
Comprehensive Geriatric Care in Older Adults: Walking Ability after an Acute Fracture

 ,
,  , and
, and
Abstract
1. Background
2. Methods
2.1. Patients and Measures
2.2. Assessment of Walking Ability (Timed Up and Go Test, TuG)
2.3. Statistical Analyses
2.4. Ethical Approval
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CGC | Comprehensive Geriatric Care |
| TuG | Timed Up and Go test |
| IQR | interquartile range |
| MMSE | Mini-Mental State Evaluation |
References
- Fuhrmann, R. Overview of health care services in clinical and rehabilitation geriatrics and their development in Germany. Z. Gerontol. Geriatr. 2001, 34 (Suppl. S1), 16–20. [Google Scholar] [CrossRef] [PubMed]
- Kolb, G.; Breuninger, K.; Gronemeyer, S.; van den Heuvel, D.; Lübke, N.; Lüttje, D.; Wittrich, A.; Wolff, J. Ten years of early complex geriatric rehabilitation therapy in the DRG system. Z. Gerontol. Geriatr. 2014, 47, 6–12. [Google Scholar] [CrossRef] [PubMed]
- van den Heuvel, D.; Veer, A.; Greuel, H.W. Geriatric health care structures in Germany. The cross-border cooperation in geriatric medicine as a needs-driven furhter development. Z. Gerontol. Geriatr. 2014, 47, 13–16. [Google Scholar] [CrossRef] [PubMed]
- Baztán, J.J.; Suárez-García, F.M.; López-Arrieta, J.; Rodríguez-Mañas, L.; Rodríguez-Artalejo, F. Effectiveness of acute geriatric units on functional decline, living at home, and case fatality among older patients admitted to hospital for acute medical disorders: Meta-analysis. BMJ 2009, 338, b50. [Google Scholar] [CrossRef] [PubMed]
- Hickman, L.D.; Phillips, J.L.; Newton, P.J.; Halcomb, E.J.; Al Abed, N.; Davidson, P.M. Multidisciplinary team interventions to optimise health outcomes for older people in acute care settings: A systematic review. Arch. Gerontol. Geriatr. 2015, 61, 322–329. [Google Scholar] [CrossRef]
- Landefeld, C.S.; Palmer, R.M.; Kresevic, D.M.; Fortinsky, R.H.; Kowal, J. A randomized trial of care in a hospital medical unit especially designed to improve outcomes of acutely ill older patients. N. Engl. J. Med. 2015, 332, 1338–1344. [Google Scholar] [CrossRef]
- Parker, S.G.; McCue, P.; Phelps, K.; McCleod, A.; Arora, S.; Nockels, K.; Kennedy, S.; Roberts, H.; Conroy, S. What is Comprehensive Geriatric Assessment (CGA)? An umbrella review. Age Ageing 2018, 47, 149–155. [Google Scholar] [CrossRef]
- Rubenstein, L.Z.; Stuck, A.E.; Siu, A.L.; Wieland, D. Impacts of geriatric evaluation and management programs on defined outcomes: Overview of the evidence. J. Am. Geriatr. Soc. 1991, 39, 8S–16S. [Google Scholar] [CrossRef]
- Wells, J.L.; Seabrook, J.A.; Stolee, P.; Borrie, M.J.; Knoefel, F. State of the art in geriatric rehabilitation. Part I: Review of frailty and comprehensive geriatric assessment. Arch. Phys. Med. Rehabil. 2003, 84, 890–897. [Google Scholar] [CrossRef]
- Abd Aziz, N.A.S.; Teng, N.I.M.F.; Abdul Hamid, M.R.; Ismail, N.H. Assessing the nutritional status of hospitalized elderly. Clin. Interv. Aging 2014, 12, 1615–1625. [Google Scholar] [CrossRef]
- Brown, P.J.; Sneed, J.R.; Rutherford, B.R.; Devanand, D.P.; Roose, S.P. The nuances of cognition and depression in older adults: The need for a comprehensive assessment. Int. J. Geriatr. Psychiatry 2014, 29, 506–514. [Google Scholar] [CrossRef]
- De Coninck, L.; Bekkering, G.E.; Bouckaert, L.; Declercq, A.; Graff, M.J.L.; Aertgeerts, B. Home- and Community-Based Occupational Therapy Improves Functioning in Frail Older People: A Systematic Review. J. Am. Geriatr. Soc. 2017, 65, 1863–1869. [Google Scholar] [CrossRef]
- Lancaster, J. Dysphagia: Its nature, assessment and management. Br. J. Community Nurs. 2015, 20, S28–S32. [Google Scholar] [CrossRef]
- Morimoto, S.S.; Kanellopoulos, D.; Manning, K.J.; Alexopoulos, G.S. Diagnosis and treatment of depression and cognitive impairment in late life. Ann. N. Y. Acad. Sci. 2015, 1345, 36–46. [Google Scholar] [CrossRef]
- Pilotto, A.; Cella, A.; Pilotto, A.; Daragjati, J.; Veronese, N.; Musacchio, C.; Mello, A.M.; Logroscino, G.; Padovani, A.; Prete, C.; et al. Three Decades of Comprehensive Geriatric Assessment: Evidence Coming from Different Healthcare Settings and Specific Clinical Conditions. J. Am. Med. Dir. Assoc. 2016, 18, e1–e192. [Google Scholar] [CrossRef]
- Sherrington, C.; Tiedemann, A. Physiotherapy in the prevention of falls in older people. J. Physiother. 2015, 61, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Steultjens, E.M.; Dekker, J.; Bouter, L.M.; Jellema, S.; Bakker, E.B.; van den Ende, C.H. Occupational therapy for community dwelling elderly people: A systematic review. Age Ageing 2004, 33, 453–460. [Google Scholar] [CrossRef]
- Afilalo, J.; Alexander, K.P.; Mack, M.J.; Maurer, M.S.; Green, P.; Allen, L.A.; Popma, J.J.; Ferrucci, L.; Forman, D.E. Frailty assessment in the cardiovascular care of older adults. J. Am. Coll. Cardiol. 2014, 63, 747–762. [Google Scholar] [CrossRef]
- Dodson, J.A.; Matlock, D.D.; Forman, D.E. Geriatric Cardiology: An Emerging Discipline. Can. J. Cardiol. 2016, 32, 1056–1064. [Google Scholar] [CrossRef] [PubMed]
- Fischer, K.; Trombik, M.; Freystätter, G. Timeline of functional recovery after hip fracture in seniors aged 65 and older: A prospective observational analysis. Osteoporos. Int. 2019, 30, 1371–1381. [Google Scholar] [CrossRef] [PubMed]
- Fisher, J.M.; Bates, C.; Banerjee, J. The growing challenge of major trauma in older people: A role for comprehensive geriatric assessment? Age Ageing 2017, 46, 709–712. [Google Scholar] [CrossRef] [PubMed]
- Laflamme, G.Y.; Rouleau, D.M.; Leduc, S. The Timed up and Go test is an early predictor of functional outcome after hemiarthroplasty for femoral neck fracture. J. Bone Joint Surg. Am. 2012, 94, 1175–1179. [Google Scholar] [CrossRef] [PubMed]
- Namioka, N.; Hanyu, H.; Hatanaka, H. Comprehensive geriatric assessment in elderly patients with dementia. Geriatr. Gerontol. Int. 2015, 15, 27–33. [Google Scholar] [CrossRef]
- Zanker, J.; Duque, G. Rapid Geriatric Assessment of Hip Fracture. Clin. Geriatr. Med. 2017, 33, 369–382. [Google Scholar] [CrossRef]
- Lin, S.N.; Su, S.F.; Yeh, W.T. Meta-analysis: Effectiveness of Comprehensive Geriatric Care for Elderly Following Hip Fracture Surgery. West. J. Nurs. Res. 2019, 42, 293–305. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Li, C.; Zhang, Y.; Jia, Y.; Zhu, Y.; Sun, R.; Li, W.; Liu, Y. The influence of inpatient comprehensive geriatric care on elderly patients with hip fractures: A meta-analysis of randomized controlled trials. Int. J. Clin. Exp. Med. 2015, 8, 19815–19830. [Google Scholar] [PubMed]
- Wang, Y.; Tang, J.; Zhou, F.; Yang, L.; Wu, J. Comprehensive geriatric care reduces acute perioperative delirium in elderly patients with hip fractures: A meta-analysis. Medicine 2017, 96, e7361. [Google Scholar] [CrossRef]
- Tanislav, C.; Grittner, U.; Misselwitz, B.; Jungehuelsing, G.J.; Enzinger, C.; von Sarnowski, B.; Putaala, J.; Kaps, M.; Kropp, P.; Rolfs, A.; et al. Lessons from everyday stroke care for clinical research and vice versa: Comparison of a comprehensive and a research population of young stroke patients. BMC Neurol. 2014, 14, 45. [Google Scholar] [CrossRef]
- Tanislav, C.; Milde, S.; Schwartzkopff, S.; Misselwitz, B.; Sieweke, N.; Kaps, M. Baseline characteristics in stroke patients with atrial fibrillation: Clinical trials versus clinical practice. BMC Res. Notes 2015, 8, 262. [Google Scholar] [CrossRef]
- Concato, J.; Shah, N.; Horwitz, R.I. Randomized controlled trials, observational studies, and the hierarchy of research designs. N. Engl. J. Med. 2000, 342, 1887–1892. [Google Scholar] [CrossRef]
- Kent, D.M.; Nelson, J.; Dahabreh, I.J.; Rothwell, P.M.; Altman, D.G.; Hayward, R.A. Risk and treatment effect heterogeneity: Re-analysis of individual participant data from 32 large clinical trials. Int. J. Epidemiol. 2016, 45, 2075–2088. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.D.; Rahman, Z.U.; Sledge, G.W.J. Selection bias in clinical trials. Breast Dis. 2001, 14, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Åhlund, K.; Bäck, M.; Öberg, B.; Ekerstad, N. Effects of comprehensive geriatric assessment on physical fitness in an acute medical setting for frail elderly patients. Clin. Interv. Aging 2017, 12, 1929–1939. [Google Scholar] [CrossRef] [PubMed]
- Thingstad, P.; Taraldsen, K.; Saltvedt, I.; Sletvold, O.; Vereijken, B.; Lamb, S.E.; Helbostad, J.L. The long-term effect of comprehensive geriatric care on gait after hip fracture: The Trondheim Hip Fracture Trial—A randomised controlled trial. Osteoporos. Int. 2016, 27, 933–942. [Google Scholar] [CrossRef]
- Blodgett, J.M.; Theou, O.; Mitnitski, A.; Howlett, S.E.; Rockwood, K. Associations between a laboratory frailty index and adverse health outcomes across age and sex. Aging Med. 2019, 2, 11–17. [Google Scholar] [CrossRef]
- Negrini, F.; Preti, M.; Zirone, E.; Mazziotti, D.; Biffi, M.; Pelosi, C.; Banfi, G.; Zapparoli, L. The importance of cognitive executive functions in gait recovery after total hip arthroplasty. Arch. Phys. Med. Rehabil. 2020, 101, 579–586. [Google Scholar] [CrossRef]
- Prestmo, A.; Saltvedt, I.; Helbostad, J.L.; Taraldsen, K.; Thingstad, P.; Lydersen, S.; Sletvold, O. Who benefits from orthogeriatric treatment? Results from the Trondheim hip-fracture trial. BMC Geriatr. 2016, 16, 49. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
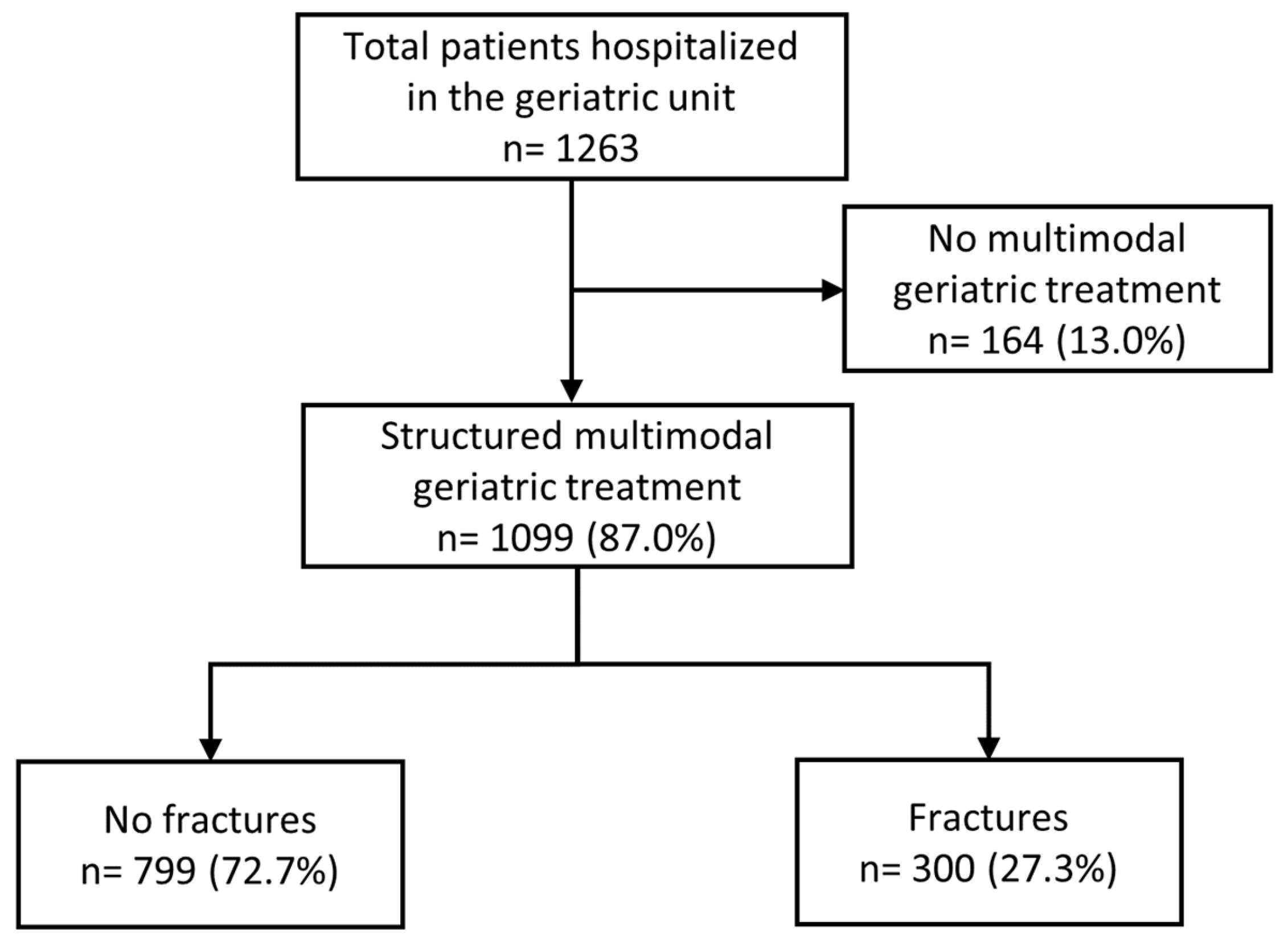
| Total Group (n = 1099) | Fractures (n = 300) | No Fractures (n = 799) | p * | |
|---|---|---|---|---|
| Age (median, IQR, years) | 83.1 (79.0–87.8) | 85.6 (81.1–89.6) | 82.4 (78.3–86.9) | 0.001 |
| Age ≥ 80 years | 754 (68.6%) | 239 (79.7%) | 515 (64.5%) | 0.001 |
| Sex | ||||
| Female | 704 (64.1%) | 219 (73.0%) | 485 (60.7%) | 0.001 |
| Male | 395 (35.9%) | 81 (27.0%) | 314 (39.3%) | |
| Co-morbidities | ||||
| Hypertension | 853 (77.6%) | 246 (82.0%) | 607(76.0%) | 0.035 |
| Diabetes mellitus | 337 (30.7%) | 69 (23.0%) | 268 (33.5%) | 0.001 |
| Heart failure | 258 (23.5%) | 66 (22.0%) | 192 (24.0%) | 0.523 |
| Renal insufficiency | 382 (34.8%) | 86 (28.7%) | 296 (37.0%) | 0.010 |
| Coronary heart disease | 281 (25.6%) | 61 (20.3%) | 220 (27.5%) | 0.016 |
| Peripheral artery disease | 59 (5.4%) | 9 (3.0%) | 50 (6.3%) | 0.035 |
| Atrial fibrillation | 388 (35.3%) | 93 (31.0%) | 295 (36.9%) | 0.076 |
| Chronic pulmonary artery disease | 108 (9.8%) | 18 (6.0%) | 90 (11.3%) | 0.009 |
| Dementia | 226 (20.6%) | 78 (26.0%) | 148 (18.5%) | 0.007 |
| Parkinson’s disease | 62 (5.6%) | 18 (6.0%) | 44 (5.5%) | 0.770 |
| Previous stroke | 90 (8.2%) | 30 (10.0%) | 60 (7.5%) | 0.177 |
| Osteoporosis | 127 (11.6%) | 54 (18.0%) | 73 (9.1%) | 0.001 |
| Vitamin B deficiency ǁ | 484 (%) | 151 (50.3%) | 333 (41.7%) | 0.012 |
| Short-term adverse events while hospitalized | ||||
| Diffuse Pain | 294 (26.8%) | 97 (32.3%) | 197 (24.7%) | 0.012 |
| Delirium | 58 (5.3%) | 14 (4.7%) | 44 (5.5%) | 0.651 |
| Pneumonia | 64 (6.1%) | 15 (5.0%) | 49 (6.1%) | 0.564 |
| Urinary tract infection | 161 (14.3%) | 47 (15.7%) | 114 (14.6%) | 0.566 |
| Dizziness | 82 (7.5%) | 15 (5.0%) | 67 (8.4%) | 0.070 |
| Deep vein thrombosis | 5 (0.5%) | 1 (0.3%) | 4 (0.5%) | 0.999 |
| Pulmonary emboli | 5 (0.5%) | 1 (0.3%) | 4 (0.5%) | 0.999 |
| Electrolyte imbalance | 410 (39.0%) | 98 (32.7%) | 312 (37.3%) | 0.059 |
| Hypokalemia | 103 (9.4%) | 26 (8.7%) | 77 (9.6%) | 0.728 |
| Hyponatremia | 354 (32.2%) | 82 (27.3%) | 272 (34.0%) | 0.036 |
| Functional assessment on admission | ||||
| Barthel Index (median, IQR) | 45 (30–60) | 40 (30–50) | 45 (30–60) | 0.001 |
| Tinetti Geriatric Assessment (median, IQR) | 11 (12–16) | 8 (1–14) | 12 (4–17) | 0.001 |
| Geriatric Depression Scale (median, IQR) | 3 (1–6) | 3 (1–6) | 3 (1–6) | 0.844 |
| Geriatric Depression Scale > 5 | 302 (27.7%) | 83 (27.8%) | 219 (27.6%) | 0.999 |
| Timed Up and Go (median, IQR) | 4 (3–5) | 5 (3–5) | 4 (3–5) | 0.001 |
| MMSE (median, IQR) (n = 812) | 26 (21–28) | 25 (19–28) | 26 (21–28) | 0.282 |
| Patients deceased during hospitalization | 36 (3.3%) | 6 (2.0%) | 30 (3.8%) | 0.183 |
| Functional assessment on discharge | n = 1000 | n = 284 | n = 716 | |
| Barthel Index (median, IQR) | 60 (40–80) | 55 (40–75) | 60 (45–80) | 0.030 |
| Tinetti Geriatric Assessment (median, IQR) | 16 (6–20) | 14 (8–19) | 16 (9–21) | 0.006 |
| Timed Up and Go (median, IQR) | 3 (2–4) | 3 (3–5) | 3 (2–4) | 0.001 |
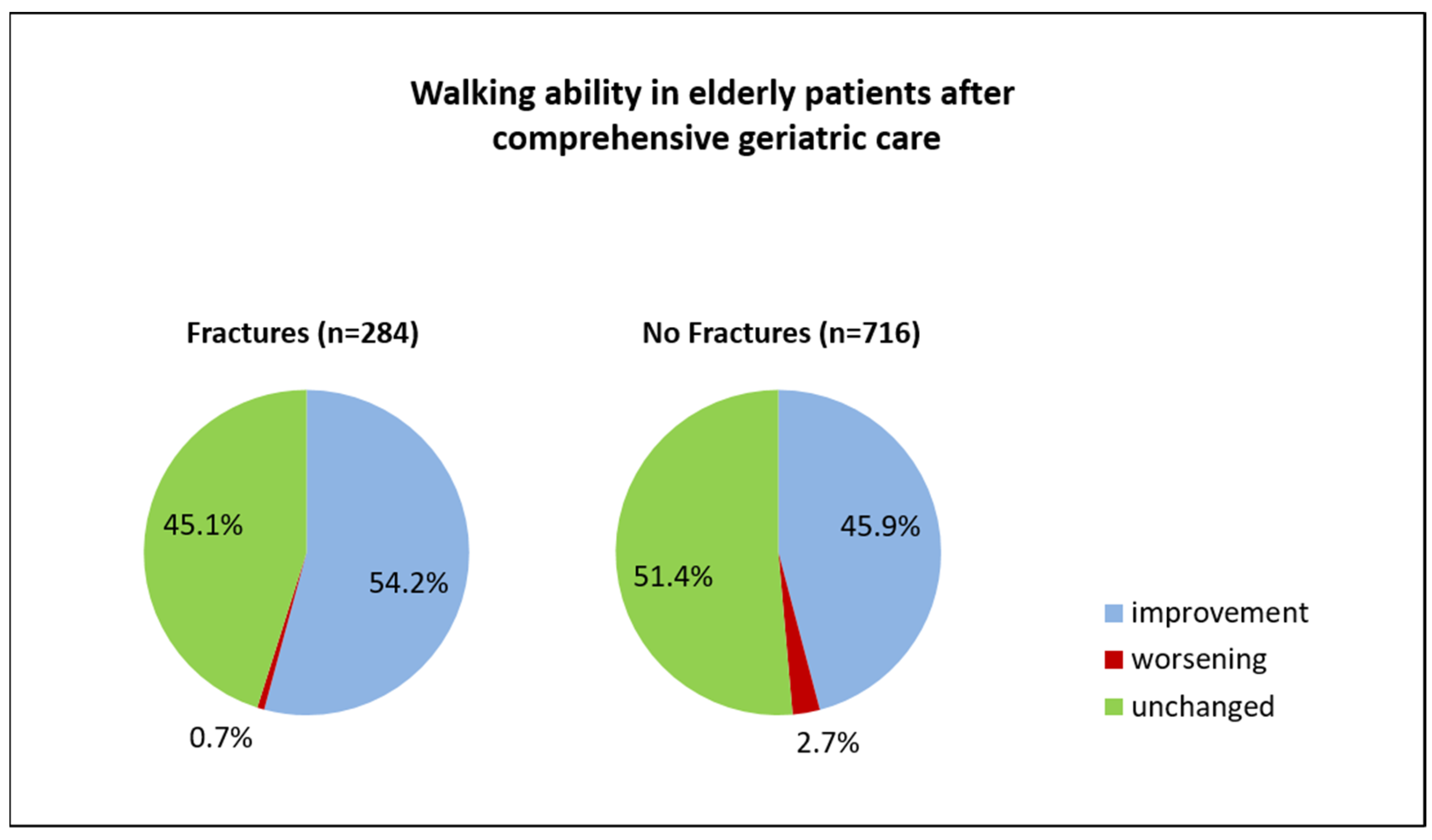
| Timed Up and Go improvement | 483 (48.3%) | 154 (54.2%) | 329 (45.9%) | 0.021 |
| Discharging modus | n = 1063 | n = 294 | n = 769 | |
| Regular discharge ‡ | 1041 (97.9%) | 291 (99%) | 750 (97.5%) | 0.156 |
| Referral to other department | 22 (2.1%) | 3 (1.0%) | 19 (2.5%) | 0.156 |
| Length of hospital stay for patients with CGC ¥ (median, IQR, days) | 17 (16–19) | 17 (16–19) | 16 (16–19) | 0.014 |
| Total Group (n = 284) | Improvement in Walking Ability (n = 154) | No Improvement in Walking Ability (n = 130) | p * | |
|---|---|---|---|---|
| Age (median, IQR, years) | 85.6 (81.1–89.9) | 84.9 (81.1–89.4) | 86.4 (81.2–90.7) | 0.250 |
| Age ≥ 80 years | 228 (80.3%) | 124 (80.5%) | 104 (80.0%) | 0.999 |
| Sex | ||||
| Female | 210 (73.9%) | 113 (73.4%) | 97 (74.6%) | 0.892 |
| Male | 74 (26.1%) | 41 (26.6%) | 33 (25.4%) | |
| Co-morbidities | ||||
| Hypertension | 231 (81.3%) | 123 (79.9%) | 108 (83.1%) | 0.534 |
| Diabetes mellitus | 66 (23.2%) | 33 (21.4%) | 33 (25.4%) | 0.482 |
| Heart failure | 60 (21.1%) | 32 (20.8%) | 28 (21.5%) | 0.885 |
| Renal insufficiency | 82 (28.9%) | 47 (30.5%) | 35 (26.9%) | 0.515 |
| Coronary heart disease | 56 (19.7%) | 31 (20.1%) | 25 (19.2%) | 0.882 |
| Peripheral artery disease | 9 (3.2%) | 5 (3.2%) | 4 (3.1%) | 0.999 |
| Atrial fibrillation | 87 (30.6%) | 47 (30.5%) | 40 (30.8%) | 0.999 |
| Chronic pulmonary artery disease | 16 (5.6%) | 8 (5.2%) | 8 (6.2%) | 0.799 |
| Dementia | 74 (26.1%) | 33 (21.4%) | 41 (31.5%) | 0.058 |
| Parkinson’s disease | 18 (6.3%) | 8 (5.2%) | 10 (7.7%) | 0.467 |
| Previous stroke | 27 (9.5%) | 12 (7.8%) | 15 (11.5%) | 0.314 |
| Osteoporosis | 53 (18.7%) | 35 (22.7%) | 18 (13.8%) | 0.067 |
| Vitamin B deficiency ǁ | 144 (50.7%) | 75 (48.7%) | 69 (53.1%) | 0.477 |
| Short-term adverse events while hospitalized | ||||
| Diffuse pain | 91 (32.0%) | 49 (31.8%) | 42 (32.3%) | 0.999 |
| Delirium | 14 (4.9%) | 7 (4.5%) | 7 (5.4%) | 0.789 |
| Pneumonia | 11 (3.9%) | 5 (3.2%) | 6 (4.6%) | 0.557 |
| Urinary tract infection | 45 (15.8%) | 25 (16.2%) | 20 (15.4%) | 0.872 |
| Dizziness | 14 (4.9%) | 10 (6.5%) | 4 (3.1%) | 0.272 |
| Deep vein thrombosis | 1 (0.4%) | 0 (0%) | 1 (0.8%) | 0.458 |
| Pulmonary emboli | 1 (0.4%) | 0 (0%) | 1 (0.8%) | 0.458 |
| Electrolyte imbalance | 91 (32.0%) | 50 (32.5%) | 41 (31.5%) | 0.899 |
| Hypokalemia | 25 (8.8%) | 16 (10.4%) | 9 (6.9%) | 0.401 |
| Hyponatremia | 75 (26.4%) | 41 (26.6%) | 34 (26.2%) | 0.999 |
| Functional assessment on admission | ||||
| Barthel index (median, IQR) | 40 (30–50) | 45 (35–55) | 35 (20–50) | 0.001 |
| Tinetti on admission (median, IQR) | 8 (1–14) | 9 (4–14.25) | 5 (0–13) | 0.001 |
| Geriatric depression scale (median, IQR) | 3 (1–6) | 4 (1.75–6) | 3 (0–6) | 0.134 |
| Geriatric depression scale >5 | 77 (27.1%) | 42 (27.3%) | 35 (26.9%) | 0.999 |
| Timed up and go (median, IQR) | 5 (3–5) | 5 (4–5) | 5 (3–5) | 0.151 |
| MMSE (median, IQR) (n = 226) | 25 (19–28) | 26 (19–28) | 25 (19–28) | 0.779 |
| Length of hospital stay for CGC ¥ (median, IQR, days) | 17 (16–19) | 17 (16–19) | 17 (16–19) | 0.895 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niemöller, U.; Arnold, A.; Stein, T.; Juenemann, M.; Erkapic, D.; Rosenbauer, J.; Kostev, K.; Meyer, M.; Tanislav, C. Comprehensive Geriatric Care in Older Adults: Walking Ability after an Acute Fracture. Med. Sci. 2023, 11, 40. https://doi.org/10.3390/medsci11020040
Niemöller U, Arnold A, Stein T, Juenemann M, Erkapic D, Rosenbauer J, Kostev K, Meyer M, Tanislav C. Comprehensive Geriatric Care in Older Adults: Walking Ability after an Acute Fracture. Medical Sciences. 2023; 11(2):40. https://doi.org/10.3390/medsci11020040
Chicago/Turabian StyleNiemöller, Ulrich, Andreas Arnold, Thomas Stein, Martin Juenemann, Damir Erkapic, Josef Rosenbauer, Karel Kostev, Marco Meyer, and Christian Tanislav. 2023. "Comprehensive Geriatric Care in Older Adults: Walking Ability after an Acute Fracture" Medical Sciences 11, no. 2: 40. https://doi.org/10.3390/medsci11020040
APA StyleNiemöller, U., Arnold, A., Stein, T., Juenemann, M., Erkapic, D., Rosenbauer, J., Kostev, K., Meyer, M., & Tanislav, C. (2023). Comprehensive Geriatric Care in Older Adults: Walking Ability after an Acute Fracture. Medical Sciences, 11(2), 40. https://doi.org/10.3390/medsci11020040