRef]
- Kaplan, K.; Salzer, M.S.; Solomon, P.; Brusilovskiy, E.; Cousounis, P. Internet peer support for individuals with psychiatric disabilities: A randomized controlled trial. Soc. Sci. Med. 2011, 72, 54–62. [Google Scholar] [CrossRef]
- Weiner, B.J.; Lewis, M.A.; Linnan, L.A. Using organization theory to understand the determinants of effective implementation of worksite health promotion programs. Health Educ. Res. 2009, 24, 292–305. [Google Scholar] [CrossRef]
- Moll, S.E. The web of silence: A qualitative case study of early intervention and support for healthcare workers with mental ill-health. BMC Public Health 2014, 14. [Google Scholar] [CrossRef]
- Cheng, C.; Kogan, A.; Chio, J.H.M. The effectiveness of a new, coping flexibility intervention as compared with a cognitive-behavioural intervention in managing work stress. Work Stress 2012, 26, 272–288. [Google Scholar] [CrossRef]
- Baicker, K.; Cutler, D.; Song, Z. Workplace wellness programs can generate savings. Health Aff. (Millwood) 2010, 29. [Google Scholar] [CrossRef] [PubMed]
- Christensen, H.; Griffiths, K.M.; Mackinnon, A.J.; Brittliffe, K. Online randomized controlled trial of brief and full cognitive behaviour therapy for depression. Psychol. Med. 2006, 36, 1737–1746. [Google Scholar] [CrossRef] [PubMed]
- Christensen, H.; Griffiths, K.M.; Farrer, L. Adherence in internet interventions for anxiety and depression. J. Med. Internet Res. 2009, 11. [Google Scholar] [CrossRef] [PubMed]
- Melville, K.M.; Casey, L.M.; Kavanagh, D.J. Dropout from internet-based treatment for psychological disorders. Br. J. Clin. Psychol. 2010, 49, 455–471. [Google Scholar] [CrossRef] [PubMed]
- Ludden, G.D.S.; Van Rompay, T.J.L.; Kelders, S.M.; Van Gemert-Pijnen, J.E.W.C. How to increase reach and adherence of web-based interventions: A design research viewpoint. J. Med. Internet Res. 2015, 17. [Google Scholar] [CrossRef] [PubMed]
- Tan, L.; Wang, M.J.; Modini, M.; Joyce, S.; Mykletun, A.; Christensen, H.; Harvey, S.B. Preventing the development of depression at work: A systematic review and meta-analysis of universal interventions in the workplace. BMC Med. 2014, 12. [Google Scholar] [CrossRef]
- Quintiliani, L.; Sattelmair, J.; Sorensen, G. The Workplace as a Setting for Interventions to Improve Diet and Promote Physical Activity; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Burton, W.N.; Conti, D.J. Depression in the workplace: The role of the corporate medical director. J. Occup. Environ. Med. 2008, 50, 476–481. [Google Scholar] [CrossRef]
- Couser, G.P. Challenges and opportunities for preventing depression in the workplace: A review of the evidence supporting workplace factors and interventions. J. Occup. Environ. Med. 2008, 50, 411–427. [Google Scholar] [CrossRef]
- Walton, L. Exploration of the attitudes of employees towards the provision of counselling within a profit-making organisation. Couns. Psychother. Res. 2003, 3, 65–71. [Google Scholar] [CrossRef]
- De Vente, W.; Kamphuis, J.H.; Emmelkamp, P.M.G.; Blonk, R.W.B. Individual and Group Cognitive-Behavioral Treatment for Work-Related Stress Complaints and Sickness Absence: A Randomized Controlled Trial. J. Occup. Health Psychol. 2008, 13, 214–231. [Google Scholar] [CrossRef]
- Tucker, M.; Oei, T.P.S. Is group more cost effective than individual cognitive behaviour therapy? The evidence is not solid yet. Behav. Cogn. Psychother. 2007, 35, 77–91. [Google Scholar] [CrossRef]
- Brown, J.S.L.; Sellwood, K.; Beecham, J.K.; Slade, M.; Andiappan, M.; Landau, S.; Johnson, T.; Smith, R. Outcome, costs and patient engagement for group and individual CBT for depression: A naturalistic clinical study. Behav. Cogn. Psychother. 2011, 39, 355–358. [Google Scholar] [CrossRef] [PubMed]
- Newman, M.G.; Szkodny, L.E.; Llera, S.J.; Przeworski, A. A review of technology-assisted self-help and minimal contact therapies for drug and alcohol abuse and smoking addiction: Is human contact necessary for therapeutic efficacy? Clin. Psychol. Rev. 2011, 31, 178–186. [Google Scholar] [CrossRef] [PubMed]
- Wan Mohd Yunus, W.M.A.; Musiat, P.; Brown, J.S.L. Evaluating the feasibility of an innovative self-confidence webinar intervention for depression in the workplace: A proof-of-concept study. JMIR Ment. Health 2019, 6. [Google Scholar] [CrossRef] [PubMed]
- Hosler, J.; Boomer, K.B. Are comic books an effectiveway to engage nonmajors in learning and appreciating science? CBE Life Sci. Educ. 2011, 10, 309–317. [Google Scholar] [CrossRef]
- Kishi, Y.; Matsumura, T.; Murishige, N.; Kodama, Y.; Hatanaka, N.; Takita, M.; Sakamoto, K.; Hamaki, T.; Kusumi, E.; Kobayashi, K.; et al. Internet-Based Survey on Medical Manga in Japan. Health Commun. 2011, 26, 676–678. [Google Scholar] [CrossRef]
- Green, M.J.; Myers, K.R. Graphic medicine: Use of comics in medical education and patient care. BMJ 2010, 340, c863. [Google Scholar] [CrossRef]
- Imamura, K.; Kawakami, N.; Furukawa, T.A.; Matsuyama, Y.; Shimazu, A.; Umanodan, R.; Kawakami, S.; Kasai, K. Effects of an internet-based cognitive behavioral therapy (iCBT) program in manga format on improving subthreshold depressive symptoms among healthy workers: A randomized controlled trial. PLoS ONE 2014, 9. [Google Scholar] [CrossRef]
- Andersson, G.; Titov, N. Advantages and limitations of Internet-based interventions for common mental disorders. World Psychiatry 2014, 13, 4–11. [Google Scholar] [CrossRef]
- Sweller, J. Cognitive load during problem solving: Effects on learning. Cogn. Sci. 1988, 12, 257–285. [Google Scholar] [CrossRef]
- Marques, J.C.; Quintela, J.; Restivo, M.T.; Trigo, V. The use of video clips in engineering education. In Proceedings of the 2012 15th International Conference on Interactive Collaborative Learning (ICL), Villach, Austria, 26–28 September 2012. [Google Scholar]
- Pan, G.; Sen, S.; David, A.; Bonk, S.; Rodgers, M.L.; Tikoo, M.; Powell, D.V. Instructor-Made Videos as a Learner Scaffolding Tool. MERLOT J. Online Learn. Teach. 2012, 8, 298. [Google Scholar]
- Zhang, D.; Zhou, L.; Briggs, R.O.; Nunamaker, J.F., Jr. Instructional video in e-learning: Assessing the impact of interactive video on learning effectiveness. Inf. Manag. 2006, 43, 15–27. [Google Scholar] [CrossRef]
- Yadav, A.; Phillips, M.M.; Lundeberg, M.A.; Koehler, M.J.; Hilden, K.; Dirkin, K.H. If a picture is worth a thousand words is video worth a million? Differences in affective and cognitive processing of video and text cases. J. Comput. High. Educ. 2011, 23, 15–37. [Google Scholar] [CrossRef]
- Stratton, M.T.; Julien, M.; Schaffer, B. GoAnimate. J. Manag. Educ. 2014, 38, 282–289. [Google Scholar] [CrossRef]
- Heisler, J.M.; Crabill, S.L. Who are stinkybug and packerfan4? Email pseudonyms and participants’ perceptions of demography, productivity, and personality. J. Comput. Mediat. Commun. 2006, 12, 114–135. [Google Scholar] [CrossRef]
- Gerrits, R.S.; van der Zanden, R.A.P.; Visscher, R.F.M.; Conijn, B.P. Master your mood online: A preventive chat group intervention for adolescents. Aust. e-J. Adv. Ment. Health 2007, 6, 152–162. [Google Scholar] [CrossRef]
- Rhodes, S.D.; Hergenrather, K.C.; Duncan, J.; Vissman, A.T.; Miller, C.; Wilkin, A.M.; Stowers, J.; Eng, E. A pilot intervention utilizing Internet chat rooms to prevent HIV risk behaviors among men who have sex with men. Public Health Rep. 2010, 125, 29–37. [Google Scholar] [CrossRef]
- Zabinski, M.F.; Wilfley, D.E.; Calfas, K.J.; Winzelberg, A.J.; Taylor, C.B. An interactive psychoeducational intervention for women at risk of developing an eating disorder. J. Consult. Clin. Psychol. 2004, 72, 914–919. [Google Scholar] [CrossRef]
- Winzelberg, A.J.; Eppstein, D.; Eldredge, K.L.; Wilfley, D.; Dasmahapatra, R.; Dev, P.; Taylor, C.B. Effectiveness of an Internet-based program for reducing risk factors for eating disorders. J. Consult. Clin. Psychol. 2000, 68, 346–350. [Google Scholar] [CrossRef]
- Bull, S.S.; McFarlane, M.; King, D. Barriers to STD/HIV prevention on the internet. Health Educ. Res. 2001, 16, 661–670. [Google Scholar] [CrossRef]
- Çamtepe, A.; Krishnamoorthy, M.S.; Yener, B. A tool for internet chatroom surveillance. In Lecture Notes in Computer Science (Including Subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics); Springer: Berlin/Heidelberg, Germany, 2004; Volume 3073, pp. 252–265. [Google Scholar]
- Day, S.X.; Schneider, P.L. Psychotherapy using distance technology: A comparison of face-to-face, video, and audio treatment. J. Couns. Psychol. 2002, 49, 499–503. [Google Scholar] [CrossRef]
- Fennell, M. Overcoming Low Self-Esteem: A Self-Help Guide Using Cognitive Behavioural Techniques; Robinson: London, UK, 1999. [Google Scholar]
- Beck, A.T.; Emery, G.; Greenberg, R. Anxiety Disorders and Phobias: A Cognitive Perspective; Basic Books: New York, NY, USA, 1985. [Google Scholar]
- Cheng, C. Assessing coping flexibility in real-life and laboratory settings: A multimethod approach. J. Personal. Soc. Psychol. 2001, 80, 814–833. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Topic Guide |
|---|
| 1. Has anyone heard of webinars? Explain. 2. When do you think is the best time to conduct this webinar? Where? How long? 3. Are there any other important aspects that need to be considered to improve webinar acceptance in the workplace? 4. What could hinder employees from taking part in the webinar intervention? 5. How could this be improved? 6. Supposed you had one minute to explain what a good workplace intervention is. What would you say? |
| Demographics | ||
|---|---|---|
| Age (years old) | Range | 23–32 |
| Median | 26 | |
| Gender | Female | 9 (90%) |
| Male | 1 (10%) | |
| Ethnicity | English/Welsh/Scottish/Northern Irish | 9 (90%) |
| Others—Australian | 1 (10%) |
| Themes | Subthemes |
|---|---|
| Personal | Content |
| Time and duration preference | |
| Features of webinar | |
| Individual participation | |
| Personalization | |
| Interpersonal | Stigma from others |
| Engagement with participants/presenter | |
| Moderated interaction | |
| Stigma from others | |
| Organizational | Endorsement from management |
| Work demand |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wan Mohd Yunus, W.M.A.; Musiat, P.; Brown, J.S.L. Innovative Self-Confidence Webinar Intervention for Depression in the Workplace: A Focus Group Study and Systematic Development. Behav. Sci. 2020, 10, 193. https://doi.org/10.3390/bs10120193
Wan Mohd Yunus WMA, Musiat P, Brown JSL. Innovative Self-Confidence Webinar Intervention for Depression in the Workplace: A Focus Group Study and Systematic Development. Behavioral Sciences. 2020; 10(12):193. https://doi.org/10.3390/bs10120193
Chicago/Turabian StyleWan Mohd Yunus, Wan Mohd Azam, Peter Musiat, and June S. L. Brown. 2020. "Innovative Self-Confidence Webinar Intervention for Depression in the Workplace: A Focus Group Study and Systematic Development" Behavioral Sciences 10, no. 12: 193. https://doi.org/10.3390/bs10120193
APA StyleWan Mohd Yunus, W. M. A., Musiat, P., & Brown, J. S. L. (2020). Innovative Self-Confidence Webinar Intervention for Depression in the Workplace: A Focus Group Study and Systematic Development. Behavioral Sciences, 10(12), 193. https://doi.org/10.3390/bs10120193