
An Unusual Case of Nephrotic Range Proteinuria in a Short-Standing Type 1 Diabetic Patient with Newly Diagnosed Systemic Lupus Erythematosus: A Case Report and Literature Review

 , , and
, , and
Abstract
1. Introduction
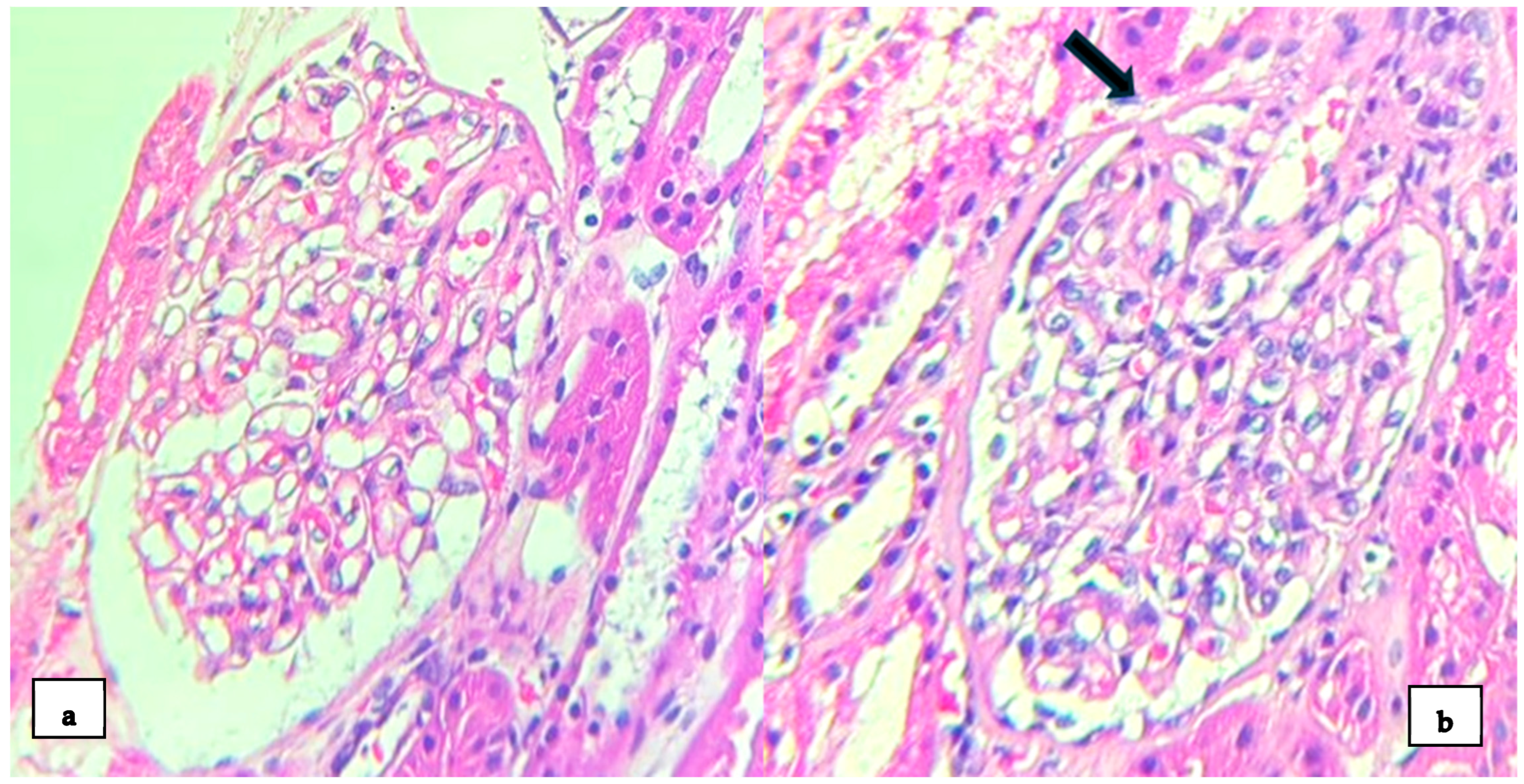
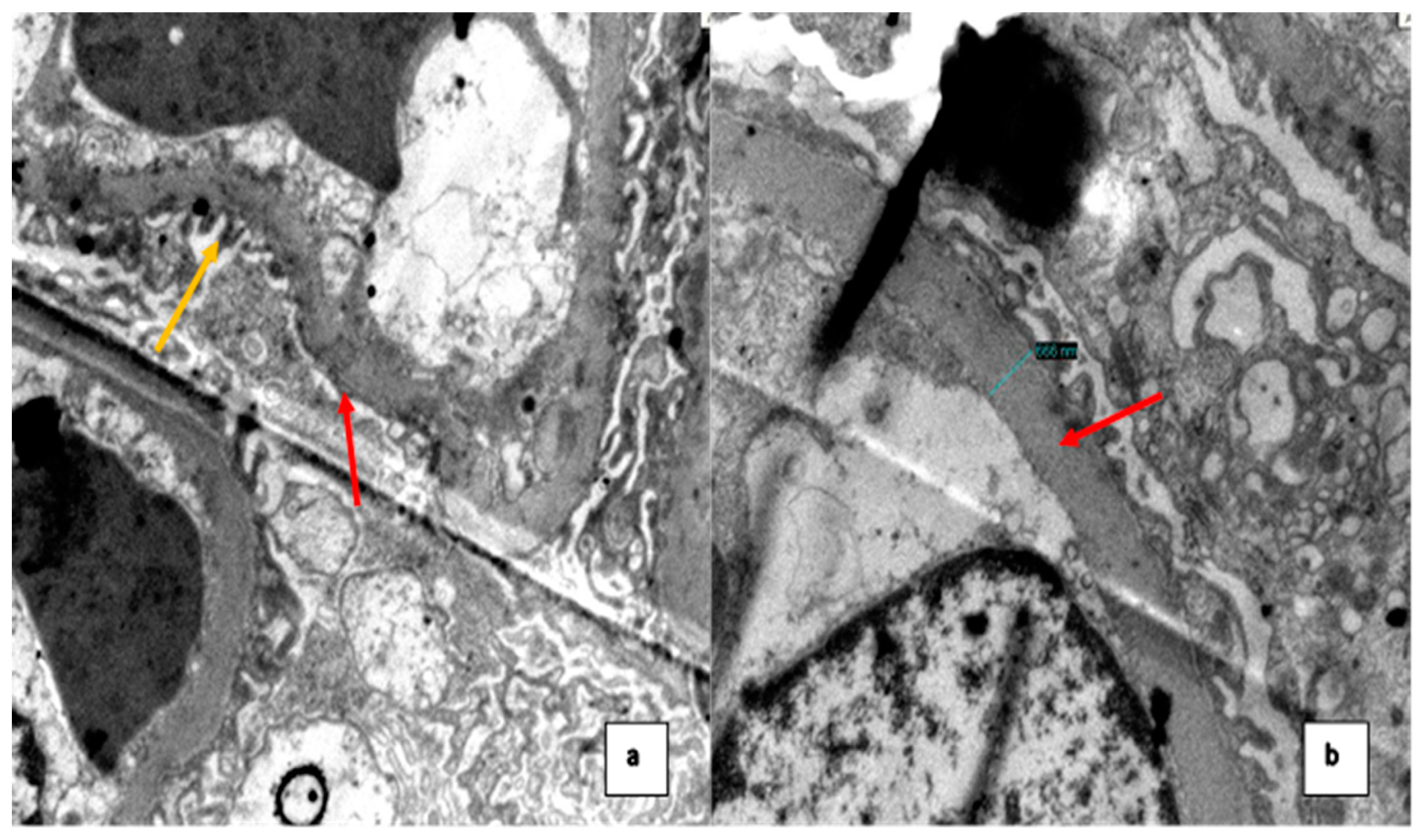
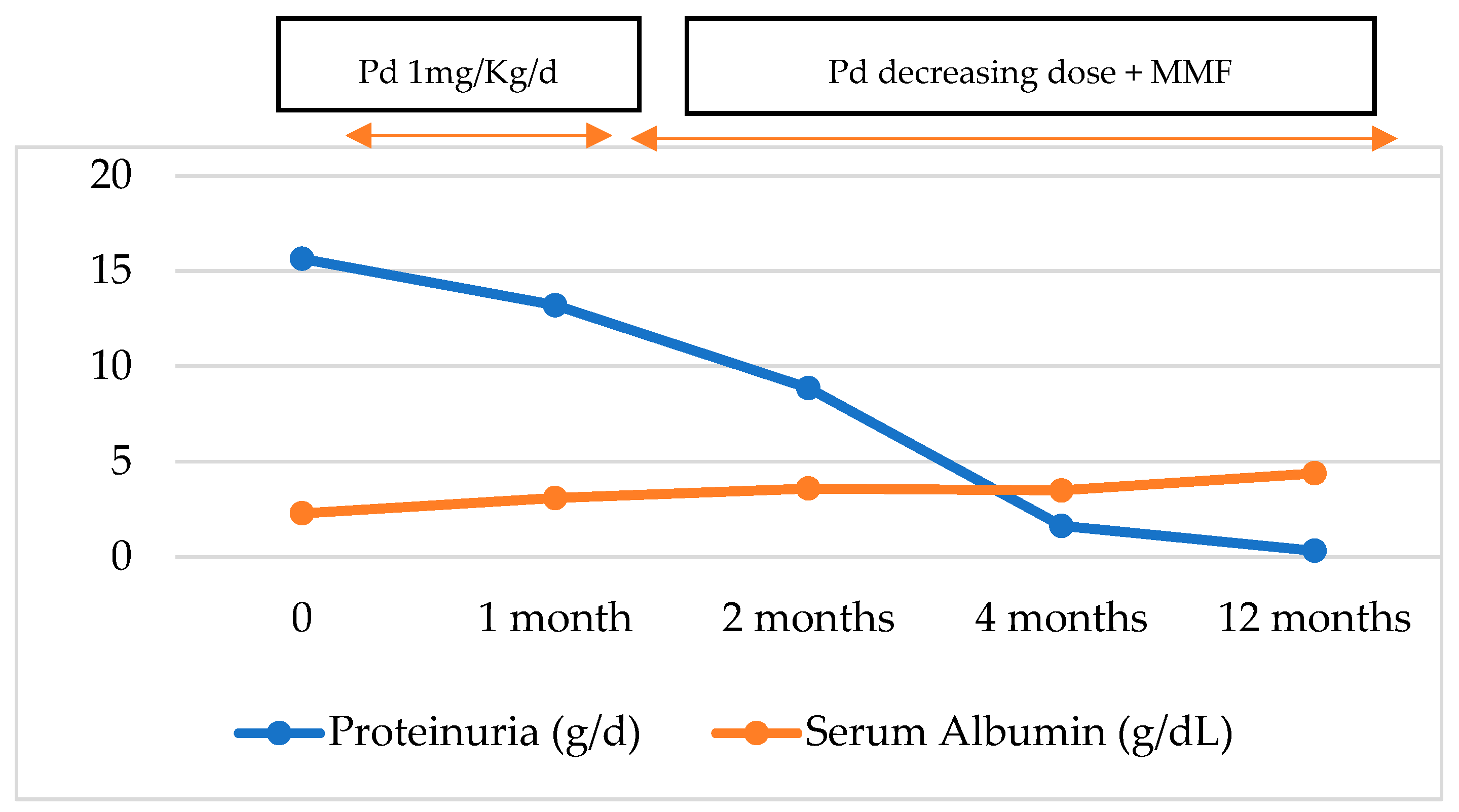
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aringer, M.; Costenbader, K.; Daikh, D.; Brinks, R.; Mosca, M.; Ramsey-Goldman, R.; Smolen, J.S.; Wofsy, D.; Boumpas, D.T.; Kamen, D.L.; et al. 2019 European League Against Rheumatism/American College of Rheumatology Classification Criteria for Systemic Lupus Erythematosus. Arthritis Rheumatol. 2019, 71, 1400–1412. [Google Scholar] [CrossRef] [PubMed]
- Ugarte-Gil, M.F.; Alarcón, G.S. Systemic lupus erythematosus in Latin America: Outcomes and therapeutic challenges. Clin. Immunol. Commun. 2023, 4, 60–64. [Google Scholar] [CrossRef]
- Parikh, S.V.; Almaani, S.; Brodsky, S.; Rovin, B.H. Update on Lupus Nephritis: Core Curriculum 2020. Am. J. Kidney Dis. 2020, 76, 265–281. [Google Scholar] [CrossRef]
- Weening, J.J.; D’agati, V.D.; Schwartz, M.M.; Seshan, S.V.; Alpers, C.E.; Appel, G.B.; Balow, J.E.; Bruijn, J.A.N.A.; Cook, T.; Ferrario, F.; et al. The classification of glomerulonephritis in systemic lupus erythematosus revisited. Kidney Int. 2004, 65, 521–530. [Google Scholar] [CrossRef]
- Oliva-Damaso, N.; Payan, J.; Oliva-Damaso, E.; Pereda, T.; Bomback, A.S. Lupus Podocytopathy: An Overview. Adv. Chronic Kidney Dis. 2019, 26, 369–375. [Google Scholar] [CrossRef]
- Hoover, P.J.; Costenbader, K.H. Insights into the epidemiology and management of lupus nephritis from the US rheumatologist’s perspective. Kidney Int. 2016, 90, 487–492. [Google Scholar] [CrossRef]
- Lewis, E.J. Lupus Podocytopathy. In Lupus Nephritis, 2nd ed.; Lewis, E.J., Schwartz, M.M., Korbet, S.M., Chan, D.T.M., Eds.; Oxford Clinical Nephrology Series; Oxford University Press: Oxford, UK, 2010; pp. 123–135. [Google Scholar]
- Bomback, A.S.; Markowitz, G.S. Lupus Podocytopathy: A Distinct Entity. Clin. J. Am. Soc. Nephrol. 2016, 11, 547–548. [Google Scholar] [CrossRef] [PubMed]
- Hu, W.; Chen, Y.; Wang, S.; Chen, H.; Liu, Z.; Zeng, C.; Zhang, H.; Liu, Z. Clinical-Morphological Features and Outcomes of Lupus Podocytopathy. Clin. J. Am. Soc. Nephrol. 2016, 11, 585–592. [Google Scholar] [CrossRef]
- Pipino, A.S.; Segretti, P.M.; Ribeiro, B.S.; Gomes, G.M.; de Segura, J.A.; Giovanni Filho, S.C.F.; Zanuto, A.C.D. WCN24-2512 Lupus podocytopathy: Case report. Kidney Int. Rep. 2024, 9 (Suppl. S4), S519. [Google Scholar] [CrossRef]
- Kraft, S.W.; Schwartz, M.M.; Korbet, S.M.; Lewis, E.J. Glomerular podocytopathy in patients with systemic lupus erythematosus. J. Am. Soc. Nephrol. 2005, 16, 175–179. [Google Scholar] [CrossRef]
- Forbes, J.M.; Cooper, M.E. Mechanisms of diabetic complications. Physiol. Rev. 2013, 93, 137–188. [Google Scholar] [CrossRef]
- Hünemörder, S.; Treder, J.; Ahrens, S.; Schumacher, V.; Paust, H.; Menter, T.; Matthys, P.; Kamradt, T.; Meyer-Schwesinger, C.; Panzer, U.; et al. TH1 and TH17 cells promote crescent formation in experimental autoimmune glomerulonephritis. J. Pathol. 2015, 237, 62–71. [Google Scholar] [CrossRef] [PubMed]
- Paquissi, F.C.; Abensur, H. The Th17/IL-17 axis and kidney diseases, with focus on lupus nephritis. Front. Med. Nephrol. 2021, 8, 654912. [Google Scholar] [CrossRef]
- Wang, Y.; Yu, F.; Song, D.; Wang, S.-X.; Zhao, M.-H. Podocyte involvement in lupus nephritis based on the 2003 ISN/RPS system: A large cohort study from a single centre. Rheumatology 2014, 53, 1235–1244. [Google Scholar] [CrossRef]
- Alqudsi, M.; Cobbs, J.; Navarrete, J. Lupus Podocytopathy Case Series in an Urban USA Population. Am. J. Kidney Dis. 2019, 73, 651. [Google Scholar] [CrossRef]
- Salvatore, S.P.; Barisoni, L.M.C.; Herzenberg, A.M.; Chander, P.N.; Nickeleit, V.; Seshan, S.V. Collapsing glomerulopathy in 19 patients with systemic lupus erythematosus or lupus-like disease. Clin. J. Am. Soc. Nephrol. 2012, 7, 914–925. [Google Scholar] [CrossRef] [PubMed]
- Vasquez, D.L.; Bembry, W.; Mesa, C.J.; Patel, N.J.; Guevara, M.E. Lupus podocytopathy: Case series and review. Lupus 2022, 31, 1017–1019. [Google Scholar] [CrossRef] [PubMed]
- Dina-Batlle, L.; Rodriguez, D.A.; Bencosme, E. Lupus podocytopathy: Case series of 4 cases from Dominican Republic. Kidney Int. Rep. 2024, 9 (Suppl. S4), S164–S165. [Google Scholar] [CrossRef]
- Alicic, R.Z.; Rooney, M.T.; Tuttle, K.R. Diabetic Kidney Disease: Challenges, Progress, and Possibilities. Clin. J. Am. Soc. Nephrol. 2017, 12, 2032–2045. [Google Scholar] [CrossRef]
- Thomas, D.; Franceschini, N.; Hogan, S.; Holder, S.T.; Jennette, C.; Falk, R.; Jennette, J. Clinical and pathologic characteristics of focal segmental glomerulosclerosis pathologic variants. Kidney Int. 2006, 69, 920–926. [Google Scholar] [CrossRef] [PubMed]
- Dube, G.K.; Markowitz, G.S.; Radhakrishnan, J.; Appel, G.B.; D’Agati, V.D. Minimal change disease in systemic lupus erythematosus. Clin. Nephrol. 2002, 57, 120–126. [Google Scholar] [CrossRef]
- Rojas-Rivera, J.E.; García-Carro, C.; Ávila, A.I.; Espino, M.; Espinosa, M.; Fernández-Juárez, G.; Fulladosa, X.; Goicoechea, M.; Macía, M.; Morales, E.; et al. Consensus document of the Spanish Group for the Study of the Glomerular Diseases (GLOSEN) for the diagnosis and treatment of lupus nephritis. Nefrologia Engl. Ed. 2023, 43, 6–47. [Google Scholar] [CrossRef] [PubMed]
- Rovin, B.H.; Ayoub, I.M.; Chan, T.M.; Liu, Z.H.; Mejía-Vilet, J.M.; Floege, J. Kidney Disease: Improving Global Outcomes (KDIGO) Lupus Nephritis Work Group. KDIGO 2024 Clinical Practice Guideline for the management of LUPUS NEPHRITIS. Kidney Int. 2024, 105 (Suppl. S1), S1–S69. [Google Scholar] [CrossRef] [PubMed]
- Saxena, A.; Ginzler, E.M.; Gibson, K.; Satirapoj, B.; Santillán, A.E.Z.; Levchenko, O.; Navarra, S.; Atsumi, T.; Yasuda, S.; Chavez-Perez, N.N.; et al. Safety and efficacy of long-term voclosporin treatment for lupus nephritis in the phase 3 AURORA 2 clinical trial. Arthritis Rheumatol. 2024, 76, 59–67. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Values | Normal Range United | |
|---|---|---|
| Hemoglobin (Hb) | 6.8 | 11–15 g/dL |
| Reticulocytes | 21.4% | 0.5–2% |
| Platelet count | 266 | 150–400 × 103 µL |
| White blood cells (WBC) | 13.7 | 5–10 × 103 µL |
| Limphocytes | 3.1 | 1.5–3.5 × 103 µL |
| Lactate dehydrogenase (LDH) | 244 | 120–246 U/L |
| Direct Coombs test | +++ | NA |
| Total bilirrubin | 1.3 | 0.2–1.3 mg/dL |
| Indirect bilirrubin | 0.2 | 0–1.1 mg/dL |
| Total proteins | 5.5 | 6.3–8.2 g/dL |
| Serum albumin | 2.3 | 3.5–5 g/dL |
| Glucose | 305 | 75–110 mg/dL |
| Urea | 16 | 15–36 mg/dL |
| Creatinine | 0.37 | 0.7–1.2 mg/dL |
| Sodium | 131 | 135–148 mmol/L |
| Potassium | 3.7 | 3.5–5.3 mmol/L |
| Total calcium | 8.2 | 8.4–10.2 mg/dL |
| Phosphorus | 4.9 | 2.5–4.5 mg/dL |
| Magnesium | 1.7 | 1.6–2.3 mg/dL |
| Total cholesterol | 362 | 0–200 mg/dL |
| Triglycerides | 176 | <150 mg/dL |
| LDL | 244.8 | 0–130 mg/dL |
| AST | 28 | 15–46 U/L |
| ALT | 23 | 13–69 U/L |
| ESR | 140 | 0–15 mm/h |
| CRP | Negative | mg/L |
| Hematuria | 0–2 xc | NA |
| Anti-VHB core | Not Reactive | NA |
| HBsAg | Not Reactive | NA |
| Anti-VHC | Not Reactive | NA |
| Anti-VIH 1-2 | Not Reactive | NA |
| RPR | Not Reactive | NA |
| Anti-HTLV 1-2 | Not Reactive | NA |
| Bengal rose test | Negative | NA |
| Blood culture | Negative | NA |
| Urine culture | Negative | NA |
| Parasitolgy stool | Negative | NA |
| 24 h urine total protein Excretion | 15,640 | 42–225 mg/24 h |
| ANA | 1/800 | NA |
| Anti-dsDNA | ||
| C3 | 103 | 90–180 mg/dL |
| C4 | 9 | 10–40 mg/dL |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dominguez Davalos, M.; De La Flor, J.C.; Bedia Castillo, C.; Lipa Chancolla, R.; Rodríguez Tudero, C.; Apaza, J.; Zamora, R.; Cieza-Terrones, M. An Unusual Case of Nephrotic Range Proteinuria in a Short-Standing Type 1 Diabetic Patient with Newly Diagnosed Systemic Lupus Erythematosus: A Case Report and Literature Review. Med. Sci. 2024, 12, 74. https://doi.org/10.3390/medsci12040074
Dominguez Davalos M, De La Flor JC, Bedia Castillo C, Lipa Chancolla R, Rodríguez Tudero C, Apaza J, Zamora R, Cieza-Terrones M. An Unusual Case of Nephrotic Range Proteinuria in a Short-Standing Type 1 Diabetic Patient with Newly Diagnosed Systemic Lupus Erythematosus: A Case Report and Literature Review. Medical Sciences. 2024; 12(4):74. https://doi.org/10.3390/medsci12040074
Chicago/Turabian StyleDominguez Davalos, Marco, José C. De La Flor, Carlos Bedia Castillo, Roxana Lipa Chancolla, Celia Rodríguez Tudero, Jacqueline Apaza, Rocío Zamora, and Michael Cieza-Terrones. 2024. "An Unusual Case of Nephrotic Range Proteinuria in a Short-Standing Type 1 Diabetic Patient with Newly Diagnosed Systemic Lupus Erythematosus: A Case Report and Literature Review" Medical Sciences 12, no. 4: 74. https://doi.org/10.3390/medsci12040074
APA StyleDominguez Davalos, M., De La Flor, J. C., Bedia Castillo, C., Lipa Chancolla, R., Rodríguez Tudero, C., Apaza, J., Zamora, R., & Cieza-Terrones, M. (2024). An Unusual Case of Nephrotic Range Proteinuria in a Short-Standing Type 1 Diabetic Patient with Newly Diagnosed Systemic Lupus Erythematosus: A Case Report and Literature Review. Medical Sciences, 12(4), 74. https://doi.org/10.3390/medsci12040074