
Change in Indications and Outcomes for Stereotactic Biopsy Following Transition from Full Field Digital Mammography + Digital Breast Tomosynthesis to Full Field Synthetic Mammography + Digital Breast Tomosynthesis

Abstract
1. Introduction
2. Methods and Materials
2.1. Imaging Technique
2.2. Statistical Analysis
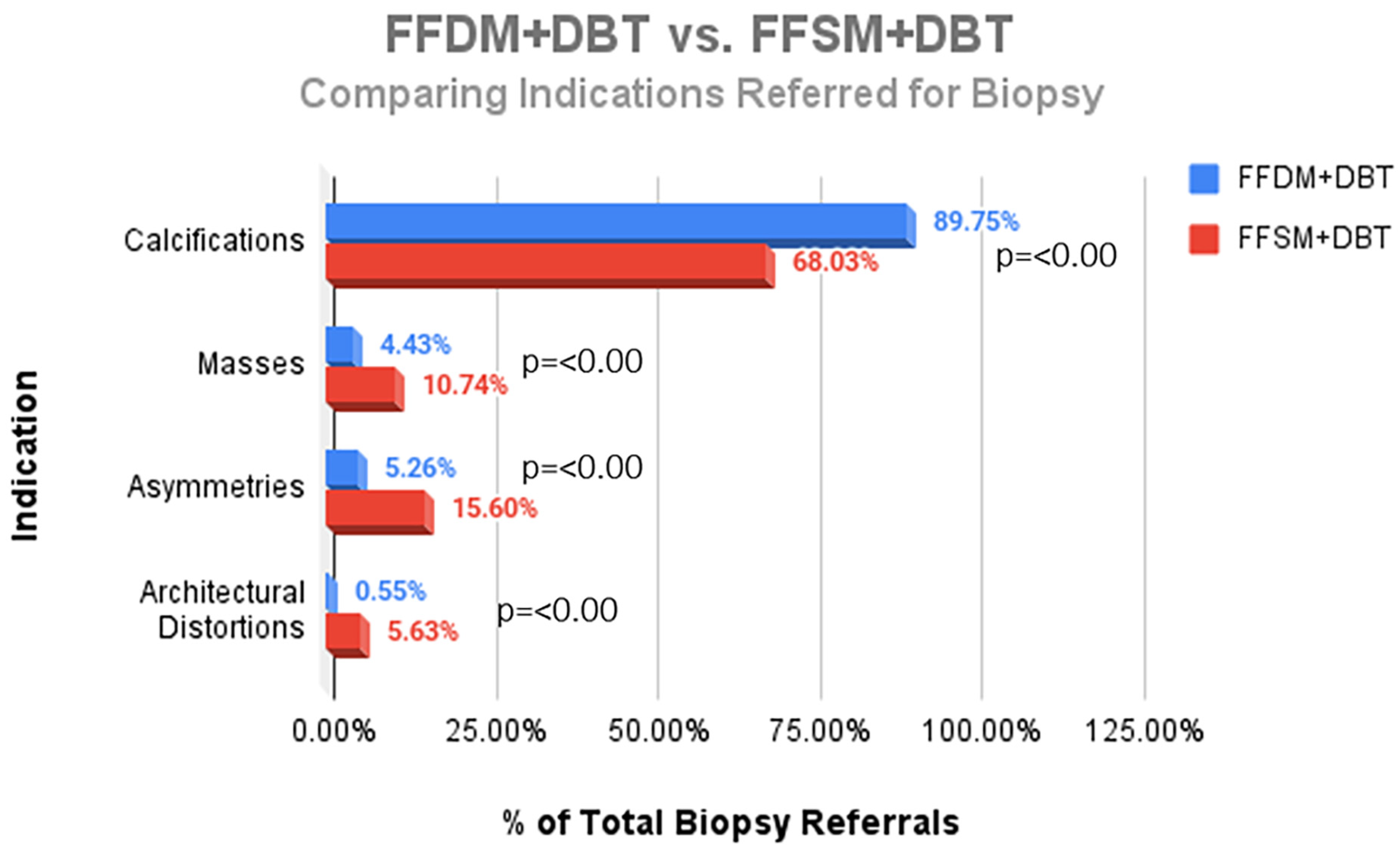
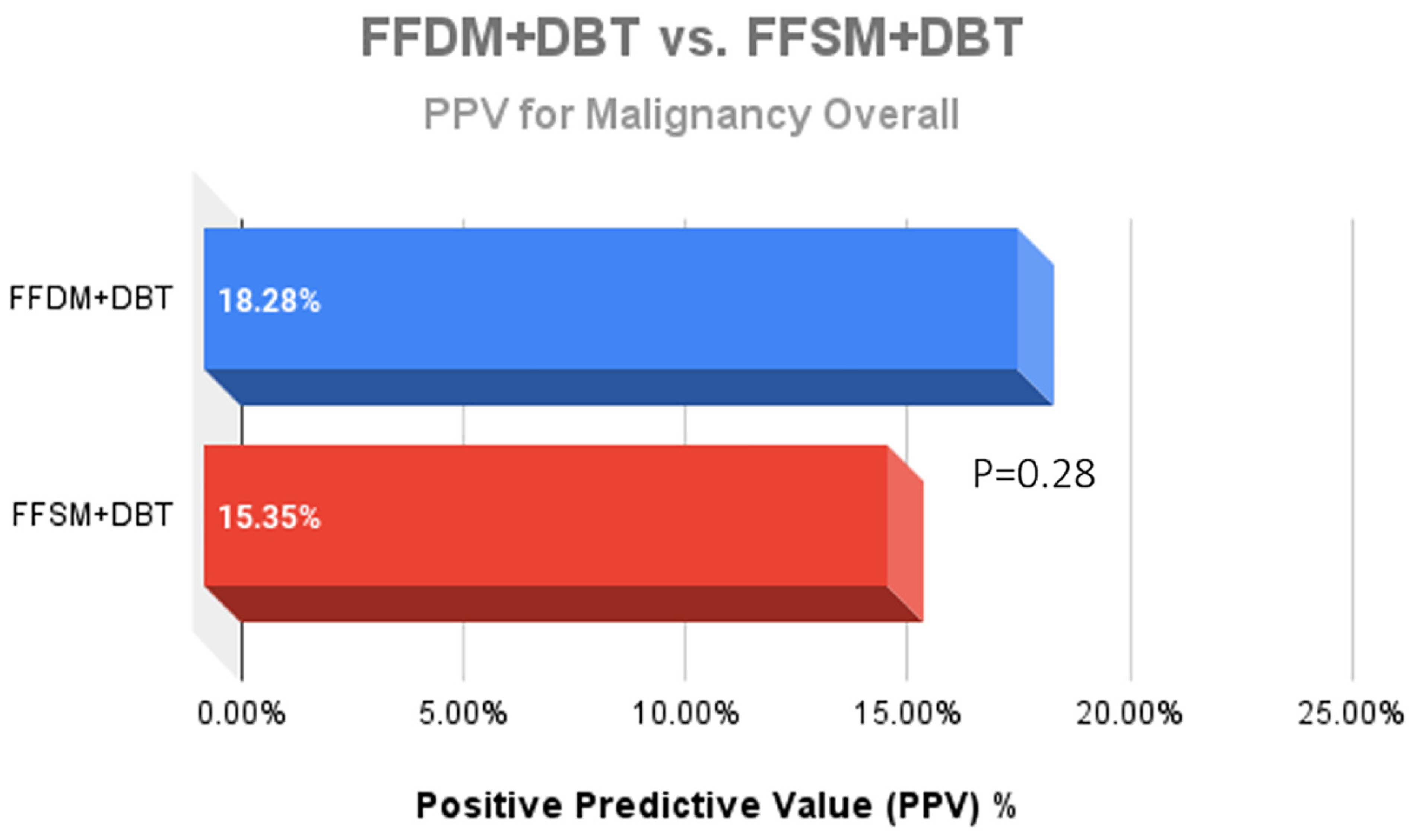
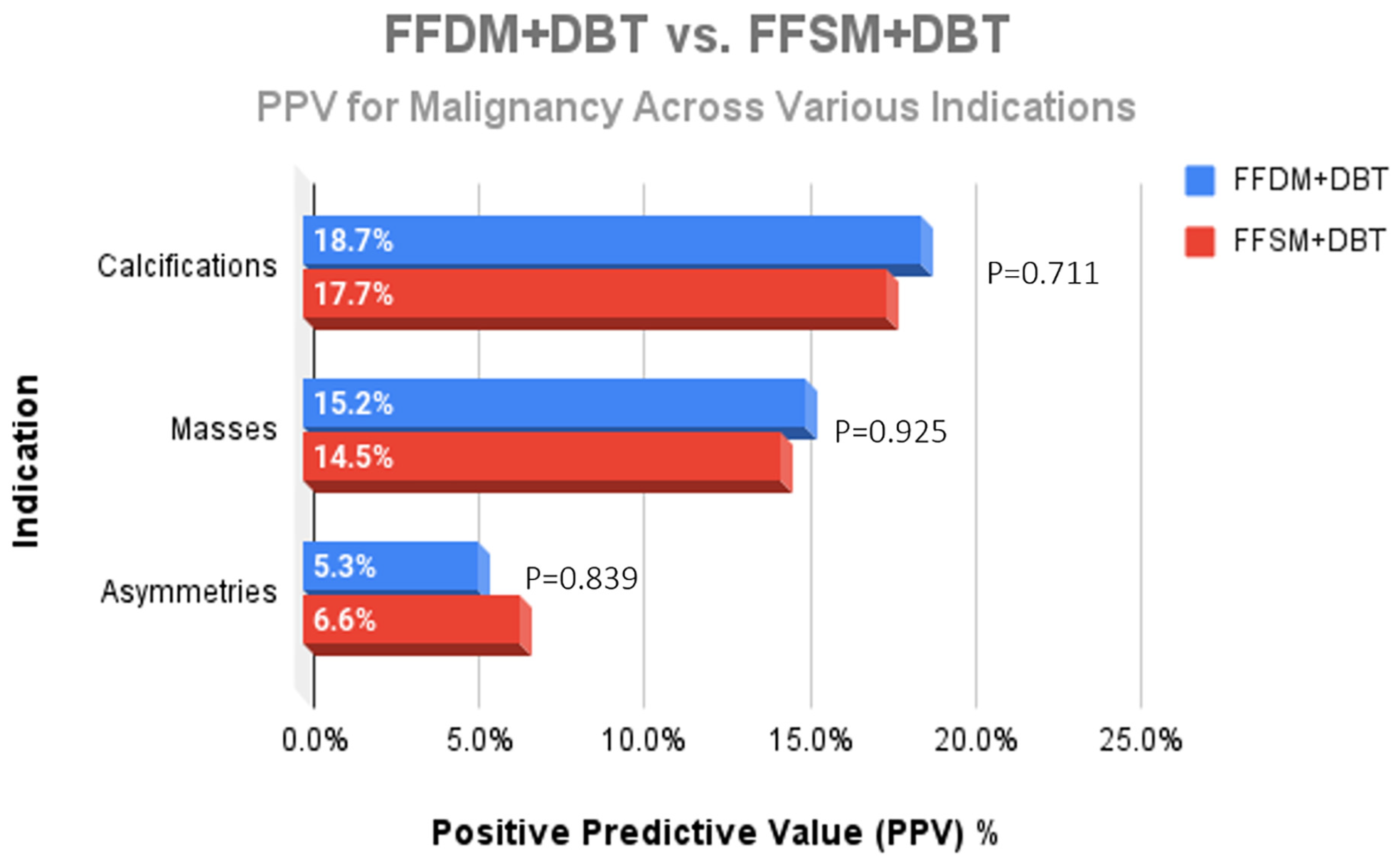
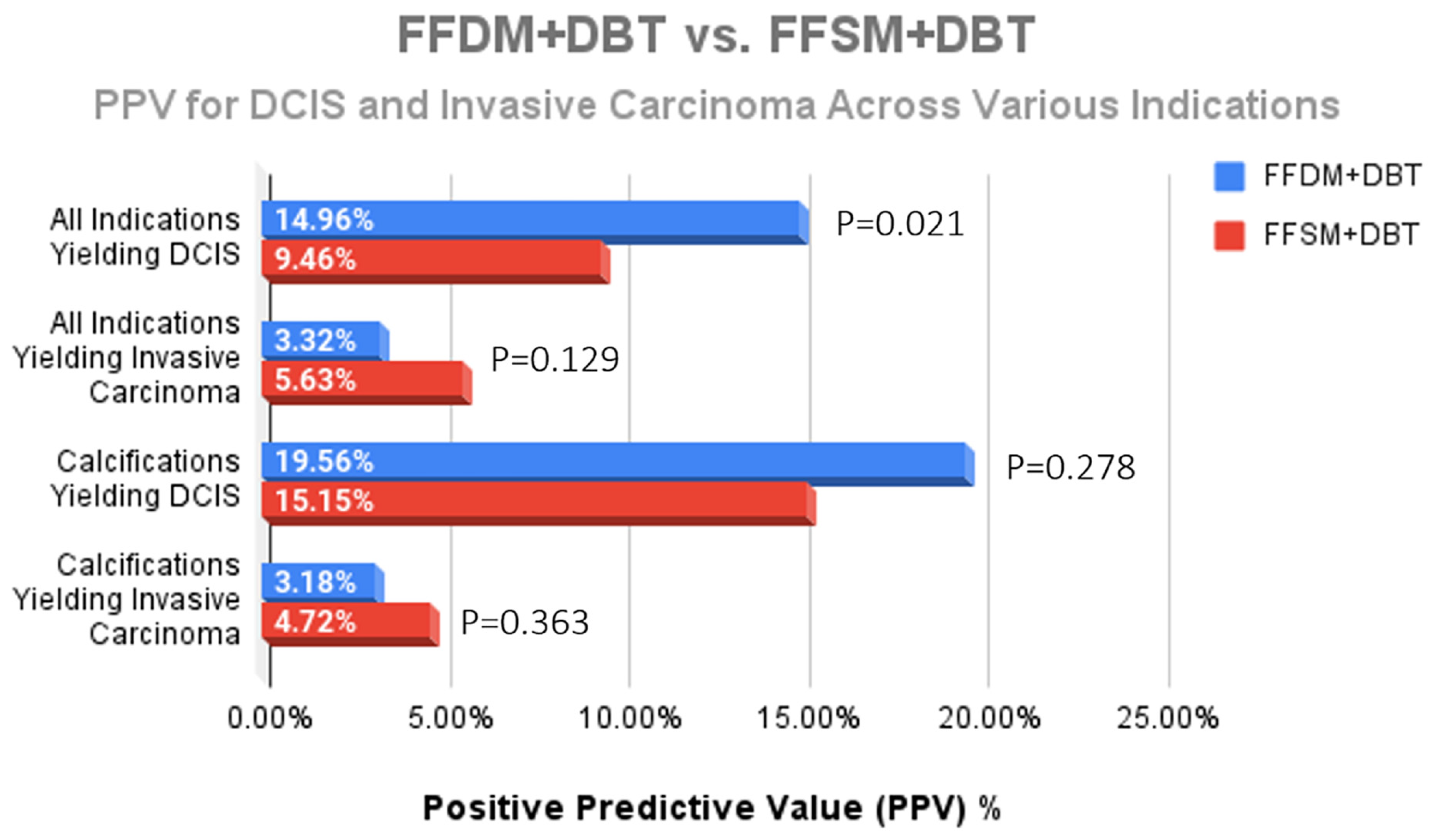
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- US Food and Drug Administration. Selenia Dimensions 3D System-P080003. Available online: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm?id=P080003 (accessed on 6 March 2025).
- Ciatto, S.; Houssami, N.; Bernardi, D.; Caumo, F.; Pellegrini, M.; Brunelli, S.; Tuttobene, P.; Bricolo, P.; Fantò, C.; Valentini, M.; et al. Integration of 3D digital mammography with tomosynthesis for population breast-cancer screening (STORM): A prospective comparison study. Lancet Oncol. 2013, 14, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Skaane, P.; Bandos, A.I.; Gullien, R.; Eben, E.B.; Ekseth, U.; Haakenaasen, U.; Izadi, M.; Jebsen, I.N.; Jahr, J.; Krager, M.; et al. Comparison of digital mammography alone and digital mammography plus tomosynthesis in a population based screening program. Radiology 2013, 267, 47–56. [Google Scholar] [CrossRef]
- Skaane, P.; Bandos, A.I.; Eben, E.B.; Jebsen, I.N.; Krager, M.; Haakenaasen, U.; Ekseth, U.; Izadi, M.; Hofvind, S.; Gullien, R. Two-view digital breast tomosynthesis screening with synthetically reconstructed projection images: Comparison with digital breast tomosynthesis with full-field digital mammographic images. Radiology 2014, 271, 655–663. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, A.M.; Kontos, D.; Synnestvedt, M.; Tan, K.S.; Heitjan, D.F.; Schnall, M.; Conant, E.F. Screening outcomes following implementation of digital breast tomosynthesis in a general-population screening program. J. Natl. Cancer Inst. 2014, 106, dju316. [Google Scholar] [CrossRef] [PubMed]
- Zuckerman, S.P.; Maidment, A.D.A.; Weinstein, S.P.; McDonald, E.S.; Conant, E.F. Imaging with synthesized 2D mammography: Differences, advantages, and pitfalls compared with digital mammography. Am. J. Roentgenol. 2017, 209, 222–229. [Google Scholar] [CrossRef]
- Zuckerman, S.P.; Sprague, B.L.; Weaver, D.L.; Herschorn, S.D.; Conant, E.F. Multicenter evaluation of breast cancer screening with digital breast tomosynthesis in combination with synthetic versus digital mammography. Radiology 2020, 297, 545–553. [Google Scholar] [CrossRef]
- Conant, E.F.; Zuckerman, S.P.; McDonald, E.S.; Weinstein, S.P.; Korhonen, K.E.; Birnbaum, J.A.; Tobey, J.D.; Schnall, M.D.; Hubbard, R.A. Five consecutive years of screening with digital breast tomosynthesis: Outcomes by screening year and round. Radiology 2020, 295, 285–293. [Google Scholar] [CrossRef]
- Friedewald, S.M.; Rafferty, E.A.; Rose, S.L.; Durand, M.A.; Plecha, D.M.; Greenberg, J.S.; Hayes, M.K.; Copit, D.S.; Carlson, K.L.; Cink, T.M.; et al. Breast cancer screening using tomosynthesis in combination with digital mammography. JAMA 2014, 311, 2499–2507. [Google Scholar] [CrossRef]
- Heindel, W.; Weigel, S.; Gerß, J.; Hense, H.W.; Sommer, A.; Krischke, M.; Kerschke, L. Digital breast tomosynthesis plus synthesised mammography versus digital screening mammography for the detection of invasive breast cancer (TOSYMA): A multicentre, open-label, randomised, controlled, superiority trial. Lancet Oncol. 2022, 23, 601–611. [Google Scholar] [CrossRef]
- Tirada, N.; Li, G.; Dreizin, D.; Robinson, L.; Khorjekar, G.; Dromi, S.; Ernst, T. Digital Breast Tomosynthesis: Physics, Artifacts, and Quality Control Considerations. Radiographics 2019, 39, 413–426. [Google Scholar] [CrossRef]
- Freer, P.E.; Winkler, N. Synthesized Digital Mammography Imaging. Radiol. Clin. N. Am. 2017, 55, 503–512. [Google Scholar] [CrossRef] [PubMed]
- Elmi, A.; Rakow-Penner, R.; Chong, A.; Eghtedari, M.; Ladd, W.; Lim, V.; Ojeda-Fournier, H. Calcifications on DBT and Synthetic Views: Update and Management Strategies. Curr. Radiol. Rep. 2020, 8, 9. [Google Scholar] [CrossRef]
- Durand, M. Synthesized Mammography: Clinical Evidence, Appearance, and Implementation. Diagnostics 2018, 8, 22. [Google Scholar] [CrossRef]
- Skaane, P.; Bandos, A.I.; Gullien, R.; Eben, E.B.; Ekseth, U.; Haakenaasen, U.; Izadi, M.; Jebsen, I.N.; Jahr, G.; Krager, M.; et al. Prospective trial comparing full-field digital mammography (FFDM) versus combined FFDM and tomosynthesis in a population-based screening programme using independent double reading with arbitration. Eur. Radiol. 2013, 23, 2061–2071. [Google Scholar] [CrossRef]
- Zuckerman, S.P.; Sprague, B.L.; Weaver, D.L.; Herschorn, S.D.; Conant, E.F. Survey results regarding uptake and impact of synthetic digital mammography with tomosynthesis in the screening setting. J. Am. Coll. Radiol. 2020, 17 Pt A, 31e7. [Google Scholar] [CrossRef]
- Zuckerman, S.P.; Conant, E.F.; Keller, B.M.; Maidment, A.D.; Barufaldi, B.; Weinstein, S.P.; Synnestvedt, M.; McDonald, E.S. Implementation of synthesized two-dimensional mammography in a population-based digital breast tomosynthesis screening program. Radiology 2016, 281, 730–736. [Google Scholar] [CrossRef]
- US Food and Drug Administration, Department of Health and Human Services. Summary of Safety and Effectiveness Data (SSED). Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf8/P080003S001B.pdf (accessed on 6 March 2025).
- Zeng, B.; Yu, K.; Gao, L.; Zeng, X.; Zhou, Q. Breast cancer screening using synthesized two-dimensional mammography: A systematic review and meta-analysis. Breast 2021, 59, 270–278. [Google Scholar] [CrossRef]
- Dodelzon, K.; Simon, K.; Dou, E.; Levy, A.D.; Michaels, A.Y.; Askin, G.; Katzen, J.T. Performance of 2D Synthetic Mammography Versus Digital Mammography in the Detection of Microcalcifications at Screening. AJR Am. J. Roentgenol. 2020, 214, 1436–1444. [Google Scholar] [CrossRef]
- Kilic, P.; Sendur, H.N.; Gultekin, S.; Gultekin, I.I.; Cindil, E.; Cerit, M. Comparison of diagnostic performances in the evaluation of breast microcalcifications: Synthetic mammography versus full-field digital mammography. Ir. J. Med. Sci. 2022, 191, 1891–1897. [Google Scholar] [CrossRef]
- Spangler, M.L.; Zuley, M.L.; Sumkin, J.H.; Abrams, G.; Ganott, M.A.; Hakim, C.; Perrin, R.; Chough, D.M.; Shah, R.; Gur, D. Detection and classification of calcifications on digital breast tomosynthesis and 2D digital mammography: A comparison. AJR Am. J. Roentgenol. 2011, 196, 320–324. [Google Scholar] [CrossRef]
- Gilbert, F.J.; Tucker, L.; Gillan, M.G.; Willsher, P.; Cooke, J.; Duncan, K.A.; Michell, M.J.; Dobson, H.M.; Lim, Y.Y.; Suaris, T.; et al. Accuracy of digital breast tomosynthesis for depicting breast cancer subgroups in a UK retrospective reading study (TOMMY trial). Radiology 2015, 277, 697–706. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.S.; Han, B.K.; Ko, E.Y.; Hahn, S.Y.; Shin, J.H.; Kim, M.J. Comparison between two-dimensional synthetic mammography reconstructed from digital breast tomosynthesis and full-field digital mam-mography for the detection of T1 breast cancer. Eur. Radiol. 2016, 26, 2538–2546. [Google Scholar] [CrossRef] [PubMed]
- Zuley, M.L.; Guo, B.; Catullo, V.J.; Chough, D.M.; Kelly, A.E.; Lu, A.H.; Rathfon, G.Y.; Spangler, M.L.; Sumkin, J.H.; Wallace, L.P.; et al. Comparison of two-dimensional synthesized mammograms versus original digital mammograms alone and in combination with tomosynthesis images. Radiology 2014, 271, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Ratanaprasatporn, L.; Chikarmane, S.A.; Giess, C.S. Strengths and weaknesses of synthetic mammography in screening. RadioGraphics 2017, 37, 1913–1927. [Google Scholar] [CrossRef]
- Mariscotti, G.; Durando, M.; Houssami, N.; Fasciano, M.; Tagliafico, A.; Bosco, D.; Casella, C.; Bogetti, C.; Bergamasco, L.; Fonio, P.; et al. Comparison of synthetic mammography, reconstructed from digital breast tomosynthesis, and digital mammography: Evaluation of lesion conspicuity and BI-RADS assessment categories. Breast Cancer Res. Treat. 2017, 166, 765–773. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Comparing Overall Cancer Center Metrics | |||
|---|---|---|---|
| FFDM + DBT | FFSM + DBT | p-Value | |
| CDR | 16.4/1000 | 21.1/1000 | <0.001 *** |
| PPV3 | 20.3% | 21.8% | 0.213 |
| ICR | 1.370/1000 | 1.197/1000 | 0.491 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Net, J.; Hamedi-Sangsari, A.; Schwartz, T.; Barrios, M.; Brofman, N.; Pluguez-Turull, C.; Spoont, J.; Stamler, S.; Yepes, M. Change in Indications and Outcomes for Stereotactic Biopsy Following Transition from Full Field Digital Mammography + Digital Breast Tomosynthesis to Full Field Synthetic Mammography + Digital Breast Tomosynthesis. Med. Sci. 2025, 13, 29. https://doi.org/10.3390/medsci13010029
Net J, Hamedi-Sangsari A, Schwartz T, Barrios M, Brofman N, Pluguez-Turull C, Spoont J, Stamler S, Yepes M. Change in Indications and Outcomes for Stereotactic Biopsy Following Transition from Full Field Digital Mammography + Digital Breast Tomosynthesis to Full Field Synthetic Mammography + Digital Breast Tomosynthesis. Medical Sciences. 2025; 13(1):29. https://doi.org/10.3390/medsci13010029
Chicago/Turabian StyleNet, Jose, Antoine Hamedi-Sangsari, Taylor Schwartz, Mirelys Barrios, Nicole Brofman, Cedric Pluguez-Turull, Jamie Spoont, Sarah Stamler, and Monica Yepes. 2025. "Change in Indications and Outcomes for Stereotactic Biopsy Following Transition from Full Field Digital Mammography + Digital Breast Tomosynthesis to Full Field Synthetic Mammography + Digital Breast Tomosynthesis" Medical Sciences 13, no. 1: 29. https://doi.org/10.3390/medsci13010029
APA StyleNet, J., Hamedi-Sangsari, A., Schwartz, T., Barrios, M., Brofman, N., Pluguez-Turull, C., Spoont, J., Stamler, S., & Yepes, M. (2025). Change in Indications and Outcomes for Stereotactic Biopsy Following Transition from Full Field Digital Mammography + Digital Breast Tomosynthesis to Full Field Synthetic Mammography + Digital Breast Tomosynthesis. Medical Sciences, 13(1), 29. https://doi.org/10.3390/medsci13010029