
Treatment of Vitamin D Deficiency in Decompensated Patients with Cirrhosis Is Associated with Improvement in Frailty

 , , , , , , , , and
, , , , , , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Patients
2.3. Treatment
2.4. Anthropometric Assessments
2.5. Frailty
2.6. Incidence of Falls and Other Clinical Events
2.7. Handgrip Muscular Strength
2.8. Body Composition by Dual Energy X-Ray Absorptiometry (DXA)
2.9. Health-Related Quality of Life (HRQoL) and Mood: SF-36, CLDQ and HADS
2.10. Analytical Determinations
2.11. Statistical Analysis
3. Results
3.1. Frailty
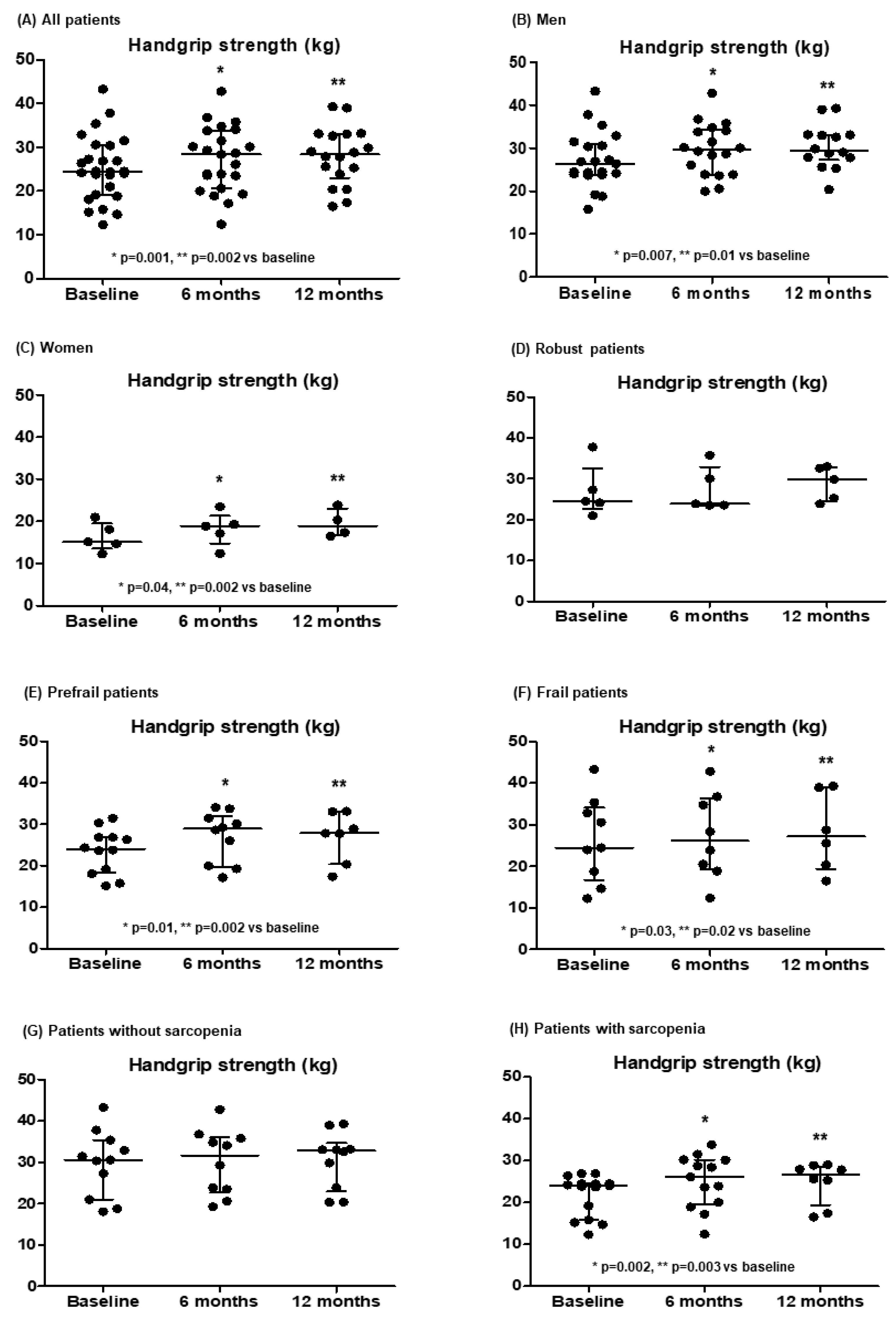
3.2. Handgrip Muscular Strength
3.3. Mood and HRQoL
3.4. Analytical Parameters
3.5. Body Composition
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tandon, P.; Montano-Loza, A.J.; Lai, J.C.; Dasarathy, S.; Merli, M. Sarcopenia and frailty in decompensated cirrhosis. J. Hepatol. 2021, 75 (Suppl. 1), S147–S162. [Google Scholar] [CrossRef]
- Wang, S.; Whitlock, R.; Xu, C.; Taneja, S.; Singh, S.; Abraldes, J.G.; Burak, K.W.; Bailey, R.J.; Lai, J.C.; Tandon, P. Frailty is associated with increased risk of cirrhosis disease progression and death. Hepatology 2022, 75, 600–609. [Google Scholar] [CrossRef] [PubMed]
- Román, E.; Parramón, M.; Flavià, M.; Gely, C.; Poca, M.; Gallego, A.; Santesmases, R.; Hernández, E.; Nieto, J.C.; Urgell, E.; et al. Frailty in outpatients with cirrhosis: A prospective observational study. Liver Int. 2021, 41, 357–368. [Google Scholar] [CrossRef] [PubMed]
- Kappus, M.R.; Mendoza, M.S.; Nguyen, D.; Medici, V.; McClave, S.A. Sarcopenia in Patients with Chronic Liver Disease: Can It Be Altered by Diet and Exercise? Curr. Gastroenterol. Rep. 2016, 18, 43. [Google Scholar] [CrossRef] [PubMed]
- Paul, S.; Kaushik, R.; Chawla, P.; Upadhyay, S.; Rawat, D.; Akhtar, A. Vitamin-D as a multifunctional molecule for overall well-being: An integrative review. Clin. Nutr. ESPEN 2024, 62, 10–21. [Google Scholar] [CrossRef]
- Russo, C.; Santangelo, R.; Malaguarnera, L. Valle MS. The “Sunshine Vitamin” and Its Antioxidant Benefits for Enhancing Muscle Function. Nutrients 2024, 16, 2195. [Google Scholar] [CrossRef]
- Anilkumar, S.A.; Dutta, S.; Aboo, S.; Ismail, A. Vitamin D as a modulator of molecular pathways involved in CVDs: Evidence from preclinical studies. Life Sci. 2024, 357, 123062. [Google Scholar] [CrossRef] [PubMed]
- Androutsakos, T.; Politou, M.; Boti, S.; Pittaras, T.; Kontos, A.; Kordossis, T.; Pouliakis, A.; Panayiotakopoulos, G. Prevalence and Causes of Vitamin D Deficiency in a Cohort of Greek HIV-Infected Individuals: A Prospective, Single Centre, Observational Study. Curr. HIV Res. 2024, 22, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Chen, J.; Li, Z.; Xiong, H.; Lei, Z.; Chen, D.; Zhang, Y.; Gao, Z.; Mo, Z. Association of vitamin D with functional cure in chronic hepatitis B: Insights from a retrospective cohort study and an intervention study. Clin. Nutr. ESPEN 2024, 64, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Zhou, T.; Lv, C.; Ni, H.; Zhao, Z.; Zhou, H.; Hu, X. Vitamin D supplementation can improve the 28-day mortality rate in patients with sepsis-associated acute kidney injury. Ren. Fail. 2024, 46, 2431632. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Okubo, T.; Atsukawa, M.; Tsubota, A.; Ono, H.; Kawano, T.; Yoshida, Y.; Arai, T.; Hayama, K.; Itokawa, N.; Kondo, C.; et al. Effect of Vitamin D Supplementation on Skeletal Muscle Volume and Strength in Patients with Decompensated Liver Cirrhosis Undergoing Branched Chain Amino Acids Supplementation: A Prospective, Randomized, Controlled Pilot Trial. Nutrients 2021, 13, 1874. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. Ross, A.C., Taylor, C.L., Yaktine, A.L., Del Valle, H.B., Eds.; Dietary Reference Intakes for Calcium and Vitamin D; National Academies Press (US): Washington DC, USA, 2011. Available online: https://www.ncbi.nlm.nih.gov/books/NBK56070/ (accessed on 1 January 2017). [CrossRef]
- Wang, J.; Thornton, J.C.; Kolesnik, S.; Pierson, R.N., Jr. Anthropometry in body composition. An overview. Ann. N. Y. Acad. Sci. 2000, 904, 317–326. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A. Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Bergstrom, N.; Braden, B.J.; Laguzza, A.; Holman, V. The Braden Scale for Predicting Pressure Sore Risk. Nurs. Res. 1987, 36, 205–210. [Google Scholar] [CrossRef]
- Centre for Metabolic Bone Diseases UoSU. FRAX WHO Fracture Risk Assessment Tool. 2020. Available online: https://www.sheffield.ac.uk/FRAX/ (accessed on 15 July 2023).
- Kerr, G.K.; Worringham, C.J.; Cole, M.H.; Lacherez, P.F.; Wood, J.M.; Silburn, P.A. Predictors of future falls in Parkinson disease. Neurology 2010, 75, 116–124. [Google Scholar] [CrossRef]
- Soriano, G.; Román, E.; Córdoba, J.; Torrens, M.; Poca, M.; Torras, X.; Villanueva, C.; Gich, I.J.; Vargas, V.; Guarner, C. Cognitive dysfunction in cirrhosis is associated with falls: A prospective study. Hepatology 2012, 55, 1922–1930. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Alonso, J.; Prieto, L.; Antó, J.M. The Spanish version of the SF-36 Health Survey (the SF-36 health questionnaire): An instrument for measuring clinical results. Med. Clin. 1995, 104, 771–776. [Google Scholar]
- Ferrer, M.; Córdoba, J.; Garin, O.; Olivé, G.; Flavià, M.; Vargas, V.; Esteban, R.; Alonso, J. Validity of the Spanish version of the Chronic Liver Disease Questionnaire (CLDQ) as a standard outcome for quality of life assessment. Liver Transpl. 2006, 12, 95–104. [Google Scholar] [CrossRef]
- Herrmann, C. International experiences with the Hospital Anxiety and Depression Scale--a review of validation data and clinical results. J. Psychosom. Res. 1997, 42, 17–41. [Google Scholar] [CrossRef]
- Lai, J.C.; Dodge, J.L.; Kappus, M.R.; Wong, R.; Mohamad, Y.; Segev, D.L.; McAdams-DeMarco, M. A multicenter pilot randomized clinical trial of a home-based exercise program for patients with cirrhosis: The Strength Training Intervention (STRIVE). Am. J. Gastroenterol. 2021, 116, 717–722. [Google Scholar] [CrossRef]
- Jamali, T.; Raasikh, T.; Bustamante, G.; Sisson, A.; Tandon, P.; Duarte-Rojo, A.; Hernaez, R. Outcomes of exercise interventions in patients with advanced liver disease: A systematic review of randomized clinical trials. Am. J. Gastroenterol. 2022, 117, 1614–1620. [Google Scholar] [CrossRef] [PubMed]
- Williams, F.R.; Berzigotti, A.; Lord, J.M.; Lai, J.C.; Armstrong, M.J. Review article: Impact of exercise on physical frailty in patients with chronic liver disease. Aliment. Pharmacol. Ther. 2019, 50, 988–1000. [Google Scholar] [CrossRef] [PubMed]
- Román, E.; Torrades, M.T.; Nadal, M.J.; Cárdenas, G.; Nieto, J.C.; Vidal, S.; Bascuñana, H.; Juárez, C.; Guarner, C.; Córdoba, J.; et al. Randomized pilot study: Effects of an exercise programme and leucine supplementation in patients with cirrhosis. Dig. Dis. Sci. 2014, 59, 1966–1975. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.W.; Ferrando, A.; White, M.G.; Dennis, R.A.; Xie, J.; Pauly, M.; Park, S.; Bartter, T.; Dunn, M.A.; Ruiz-Margain, A.; et al. Home-based physical activity and diet intervention to improve physical function in advanced liver disease: A randomized pilot trial. Dig. Dis. Sci. 2020, 65, 3350–3359. [Google Scholar] [CrossRef]
- Hernández-Conde, M.; Llop, E.; Gómez-Pimpollo, L.; Fernández Carrillo, C.; Rodríguez, L.; Van Den Brule, E.; Perelló, C.; López-Gómez, M.; Abad, J.; Martínez-Porras, J.L.; et al. Adding branched-chain amino acids to an enhanced standard-of-care treatment improves muscle mass of cirrhotic patients with sarcopenia: A placebo-controlled trial. Am. J. Gastroenterol. 2021, 116, 2241–2249. [Google Scholar] [CrossRef]
- Colosimo, S.; Bertoli, S.; Saffioti, F. Use of branched-chain amino acids as a potential treatment for improving nutrition-related outcomes in advanced chronic liver disease. Nutrients 2023, 15, 4190. [Google Scholar] [CrossRef]
- Siramolpiwat, S.; Limthanetkul, N.; Pornthisarn, B.; Vilaichone, R.K.; Chonprasertsuk, S.; Bhanthumkomol, P.; Nunanan, P.; Issariyakulkarn, N. Branched-chain amino acids supplementation improves liver frailty index in frail compensated cirrhotic patients: A randomized controlled trial. BMC Gastroenterol. 2023, 23, 154. [Google Scholar] [CrossRef]
- Sinclair, M.; Grossmann, M.; Hoermann, R.; Angus, P.W.; Gow, P.J. Testosterone therapy increases muscle mass in men with cirrhosis and low testosterone: A randomised controlled trial. J. Hepatol. 2016, 65, 906–913. [Google Scholar] [CrossRef]
- Román, E.; Nieto, J.C.; Gely, C.; Vidal, S.; Pozuelo, M.; Poca, M.; Juárez, C.; Guarner, C.; Manichanh, C.; Soriano, G. Effect of a multistrain probiotic on cognitive function and risk of falls in patients with cirrhosis: A randomized trial. Hepatol. Commun. 2019, 12, 632–645. [Google Scholar] [CrossRef] [PubMed]
- Román, E.; Kaür, N.; Sánchez, E.; Poca, M.; Padrós, J.; Nadal, M.J.; Cuyàs, B.; Alvarado, E.; Vidal, S.; Ortiz, M.À.; et al. Home exercise, branched-chain amino acids, and probiotics improve frailty in cirrhosis: A randomized clinical trial. Hepatol. Commun. 2024, 8, e0443. [Google Scholar] [CrossRef]
- Okubo, T.; Atsukawa, M.; Tsubota, A.; Yoshida, Y.; Arai, T.; Iwashita, A.N.; Itokawa, N.; Kondo, C.; Iwakiri, K. Relationship between serum vitamin D level and sarcopenia in chronic liver disease. Hepatol. Res. 2020, 50, 588–597. [Google Scholar] [CrossRef] [PubMed]
- Wierzbicka, A.; Oczkowicz, M. Sex differences in vitamin D metabolism, serum levels and action. Br. J. Nutr. 2022, 128, 2115–2130. [Google Scholar] [CrossRef]
- Karampela, I.; Sakelliou, A.; Vallianou, N.; Christodoulatos, G.S.; Magkos, F.; Dalamaga, M. Vitamin D and Obesity: Current Evidence and Controversies. Curr. Obes. Rep. 2021, 10, 162–180. [Google Scholar] [CrossRef]
- Chattranukulchai Shantavasinkul, P.; Nimitphong, H. Vitamin D and Visceral Obesity in Humans: What Should Clinicians Know? Nutrients 2022, 14, 3075. [Google Scholar] [CrossRef] [PubMed]
- Wamberg, L. Effects of vitamin D supplementation on body fat accumulation, inflammation, and metabolic risk factors in obese adults with low vitamin D levels—Results from a randomized trial. Eur. J. Intern. Med. 2013, 24, 644–649. [Google Scholar] [CrossRef]
- Sripongpunku, C.; Aisawan, P.; Tanchanoj, C.; Thanapluetiwong, S.; Sriwannopas, O.; Chansirikarnjana, S.; Assavapokee, T.; Srisuwarn, P.; Ruangritchankul, S. Factors associated with unintentional weight loss among older adults in a geriatric outpatient clinic of university hospital. PLoS ONE 2021, 16, e0260233. [Google Scholar] [CrossRef] [PubMed]
- Bischoff-Ferrari, H.A.; Giovannucci, E.; Willett, W.C.; Dietrich, T.; Dawson-Hughes, B. Estimation of optimal serum concentrations of 25-hydroxyvitamin D for multiple health outcomes. Am. J. Clin. Nutr. 2006, 84, 18–28. [Google Scholar] [CrossRef]
- Kouba, B.R.; Camargo, A.; Gil-Mohapel, J.; Rodrigues, A.L.S. Molecular Basis Underlying the Therapeutic Potential of Vitamin D for the Treatment of Depression and Anxiety. Int. J. Mol. Sci. 2022, 23, 7077. [Google Scholar] [CrossRef]
- Zittermann, A. Vitamin D supplementation enhances the beneficial effects of weight loss on cardiovascular disease risk markers. Am. J. Clin. Nutr. 2009, 89, 1321–1327. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo-López, L.; Maseda, A.; de Labra, C.; Regueiro-Folgueira, L.; Rodríguez-Villamil, J.L.; Millán-Calenti, J.C. Nutritional determinants of frailty in older adults: A systematic review. BMC Geriatr. 2017, 17, 108. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| All Patients n = 27 | HGUGM n = 14 | HSCSP n = 13 | p-Value | |
|---|---|---|---|---|
| Age (yr) | 62 (55–72) | 58 (51.5–64.7) | 67 (56.5–76.5) | 0.02 |
| Gender (male; n, %) | 22 (81.5%) | 12 (85%) | 10 (77%) | 0.56 |
| BMI (kg/m2) | 28.7 (24.7–30.1) | 28.6 (26.2–29.6) | 28.7 (24.5–30.8) | 0.59 |
| Comorbidity (Charlson score) | 6 (5–7) | 6 (4.7–7.2) | 6 (5–7) | 0.72 |
| Treatments | ||||
| Antidepressants (n, %) | 1 (3.7%) | 0 (0.0%) | 1 (7.7%) | 0.29 |
| Benzodiazepines (n, %) | 2 (7.4%) | 0 (0%) | 2 (15.4%) | 0.12 |
| Opioids (n, %) | 1 (3.7%) | 0 (0%) | 1 (7.7%) | 0.20 |
| Diuretics (n, %) | 19 (70.4%) | 9 (64.3%) | 10 (77%) | 0.47 |
| Beta-blockers (n, %) | 16 (59.2%) | 7 (50%) | 9 (69%) | 0.31 |
| Non-absorbable disaccharides (n, %) | 13 (48.1%) | 6 (42.8%) | 7 (53.8%) | 0.70 |
| Rifaximin (n, %) | 5 (18.5%) | 4 (28.6%) | 1 (7.7%) | 0.32 |
| Characteristics of cirrhosis | ||||
| Alcohol aetiology (n, %) | 9 (33.3%) | 4 (28.6%) | 5 (38.5%) | 0.90 |
| Child–Pugh score | 7 (6–8) | 7 (6–8.2) | 7 (6–7) | 0.17 |
| Child–Pugh A/B/C (n, %) | 9 (33%)/16 (59%)/2 (8%) | 4 (29%)/8 (57%)/2 (14%) | 5 (38%)/8 (62%)/0 | 0.15 |
| MELD score | 11 (9–14) | 13 (10.7–17.5) | 9 (7–11) | <0.001 |
| Oesophageal varices (n, %) | 21 (77.8%) | 11 (78.6%) | 10 (77%) | 0.91 |
| Hepatocellular carcinoma (n, %) | 4 (14.8%) | 3 (21.4%) | 1 (7.7%) | 0.31 |
| Previous ascites (n, %) | 24 (88.9%) | 14 (100%) | 10 (77%) | 0.05 |
| Previous variceal bleeding (n, %) | 12 (44.4%) | 7 (50%) | 5 (38.5%) | 0.54 |
| Previous overt hepatic encephalopathy (n, %) | 9 (33.3%) | 6 (42.9%) | 3 (23%) | 0.27 |
| Previous infection last year (n, %) | 12 (44.4%) | 9 (64%) | 3 (23%) | 0.054 |
| Previous SBP (n, %) | 7 (25.9%) | 5 (36%) | 2 (15.4%) | 0.22 |
| Parameters of frailty and body composition | ||||
| Fried frailty index | 1 (1–3) | 2 (1–3) | 1 (0–3) | 0.09 |
| Handgrip strength (kg) | 24.4 (19.1–0.5) | 25.4 (22.6–30.8) | 23.9 (16.6–27.2) | 0.32 |
| Previous falls/fractures (n, %) (previous year) | 11 (41%)/2 (7.4%) | 5 (36%)/1 (7.1%) | 6 (46%)/1 (7.7%) | 0.70/1.00 |
| FRAX risk of osteoporotic fracture at 10 years (%) | 3.7 (1.9–6.4) | 1.9 (1.7–3.7) | 5.4 (3.5–8.4) | 0.004 |
| FRAX risk of hip fracture at 10 years (%) | 1.3 (0.3–2.3) | 0.4 (0.2–1.6) | 2 (0.6–3.1) | 0.03 |
| Right arm circumference (cm) | 30 (25.7–32.4) | 30.2 (25.8–32.2) | 30 (24.5–33.5) | 0.89 |
| Right arm skinfold (mm) | 1.4 (1.0–1.9) | 1.1 (0.8–1.6) | 1.6 (1.2–3.0) | 0.02 |
| Tinetti total score | 27 (26–28) | 27 (26.5–27.5) | 28 (25.5–28) | 0.45 |
| Braden score | 22 (22–23) | 22 (21.7–23) | 22 (22–23) | 0.98 |
| HADS anxiety score | 5 (1–7) | 5.5 (2.7–9) | 2 (2–6.5) | 0.10 |
| HADS depression score | 5 (2–8) | 7 (4.7–9.2) | 2 (0.5–5) | 0.001 |
| Analytical parameters | ||||
| INR | 1.26 (1.18–1.45) | 1.38 (1.21–1.58) | 1.25 (1.12–1.27) | 0.006 |
| Bilirubin (mg/dL) | 1.54 (1.27–2.40) | 2 (1.07–3.4) | 1.44 (1.33–1.55) | 0.08 |
| Albumin (g/L) | 33.1 (30.2–39) | 35.5 (28.7–40.5) | 32 (31.5–35.4) | 0.37 |
| Sodium (mmol/L) | 138 (136–140) | 138 (135–141) | 138 (136–139) | 0.54 |
| Creatinine (mg/dL) | 0.81 (0.72–1.00) | 0.87 (0.72–1.15) | 0.78 (9.72–0.88) | 0.20 |
| 25OH Vitamin D (ng/mL) | 12.7 (8.8–21) | 16.2 (12.4–24.9) | 8.9 (5.5–12.2) | 0.046 |
| Baseline n = 27 | 6 Months n = 27 | 12 Months n = 22 | |
|---|---|---|---|
| Robust/prefrail/frail (n, %) | 6 (22%)/12 (44%)/9 (33%) | 14 (52%)/10 (37%)/3 (11%) 1 | 6 (27%)/10 (45%)/5 (23%) * |
| Handgrip strength (kg) | 24.4 (19.1–30.4) | 28.4 (20.6–33.8) 2 | 28.3 (23–33) 3 |
| FRAX risk of osteoporotic fracture at 10 years (%) | 3.7 (1.9–6.4) | - | 3.3 (1.8–6.6) |
| FRAX risk of hip fracture at 10 years (%) | 1.3 (0.3–2.3) | - | 1.0 (0.2–2.6) |
| Tinetti total score | 27 (26–28) | 28 (26.5–28) | 27.5 (22–28) |
| Braden scale total | 22 (22–23) | 22 (22–23) | 23 (21–23) |
| - Braden scale nutrition | 3 (3–4) | 4 (3–4) | 4 (4–4) 4 |
| HADS anxiety | |||
| - all patients (n = 27) | 5 (1–7) | 3 (1–6) | 3 (1–7) |
| - frail patients (n = 9) | 7 (3.5–11) | 3 (1–5.5) 5 | 7 (3–9) |
| HADS depression | 5 (2–8) | 3 (0–6) | 3 (0.7–5) |
| SF-36 physical component | 42.1 (34.5–47.5) | 40.5 (32.1–52.9) | 46.1 (35.8–55.7) |
| SF-36 mental component | |||
| - all patients | 50.1 (41.5–54.7) | 50.2 (43.5–56.3) | 53.3 (46.1–58.7) |
| - frail and prefrail patients (n = 21) | 45.3 (35.53.6) | 48.7 (40.6–53.2) 6 | 51 (39–58.3) |
| CLDQ | 5.03 (4.31–5.86) | 4.93 (4.17–6.15) | 5.24 (4.20–6.01) |
| Baseline n = 27 | 6 Months n = 27 | 12 Months n = 22 | |
|---|---|---|---|
| Haemoglobin (g/dL) | 12.1 (9.9–13) | 13.3 (10.4–14.6) 1 | 13.4 (10.8–14) |
| Platelets (1 × 109/L) | 85 (68–96) | 83 (59–106) | 72 (60.5–85) 2 |
| Creatinine (mg/dL) | 0.81 (0.72–1.00) | 0.90 (0.75–1.12) | 0.81 (0.73–1.05) |
| Sodium (mmol/L) | 138 (136–140) | 138 (136–141) | 137 (135–140) |
| AST (U/L) | 37 (29–48) | 38 (31–55) | 40 (31–64.5) |
| ALT (U/L) | 25 (18–33) | 33 (20–43) | 28 (21–50.5) |
| ALP (U/L) | 93 (50–195) | 105 (49–251) | 111 (66–199) |
| GGT (U/L) | 134 (121–172) | 140 (112–195) | 130 (106–173) |
| INR | 1.26 (1.18–1.45) | 1.30 (1.14–1.42) | 1.30 (1.20–1.48) |
| Bilirubin (mg/dL) | 1.54 (1.27–2.40) | 1.57 (1.00–2.40) | 1.69 (1.11–2.81) |
| Albumin (g/L) | 33.1 (30.2–39) | 35.9 (30.3–40) | 37.9 (31.9–39.1) |
| Child–Pugh score | 7 (6–8) | 7 (6–7) | 7 (5–7.5) |
| Child–Pugh class A/B/C (%) | 9 (33%)/16 (59%)/2 (8%) | 13 (48%)/11 (41%)/3 (11%) | 10 (45%)/9 (41%)/3 (14%) |
| MELD score | 11 (9–14) | 11 (9–14) | 12 (10–15) |
| Prealbumin (mg/dL) | 8.0 (6.0–11.0) | 10.0 (8.0–13.2) 3 | 11.0 (9.0–14.0) 3 |
| Triglycerides (mg/dL) | 83.2 (61.1–114) | 85 (69.8–123.2) | 75.7 (66.5–178) |
| Cholesterol (mg/dL) | 132 (92.5–153) | 164.5 (119.5–182.8) 4 | 154.3 (123.6–175.2) 3 |
| LDL cholesterol (mg/dL) | 68 (44–98) | 86.2 (61.2–110.2) | 82.7 (66.9–98) |
| HDL cholesterol (mg/dL) | 36.4 (24.4–45) | 47.4 (36.6–56.2) 5 | 48 (32–61.5) 6 |
| Magnesium (mg/dL) | 1.8 (1.6–1.9) | 1.8 (1.7–1.9) | 1.8 (1.6–1.9) |
| Zinc (µg/L) | 53.0 (45.8–66.0) | 66.4 (53.0–75.1) 4 | 61.6 (44.6–68.6) |
| Copper (µg/L) | 86 (78–100) | 82 (66–102) | 85 (69–98) |
| Ferritin (µg/L) | 127 (38–272) | 89 (29–313) | 83 (44–177) |
| Calcium (mg/dL) | 8.9 (8.6–9.6) | 8.9 (8.7–9.4) | 9.2 (8.9–9.5) |
| Phosphate (mg/dL) | 3.4 (2.7–3.5) | 3.4 (3.0–3.7) | 3.2 (2.5–3.6) |
| 25OH Vitamin D (ng/mL) | 12.7 (8.8–21) | 37.2 (18.6–55.4) 5 | 44.5 (28.3–59.1) 5 |
| Vitamin D: | |||
| Sufficient | 0 (0%) | 17 (63%) | 15 (68%) |
| Insufficient | 8 (30%) | 4 (15%) | 5 (23%) |
| Deficient (n, %) | 19 (70%) | 6 (22%) 5 | 2 (9%) 5 |
| Parathyroid hormone (ng/L) | 32.5 (28.3–53.0) | 28.8 (17.0–51.8) | 25.1 (21.1–34.8) 7 |
| Vitamin A (µg/dL) | 14 (10–22) | 24 (17–29) 8 | 23 (18–33) 9 |
| Vitamin E (µg/dL) | 1102 (836–1387) | 1148 (951–1319) | 1038 (858–1537) |
| Vitamin B12 (ng/L) | 677 (450–883) | 634 (419–1221) | 412 (337–721) |
| Folate (µg/L) | 9.2 (6.6–16.1) | 12.7 (8.2–21.9) 10 | 15.2 (10.0–19.1) 3 |
| Baseline n = 27 | 6 Months n = 27 | 12 Months n = 22 | |
|---|---|---|---|
| Anthropometry | |||
| BMI (kg/m2) | 28.7 (24.7–30.1) | 29.9 (25.5–30.1) | 29.8 (26.2–31.2) 1 |
| Right arm circumference (cm) | 30 (25.7–32.4) | 30.1 (28–33) | 29 (26.5–32.5) |
| Right arm skinfold (mm) | 1.43 (1.04–1.92) | 1.69 (1.11–2.50) 2 | 1.73 (1.25–2.97) |
| Mid-arm muscle circumference (cm) | 24.8 (20.9–28.1) | 25.0 (22.3–26.5) | 23.9 (21.1–25.4) |
| DXA (n = 22) | |||
| Pelvis (g/cm2) median (IQR) | 0.940 (0.877–1.074) | - | 0.950 (0.847–1.098) |
| Spine (g/cm2) | 0.937 (0.785–1.146) | - | 0.968 (0.792–1.118) |
| Total bone (g/cm2) | 1.077 (0.991–1.149) | - | 1.067 (0.987–1.136) |
| Fat right arm (g) | 974 (814–1386) | - | 1173 (932–1805) 3 |
| Fat right leg (g) | 3168 (2421–3855) | - | 3487 (2890–4691) 4 |
| Fat trunk (g) | 10,463 (7578–15,358) | - | 12,858 (9232–16,409) 5 |
| Android fat (g) | 1613 (1239–2460) | - | 2073 (1482–2929) 6 |
| Total fat (g) | 19,022 (16,763–27,243) | - | 25,889 (17,210–27,928) 4 |
| Fat (%) | 26.2 (21.4–32.2) | - | 31.4 (25.5–36.2) 7 |
| Lean right arm (g) | 2354 (2003–2884) | - | 2725 (2081–2988) 1 |
| Lean right leg (g) | 7803 (6923–9058) | - | 7815 (7077–8750) |
| Lean total (g) | 52,774 (43,652–60,660) | - | 54,181 (47,212–57,775) |
| Lean arms/height2 (g/m2) | 1621 (1421–1832) | - | 1805 (1437–1946) 8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Díaz-Ruíz, R.; Poca, M.; Román, E.; Cuyàs, B.; Bañares, I.; Morales, Á.; Hernández Martínez-Esparza, E.; Panadero, R.; Velasco, C.; Rapado-Castro, M.; et al. Treatment of Vitamin D Deficiency in Decompensated Patients with Cirrhosis Is Associated with Improvement in Frailty. Med. Sci. 2025, 13, 30. https://doi.org/10.3390/medsci13010030
Díaz-Ruíz R, Poca M, Román E, Cuyàs B, Bañares I, Morales Á, Hernández Martínez-Esparza E, Panadero R, Velasco C, Rapado-Castro M, et al. Treatment of Vitamin D Deficiency in Decompensated Patients with Cirrhosis Is Associated with Improvement in Frailty. Medical Sciences. 2025; 13(1):30. https://doi.org/10.3390/medsci13010030
Chicago/Turabian StyleDíaz-Ruíz, Raquel, Maria Poca, Eva Román, Berta Cuyàs, Irene Bañares, Ángela Morales, Elvira Hernández Martínez-Esparza, Rocío Panadero, Cristina Velasco, Marta Rapado-Castro, and et al. 2025. "Treatment of Vitamin D Deficiency in Decompensated Patients with Cirrhosis Is Associated with Improvement in Frailty" Medical Sciences 13, no. 1: 30. https://doi.org/10.3390/medsci13010030
APA StyleDíaz-Ruíz, R., Poca, M., Román, E., Cuyàs, B., Bañares, I., Morales, Á., Hernández Martínez-Esparza, E., Panadero, R., Velasco, C., Rapado-Castro, M., Bretón, I., Bañares, R., Soriano, G., & García-Martínez, R. (2025). Treatment of Vitamin D Deficiency in Decompensated Patients with Cirrhosis Is Associated with Improvement in Frailty. Medical Sciences, 13(1), 30. https://doi.org/10.3390/medsci13010030