Should Mumps Be Higher Up on the Public Health Agenda in India? A Concern for Global Health Security



Abstract
1. Introduction
2. Methodology
2.1. Disease Surveillance in India
2.2. Universal Immunization Programme of India
2.3. Arguments against Vaccination
2.4. Integrated Disease Surveillance Programme and Mumps
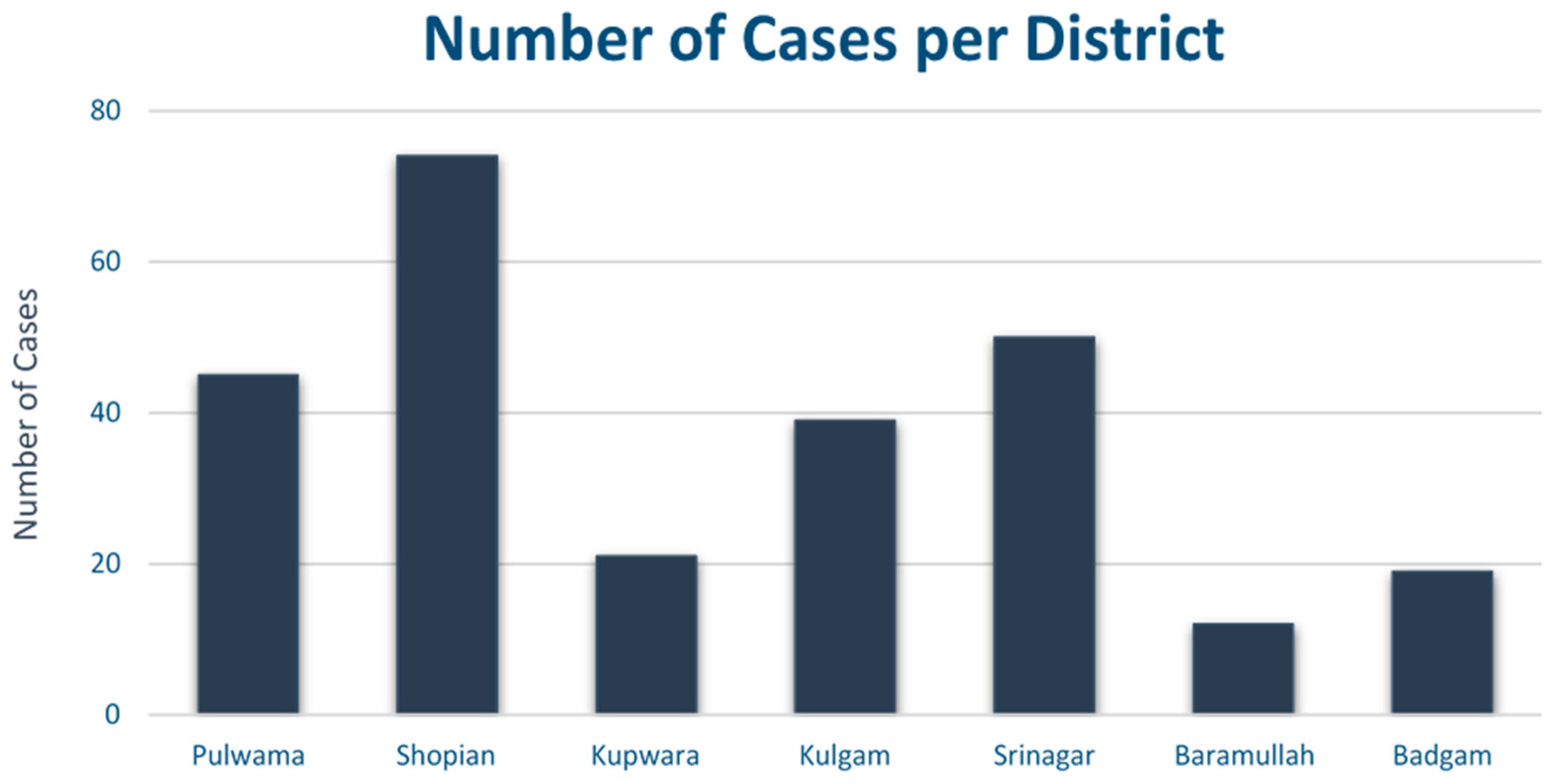
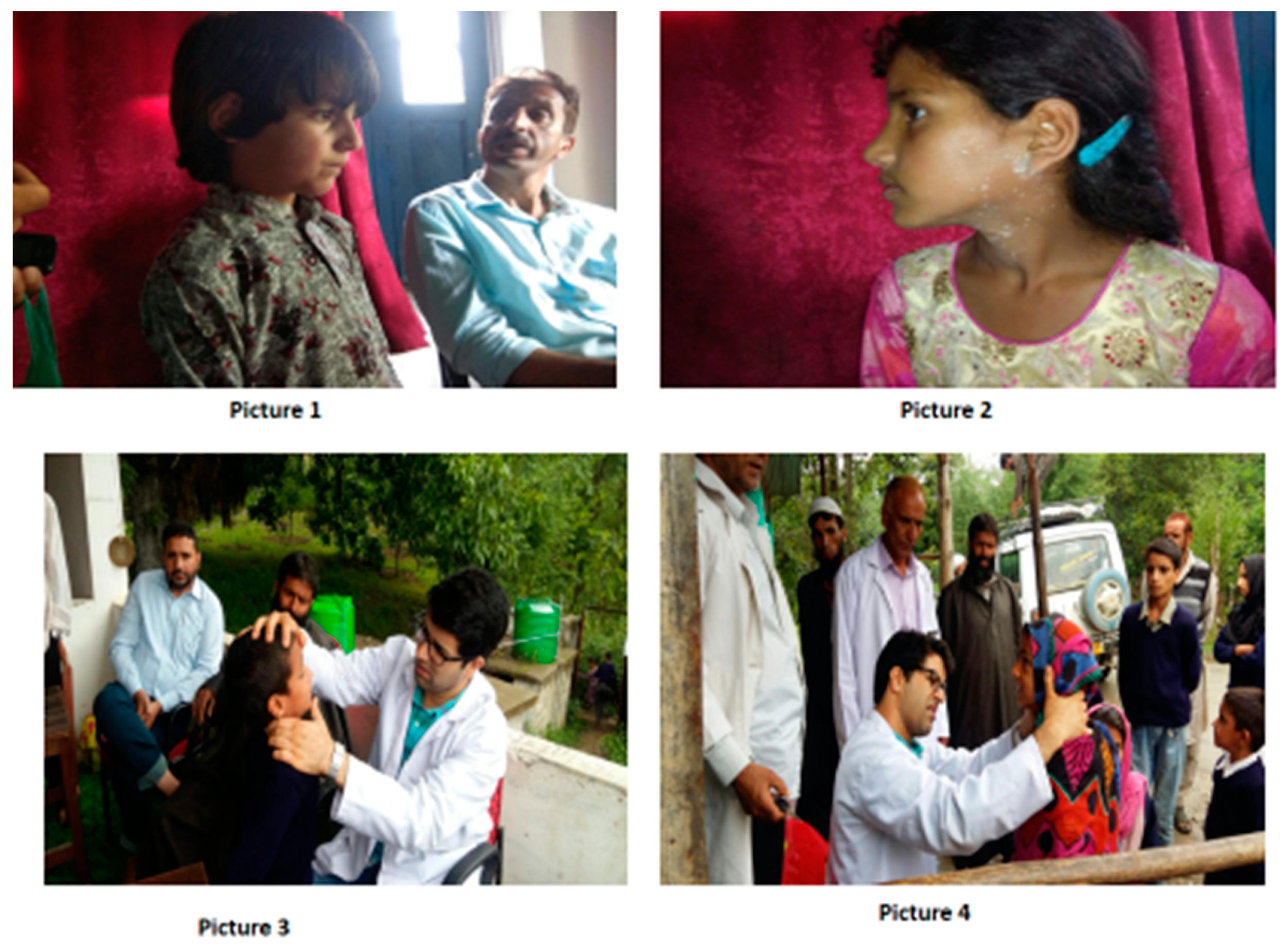
2.5. Mumps Outbreak and Indepth Analysis of Shopian District
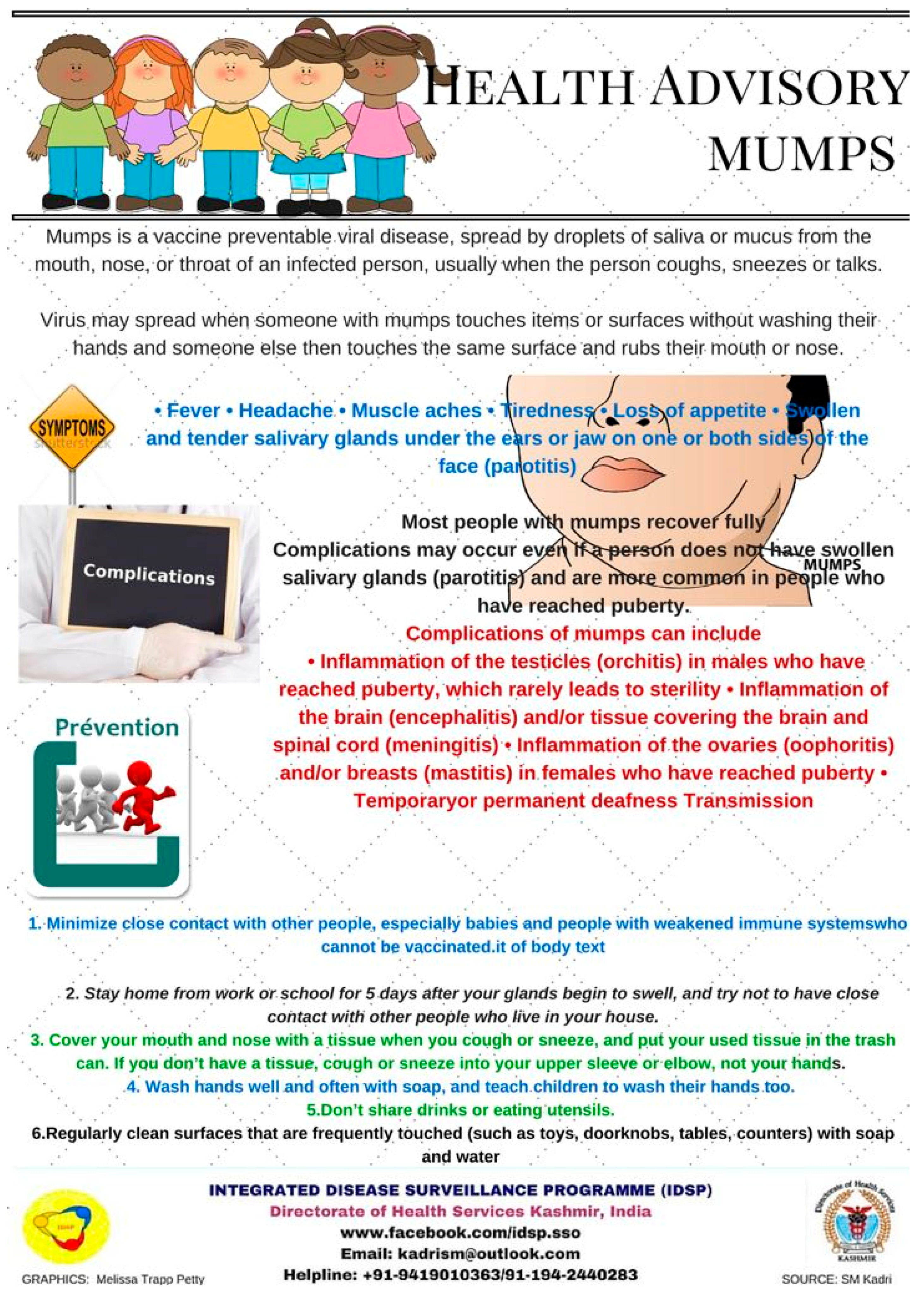
- Keep affected children isolated from gathering.
- Wash hands thoroughly with soap.
- Keep affected children at home for five days and avoid close contact with others in house.
3. Discussion
3.1. Global Scenario
3.2. Issues of Global Health Security
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Universal Immunization Programme (UIP), National Health Portal of India. Available online: https://www.nhp.gov.in/universal-immunisation-programme_pg (accessed on 29 December 2017).
- Signs & Symptoms of Mumps, Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/mumps/about/signs-symptoms.html (accessed on 29 December 2017).
- Mumps Vaccination, Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/mumps/vaccination.html (accessed on 29 December 2017).
- Indian Academy of Pediatrics (IAP). Available online: https://www.iapindia.org/immunization-schedule-for-children-aged-0-through-18-years/ (accessed on 2 August 2018).
- IDSP: Integrated Disease Surveillance Programme. Available online: https://www.dhskashmir.org/pdf/IDSP%20Annual%20Report%202017.pdf (accessed on 30 July 2018).
- The Universal Immunization Programme in India, Centre for Public Impact. Available online: https://www.centreforpublicimpact.org/case-study/universal-immunization-program-india/ (accessed on 29 December 2017).
- Vashishtha, V.M.; Yadav, S.; Dabas, A.; Bansal, C.P.; Agarwal, R.C.; Yewale, V.N.; Thacker, N.; Kamath, S.S.; Mehta, P.J. IAP position paper on burden of mumps in India and vaccination strategies. Indian Pediatr. 2015, 52, 505–514. [Google Scholar] [CrossRef] [PubMed]
- Zamir, C.S.; Schroeder, H.; Shoob, H.; Abramson, N.; Zentner, G. Characteristics of a large mumps outbreak: Clinical severity, complications and association with vaccination status of mumps outbreak cases. Hum. Vaccin. Immunother. 2015, 11, 1413–1417. [Google Scholar] [CrossRef] [PubMed]
- Aasheim, E.T.; Inns, T.; Trindall, A.; Emmett, L.; Brown, K.E.; Williams, C.J.; Reacher, M. Outbreak of mumps in a school setting, United Kingdom, 2013. Hum. Vaccin. Immunother. 2014, 10, 2446–2449. [Google Scholar] [CrossRef] [PubMed]
- Vygen, S.; Fischer, A.; Meurice, L.; Mounchetrou Njoya, I.; Gregoris, M.; Ndiaye, B.; Ghenassia, A.; Poujol, I.; Stahl, J.P.; Antona, D.; et al. Waning immunity against mumps in vaccinated young adults, France 2013. Euro Surveill. 2016, 21, 12–19. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO-Recommended Surveillance Standard of Mumps. Available online: http://www.who.int/immunization/monitoring_surveillance/burden/vpd/surveillance_type/passive/mumps_standards/en/ (accessed on 29 December 2017).
- Quinlisk, M.P. Mumps Control Today. J. Infect. Dis. 2010, 202, 655–656. [Google Scholar] [CrossRef] [PubMed]
- Levine, H.; Zarka, S.; Ankol, O.E.; Rozhavski, V.; Davidovitch, N.; Aboudy, Y.; Balicer, R.D. Seroprevalence of measles, mumps and rubella among young adults, after 20 years of universal 2-dose MMR vaccination in Israel. Hum. Vaccin. Immunother. 2015, 11, 1400–1405. [Google Scholar] [CrossRef] [PubMed]
- Janaszek-Seydlitz, W.; Bucholc, B.; Gorska, P.; Slusarczyk, J. Mumps in Poland since 1990 to 2003; epidemiology and antibody prevalence. Vaccine 2005, 23, 2711–2716. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Immunization, Vaccines and Biologicals. Mumps. Available online: http://www.who.int/immunization/diseases/mumps/en/ (accessed on 29 December 2017).
- Rise in Mumps Outbreaks Prompts U.S. Panel to Endorse 3rd Vaccine Dose. The Washington Post. Available online: https://www.washingtonpost.com/news/to-your-health/wp/2017/10/25/rise-in-mumps-outbreaks-prompts-u-s-panel-to-endorse-3rd-vaccine-dose/?utm_term=.d94ae5b40249 (accessed on 25 May 2018).
- Flahault, A.; Wernli, D.; Zylberman, P.; Tanner, M. From global health security to global health solidarity, security and sustainability. Bull. World Health Organ. 2016, 94. [Google Scholar] [CrossRef] [PubMed]
- Chattu, V.K.; Kumar, R.; Kumary, S.; Kajal, F.; David, J.K. Nipah virus epidemic in southern India and emphasizing “One Health” approach to ensure global health security. J. Fam. Med. Prim. Care 2018, 7, 275–287. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Vaccination | Timing |
|---|---|
| Bacillus Calmette–Guerin | One dose at birth (up to one year if not given earlier) |
| Diphtheria, pertussis, tetanus toxoid | Five doses; three primary doses at 6, 10 and 14 weeks and two booster doses at 16–24 months and 5 years of age |
| Oral polio vaccine | Five doses; zero doses at birth, three primary doses at 6, 10 and 14 weeks and one booster at 16–24 months of age |
| Hepatitis B vaccine | Four doses; zero doses within 24 h of birth and three doses at 6, 10 and 14 weeks of age |
| Measles | Two doses; first dose at 9–12 months and second dose at 16–24 months of age |
| Tetanus toxoid | Two doses at 10 years and 16 years of age |
| Outbreak Number | Date of Occurrence | District | Village Affected | Number of Cases |
|---|---|---|---|---|
| 1 | 17 July 2017 | Pulwana | Lasidaban | 10 |
| 2 | 24 July 2017 | Shopian | Naserpora | 25 |
| 3 | 27 July 2017 | Shopian | Tukroo | 11 |
| 4 | 15 August 2017 | Shopian | Pinjoora | 20 |
| 5 | 21 August 2017 | Kupwara | Bowan Zachaldar | 21 |
| 6 | 22 August 2017 | Pulwama | Abhama | 20 |
| 7 | 25 August 2017 | Kulgam | Lirrow | 7 |
| 8 | 26 August 2017 | Pulwama | Dogripora | 7 |
| 9 | 27 August 2017 | Pulwama | Wahipora | 8 |
| 10 | 28 August 2017 | Shopian | Harman Nildoora | 8 |
| 11 | 28 August 2017 | Srinagar | Govt Middle School, Khawja Bagh Maloora | 50 |
| 12 | 7 August 2017 | Baramullah | Sheeri Najibhat | 12 |
| 13 | 15 September 2017 | Shopian | Batpora | 10 |
| 14 | 16 September 2017 | Kulgam | Yaripora | 32 |
| 15 | 16 September 2017 | Badgam | Babapora | 19 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kadri, S.M.; Rehman, S.-u.; Rehana, K.; Brady, A.H.; Chattu, V.K. Should Mumps Be Higher Up on the Public Health Agenda in India? A Concern for Global Health Security. Med. Sci. 2018, 6, 62. https://doi.org/10.3390/medsci6030062
Kadri SM, Rehman S-u, Rehana K, Brady AH, Chattu VK. Should Mumps Be Higher Up on the Public Health Agenda in India? A Concern for Global Health Security. Medical Sciences. 2018; 6(3):62. https://doi.org/10.3390/medsci6030062
Chicago/Turabian StyleKadri, Syed Manzoor, Saleem-ur Rehman, Kausar Rehana, Ailbhe Helen Brady, and Vijay Kumar Chattu. 2018. "Should Mumps Be Higher Up on the Public Health Agenda in India? A Concern for Global Health Security" Medical Sciences 6, no. 3: 62. https://doi.org/10.3390/medsci6030062
APA StyleKadri, S. M., Rehman, S.-u., Rehana, K., Brady, A. H., & Chattu, V. K. (2018). Should Mumps Be Higher Up on the Public Health Agenda in India? A Concern for Global Health Security. Medical Sciences, 6(3), 62. https://doi.org/10.3390/medsci6030062