Verbal Interactional Synchronization between Therapist and Children with Autism Spectrum Disorder during Dolphin Assisted Therapy: Five Case Studies

 , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
2.2. Participants
2.3. Procedure
2.4. Measurements
Coding of Verbal Behavior
2.5. Data Analysis
3. Results
3.1. Participant 1
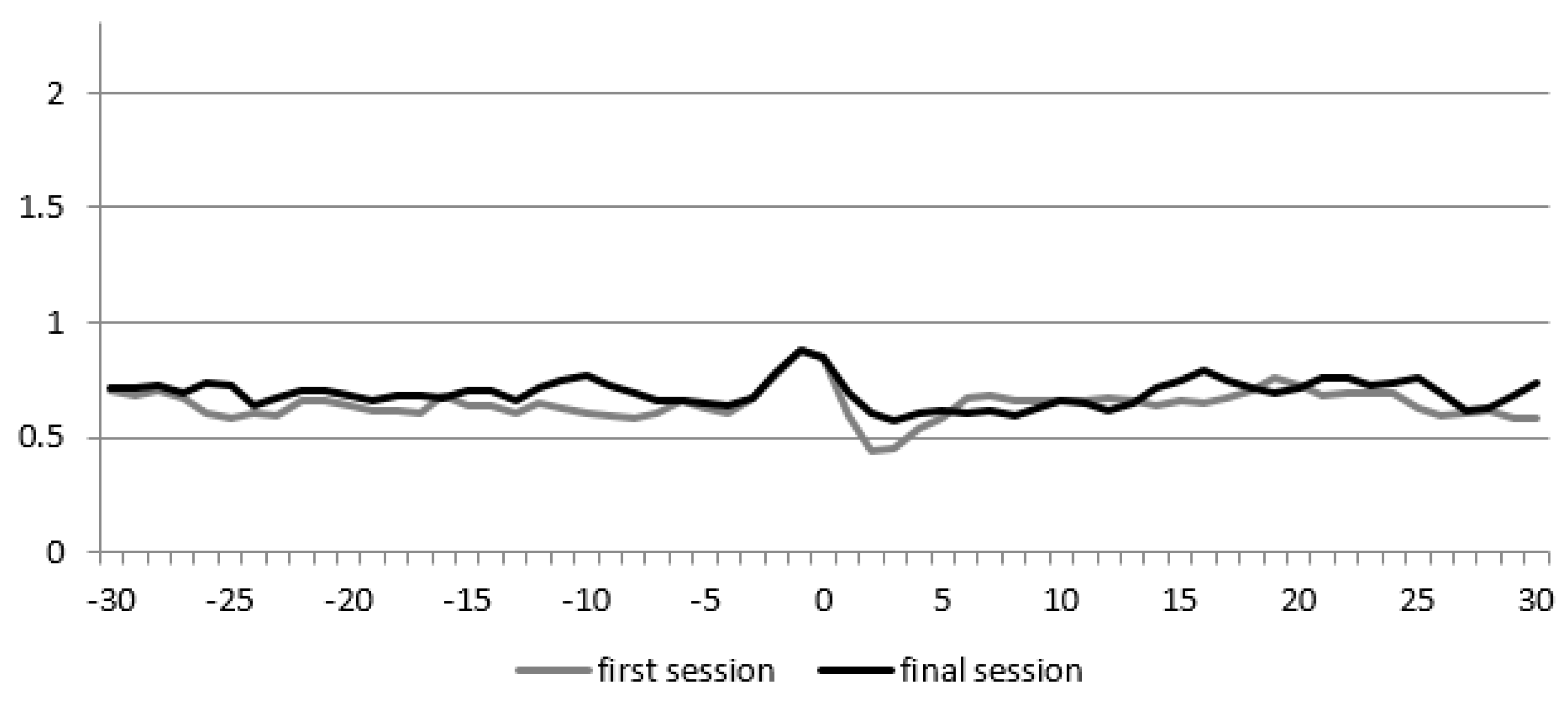
Analysis of Turn-Taking
3.2. Participant 2
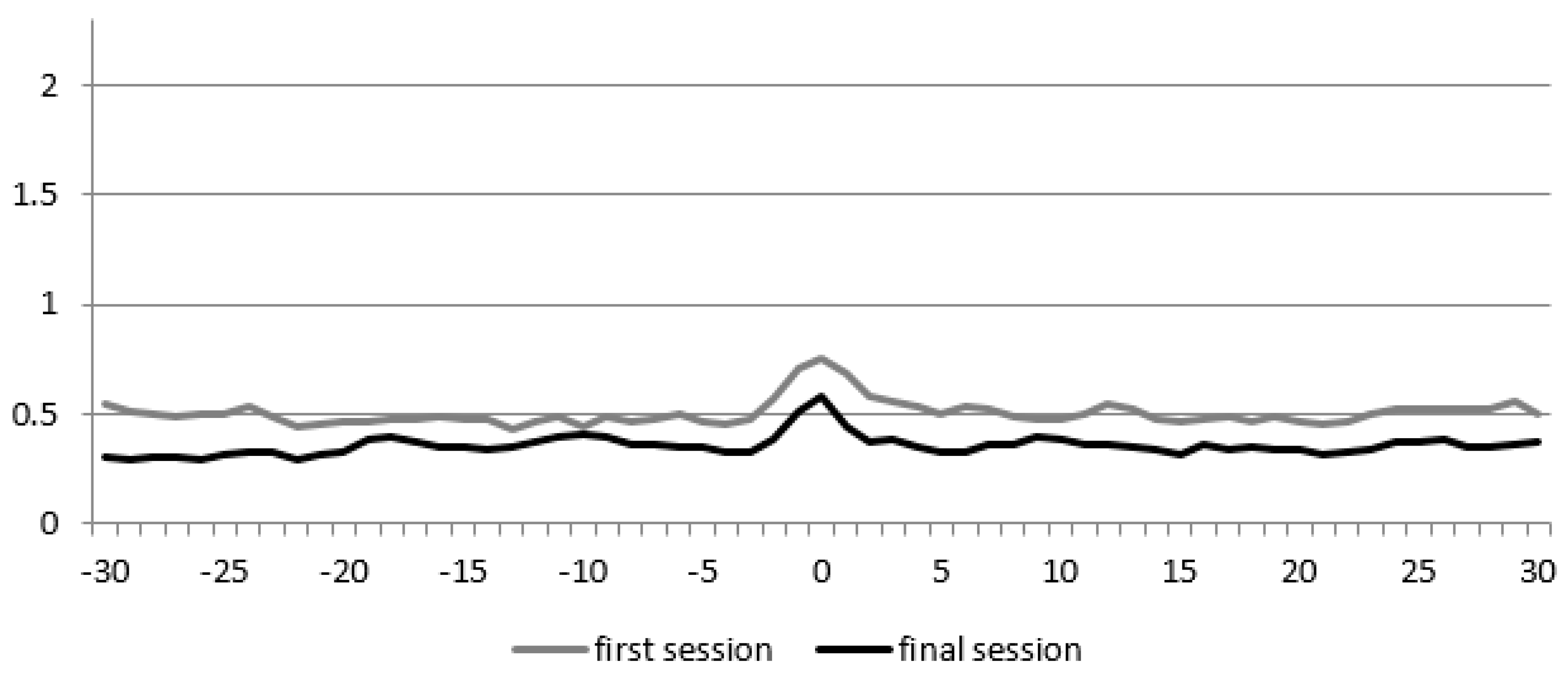
Analysis of Turn-Taking
3.3. Participant 3
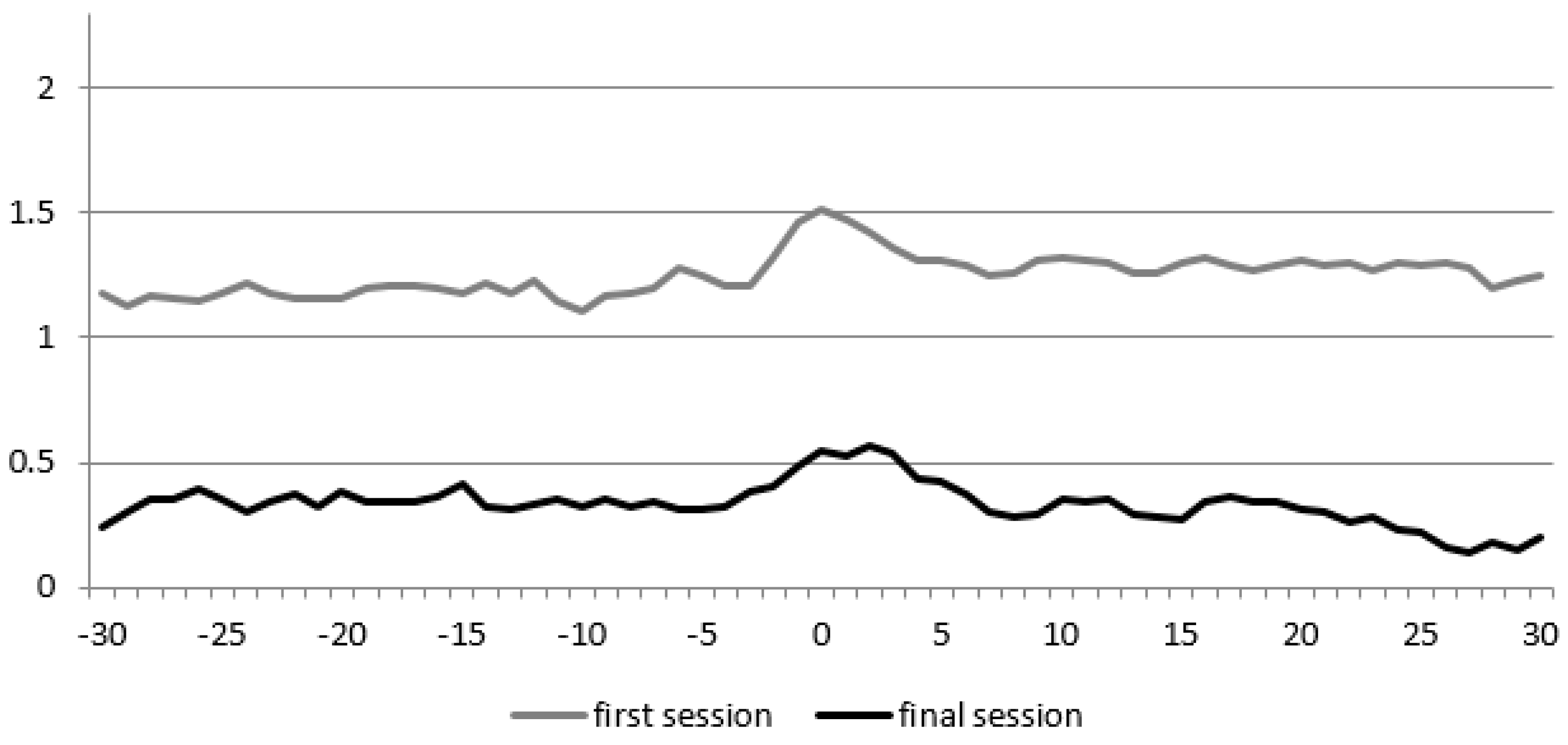
Analysis of Turn-Taking
3.4. Participant 4
Analysis of Turn-Taking
3.5. Participant 5
Analysis of Turn-Taking
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®)—American Psychiatric Association—Google Boeken. 2013. Available online: https://books.google.nl/books?hl=nl&lr=&id=-JivBAAAQBAJ&oi=fnd&pg=PT18&dq=%22dsm+5%22+manual+of+mental+disorders&ots=ceTK12NKvb&sig=CyFdgiiY2Vqv5oJXqT7YEG-x07w#v=onepage&q=%22dsm 5%22 manual of mental disorders&f=false (accessed on 11 June 2019).
- Mody, M.; Belliveau, J.W. Speech and Language Impairments in Autism: Insights from Behavior and Neuroimaging. N. Am. J. Med. Sci. 2013, 5, 157–161. [Google Scholar] [CrossRef]
- Sterling, A. Grammar in Boys With Idiopathic Autism Spectrum Disorder and Boys with Fragile X Syndrome Plus Autism Spectrum Disorder. J. Speech Lang. Hear. Res. 2018, 61, 857. [Google Scholar] [CrossRef] [PubMed]
- Volden, J.; Coolican, J.; Garon, N.; White, J.; Bryson, S. Brief Report: Pragmatic Language in Autism Spectrum Disorder: Relationships to Measures of Ability and Disability. J. Autism Dev. Disord. 2009, 39, 388–393. [Google Scholar] [CrossRef] [PubMed]
- Landa, R. Early communication development and intervention for children with autism. Ment. Retard. Dev. Disabil. Res. Rev. 2007, 13, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Rutgers, A.H.; Bakermans-Kranenburg, M.J.; Ijzendoorn, M.H.; Berckelaer-Onnes, I.A. Autism and attachment: A meta-analytic review. J. Child Psychol. Psychiatry 2004, 45, 1123–1134. [Google Scholar] [CrossRef] [PubMed]
- Watt, N.; Wetherby, A.; Shumway, S. Prelinguistic Predictors of Language Outcome at 3 Years of Age. J. Speech Lang. Hear. Res. 2006, 49, 1224. [Google Scholar] [CrossRef]
- Feldman, R. Parent-infant synchrony and the construction of shared timing; physiological precursors, developmental outcomes, and risk conditions. J. Child Psychol. Psychiatry 2007, 48, 329–354. [Google Scholar] [CrossRef]
- Harrist, A.W.; Waugh, R.M. Dyadic synchrony: Its structure and function in children’s development. Dev. Rev. 2002, 22, 555–592. [Google Scholar] [CrossRef]
- Lindsey, E.W.; Cremeens, P.R.; Colwell, M.J.; Caldera, Y.M. The Structure of Parent-Child Dyadic Synchrony in Toddlerhood and Children’s Communication Competence and Self-control. Soc. Dev. 2009, 18, 375–396. [Google Scholar] [CrossRef]
- Trevarthen, C. Neuroembryology and the Development of Perception. In Human Growth; Springer: Boston, MA, USA, 1979; pp. 3–96. [Google Scholar]
- Bernieri, F.J.; Rosenthal, R. Interpersonal coordination: Behavior matching and interactional synchrony. In Fundamentals of Nonverbal Behavior; Feldman, R.S., Rime, B., Eds.; Cambridge University Press: Cambridge, UK, 1991. [Google Scholar]
- Fogel, A. Developing through Relationships: Origins of Communication, Self, and Culture; University of Chicago Press: Chicago, IL, USA, 1993. [Google Scholar]
- Stern, D. The issue of vitality. Nord. J. Music Ther. 2010, 19, 88–102. [Google Scholar] [CrossRef]
- Leclère, C.; Viaux, S.; Avril, M.; Achard, C.; Chetouani, M.; Missonnier, S.; Cohen, D. Why Synchrony Matters during Mother-Child Interactions: A Systematic Review. PLoS ONE 2014, 9, e113571. [Google Scholar] [CrossRef]
- Reuzel, E.; Embregts, P.J.C.M.; Bosman, A.M.T.; Cox, R.; van Nieuwenhuijzen, M.; Jahoda, A. Conversational Synchronization in Naturally Occurring Settings: A Recurrence-Based Analysis of Gaze Directions and Speech Rhythms of Staff and Clients with Intellectual Disability. J. Nonverbal Behav. 2013, 37, 281–305. [Google Scholar] [CrossRef]
- Forster, S.; Iacono, T. The nature of affect attunement used by disability support workers interacting with adults with profound intellectual and multiple disabilities. J. Intellect. Disabil. Res. 2014, 58, 1105–1120. [Google Scholar] [CrossRef]
- Jaffe, J.; Beebe, B.; Feldstein, S.; Crown, C.L.; Jasnow, M.D.; Rochat, P.; Stern, D.N. Rhythms of Dialogue in Infancy: Coordinated Timing in Development. Monogr. Soc. Res. Child Dev. Rhythm Dialogue Infancy Coord Timing Dev. 2001, 66, 149. [Google Scholar]
- Marsh, K.L.; Richardson, M.J.; Schmidt, R.C. Social Connection Through Joint Action and Interpersonal Coordination. Top. Cogn. Sci. 2009, 1, 320–339. [Google Scholar] [CrossRef]
- Fitzpatrick, P.; Diorio, R.; Richardson, M.J.; Schmidt, R.C. Dynamical methods for evaluating the time-dependent unfolding of social coordination in children with autism. Front. Integr. Neurosci. 2013, 7, 21. [Google Scholar] [CrossRef] [Green Version]
- Lord, C.; Risi, S.; Lambrecht, L.; Cook, E.H.; Leventhal, B.L.; DiLavore, P.C.; Pickles, A.; Rutter, M. The Autism Diagnostic Observation Schedule—Generic: A Standard Measure of Social and Communication Deficits Associated with the Spectrum of Autism. J. Autism Dev. Disord. 2000, 30, 205–223. [Google Scholar] [CrossRef]
- Marsh, K.L.; Isenhower, R.W.; Richardson, M.J.; Helt, M.; Verbalis, A.D.; Schmidt, R.C.; Fein, D. Autism and social disconnection in interpersonal rocking. Front. Integr. Neurosci. 2013, 7, 4. [Google Scholar] [CrossRef] [Green Version]
- Osterling, J.A.; Dawson, G.; Munson, J.A. Early recognition of 1-year-old infants with autism spectrum disorder versus mental retardation. Dev. Psychopathol. 2002, 14, 239–251. [Google Scholar] [CrossRef] [Green Version]
- Kasari, C.; Locke, J.; Gulsrud, A.; Rotheram-Fuller, E. Social Networks and Friendships at School: Comparing Children With and Without ASD. J. Autism Dev. Disord. 2011, 41, 533–544. [Google Scholar] [CrossRef]
- Dumas, G.; Nadel, J.; Soussignan, R.; Martinerie, J.; Garnero, L. Inter-Brain Synchronization during Social Interaction. PLoS ONE 2010, 5, e12166. [Google Scholar] [CrossRef]
- Levinson, S.C. Turn-taking in Human Communication—Origins and Implications for Language Processing. Trends Cogn. Sci. 2016, 20, 6–14. [Google Scholar] [CrossRef]
- Pika, S.; Wilkinson, R.; Kendrick, K.H.; Vernes, S.C. Taking turns: Bridging the gap between human and animal communication. Proc. Biol. Sci. 2018, 285, 20180598. [Google Scholar] [CrossRef]
- Stivers, T.; Enfield, N.J.; Brown, P.; Englert, C.; Hayashi, M.; Heinemann, T.; Hoymann, G.; Rossano, F.; De Ruiter, J.P.; Yoon, K.E.; et al. Universals and cultural variation in turn-taking in conversation. Proc. Natl. Acad. Sci. USA 2009, 106, 10587–10592. [Google Scholar] [CrossRef] [Green Version]
- Siller, M.; Sigman, M. The Behaviors of Parents of Children with Autism Predict the Subsequent Development of Their Children’s Communication. J. Autism Dev. Disord. 2002, 32, 77–89. [Google Scholar] [CrossRef]
- Steiner, A.M.; Gengoux, G.W.; Smith, A.; Chawarska, K. Parent-Child Interaction Synchrony for Infants At-Risk for Autism Spectrum Disorder. J. Autism Dev. Disord. 2018, 48, 3562–3572. [Google Scholar] [CrossRef]
- Yoder, P.; Stone, W.L. Randomized Comparison of Two Communication Interventions for Preschoolers with Autism Spectrum Disorders. J. Consult. Clin. Psychol. 2006, 74, 426. [Google Scholar] [CrossRef]
- Bureau, J.F.; Martin, J.; Yurkowski, K.; Schmiedel, S.; Quan, J.; Moss, E.; Deneault, A.A.; Pallanca, D. Correlates of child–father and child-mother attachment in the preschool years. Attach. Hum. Dev. 2017, 19, 130–150. [Google Scholar] [CrossRef]
- Sable, P. The Pet Connection: An Attachment Perspective. Clin. Soc. Work J. 2013, 41, 93–99. [Google Scholar] [CrossRef]
- Griffioen, R.E.; Enders-Slegers, M.-J. The Effect of Dolphin-Assisted Therapy on the Cognitive and Social Development of Children with Down Syndrome. Anthrozoos 2014, 27, 569–580. [Google Scholar] [CrossRef]
- O’Haire, M.E.; McKenzie, S.J.; McCune, S.; Slaughter, V. Effects of Classroom Animal-Assisted Activities on Social Functioning in Children with Autism Spectrum Disorder. J. Altern. Complement. Med. 2014, 20, 162–168. [Google Scholar] [CrossRef] [Green Version]
- Becker, J.L.; Rogers, E.C.; Burrows, B. Animal-assisted Social Skills Training for Children with Autism Spectrum Disorders. Anthrozoos 2017, 30, 307–326. [Google Scholar] [CrossRef]
- Silva, K.; Correia, R.; Lima, M.; Magalhães, A.; de Sousa, L. Can Dogs Prime Autistic Children for Therapy? Evidence from a Single Case Study. J. Altern. Complement. Med. 2011, 17, 655–659. [Google Scholar] [CrossRef]
- Nimer, J.; Lundahl, B. Animal-Assisted Therapy: A Meta-Analysis. Anthrozoos 2007, 20, 225–238. [Google Scholar] [CrossRef] [Green Version]
- Kamioka, H.; Okada, S.; Tsutani, K.; Park, H.; Okuizumi, H.; Handa, S.; Oshio, T.; Park, S.J.; Kitayuguchi, J.; Abe, T.; et al. Effectiveness of animal-assisted therapy: A systematic review of randomized controlled trials. Complement. Ther. Med. 2014, 22, 371–390. [Google Scholar] [CrossRef]
- Parish-Plass, N. Animal-Assisted Psychotherapy: Theory, Issues, and Practice. 2013. Available online: https://books.google.nl/books?hl=nl&lr=&id=5p12K4pN2iYC&oi=fnd&pg=PR13&dq=transmission+triangle+in+psychotherapy&ots=-pGGXTuPHh&sig=L92PJeYTAR3q8aAoWzIFwJPCoaI#v=onepage&q=transmission triangle in psychotherapy&f=false (accessed on 21 August 2018).
- Nathanson, D.; Castro, D.; de Friend, H.; McMahon, M. Effectiveness of short-term dolphin-assisted therapy for children with severe disabilities. Anthrozoos 1997, 10, 90–100. [Google Scholar] [CrossRef]
- Nathanson, D.E. Long-Term Effectiveness of Dolphin-Assisted Therapy for Children with Severe Disabilities. Anthrozoos 1998, 11, 22–32. [Google Scholar] [CrossRef]
- Breitenbach, E.; Stumpf, E.; Fersen, L.V.; Ebert, H. Dolphin-Assisted Therapy: Changes in Interaction and Communication between Children with Severe Disabilities and Their Caregivers. Anthrozoos 2009, 22, 277–289. [Google Scholar] [CrossRef]
- Servais, V. Some Comments on Context Embodiment in Zootherapy: The Case of the Autidolfijn Project. Anthrozoos 1999, 12, 5–15. [Google Scholar] [CrossRef]
- O’Haire, M.E.; McKenzie, S.J.; Beck, A.M.; Slaughter, V. Social behaviors increase in children with autism in the presence of animals compared to toys. PLoS ONE 2013, 8, e57010. [Google Scholar] [CrossRef]
- O’Haire, M.E. Research on animal-assisted intervention and autism spectrum disorder, 2012–2015. Appl. Dev. Sci. 2017, 21, 200–216. [Google Scholar] [CrossRef]
- Bachi, K.; Parish-Plass, N. Animal-assisted psychotherapy: A unique relational therapy for children and adolescents. Clin. Child Psychol. Psychiatry 2017, 22, 3–8. [Google Scholar] [CrossRef]
- Beck, A.M.; Katcher, A.H. Future Directions in Human-Animal Bond Research. Am. Behav. Sci. 2003, 47, 79–93. [Google Scholar] [CrossRef]
- Steenbeek, H.W.; van Geert, P.L.C. A Theory and Dynamic Model of Dyadic Interaction: Concerns, Appraisals, and Contagiousness in a Developmental Context. Available online: www.elsevier.com/locate/dr (accessed on 16 January 2017).
- Marwan, N.; Carmenromano, M.; Thiel, M.; Kurths, J. Recurrence plots for the analysis of complex systems. Phys. Rep. 2007, 438, 237–329. [Google Scholar] [CrossRef]
- Marwan, N.; Webber, C.L. Mathematical and Computational Foundations of Recurrence Quantifications; Springer: Cham, Switzerland, 2015; pp. 3–43. [Google Scholar]
- Zbilut, J.P.; Giuliani, A.; Webber, C.L. Recurrence quantification analysis and principal components in the detection of short complex signals. Phys. Lett. A 1998, 237, 131–135. [Google Scholar] [CrossRef] [Green Version]
- Cox, R.F.A.; van Dijk, M. Microdevelopment in Parent-Child Conversations: From Global Changes to Flexibility. Ecol. Psychol. 2013, 25, 304–315. [Google Scholar] [CrossRef]
- Dale, R.; Spivey, M.J. Unraveling the Dyad: Using Recurrence Analysis to Explore Patterns of Syntactic Coordination Between Children and Caregivers in Conversation. Lang. Learn. 2006, 56, 391–430. [Google Scholar] [CrossRef]
- De Jonge-Hoekstra, L.; Van der Steen, S.; Van Geert, P.; Cox, R.F.A. Asymmetric Dynamic Attunement of Speech and Gestures in the Construction of Children’s Understanding. Front. Psychol. 2016, 7, 473. [Google Scholar] [CrossRef]
- López Pérez, D.; Leonardi, G.; Niedźwiecka, A.; Radkowska, A.; Rączaszek-Leonardi, J.; Tomalski, P. Combining Recurrence Analysis and Automatic Movement Extraction from Video Recordings to Study Behavioral Coupling in Face-to-Face Parent-Child Interactions. Front. Psychol. 2017, 8, 2228. [Google Scholar] [CrossRef]
- Vink, R.; Wijnants, M.L.; Cillessen, A.H.N.; Bosman, A.M.T. Cooperative Learning and Interpersonal Synchrony. Nonlinear Dynamics, Psychology, and Life Sciences. 2017. Available online: https://www.researchgate.net/profile/Roy_Vink/publication/316190878_Cooperative_Learning_and_Interpersonal_Synchrony/links/58f5f04ba6fdcc11e56a0605/Cooperative-Learning-and-Interpersonal-Synchrony.pdf (accessed on 19 June 2019).
- Griffioen, R.; Steen, S.; Cox, R.; Verheggen, T.; Enders-Slegers, M. Changes in behavioral synchrony during Dog-assisted therapy for children with Autism spectrum disorder and children with Down syndrome. J. Appl. Res. Intellect. Disabil. 2019. under review. [Google Scholar]
- Cox, R.F.A.; van der Steen, S.; Guevara, M.; de Jonge-Hoekstra, L.; van Dijk, M. Chromatic and Anisotropic Cross-Recurrence Quantification Analysis of Interpersonal Behavior; Springer: Berlin, Germany, 2016; pp. 209–225. [Google Scholar]
- Reuzel, E.; Embregts, P.J.C.M.; Bosman, A.M.T.; Cox, R.F.A.; van Nieuwenhuijzen, M.; Jahoda, A. Verbal interactional dominance and coordinative structure of speech rhythms of staff and clients with an intellectual disability. Nonlinear Dyn. Psychol. Life Sci. 2014, 18, 371–396. [Google Scholar]
- Abney, D.H.; Warlaumont, A.S.; Oller, D.K.; Wallot, S.; Kello, C.T. Multiple Coordination Patterns in Infant and Adult Vocalizations. Infancy 2017, 22, 514–539. [Google Scholar] [CrossRef]
- Nomikou, I.; Leonardi, G.; Rohlfing, K.J.; Rączaszek-Leonardi, J. Constructing Interaction: The Development of Gaze Dynamics. Infant Child Dev. 2016, 25, 277–295. [Google Scholar] [CrossRef] [Green Version]
- Davis, T.J.; Pinto, G.B.; Kiefer, A.W. The Stance Leads the Dance: The Emergence of Role in a Joint Supra-Postural Task. Front. Psychol. 2017, 8, 718. [Google Scholar] [CrossRef]
- Marino, L. Construct validity of animal-assisted therapy and activities: How important is the animal in AAT? Anthrozoös 2012, 25, S139–S151. [Google Scholar] [CrossRef]
- Stanton-Chapman, T.L.; Snell, M.E. Promoting turn-taking skills in preschool children with disabilities: The effects of a peer-based social communication intervention. Early Child Res. Q. 2011, 26, 303–319. [Google Scholar] [CrossRef]
- Noterdaeme, M.; Amorosa, H.; Mildenberger, K.; Sitter, S.; Minow, F. Evaluation of attention problems in children with autism and children with a specific language disorder. Eur. Child Adolesc. Psychiatry 2001, 10, 58–66. [Google Scholar] [CrossRef]
- Travers, B.; Klinger, M.; Klinger, L. The Neuropsychology of Autism—Google Boeken. Attention and Working Memory in ASD. 2011. Available online: https://books.google.nl/books?hl=nl&lr=&id=dSpVikpnJgcC&oi=fnd&pg=PA161&dq=ASD+and+delayed+reaction+time&ots=1-eO3QegZW&sig=I4s3m8UlsWS-FkpMgVutln3mfWk#v=onepage&q=ASD and delayed reaction time&f=false (accessed on 3 June 2019).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant Characteristic | Pp 1 | Pp 2 | Pp 3 | Pp 4 | Pp 5 |
|---|---|---|---|---|---|
| Age | 7.5 | 8.5 | 6 | 7.5 | 8 |
| Gender | Female | Male | Male | Male | Male |
| Diagnosis | ASD | ASD/ADHD | ASD | ASD | ASD |
| Education | Special | Special | Special | Special | Special |
| Medical treatment | - | Salbutamol (Asthma) and Methylphenidate (ADHD) | - | Levetiracetam (Epilepsy) | - |
| Sensory problems | - | - | - | Glasses | Glasses |
| Motor problems | Physiotherapy | - | - | Orthopedic shoes | - |
| Behavioral problems | Anxious and aggressive behavior in unexpected situations | Aggressive toward sibling, often screams, runs away | Easily over-stimulated, repetitive movements | - | Acts young for age, frustration when he cannot pronounce words |
| Participants | Seconds of Spoken Language Participant | Seconds of Spoken Language Therapist | RR | RRpeak | Qlos | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| First | Last | First | Last | First | Last | First | Last | First | Last | |
| Pp 1 | 232 | 278 | 542 | 490 | 0.18 | 0.26 | 0.24 | 0.29 | −0.03 | −0.02 |
| Pp 2 | 199 | 138.5 | 599 | 450 | 0.17 | 0.19 | 0.23 | 0.24 | −0.07 | −0.03 |
| Pp 3 | 113.5 | 126 | 562.2 | 605.5 | 0.08 | 0.09 | 0.11 | 0.12 | 0.005 | 0.02 |
| Pp 4 | 176 | 174.5 | 854 | 943 | 0.19 | 0.07 | 0.06 | 0.04 | −0.02 | −0.01 |
| Pp 5 | 153 | 34.5 | 509 | 276.5 | 0.2 | 0.08 | 0.16 | 0.04 | −0.04 | 0.04 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Griffioen, R.; van der Steen, S.; Cox, R.F.A.; Verheggen, T.; Enders-Slegers, M.-J. Verbal Interactional Synchronization between Therapist and Children with Autism Spectrum Disorder during Dolphin Assisted Therapy: Five Case Studies. Animals 2019, 9, 716. https://doi.org/10.3390/ani9100716
Griffioen R, van der Steen S, Cox RFA, Verheggen T, Enders-Slegers M-J. Verbal Interactional Synchronization between Therapist and Children with Autism Spectrum Disorder during Dolphin Assisted Therapy: Five Case Studies. Animals. 2019; 9(10):716. https://doi.org/10.3390/ani9100716
Chicago/Turabian StyleGriffioen, Richard, Steffie van der Steen, Ralf F. A. Cox, Theo Verheggen, and Marie-Jose Enders-Slegers. 2019. "Verbal Interactional Synchronization between Therapist and Children with Autism Spectrum Disorder during Dolphin Assisted Therapy: Five Case Studies" Animals 9, no. 10: 716. https://doi.org/10.3390/ani9100716
APA StyleGriffioen, R., van der Steen, S., Cox, R. F. A., Verheggen, T., & Enders-Slegers, M.-J. (2019). Verbal Interactional Synchronization between Therapist and Children with Autism Spectrum Disorder during Dolphin Assisted Therapy: Five Case Studies. Animals, 9(10), 716. https://doi.org/10.3390/ani9100716