Effectiveness of a Two-Step Testing Algorithm for Reliable and Cost-Effective Detection of Clostridium difficile Infection in a Tertiary Care Hospital in Saudi Arabia

Abstract
1. Introduction
2. Materials and Methods
2.1. Clinical Specimens
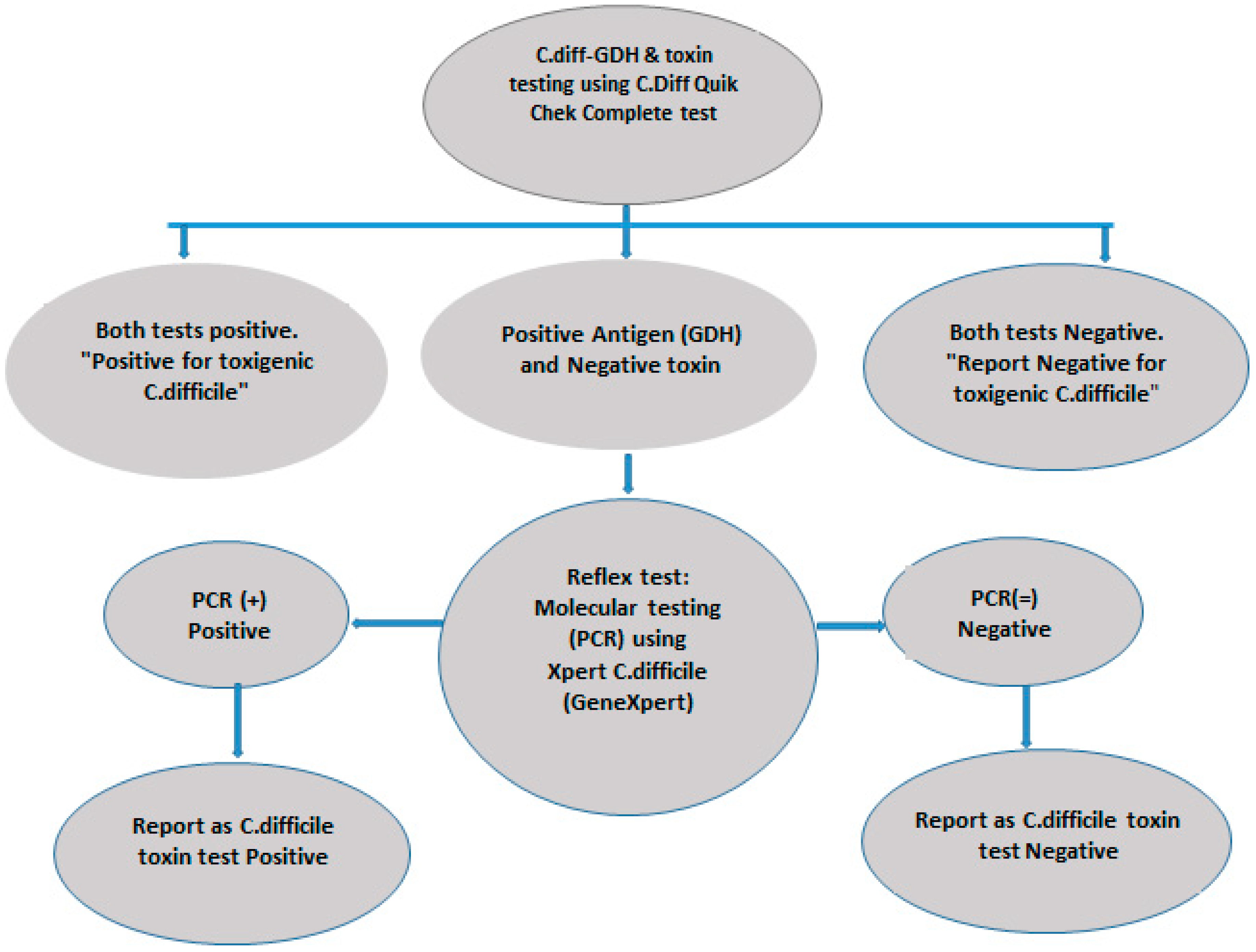
2.2. C. difficile Antigen and Toxin Assays
2.3. Xpert C. difficile PCR Assay
2.4. Data Analysis
3. Results
3.1. Phase 1
3.2. Phase 2
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Lessa, F.C.; Mu, Y.; Bamberg, W.M.; Beldavs, Z.G.; Dumyati, G.K.; Dunn, J.R.; Farley, M.M.; Holzbauer, S.M.; Meek, J.I.; Phipps, E.C.; et al. Burden of Clostridium difficile infection in the United States. N. Engl. J. Med. 2015, 372, 825–834. [Google Scholar] [CrossRef] [PubMed]
- Polage, C.R.; Solnick, J.V.; Cohen, S.H. Nosocomial Diarrhea: Evaluation and Treatment of Causes Other Than Clostridium difficile. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2012, 55, 982–989. [Google Scholar] [CrossRef] [PubMed]
- Titov, L.; Lebedkova, N.; Shabanov, A.; Tang, Y.J.; Cohen, S.H.; Silva, J. Isolation and Molecular Characterization of Clostridium difficile Strains from Patients and the Hospital Environment in Belarus. J. Clin. Microbiol. 2000, 38, 1200–1202. [Google Scholar] [PubMed]
- Martin, J.S.; Monaghan, T.M.; Wilcox, M.H. Clostridium difficile infection: Epidemiology, diagnosis and understanding transmission. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 206–216. [Google Scholar] [CrossRef] [PubMed]
- Oldfield, E.C., IV; Oldfield, E.C., III; Johnson, D.A. Clinical update for the diagnosis and treatment of Clostridium difficile infection. World J. Gastrointest. Pharmacol. Ther. 2014, 5, 1–26. [Google Scholar] [PubMed]
- Tonna, I.; Welsby, P.D. Pathogenesis and treatment of Clostridium difficile infection. Postgrad. Med. J. 2005, 81, 367–369. [Google Scholar] [CrossRef] [PubMed]
- Sayedy, L.; Kothari, D.; Richards, R.J. Toxic megacolon associated Clostridium difficile colitis. World J. Gastrointest. Endosc. 2010, 2, 293–297. [Google Scholar] [CrossRef]
- Swindells, J.; Brenwald, N.; Reading, N.; Oppenheim, B. Evaluation of diagnostic tests for Clostridium difficile infection. J. Clin. Microbiol. 2010, 48, 606–608. [Google Scholar] [CrossRef]
- Cohen, S.H.; Gerding, D.N.; Johnson, S.; Kelly, C.P.; Loo, V.G.; McDonald, L.C.; Pepin, J.; Wilcox, M.H. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the society for healthcare epidemiology of America [SHEA] and the infectious diseases society of America [IDSA]. Infect. Control Hosp. Epidemiol. 2010, 31, 431–455. [Google Scholar] [CrossRef]
- McDonald, L.C.; Gerding, D.N.; Johnson, S.; Bakken, J.S.; Carroll, K.C.; Coffin, S.E.; Dubberke, E.R.; Garey, K.W.; Gould, C.V.; Kelly, C.; et al. Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America [IDSA] and Society for Healthcare Epidemiology of America [SHEA]. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2018, 66, e1–e48. [Google Scholar] [CrossRef]
- Shetty, N.; Wren, M.; Coen, P. The role of glutamate dehydrogenase for the detection of Clostridium difficile in faecal samples: A meta-analysis. J. Hosp. Infect. 2011, 77, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Fenner, L.; Widmer, A.F.; Goy, G.; Rudin, S.; Frei, R. Rapid and reliable diagnostic algorithm for detection of Clostridium difficile. J. Clin. Microbiol. 2008, 46, 328–330. [Google Scholar] [CrossRef] [PubMed]
- Avila, M.B.; Avila, N.P.; Dupont, A.W. Recent Advances in the Diagnosis and Treatment of Clostridium Difficile Infection. F1000Research 2016, 5. [Google Scholar] [CrossRef] [PubMed]
- Umscheid, C.A.; Mitchell, M.D.; Doshi, J.A.; Agarwal, R.; Williams, K.; Brennan, P.J. Estimating the Proportion of Healthcare-Associated Infections That Are Reasonably Preventable and the Related Mortality and Costs. Infect. Control Hosp. Epidemiol. 2015, 32, 101–114. [Google Scholar] [CrossRef] [PubMed]
- McGlone, S.M.; Bailey, R.R.; Zimmer, S.M.; Popovich, M.J.; Tian, Y.; Ufberg, P.; Muder, R.R.; Lee, B.Y. The economic burden of Clostridium difficile. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2012, 18, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Vindigni, S.M.; Surawicz, C.M. C. difficile Infection: Changing Epidemiology and Management Paradigms. Clin. Trans. Gastroenterol. 2015, 6, e99. [Google Scholar] [CrossRef] [PubMed]
- Carroll, K.C. Tests for the diagnosis of Clostridium difficile infection: The next generation. Anaerobe 2011, 17, 170–174. [Google Scholar] [CrossRef]
- Kufelnicka, A.M.; Kirn, T.J. Effective utilization of evolving methods for the laboratory diagnosis of Clostridium difficile infection. Clin. Infect. Dis. 2011, 52, 1451–1457. [Google Scholar] [CrossRef]
- Culbreath, K.; Ager, E.; Nemeyer, R.J.; Kerr, A.; Gilligan, P.H. Evolution of testing algorithms at a university hospital for detection of Clostridium difficile infections. J. Clin. Microbiol. 2012, 50, 3073–3076. [Google Scholar] [CrossRef]
- Qutub, M.O.; AlBaz, N.; Hawken, P.; Anoos, A. Comparison between the two-step and the three-step algorithms for the detection of toxigenic Clostridium difficile. Indian J. Med. Microbiol. 2011, 29, 293–296. [Google Scholar] [CrossRef]
- Khanna, S.; Pardi, D.S. The growing incidence and severity of Clostridium difficile infection in inpatient and outpatient settings. Expert Rev. Gastroenterol. Hepatol. 2010, 4, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Kato, H.; Kato, N.; Watanabe, K.; Iwai, N.; Nakamura, H.; Yamamoto, T.; Suzuki, K.; Kim, S.M.; Chong, Y.; Wasito, E.B. Identification of toxin A-negative, toxin B-positive Clostridium difficile by PCR. J. Clin. Microbiol. 1998, 36, 2178–2182. [Google Scholar] [PubMed]
- Quinn, C.D.; Sefers, S.E.; Babiker, W.; He, Y.; Alcabasa, R.; Stratton, C.W.; Carroll, K.C.; Tang, Y.W. C. Diff Quik Chek Complete Enzyme Immunoassay Provides a Reliable First-Line Method for Detection of Clostridium difficile in Stool Specimens. J. Clin. Microbiol. 2010, 48, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Sharp, S.E.; Ruden, L.O.; Pohl, J.C.; Hatcher, P.A.; Jayne, L.M.; Ivie, W.M. Evaluation of the C.Diff Quik Chek Complete Assay, a New Glutamate Dehydrogenase and A/B Toxin Combination Lateral Flow Assay for Use in Rapid, Simple Diagnosis of Clostridium difficile Disease. J. Clin. Microbiol. 2010, 48, 2082–2086. [Google Scholar] [CrossRef] [PubMed]
- Luna, R.A.; Boyanton, B.L.; Mehta, S.; Courtney, E.M.; Webb, C.R.; Revell, P.A.; Versalovic, J. Rapid Stool-Based Diagnosis of Clostridium difficile Infection by Real-Time PCR in a Children’s Hospital. J. Clin. Microbiol. 2011, 49, 851–857. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.Y.; Jeong, J.H.; Kim, K.H.; Ahn, J.Y.; Park, P.W.; Seo, Y.H. Laboratory diagnosis of Clostridium difficile infection: Comparison of Techlab C. diff Quik Chek Complete, Xpert C. difficile, and multistep algorithmic approach. J. Clin. Lab. Anal. 2017, 31, e22135. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.S.; Lee, M. Evaluation of the performance of C. DIFF QUIK CHEK COMPLETE and its usefulness in a hospital setting with a high prevalence of Clostridium difficile infection. J. Investig. Med. Off. Publ. Am. Fed. Clin. Res. 2017, 65, 88–92. [Google Scholar]
- Martínez-Meléndez, A.; Camacho-Ortiz, A.; Morfin-Otero, R.; Maldonado-Garza, H.J.; Villarreal-Treviño, L.; Garza-González, E. Current knowledge on the laboratory diagnosis of Clostridium difficile infection. World J. Gastroenterol. 2017, 23, 1552–1567. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Xpert C. difficile PCR | Sensitivity | Specificity | PPV | NPV | |||
|---|---|---|---|---|---|---|---|
| Positive | Negative | % | % | % | % | ||
| Quik Chek | Positive | 7 | 0 | ||||
| 46.7 | 100 | 100 | 91.7 | ||||
| Complete EIA | Negative | 8 * | 88 | ||||
| 95% Confidence interval | (21.3–73.4%) | (95.9–100%) | 100% | (87.3–94.6%) | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qutub, M.; Govindan, P.; Vattappillil, A. Effectiveness of a Two-Step Testing Algorithm for Reliable and Cost-Effective Detection of Clostridium difficile Infection in a Tertiary Care Hospital in Saudi Arabia. Med. Sci. 2019, 7, 6. https://doi.org/10.3390/medsci7010006
Qutub M, Govindan P, Vattappillil A. Effectiveness of a Two-Step Testing Algorithm for Reliable and Cost-Effective Detection of Clostridium difficile Infection in a Tertiary Care Hospital in Saudi Arabia. Medical Sciences. 2019; 7(1):6. https://doi.org/10.3390/medsci7010006
Chicago/Turabian StyleQutub, Mohammed, Prasanth Govindan, and Anupama Vattappillil. 2019. "Effectiveness of a Two-Step Testing Algorithm for Reliable and Cost-Effective Detection of Clostridium difficile Infection in a Tertiary Care Hospital in Saudi Arabia" Medical Sciences 7, no. 1: 6. https://doi.org/10.3390/medsci7010006
APA StyleQutub, M., Govindan, P., & Vattappillil, A. (2019). Effectiveness of a Two-Step Testing Algorithm for Reliable and Cost-Effective Detection of Clostridium difficile Infection in a Tertiary Care Hospital in Saudi Arabia. Medical Sciences, 7(1), 6. https://doi.org/10.3390/medsci7010006