
Patient-Specific 3D-Printed Osteotomy Guides and Titanium Plates for Distal Femoral Deformities in Dogs with Lateral Patellar Luxation

 , and
, and
Abstract
Simple Summary
Abstract
1. Introduction
2. Case Description
2.1. Animals and Study Design
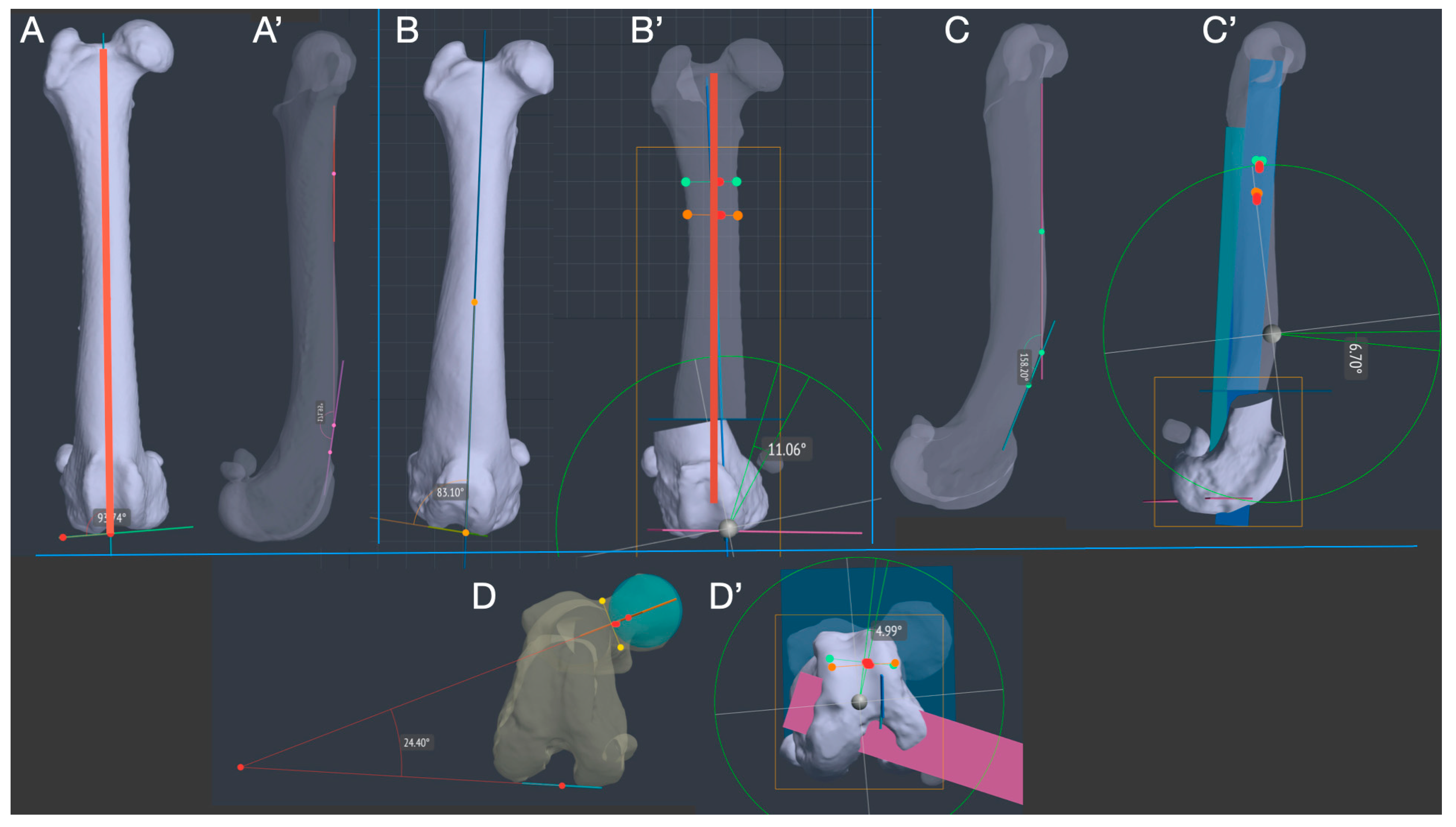
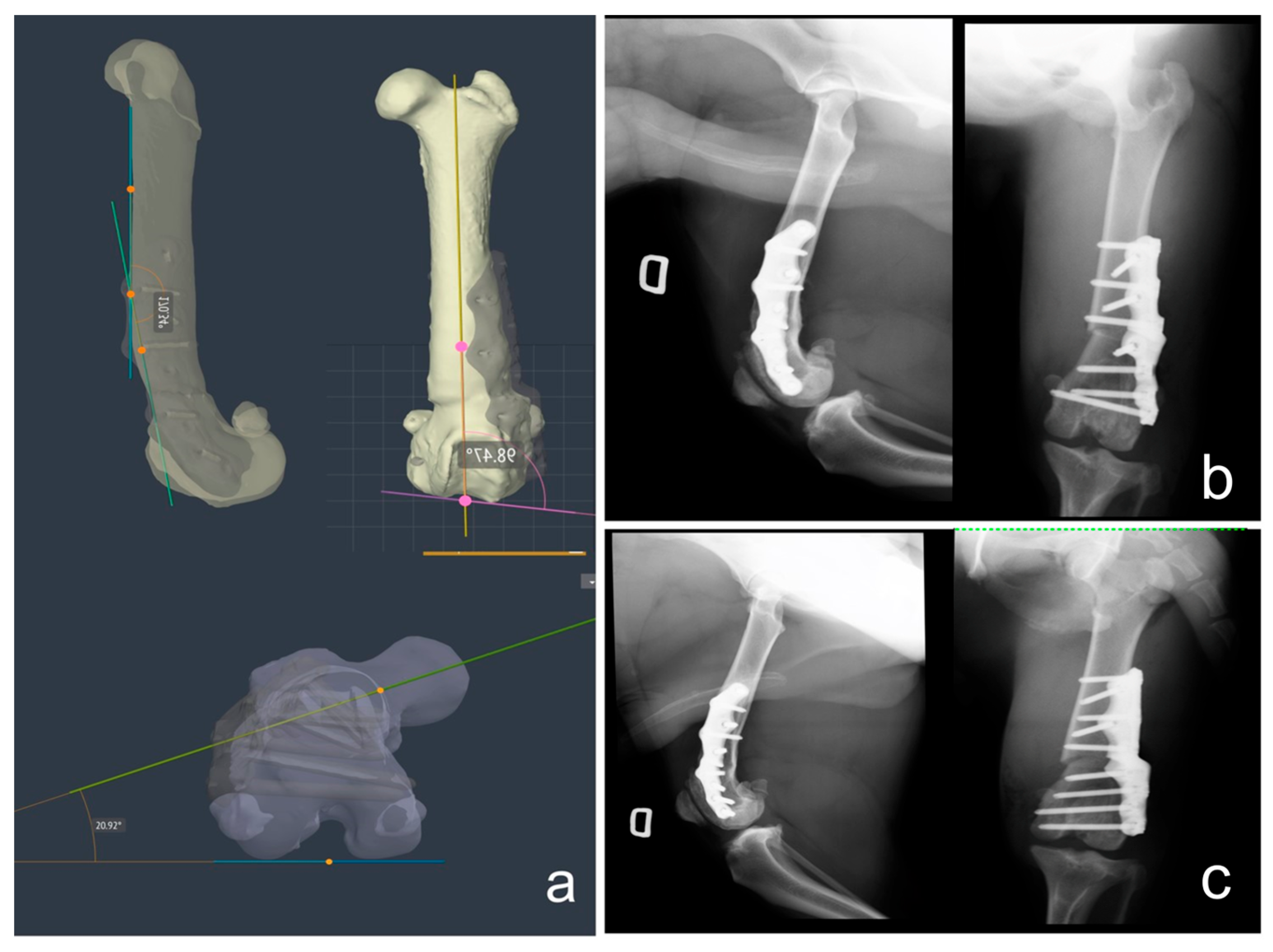
2.2. CT Scan Acquisition and Deformity 3D Measurements
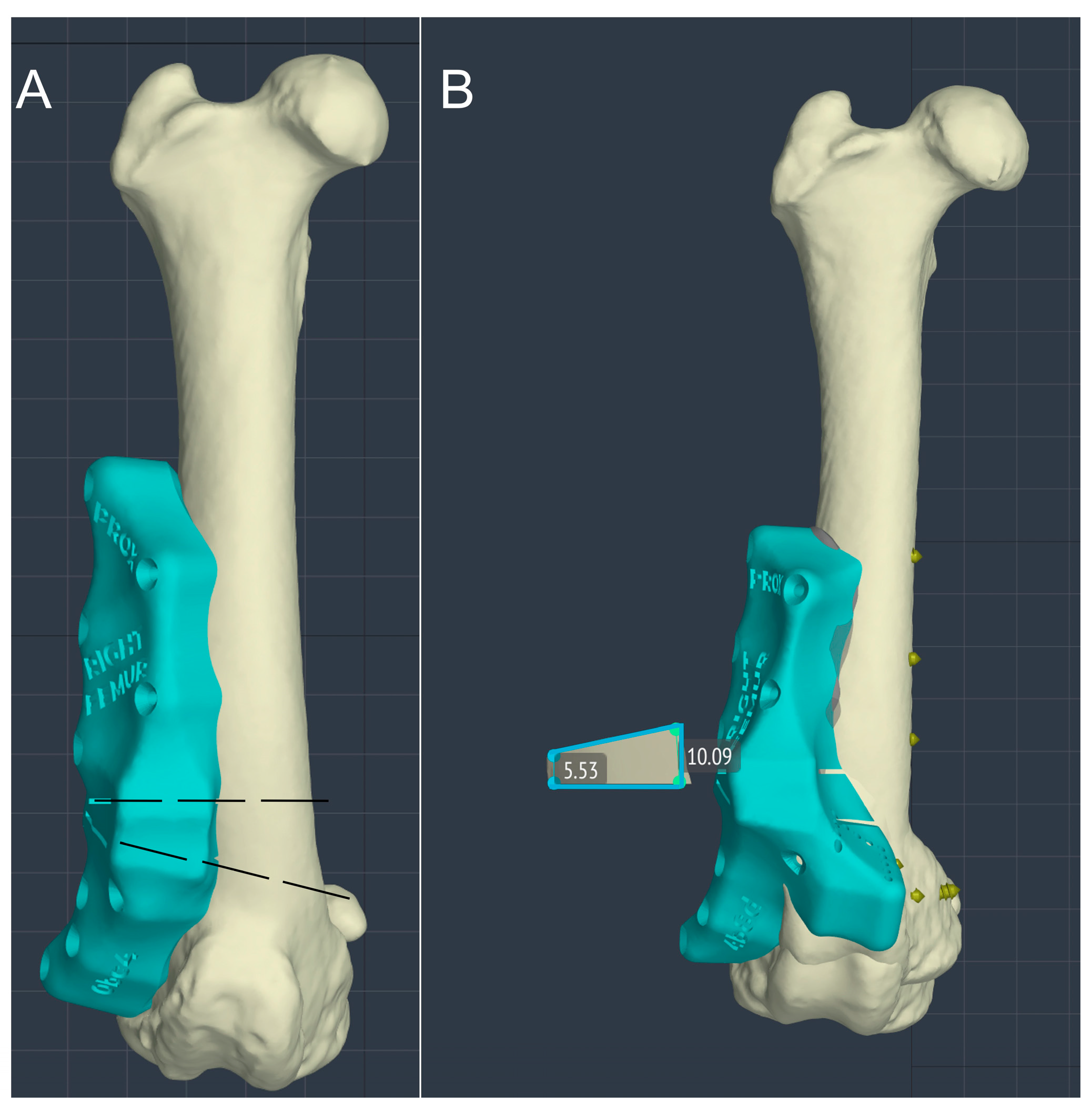
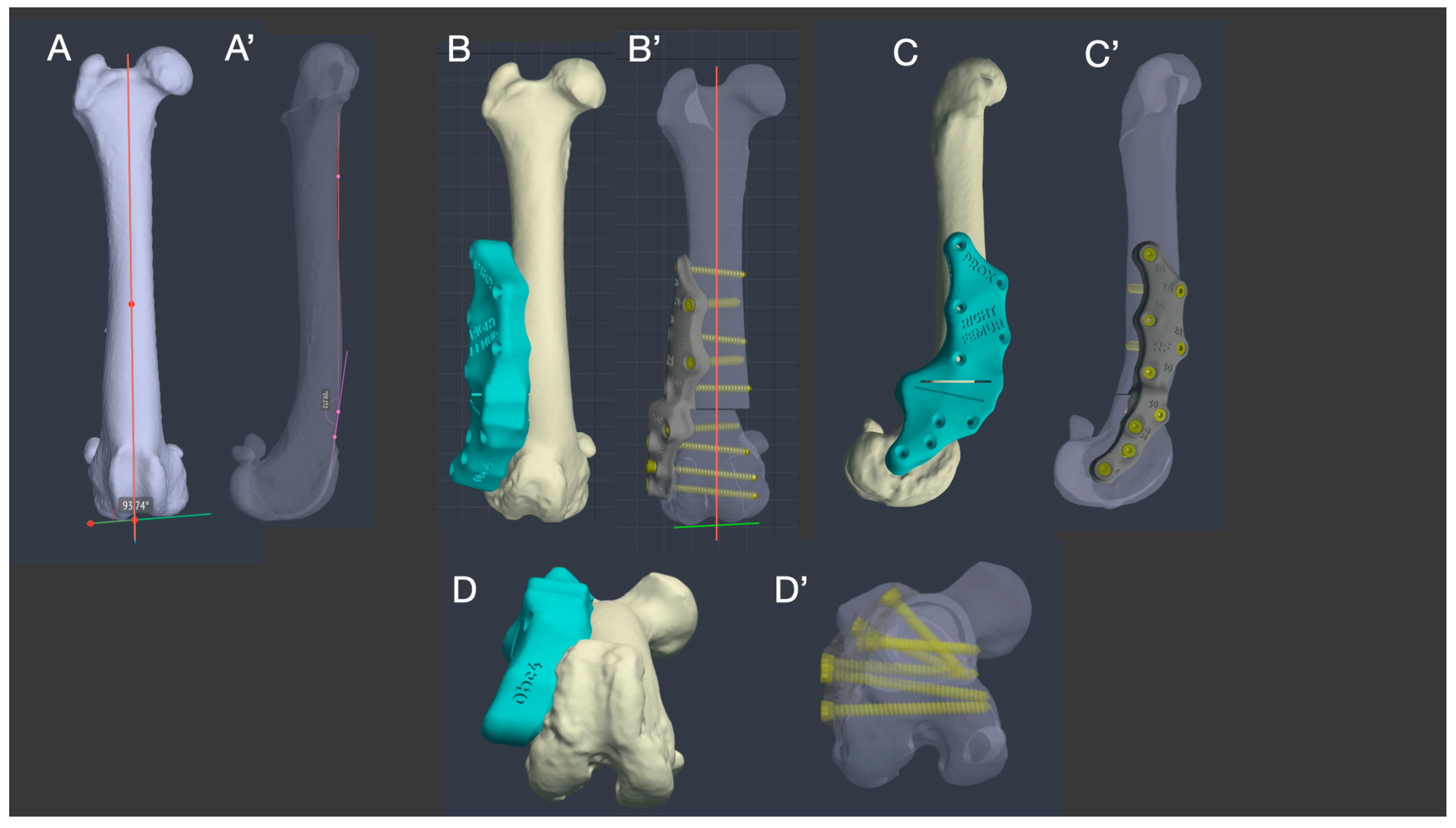
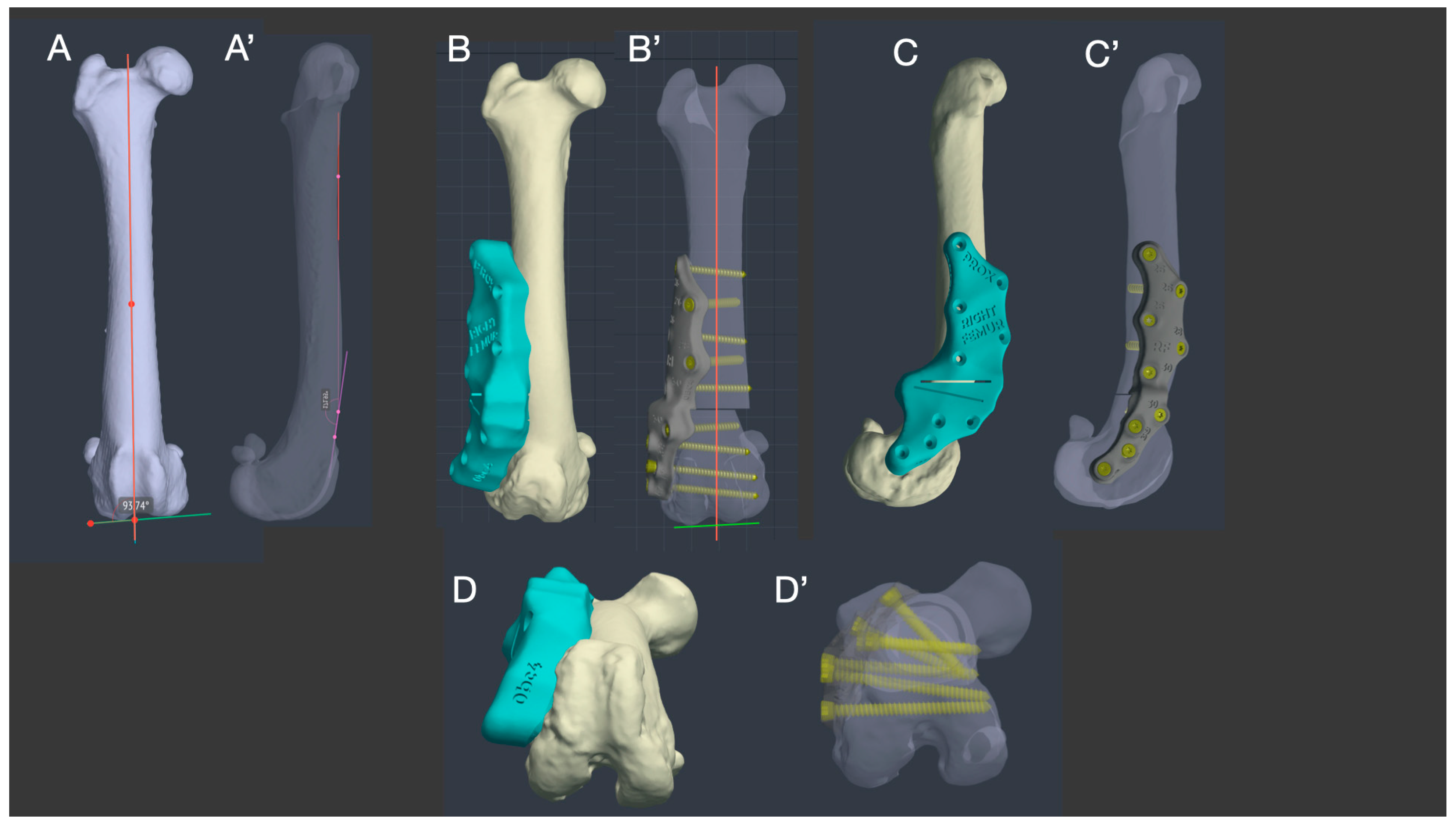
2.3. Virtual Surgery, Patient-Specific Osteotomy Guide and Titanium Plate Design
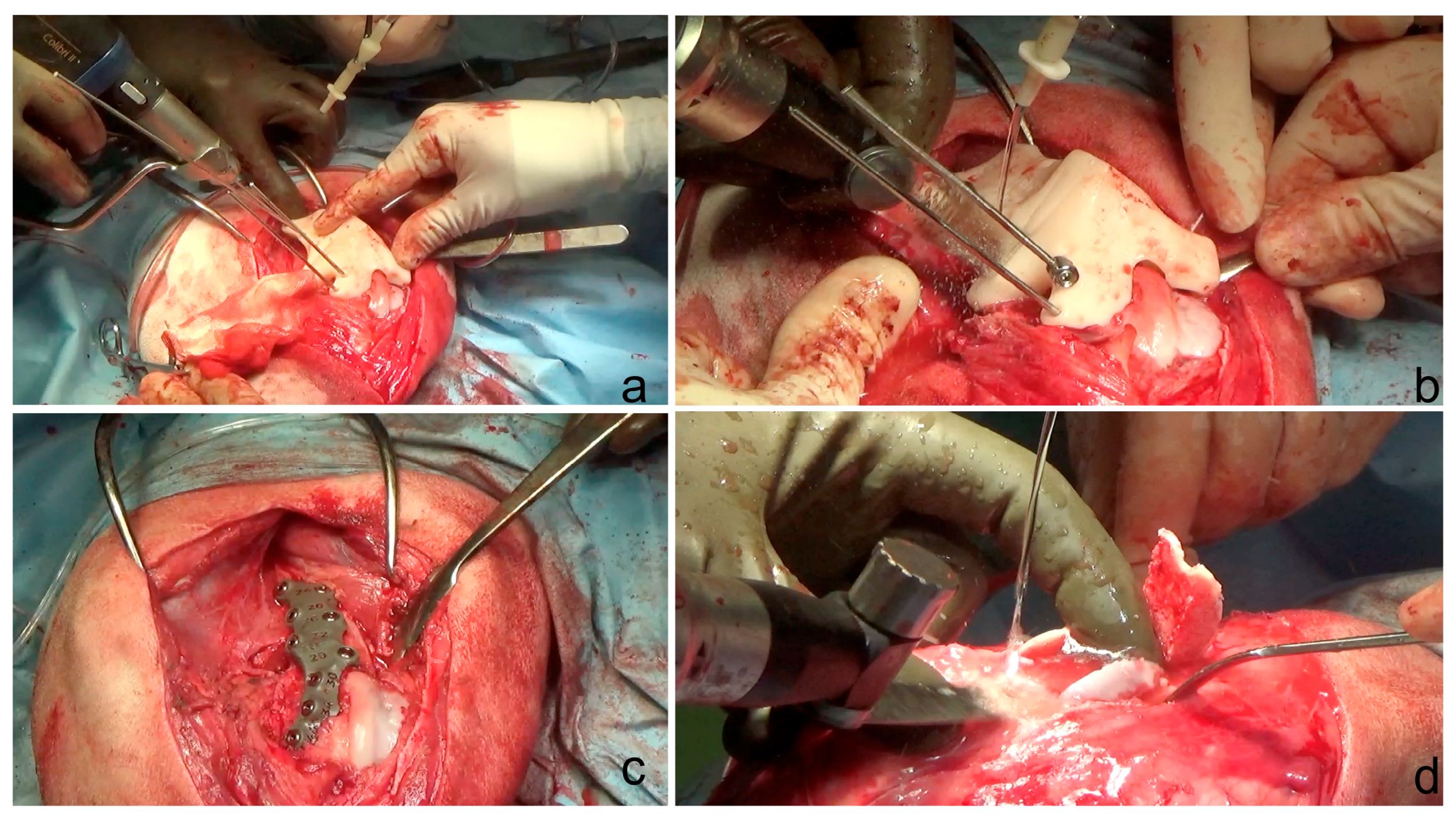
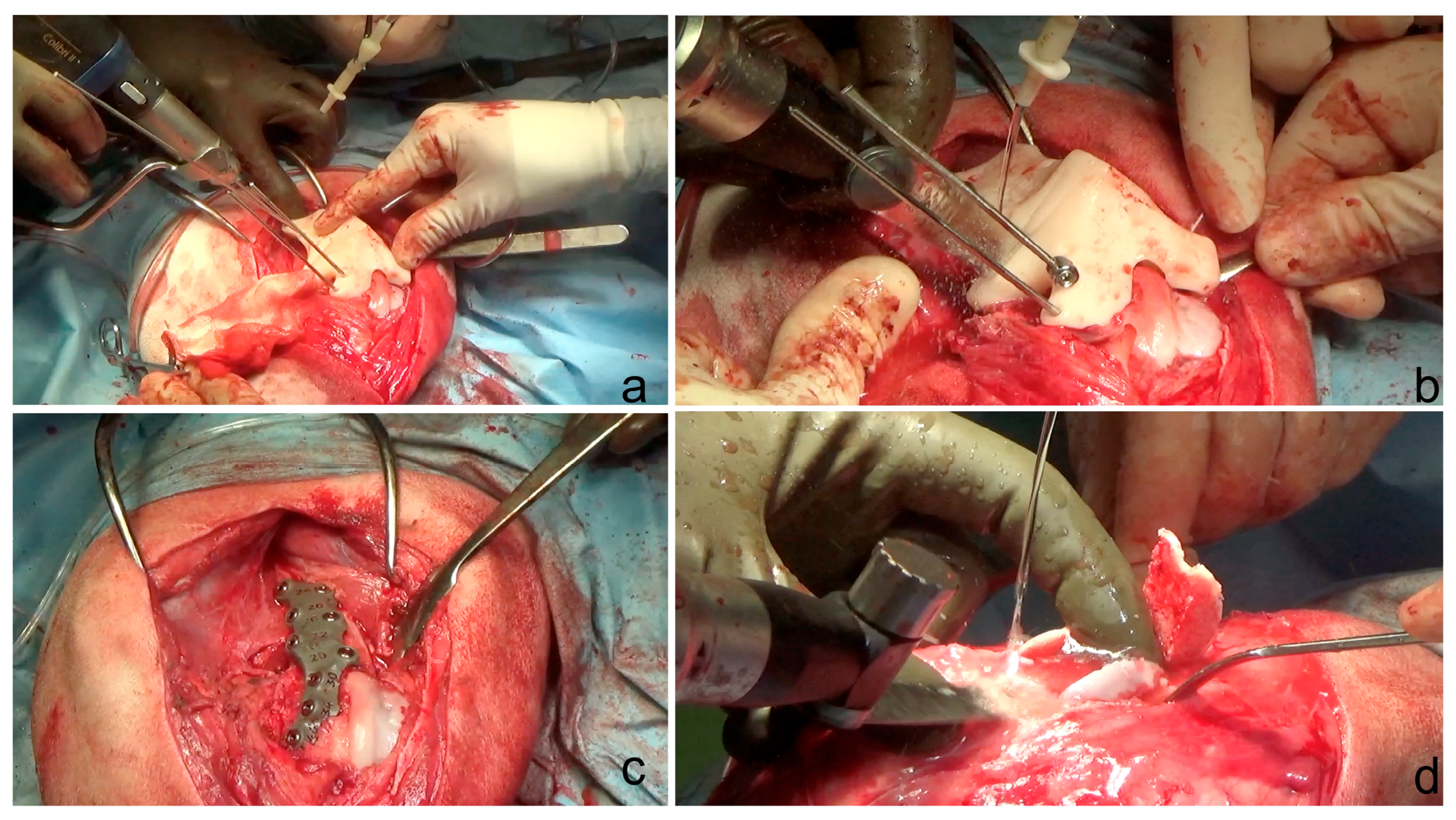
2.4. Surgical Technique
2.5. Postoperative Care
2.6. Postoperative CT Scan, X-rays and Joint Angle Measurements
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Di Dona, F.; Della Valle, G.; Fatone, G. Patellar luxation in dogs. Vet. Med. 2018, 9, 23–32. [Google Scholar] [CrossRef]
- Di Dona, F.; Della Valle, G.; Balestriere, C.; Lamagna, B.; Meomartino, L.; Napoleone, G.; Lamagna, F.; Fatone, G. Lateral patellar luxation in nine small breed dogs. Open Vet. J. 2016, 6, 255–258. [Google Scholar] [CrossRef]
- Kalff, S.; Butterworth, S.J.; Miller, A.; Keeley, B.; Baines, S.; McKee, W.M. Lateral patellar luxation in dogs: A retrospective study of 65 dogs. Vet. Comp. Orthop. Traumatol. 2014, 27, 130–134. [Google Scholar]
- Shaver, S.L.; Mayhew, K.N.; Sutton, J.S.; Mayhew, P.D.; Runge, J.J.; Brown, D.C.; Kass, P.H. Complications after corrective surgery for lateral patellar luxation in dogs: 36 cases (2000–2011). J. Am. Vet. Med. Assoc. 2014, 244, 444–448. [Google Scholar] [CrossRef]
- Gibbons, S.E.; Macias, C.; Tonzing, M.A.; Pinchbeck, G.L.; McKee, W.M. Patellar luxation in 70 large breed dogs. J. Small Anim. Pract. 2006, 47, 3–9. [Google Scholar] [CrossRef]
- Alam, M.R.; Lee, J.I.; Kang, H.S.; Kim, I.S.; Park, S.Y.; Lee, K.C.; Kim, N.S. Frequency and distribution of patellar luxation in dogs. 134 cases (2000 to 2005). Vet. Comp. Orthop. Traumatol. 2007, 20, 59–64. [Google Scholar] [CrossRef]
- LaFond, E.; Breur, G.J.; Austin, C.C. Breed susceptibility for developmental orthopedic diseases in dogs. J. Am. Anim. Hosp. Assoc. 2002, 38, 467–477. [Google Scholar] [CrossRef]
- L’Eplattenier, H.F.; Montavon, P. Patellar luxation in dogs and cats: Management and prevention. Comp. Cont. Edu. Pract. Vet. 2002, 24, 292–300. [Google Scholar]
- Bound, N.; Zakai, D.; Butterworth, S.J.; Pead, M. The prevalence of canine patellar luxation in three centres. Clinical features and radiographic evidence of limb deviation. Vet. Comp. Orthop. Traumatol. 2009, 22, 32–37. [Google Scholar] [PubMed]
- Harasen, G. Patellar luxation: Pathogenesis and surgical correction. Can. Vet. J. 2006, 47, 1037–1039. [Google Scholar] [PubMed]
- DeTora, M.D.; Boudrieau, R.J. Complex angular and torsional deformities (distal femoral malunions). Preoperative planning using stereolithography and surgical correction with locking plate fixation in four dogs. Vet. Comp. Orthop. Traumatol. 2016, 29, 416–425. [Google Scholar] [CrossRef]
- Arthurs, G.I.; Langley-Hobbs, S.J. Complications associated with corrective surgery for patellar luxation in 109 dogs. Vet. Surg. 2006, 35, 559–566. [Google Scholar] [CrossRef]
- Roch, S.P.; Gemmill, T.J. Treatment of medial patellar luxation by femoral closing wedge ostectomy using a distal femoral plate in four dogs. J. Small Anim. Pract. 2008, 49, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Bosio, F.; Bufalari, A.; Peirone, B.; Petazzoni, M.; Vezzoni, A. Prevalence, treatment and outcome of patellar luxation in dogs in Italy. A retrospective multicentric study (2009–2014). Vet. Comp. Orthop. Traumatol. 2017, 30, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Brower, B.E.; Kowaleski, M.P.; Peruski, A.M.; Pozzi, A.; Dyce, J.; Johnson, K.A.; Boudrieau, R.J. Distal femoral lateral closing wedge osteotomy as a component of comprehensive treatment of medial patellar luxation and distal femoral varus in dogs. Vet. Comp. Orthop. Traumatol. 2017, 30, 20–27. [Google Scholar] [CrossRef]
- Panichi, E.; Cappellari, F.; Olimpo, M.; Piras, L.A.; Radasch, R.; Ferretti, A.; Peirone, B. Distal femoral osteotomy using a novel deformity reduction device. Vet. Comp. Orthop. Traumatol. 2016, 29, 426–432. [Google Scholar]
- Swiderski, J.K.; Palmer, R.H. Long-term outcome of distal femoral osteotomy for treatment of combined distal femoral varus and medial patellar luxation: 12 cases (1999–2004). J. Am. Vet. Med. Assoc. 2007, 231, 1070–1075. [Google Scholar] [CrossRef]
- Gigi, R.; Gortzak, Y.; Barriga Moreno, J.; Golden, E.; Gabay, R.; Rumack, N.; Yaniv, M.; Dadia, S.; Segev, E. 3D-printed Cutting Guides for Lower Limb Deformity Correction in the Young Population. J. Pediatr. Orthop. 2022, 42, e427–e434. [Google Scholar] [CrossRef] [PubMed]
- Oraa, J.; Beitia, M.; Fiz, N.; González, S.; Sánchez, X.; Delgado, D.; Sánchez, M. Custom 3D-Printed Cutting Guides for Femoral Osteotomy in Rotational Malalignment Due to Diaphyseal Fractures: Surgical Technique and Case Series. J. Clin. Med. 2021, 10, 3366. [Google Scholar] [CrossRef]
- Fiz, N.; Delgado, D.; Sánchez, X.; Sánchez, P.; Bilbao, A.M.; Oraa, J.; Sánchez, M. Application of 3D Technology and Printing for Femoral Derotation Osteotomy: Case and Technical Report. Ann. Transl. Med. 2017, 5, 400. [Google Scholar] [CrossRef]
- Wong, K.C. 3D-Printed Patient-Specific Applications in Orthopedics. Orthop. Res. Rev. 2016, 8, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Chai, W.; Xu, M.; Zhang, G.; Zhang, L.; Gou, W.; Ni, M.; Chen, J. Computer-Aided Design and Custom-Made Guide in Corrective Osteotomy for Complex Femoral Deformity. J. Huazhong Univ. Sci. Technol. Med. Sci. 2013, 33, 398–405. [Google Scholar] [CrossRef]
- Memarian, P.; Pishavar, E.; Zanotti, F.; Trentini, M.; Camponogara, F.; Soliani, E.; Gargiulo, P.; Isola, M.; Zavan, B. Active Materials for 3D Printing in Small Animals: Current Modalities and Future Directions for Orthopedic Applications. Int. J. Mol. Sci. 2022, 23, 1045. [Google Scholar] [CrossRef]
- Mendaza-DeCal, R.; Peso-Fernandez, S.; Rodriguez-Quiros, J. Orthotics and prosthetics by 3D-printing: Accelerating its fabrication flow. Res. Vet. Sci. 2023, 162, 104960. [Google Scholar] [CrossRef]
- De Armond, C.C.; Lewis, D.D.; Kim, S.E.; Biedrzycki, A.H. Accuracy of virtual surgical planning and custom three-dimensionally printed osteotomy and reduction guides for acute uni- and biapical correction of antebrachial deformities in dogs. J. Am. Vet. Med. Assoc. 2022, 260, 1–9. [Google Scholar] [CrossRef]
- Carvajal, J.L.; Kim, S.E. Proximal femoral deformity correction and total hip arthroplasty in a dog using 3D printed custom guides. Vet. Surg. 2023, 52, 168–175. [Google Scholar] [CrossRef]
- Carwardine, D.R.; Gosling, M.J.; Burton, N.J.; O’Malley, F.L.; Parsons, K.J. Three-dimensional-printed patient-specific osteotomy guides, repositioning guides and titanium plates for acute correction of antebrachial limb deformities in dogs. Vet. Comp. Orthop. Traumatol. 2021, 34, 43–52. [Google Scholar] [CrossRef]
- Hall, E.L.; Baines, S.; Bilmont, A.; Oxley, B. Accuracy of patientspecific three-dimensional-printed osteotomy and reduction guides for distal femoral osteotomy in dogs with medial patella luxation. Vet. Surg. 2019, 48, 584–591. [Google Scholar] [CrossRef]
- Oxley, B. Bilateral shoulder arthrodesis in a Pekinese using three-dimensional printed patient-specific osteotomy and reduction guides. Vet. Comp. Orthop. Traumatol. 2017, 30, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Fracka, A.B.; Oxley, B.; Allen, M.J. 3D-printed, patient-specific cutting guides improve femoral and tibial cut alignment in canine total knee replacement. Vet. Surg. 2023, 52, 674–685. [Google Scholar] [CrossRef]
- Longo, F.; Penelas, A.; Gutbrod, A.; Pozzi, A. Three-dimensional computer-assisted corrective osteotomy with a patient-specific surgical guide for an antebrachial limb deformity in two dogs. Schweiz. Arch. Tierheilkd. 2019, 161, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Longo, F.; Nicetto, T.; Knell, S.C.; Evans, R.B.; Isola, M.; Pozzi, A. Three-dimensional volume rendering planning, surgical treatment, and clinical outcomes for femoral and tibial detorsional osteotomies in dogs. Vet. Surg. 2022, 51, 1126–1141. [Google Scholar] [CrossRef]
- Shi, J.; Lv, W.; Wang, Y.; Ma, B.; Cui, W.; Liu, Z.; Han, K. Three dimensional patient-specific printed cutting guides for closing-wedge distal femoral osteotomy. Int. Orthop. 2019, 43, 619–624. [Google Scholar] [CrossRef]
- Worth, A.J.; Crosse, K.R.; Kersley, A. Computer-Assisted Surgery Using 3D Printed Saw Guides for Acute Correction of Antebrachial Angular Limb Deformities in Dogs. Vet. Comp. Orthop. Traumatol. 2019, 32, 241–249. [Google Scholar] [CrossRef]
- Popov, V.V.; Muller-Kamskii, G.; Katz-Demyanetz, A.; Kovalevsky, A.; Usov, S.; Trofimcow, D.; Dzhenzhera, G.; Koptyug, A. Additive manufacturing to veterinary practice: Recovery of bony defects after the osteosarcoma resection in canines. Biomed. Eng. Lett. 2019, 9, 97–108. [Google Scholar] [CrossRef]
- Easter, T.G.; Bilmont, A.; Pink, J.; Oxley, B. Accuracy of threedimensional printed patient-specific drill guides for treatment of canine humeral intracondylar fissure. Vet. Surg. 2020, 49, 363–372. [Google Scholar] [CrossRef]
- Lam, G.; Kim, S.Y. Three-dimensional computer-assisted surgical planning and use of three-dimensional printing in the repair of a complex articular femoral fracture in a dog. Vet. Comp. Orthop. Traumatol. 2018, 1, e12–e18. [Google Scholar] [CrossRef]
- Oxley, B. A 3-dimensional-printed patient-specific guide system for minimally invasive plate osteosynthesis of a comminuted mid-diaphyseal humeral fracture in a cat. Vet. Surg. 2018, 47, 445–453. [Google Scholar] [CrossRef]
- Toni, C.; Oxley, B.; Behr, S. Atlanto-axial ventral stabilisation using 3D-printed patient-specific drill guides for placement of bicortical screws in dogs. J. Small Anim. Pract. 2020, 61, 609–616. [Google Scholar] [CrossRef]
- Kamishina, H.; Sugawara, T.; Nakata, K.; Nishida, H.; Yada, N.; Fujioka, T.; Nagata, Y.; Doi, A.; Konno, N.; Uchida, F.; et al. Clinical application of 3D printing technology to the surgical treatment of atlantoaxial subluxation in small breed dogs. PLoS ONE 2019, 14, e0216445. [Google Scholar] [CrossRef] [PubMed]
- Toni, C.; Oxley, B.; Clarke, S.; Behr, S. Accuracy of placement of pedicle screws in the lumbosacral region of dogs using 3Dprinted patient-specific drill guides. Vet. Comp. Orthop. Traumatol. 2021, 34, 53–58. [Google Scholar]
- Hamilton-Bennett, S.E.; Oxley, B.; Behr, S. Accuracy of a patient-specific 3D printed drill guide for placement of cervical transpedicular screws. Vet. Surg. 2018, 47, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Dudley, R.M.; Kowaleski, M.P.; Drost, W.T.; Dyce, J. Radiographic and computed tomographic determination of femoral varus and torsion in the dog. Vet. Radiol. Ultrasound 2006, 47, 546–552. [Google Scholar] [CrossRef]
- Paley, D. Principles of Deformity Correction; Paley, D., Herzenberg, J.E., Eds.; Springer: Berlin/Heidelberg, Germany, 2002; pp. 99–154. [Google Scholar]
- Kieves, N.R.; Bergh, M.S.; Zellner, E.; Wang, C. Pilot study measuring the effects of bandaging and cold compression therapy following tibial plateau levelling osteotomy. J. Small Anim. Pract. 2016, 57, 543–547. [Google Scholar] [CrossRef] [PubMed]
- Drygas, K.A.; Mcclure, S.R.; Goring, R.L.; Pozzi, A.; Robertson, S.A.; Wang, C. Effect of cold compression therapy on postoperative pain, swelling, range of motion, and lameness after tibial plateau leveling osteotomy in dogs. J. Am. Vet. Med. Assoc. 2011, 238, 1284–1291. [Google Scholar] [CrossRef] [PubMed]
- Szabo, S.D.; Levine, D.; Marcellin-Little, D.J.; Sidaway, B.K.; Hofmeister, E.; Urtuzuastegui, E. Cryotherapy Improves Limb Use but Delays Normothermia Early After Stifle Joint Surgery in Dogs. Front. Vet. Sci. 2020, 7, 381. [Google Scholar] [CrossRef]
- Fox, D.B.; Tomlinson, J.L.; Cook, J.L.; Breshears, L.M. Principles of uniapical and biapical radial deformity correction using dome osteotomies and the center of rotation of angulation methodology in dogs. Vet. Surg. 2006, 35, 67–77. [Google Scholar] [CrossRef]
- Knapp, J.L.; Tomlinson, J.L.; Fox, D.B. Classification of angular limb deformities affecting the canine radius and ulna using the center of rotation of angulation method. Vet. Surg. 2016, 45, 295–302. [Google Scholar] [CrossRef]
- Meola, S.D.; Wheeler, J.L.; Rist, C.L. Validation of a technique to assess radial torsion in the presence of procurvatum and valgus deformity using computed tomography: A cadaveric study. Vet. Surg. 2008, 37, 525–529. [Google Scholar] [CrossRef]
- Piras, L.A.; Peirone, B.; Fox, D. Effects of antebrachial torsion on the measurement of angulation in the frontal plane: A cadaveric radiographic analysis. Vet. Comp. Orthop. Traumatol. 2012, 25, 89–94. [Google Scholar] [CrossRef]
- Eby, A.; Bleedorn, J. A computed tomographic graphical approach to guide correction of femoral torsion. Vet. Surg. 2020, 49, 1015–1023. [Google Scholar] [CrossRef] [PubMed]
- Oxley, B.; Gemmill, T.J.; Pink, J.; Clarke, S.; Parry, A.; Baines, S.; Malcolm McKee, W. Precision of a novel computed tomographic method for quantification of femoral varus in dogs and an assessment of the effect of femoral malpositioning. Vet. Surg. 2013, 42, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Barnes, D.M.; Anderson, A.A.; Frost, C.; Barnes, J. Repeatability and reproducibility of measurements of femoral and tibial alignment using computed tomography multiplanar reconstructions. Vet. Surg. 2015, 44, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Tomlinson, J.; Fox, D.; Cook, J.L.; Keller, G.G. Measurement of femoral angles in four dog breeds. Vet. Surg. 2007, 36, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Marcellin-Little, D.J.; Levine, D. Principles and application of range of motion and stretching in companion animals. Vet. Clin. N. Am. Small Anim. Pract. 2015, 45, 57–72. [Google Scholar] [CrossRef]
- Baltzer, W.I. Rehabilitation of companion animals following orthopaedic surgery. N. Z. Vet. J. 2020, 68, 157–167. [Google Scholar] [CrossRef]
- Drum, M.G.; Marcellin-Little, D.J.; Davis, M.S. Principles and applications of therapeutic exercises for small animals. Vet. Clin. N. Am. Small Anim. Pract. 2015, 45, 73–90. [Google Scholar] [CrossRef]
- Townsend, A.; Guevar, J.; Oxley, B.; Hetzel, S.; Bleedorn, J. Comparison of three-dimensional printed patient-specific guides versus freehand approach for radial osteotomies in normal dogs: Ex vivo model. Vet. Surg. 2024, 53, 234–242. [Google Scholar] [CrossRef]
- Lee, H.R.; Adam, G.O.; Yang, D.K.; Tungalag, T.; Lee, S.J.; Kim, J.S.; Kang, H.S.; Kim, S.J.; Kim, N.S. An Easy and Economical Way to Produce a Three-Dimensional Bone Phantom in a Dog with Antebrachial Deformities. Animals 2020, 10, 1445. [Google Scholar] [CrossRef] [PubMed]
- Olimpo, M.; Piras, L.A.; Peirone, B.; Fox, D.B. Comparison of osteotomy technique and jig type in completion of distal femoral osteotomies for correction of medial patellar luxation: An in vitro study. Vet. Comp. Orthop. Traumatol. 2017, 30, 28–36. [Google Scholar] [PubMed]
- Hespel, A.M.; Wilhite, R.; Hudson, J. Invited review—Applications for 3D printers in veterinary medicine. Vet. Radiol. Ultrasound 2014, 55, 347–358. [Google Scholar] [CrossRef] [PubMed]
- Mulford, J.S.; Babazadeh, S.; Mackay, N. Three-dimensional printing in orthopaedic surgery: Review of current and future applications. ANZ J. Surg. 2016, 86, 648–653. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dog | Side | aLDFA(°) | Proc. | FTA | Imaging Modality | Concurrent Deformity | Other Procedures | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre Op | Virtual Op | Post Op | Pre Op | Virtual Op | Post Op | Pre Op | Virtual Op | Post Op | |||||
| 1 | R | 83° | 94° | 98° | 158° | 170° | 170° | 25° | 20° | 20° | CT | Mild Metatarsal rotation | CWO; TBR; LD; MER. |
| 1 | L | 82° | 94° | 98° | 156° | 170° | 169° | 29° | 20° | 20° | CT | Mild Metatarsal rotation | CWO; TBR; LD; MER. |
| 2 | R | 82° | 94° | 95° | 163° | 170° | 172° | 29° | 20° | 20° | CT | Mild Metatarsal rotation | CWO; TBR; LD; MER. |
| PROM | TIE Circumference | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Dog | Side | Pre Operative | FWUP 6 m | FWUP 18 m | FWUP 24 m | FWUP 36 m | Pre Operative | FWUP 6 m | FWUP 18 m | FWUP 24 m | FWUP 36 m |
| 1 | R | 1 = 130 2 = 35° | 1 = 140 2 = 90° | 1 = 150 2 = 80° | 1 = 138 2 = 80° | 1 = 138 2 = 80° | 28 cm | 38 cm | 42 cm | 42 cm | 42 cm |
| 1 | L | 1 = 125 2 = 35° | 1 = 140 2 = 80° | 1 = 138 2 = 80° | 1 = 138 2 = 80° | 1 = 140 2 = 80° | 28 cm | 39 cm | 32 cm | 39 cm | 40 cm |
| 2 | R | 1 = 130 2 = 35° | 1 = 155 2 = 70° | 1 = 155 2 = 60° | 1 = 155 2 = 60° | 1 = 155 2 = 60° | 30 cm | 37 cm | 42 cm | 42 cm | 42 cm |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Panichi, E.; Cappellari, F.; Burkhan, E.; Principato, G.; Currenti, M.; Tabbì, M.; Macrì, F. Patient-Specific 3D-Printed Osteotomy Guides and Titanium Plates for Distal Femoral Deformities in Dogs with Lateral Patellar Luxation. Animals 2024, 14, 951. https://doi.org/10.3390/ani14060951
Panichi E, Cappellari F, Burkhan E, Principato G, Currenti M, Tabbì M, Macrì F. Patient-Specific 3D-Printed Osteotomy Guides and Titanium Plates for Distal Femoral Deformities in Dogs with Lateral Patellar Luxation. Animals. 2024; 14(6):951. https://doi.org/10.3390/ani14060951
Chicago/Turabian StylePanichi, Enrico, Fulvio Cappellari, Ekaterina Burkhan, Gaetano Principato, Marco Currenti, Marco Tabbì, and Francesco Macrì. 2024. "Patient-Specific 3D-Printed Osteotomy Guides and Titanium Plates for Distal Femoral Deformities in Dogs with Lateral Patellar Luxation" Animals 14, no. 6: 951. https://doi.org/10.3390/ani14060951
APA StylePanichi, E., Cappellari, F., Burkhan, E., Principato, G., Currenti, M., Tabbì, M., & Macrì, F. (2024). Patient-Specific 3D-Printed Osteotomy Guides and Titanium Plates for Distal Femoral Deformities in Dogs with Lateral Patellar Luxation. Animals, 14(6), 951. https://doi.org/10.3390/ani14060951