
The Role of Early Rehabilitation and Functional Electrical Stimulation in Rehabilitation for Cats with Partial Traumatic Brachial Plexus Injury: A Pilot Study on Domestic Cats in Portugal

 , ,
, ,  ,
,  , ,
, ,  ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Participants
2.2. Study Design
2.3. Procedures
2.3.1. Intensive Neurorehabilitation Protocol (INRP)
1st–3rd Week of INRP

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Rehabilitation Modality/Exercise | Parameters | Implementation |
|---|---|---|
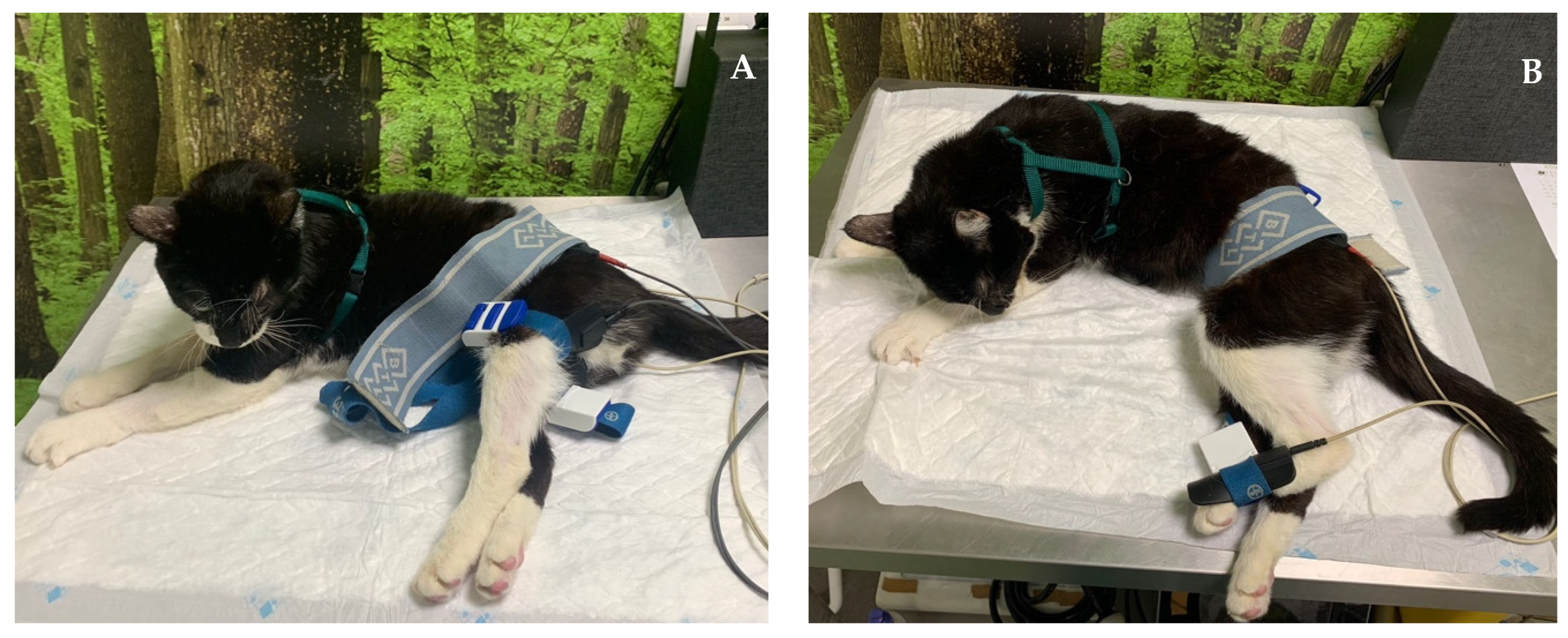
| Laser therapy (A) | 18–22 J/cm2 Class IV laser Radial nerve pathway; SID | Regenerative |
| 5–10 J/cm2 Class IV laser 4-point joint technique; SID (Shoulder, Elbow, Carpus) | Analgesia, Anti-inflammatory effects | |
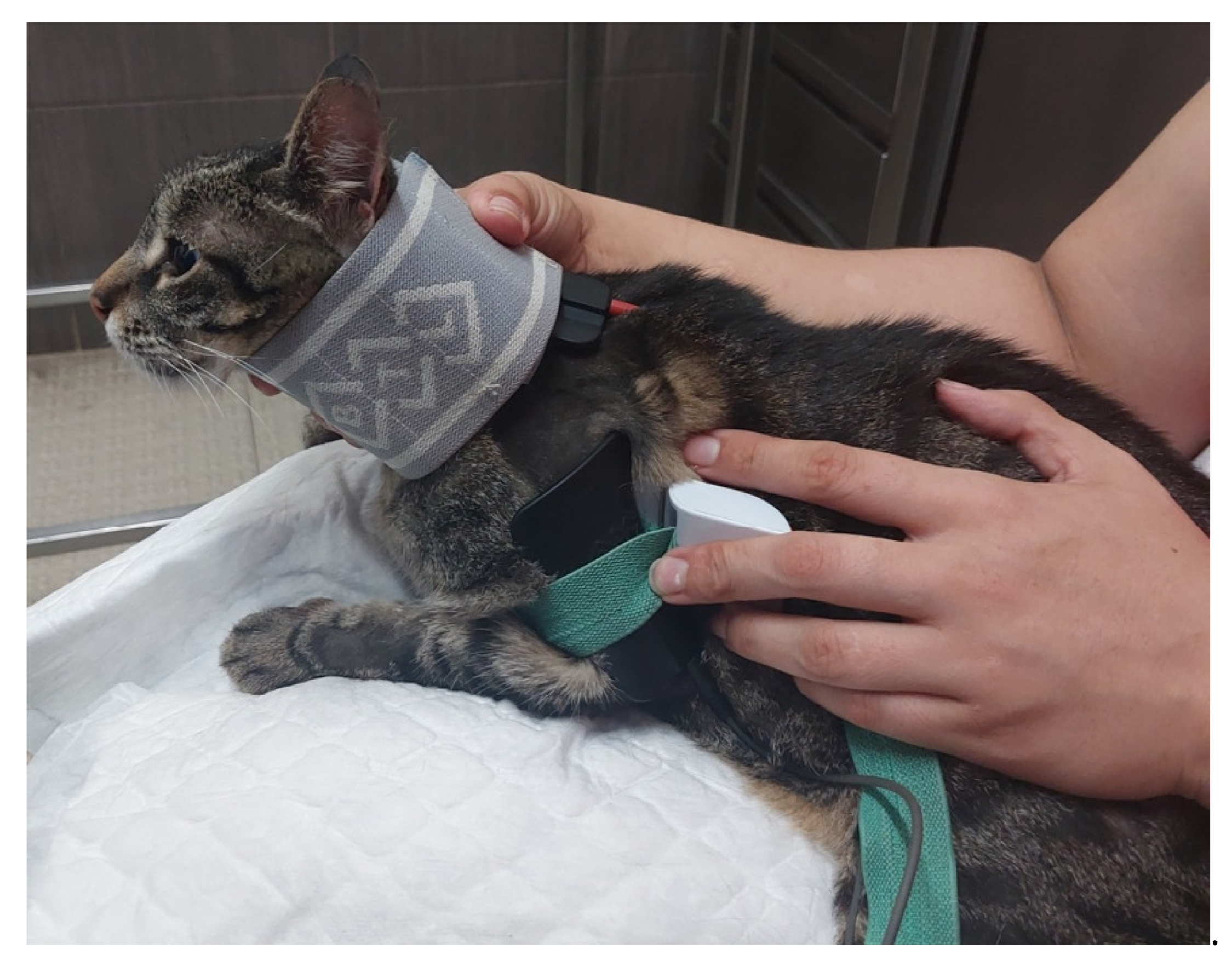
| FES of the radial nerve (B) | 30–40 Hz; 6–16 mA; 200 µs [49] Trapezoidal modulation 1:4 duty cycle 2–4 s ramp up; 8 s plateau; 1–2 s ramp down; 10 min; TID | Deep pain |
| 30–40 Hz; 6–24 mA; 200 µs [49] Trapezoidal modulation 1:4 or 1:5 duty cycle 2–4 s ramp up; 8 s plateau; 1–2 s ramp down; 10 min; TID | No deep pain | |
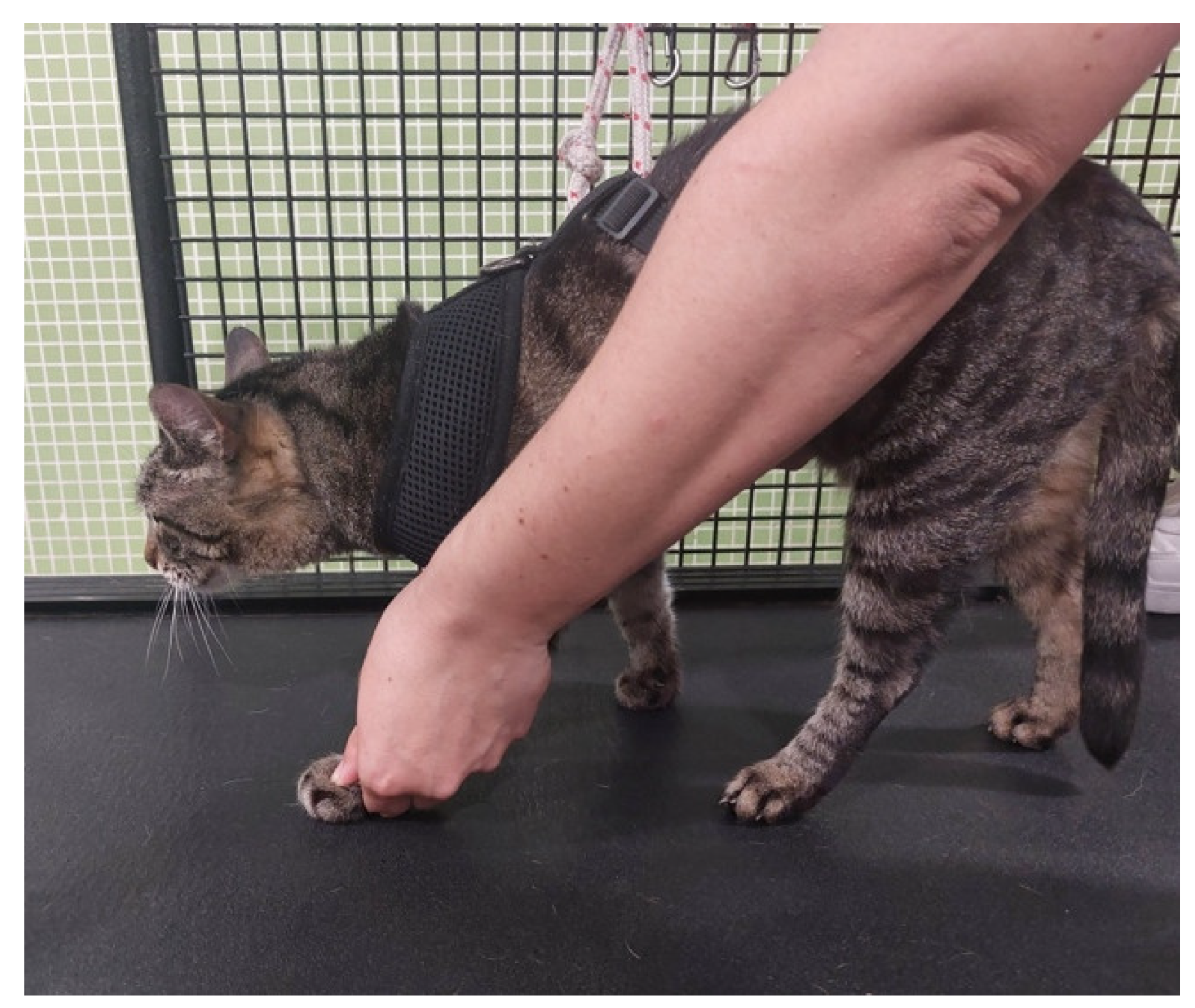
| Range-of-motion exercises (C) | 10–30 sets 4–6 times/day | All joints: shoulder, elbow, carpal and digits |
| Postural standing position (D) | 2–3 min 4–6 times/day | |
| Ultrasound (E) | 1 MHz; 1.5 w/cm2; 10 min Pulsed mode; Duty cycle of 20%; Pulse ratio 1:4; 5 cm transducer head | Muscles: triceps brachialis; biceps brachialis; extensor carpi radialis; lateral and common digital extensor |
4th–6th Week of INRP
6th–8th Week of INRP
Neuropathic Pain
2.4. Data Collection
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Uemura, E.E. Motor system. In Fundamentals of Canine Neuroanatomy and Neurophysiology; Uemura, E.E., Ed.; John Wiley & Sons: Ames, IA, USA, 2015; pp. 257–288. [Google Scholar]
- Troupel, T.; Caenegem, N.V.; Jeandel, A.; Thibaud, J.; Nicolle, A.; Blot, S. Epidemiological, clinical, and electrophysiological findings in dogs and cats with traumatic brachial plexus injury: A retrospectove study of 226 cases. J. Vet. Intern. Med. 2021, 35, 2837–2845. [Google Scholar] [CrossRef] [PubMed]
- De Lahunta, A.; Glass, E.; Kent, M. Lower motor neuron: Spinal nerve, general somatic efferent system. In Veterinary Neuroanatomy and Clinical Neurology, 4th ed.; de Lahunta, A., Glass, E., Klent, M., Eds.; Elsevier: St. Louis, MO, USA, 2014; pp. 102–161. [Google Scholar]
- Wheeler, S.J.; Jones, D.G.; Wright, J.A. The diagnosis of brachial plexus disoreders in dogs: A review of twenty-two cases. J. Small Anim. Pract. 1986, 27, 147–157. [Google Scholar] [CrossRef]
- Soens, I.V.; Struys, M.M.; Polis, I.E.; Bhatti, S.F.; Meervenne, S.A.; Martlé, V.A.; Nollet, H.; Tshamala, M.; Vanhaesebrouck, A.E.; Ham, L.M. Magnetic stimulation of the radial nerve in dogs and cats with brachial plexus trauma: A report of 53 cases. Vet. J. 2009, 182, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, I.R.; Duncan, I.D.; Lawson, D.D. Avulsion of the brachial plexus-2. Clinical aspects. J. Small Anim. Pract. 1974, 15, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, H.S. Brachial plexus injuries and dysfunctions. Vet. Clin. N. Am. Small Anim. Pract. 1988, 18, 565–580. [Google Scholar] [CrossRef] [PubMed]
- Wood, M.D.; Kemp, S.W.; Weber, C.; Borschel, G.H.; Gordon, T. Outcome measures of peripheral nerve regeneration. Ann. Anat. 2011, 193, 321–333. [Google Scholar] [CrossRef] [PubMed]
- Anson, A.; Gil, F.; Laredo, F.G.; Soler, M.; Belda, E.; Ayala, M.D.; Agut, A. Correlative ultrasound anatomy of the feline brachial plexus and major nerves of the thoracic limb. Vet. Radiol. Ultrasound 2013, 54, 185–193. [Google Scholar] [CrossRef]
- Grinsell, D.; Keating, C.P. Peripheral nerve reconstruction after injury: A review of clinical and experimental therapies. Biomed Res. Int. 2014, 2014, 698256. [Google Scholar] [CrossRef]
- Effron, C.R.; Beasley, R.W. Compression neuropathies in the upper limb and electrophysiological studies. In Grabb and Smith’s Plastic Surgery; Thorne, C.H., Bartlett, S.P., Beasley, R.W., Aston, S.J., Gurtner, G.C., Spear, S.L., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006; p. 86. [Google Scholar]
- Robinson, L.R. Traumatic injury to peripheral nerves. Muscle Nerve 2000, 23, 863–887. [Google Scholar] [CrossRef]
- Seddon, H.J. Three types of nerve injury. Brain 1943, 66, 237. [Google Scholar] [CrossRef]
- Menorca, R.M.; Fussell, T.S.; Elfar, J.C. Peripheral nerve trauma: Mechanisms of injury and recovery. Hand Clin. 2013, 29, 317–330. [Google Scholar] [CrossRef] [PubMed]
- Hussain, G.; Wang, J.; Rasul, A.; Anwar, H.; Qasim, M.; Zafar, S.; Aziz, N.; Razzaq, A.; Hussain, R.; Aguilar, J.; et al. Current status of therapeutic approaches against peripheral nerve injuries: A detailed story from injury to recovery. Int. J. Biol. Sci. 2020, 16, 116–134. [Google Scholar] [CrossRef] [PubMed]
- Houschyar, K.S.; Momeni, A.; Pyles, M.N.; Cha, J.Y.; Maan, Z.N.; Duscher, D.; Jew, O.S.; Siemers, F.; Schoonhoven, J. The role of current techniques and concepts in peripheral nerve repair. Plastic Surg. Int. 2016, 2016, 4175293. [Google Scholar] [CrossRef] [PubMed]
- Modrak, M.; Talukder, M.A.; Gurgenashvili, K.; Noble, M.; Elfar, J.C. Peripheral nerve injury and myelination: Potential therapeutic strategies. J. Neurosci. Res. 2020, 98, 780–795. [Google Scholar] [CrossRef] [PubMed]
- Pfister, B.J.; Gordon, T.; Loverde, J.R.; Kochar, A.S.; Mackinnon, S.E.; Cullen, D.K. Biomedical engineering strategies for peripheral nerve repair: Surgical application, atate of the art, and future challenges. Crit. Rev. Biomed. Eng. 2011, 39, 81–124. [Google Scholar] [CrossRef] [PubMed]
- De Lahunta, A. Feline neurology. Vet. Clin. N. Am. 1976, 6, 433–451. [Google Scholar] [CrossRef] [PubMed]
- Dessal, F. Fundamentos de Neuroanatomia. In Neurologia Felina; Dessal, F., Ed.; Editorial Inter-Médica: Buenos Aires, Argentina, 2020. [Google Scholar]
- Drum, M.G.; Bockstahler, B.; Levine, D.; Marcellin-Little, D.J. Feline rehabilitation. Vet. Clin. N. Am. Small Anim. Pract. 2015, 45, 185–201. [Google Scholar] [CrossRef]
- Willand, M.P. Electrical stimulation enhances reinnervation after nerve injury. Eur. J. Trans. Myol. 2015, 25, 243–248. [Google Scholar] [CrossRef]
- Kao, C.; Chen, J.; Hsu, Y.; Bau, D.; Yao, C.; Chen, Y. High-Frequency electrical stimulation can be a complementary therapy to promote nerve regeneration in diabetic rats. PLoS ONE 2013, 8, e79078. [Google Scholar] [CrossRef]
- Foecking, E.M.; Fargo, K.N.; Coughlin, L.M.; Kim, J.T.; Marzo, S.J.; Jones, K.J. Single session if brief electrical stimulation immeadiately following crush injury enhances functional recovery of rat facial nerve. J. Rehabil. Res. Dev. 2012, 49, 451–458. [Google Scholar] [CrossRef]
- Gigo-Benato, D.; Russo, T.L.; Geuna, S.; Domingues, N.; Salvini, T.F.; Parizotto, N.A. Electrical stimulation impairs early functional recovery and accentuates skeletal muscle atrophy after sciatic nerve crush injury in rats. Muscle Nerve 2010, 41, 685–693. [Google Scholar] [CrossRef] [PubMed]
- Brushart, T.M.; Hoffman, P.N.; Royall, R.M.; Murinson, B.B.; Witzel, C.; Gordon, T. Electrical stimulation promotes motoneuron regeneration without increasing its speed or conditioning the neuron. J. Neurosci. 2002, 22, 6631–6638. [Google Scholar] [CrossRef] [PubMed]
- Brushart, T.M.; Jari, R.; Verge, V.; Rohde., C.; Gordon, T. Electrical stimulation restores the specificity of sensory axon regeneration. Exp. Neurol. 2005, 194, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Evans, G.R. Peripheral nerve injury: A review and approach to tissue engineered constructs. Anat. Rec. 2001, 263, 396–404. [Google Scholar] [CrossRef]
- Marqueste, T.; Alliez, J.R.; Alluin, O.; Jammes, Y.; Decherchi, P. Neuromuscular rehabilitation by treadmill running or electrical stimulation af- ter peripheral nerve injury and repair. J. Appl. Physiol. 2004, 96, 1988–1995. [Google Scholar] [CrossRef] [PubMed]
- Russo, T.L.; Peviani, S.M.; Durigan, J.L.; Salvini, T.F. Electrical stimulation increases matrix metalloproteinase-2 gene expression but does not change its activity in denervated rat muscle. Muscle Nerve 2008, 37, 593–600. [Google Scholar] [CrossRef]
- Varejão, A.S.; Cabrita, A.M.; Meek, M.F.; Bulas-Cruz, J.; Melo-Pinto, P.; Raimondo, S.; Geuna, S.; Giacobini-Robecchi, M.G. Functional and morphological assessment of a standardized rat sciatic nerve crush injury with a non-serrated clamp. J. Neurotrauma 2004, 21, 1652–1670. [Google Scholar] [CrossRef]
- Baptista, A.F.; Gomes, J.R.; Oliveira, J.T.; Santos, S.M.; Vannier-Santos, M.A.; Martinez, A.M. High- and low-frequency transcutaneous electrical nerve stimulation delay sciatic nerve regeneration after crush lesion in the mouse. J. Peripher. Nerv. Syst. 2008, 13, 71–80. [Google Scholar] [CrossRef]
- Kerns, J.M.; Lucchinetti, C. Electrical field effects on crushed nerve regeneration. Exp. Neurol. 1992, 117, 71–80. [Google Scholar] [CrossRef]
- Lundborg, G. Enhancing posttraumatic nerve regeneration. J. Peripher. Nerv. Syst. 2002, 7, 139–140. [Google Scholar] [CrossRef]
- Samii, M.; Carvalho, G.A.; Nikkhah, G.; Penkert, G. Surgical reconstruction of the musculocutaneous nerve in traumatic brachial plexus injuries. J. Neurosurg. 1997, 87, 881–886. [Google Scholar] [CrossRef]
- Mendonça, A.C.; Barbieri, C.H.; Mazzer, N. Directly applied low intensity direct electric current enhances peripheral nerve regeneration in rats. J. Neurosci. Methods 2003, 129, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Dow, D.E.; Cederna, P.S.; Hassett, C.A.; Kostrominova, T.Y.; Faulkner, J.A.; Dennis, R.G. Number of contractions to maintain mass and force of a denervated rat muscle. Muscle Nerve 2004, 30, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Denny, H.R.; Butterworth, S.J. Peripheral nerve injury. In A Guide to Canine and Feline Orthopaedic Surgery; Denny, H.R., Butterworth, S.J., Eds.; Blackwell Science Lds.: Oxford, UK, 2000; pp. 201–205. [Google Scholar]
- Añor, S. Monoparesis. In BSAVA Manual of Canine and Feline Neurology; Platt, S., Olby, N., Eds.; Brithish Small Animal Veterinary Association: Cheltenahm, UK, 2013; pp. 328–341. [Google Scholar]
- Levine, D.; Millis, D.L.; Marcellin-Little, D.J.; Taylor, R. (Eds.) Therapeutic exercise and manual therapy. In Reabilitaçāo e Fisioterapia na Prática de Pequenos Animais; Roca: São Paulo, Brasil, 2008; pp. 447–463. [Google Scholar]
- Levine, D.; Millis, D.L.; Marcellin-Little, D.J.; Taylor, R. (Eds.) Physical therapy for specific diagnoses. In Reabilitação e Fisioterapia na Prática de Pequenos Animais; Roca: São Paulo, Brasil, 2008; pp. 609–627. [Google Scholar]
- Shores, A.; Pearce, L. Traumatic and Neoplastic Diseases of the Brachial Plexus. In Mechanisms of Disease in Small Animal Surgery; Bojrab, M.J., Monnet, E., Eds.; Teton New Media Inc.: Jackson, WY, USA, 2010. [Google Scholar]
- Marcellin-Little, D.J.; Levine, D. Principles and application of range of motion and stretching in companion animals. Vet. Clin. N. Am. Small Anim. Pract. 2015, 45, 57–72. [Google Scholar] [CrossRef] [PubMed]
- Knecht, C.D.; Raffe, M.R. Diseases of the Brachial Plexus. In Textbook of Small Animal Orthopaedics; Newton, C.D., Nunamaker, D.M., Eds.; Lippincott: Philadelphia, PA, USA, 1985. [Google Scholar]
- Marcolino, A.M.; Barbosa, R.I.; Fonseca, M.C.; Mazzer, N.; Ellui, V.M. Reabilitação fisioterapêutica na lesaõ do plexo braquial: Relato de caso. Fisioter. Mov. 2008, 21, 53–60. [Google Scholar]
- Monte-Raso, V.V.; Barbieri, C.H.; Mazzer, N.; Fazan, V.P. Os efeitos do ultra- som terapêutico nas lesões por esmagamento do nervo ciático de ratos: Análise funcional da marcha. Rev. Bras. Fisioter. 2006, 10, 113–119. [Google Scholar] [CrossRef]
- Millis, D.L.; Levine, D. Basic science of veterinary rheabilitation. In Canine Rehabilitation and Physical Therapy; Millis, D.L., Levine, D., Eds.; W. B. Saunders Co., Ltd.: Philadelphia, PA, USA, 2014; pp. 79–153. [Google Scholar]
- Bocksthler, B.; Wittek, K. Passive Range of Motion Exercises and Stretching. In Essential Facts of Physical Medicine, Rehabilitation and Sports Medicine in Companion Animals; Bocksthler, B., Wittek, K., Eds.; VBS GmbH: Munich, Germany, 2019; p. 110. [Google Scholar]
- Sawaya, S.G.; Combet, D.; Chanoit, G.; Thiebault, J.J.; Levine, D.; Marcellin-Little, D.J. Assessment of impulse duration thresholds for electrical stimulation of muscles (chronaxy) in dogs. Am. J. Vet. Res. 2008, 69, 1305–1309. [Google Scholar] [CrossRef]
- Gouveia, D.; Fonseca, S.; Carvalho, C.; Cardoso, A.; Almeida, A.; Gamboa, Ó.; Canejo-Teixeira, R.; Ferreira, A.; Martins, Â. Clinical occurrences in the neurorehabilitation of dogs with severe spinal cord injury. Animals 2023, 13, 1164. [Google Scholar] [CrossRef]
- Martins, Â.; Gouveia, D.; Cardoso, A.; Viegas, I.; Gamboa, Ó.; Ferreira, A. A comparison between body weight-supported treadmill training and conventional over-ground training in dogs with incomplete spinal cord injury. Front. Vet. Sci. 2021, 8, 597949. [Google Scholar] [CrossRef]
- Martins, Â.; Gouveia, D.; Cardoso, A.; Carvalho, C.; Silva, C.; Coelho, T.; Gamboa, Ó.; Ferreira, A. Functional neurorehabilitation in dogs with an incomplete recovery 3 months following intervertebral disc surgery: A case series. Animals 2021, 11, 2442. [Google Scholar] [CrossRef]
- Lewis, M.J.; Jeffery, N.D.; Olby, N.J. Ambulation in dogs with absent pain perception after acute thoracolumbar Spinal Cord Injury. Front. Vet. Sci. 2020, 7, 560–572. [Google Scholar] [CrossRef] [PubMed]
- Menchetti, M.; Gandini, G.; Bravaccini, B.; Dondi, M.; Gagliardo, T.; Bianchi, E. Clinical and electrodiagnostic findings and quality of life of dogs and cats with brachial plexus injury. Vet. Sci. 2020, 7, 101. [Google Scholar] [CrossRef] [PubMed]
- Mackinnon, S.; Dellon, A.L. Surgery of the peripheral nerve. In Diagnosis of Nerve Injury; Thieme: New York, NY, USA, 1988; pp. 74–78. [Google Scholar]
- Alvites, R.; Rita Caseiro, A.; Santos Pedrosa, S.; Vieira Branquinho, M.; Ronchi, G.; Geuna, S.; Varejão, A.S.P.; Colette Maurício, A.; Spurkland, A. Peripheral nerve injury and axonotmesis: State of the art and recent advances. Cogent. Med. 2018, 5, 1466404. [Google Scholar] [CrossRef]
- Lopes, B.; Sousa, P.; Alvites, R.; Branquinho, M.; Sousa, A.C.; Mendonça, C.; Atayde, L.M.; Luís, A.L.; Varejão, A.S.P.; Maurício, A.C. Peripheral Nerve Injury Treatments and Advances: One Health Perspective. Int. J. Mol. Sci. 2022, 23, 918. [Google Scholar] [CrossRef] [PubMed]
- Vijayavenkataraman, S. Nerve guide conduits for peripheral nerve injury repair: A review on design, materials and fabrication methods. Acta Biomater. 2020, 106, 54–69. [Google Scholar] [CrossRef] [PubMed]
- Maugeri, G.; D’Agata, V.; Trovato, B.; Roggio, F.; Castorina, A.; Vecchio, M.; Di Rosa, M.; Musumeci, G. The role of exercise on peripheral nerve regeneration: From animal model to clinical application. Heliyon 2021, 7, e08281. [Google Scholar] [CrossRef] [PubMed]
- Franzblau, L.E.; Shauver, M.J.; Chung, K.C. Patient satisfaction and self-reported outcomes after complete brachial plexus avulsion injury. J. Hand Surg. 2014, 39, 948–955. [Google Scholar] [CrossRef]
- Welch, J.A. Peripheral nerve injury. Semin. Vet. Med. Surg. Small Anim. 1996, 11, 273–284. [Google Scholar] [CrossRef]
- Santifort, K.M. Return of function in a feline thoracic limb after suspected traumatic brachial plexus injury with loss of nociception. Vet. Rec. Case Rep. 2016, 4, e000334. [Google Scholar] [CrossRef]
- Smith, B.W.; Daunter, A.K.; Yang, L.J.S.; Wilson, T.J. An Update on the Management of Neonatal Brachial Plexus Palsy—Replacing Old Paradigms: A Review. JAMA Pediatr. 2018, 172, 585. [Google Scholar] [CrossRef]
- Rich, J.A.; Newell, A.; Williams, T. Traumatic brachial plexus injury rehabilitation using neuromuscular electrical muscle stimulation in a polytrauma patient. BMJ Case Rep. 2019, 12, e232107. [Google Scholar] [CrossRef] [PubMed]
- Helgeson, K.; Stoneman, P. Shoulder injuries in rugby players: Mechanisms, examination, and rehabilitation. Phys. Ther. Sport 2014, 15, 218. [Google Scholar] [CrossRef] [PubMed]
- Dijkstra, J.R.; Meek, M.; Robinson, P.H.; Gramsbergen, A. Methods to evaluate functional nerve recovery in adult rats: Walking track analysis, video analysis and the withdrawal reflex. J. Neurosci. Methods 2000, 96, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Meek, M.F.; Van Der Werff, J.F.A.; Nicolai, J.P.A.; Gramsbergen, A. Biodegradable p (DLLA-e-CL) Nerve guides versus autologous nerve grafts: Electromyographic amd video analysis. Muscle Nerve 2001, 24, 753–759. [Google Scholar] [CrossRef] [PubMed]
- Watson, N.C.; Jejurikar, S.; Kalliainen, L.K.; Calderon, M.S.; Urbanchek, M.G.; Eguchi, T.; Kuzon, J.R. Range of motion physiotherapy reduces the force deficit in antagonists to denervated rat muscles. J. Surg. Res. 2001, 99, 156–160. [Google Scholar] [CrossRef] [PubMed]
- Siegel, S.G.; Patton, B.; English, A.W. Ciliary neurotrophic factor is required for motoneuron sprouting. Exp. Neurol. 2000, 166, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Varejão, A.S.P.; Cabrita, A.M.; Geuna, S.; Melo-Pinto, P.; Filipe, V.M.; Gramsbergen, A.; Meek, M.F. Toe out angle: A functional index for the evaluation of sciatic nerve recovey in the rat model. Exp. Neurol. 2003, 183, 695–699. [Google Scholar] [CrossRef]
- Sullivan, R.; Dailey, T.; Duncan, K.; Abel, N.; Borlongan, C.V. Peripheral Nerve Injury: Stem Cell Therapy and Peripheral Nerve Transfer. Int. J. Mol. Sci. 2016, 17, 2101. [Google Scholar] [CrossRef]
- Faroni, A.; Mobasseri, S.A.; Kingham, P.J.; Reid, A.J. Peripheral nerve regeneration: Experimental strategies and future perspectives. Adv. Drug Deliv. Rev. 2015, 82–83, 160–167. [Google Scholar] [CrossRef]
- Magnaghi, V.; Procacci, P.; Tata, A.M. Chapter 15: Novel pharmacological approaches to Schwann cells as neuroprotective agents for peripheral nerve regeneration. Int. Rev. Neurobiol. 2009, 87, 295–315. [Google Scholar]
- Ni, L.; Yao, Z.; Zhao, Y.; Zhang, T.; Wang, J.; Li, S.; Chen, Z. Electrical stimulation therapy for peripheral nerve injury. Front. Neurol. 2023, 14, 1081458. [Google Scholar] [CrossRef] [PubMed]
- Belviso, I.; Palermi, S.; Sacco, A.M.; Romano, V.; Corrado, B.; Zappia, M.; Sirico, F. Brachial plexus injuries in sport medicine: Clinical evaluation, diagnostic approaches, treatment options and rehabilitative interventions. J. Funct. Morphol. Kinesiol. 2020, 5, 22. [Google Scholar] [CrossRef] [PubMed]
- Javeed, S.; Faraji, A.H.; Dy, C.; Ray, W.Z.; MacEwan, M.R. Application of electrical stimulation for peripheral nerve regeneration: Stimulation parameters and future horizons. Interdiscip. Neurosurg. Adv. Tech. Case Manag. 2021, 24, 101117. [Google Scholar] [CrossRef]
- Gordon, T.; Udina, E.; Verge, V.M.K.; de Chaves, E.I.P. Brief electrical stimulation accelerates axon regeneration in the peripheral nervous system and promotes sensory axon regeneration in the central nervous system. Motor Control 2009, 13, 412–441. [Google Scholar] [CrossRef] [PubMed]
- Aglah, C.; Gordon, T.; de Chaves, E.I.P. cAMP promotes neurite outgrowth and extension through protein kinase A but independently of Erk activation in cultured rat motoneurons. Neuropharmacology 2008, 55, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Singh, B.; Xu, Q.-G.; Franz, C.K.; Zhang, R.; Dalton, C.; Gordon, T.; Verge, V.M.K.; Midha, R.; Zochodne, D.W. Accelerated axon outgrowth, guidance, and target reinnervation across nerve transection gaps following a brief electrical stimulation paradigm: Laboratory investigation. J. Neurosurg. 2012, 116, 498–512. [Google Scholar] [CrossRef]
- McGregor, C.E.; English, A.W. The role of BDNF in peripheral nerve regeneration: Activity-dependent treatments and Val66Met. Front. Cell. Neurosci. 2019, 12, 522. [Google Scholar] [CrossRef]
- Hoffman, H. Acceleration and retardation of the process of axon-sprouting in partially denervated muscles. Aust. J. Exp. Biol. Med. Sci. 1952, 30, 541–566. [Google Scholar] [CrossRef]
- Nix, W.A.; Hopf, H.C. Electrical stimulation of regenerating nerve and its effect on motor recovery. Brain Res. 1983, 272, 21–25. [Google Scholar] [CrossRef]
- Huang, J.; Zhang, Y.; Lu, L.; Hu, X.; Luo, Z. Electrical stimulation accelerates nerve regeneration and functional recovery in delayed peripheral nerve injury in rats. Eur. J. Neurosci. 2013, 38, 3691–3701. [Google Scholar] [CrossRef]
- Song, S.; McConnell, K.W.; Amores, D.; Levinson, A.; Vogel, H.; Quarta, M.; Rando, T.A.; George, P.M. Electrical stimulation of human neural stem cells via conductive polymer nerve guides enhances peripheral nerve recovery. Biomaterials 2021, 275, 120982. [Google Scholar] [CrossRef] [PubMed]
- Cobianchi, S.; Casals-Diaz, L.; Jaramillo, J.; Navarro, X. Differential effects of activity dependent treatments on axonal regeneration and neuropathic pain after peripheral nerve injury. Exp. Neurol. 2013, 240, 157–167. [Google Scholar] [CrossRef] [PubMed]
- English, A.W.; Meador, W.; Carrasco, D.I. Neurotrophin-4/5 is required for the early growth of regenerating axons in peripheral nerves. Eur. J. Neurosci. 2005, 21, 2624–2634. [Google Scholar] [CrossRef]
- Singh, B.; Krishnan, A.; Micu, I.; Koshy, K.; Singh, V.; Martinez, J.A.; Koshy, D.; Xu, F.; Chandrasekhar, A.; Dalton, C.; et al. Peripheral neuron plasticity is enhanced by brief electrical stimulation and overrides attenuated regrowth in experimental diabetes. Neurobiol. Dis. 2015, 83, 134–151. [Google Scholar] [CrossRef] [PubMed]
- Udina, E.; Furey, M.; Busch, S.; Silver, J.; Gordon, T.; Fouad, K. Electrical stimulation of intact peripheral sensory axons in rats promotes outgrowth of their central projections. Exp. Neurol. 2008, 210, 238–247. [Google Scholar] [CrossRef] [PubMed]
- Richard, M.A.; Spaich, E.G.; Serrao, M.; Andersen, O.K. Stimulation site and phase modulation of the withdrawal reflex during gait initiaion. Clin. Neurophysiol. 2015, 126, 2282–2289. [Google Scholar] [CrossRef] [PubMed]
- Pilkar, R.B.; Yarossi, M.; Forrest, G. Empirical mode decomposition as a tool to remove the function electrical stimulation artifact from surface electromyograms: Preliminary investigation. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 1847–1850. [Google Scholar]
- Martins, A.; Gouveia, D.; Cardoso, A.; Gamboa, Ó.; Millis, D.; Ferreira, A. Nervous system modulation through electrical stimulation in companion animals. Acta Vet. Scand. 2021, 63, 22. [Google Scholar] [CrossRef]
- Levine, D.; Bockstahler, B. Electrical stimulation. In Canine Rehabilitation and Physical Therapy; Millis, D., Levine, D., Eds.; Elseviers: Philadelphia, PA, USA, 2014; pp. 342–356. [Google Scholar]
- Haastert-Talini, K.; Schmitte, R.; Korte, N.; Klode, D.; Ratzka, A.; Grothe, C. Electrical stimulation accelerates axonal and functional peripheral nerve regeneration across long gaps. J. Neurotrauma 2011, 28, 661–674. [Google Scholar] [CrossRef]
- Pieber, K.; Herceg, M.; Paternostro-Sluga, T.; Schuhfried, O. Optimizing stimulation parameters in functional electrical stimulation of denervated muscles: A cross-sectional study. J. Neuroeng. Rehabil. 2015, 12, 51. [Google Scholar] [CrossRef]
- Chiaramonte, R.; Pavone, V.; Testa, G.; Pesce, I.; Scaturro, D.; Musumeci, G.; Mauro, G.; Vecchio, M. The role of physical exercise and rehabilitative implication in the process of nerve repair in peripheral neuropathies: A systematic review. Diagnostics 2023, 13, 364. [Google Scholar] [CrossRef]
- Pachter, B.R.; Eberstein, A. Passive Exercise and Reinnervation of the Rat Denervated Extensor Digitorum Longus Muscle after Nerve Crush. Am. J. Phys. Med. Rehabil. 1989, 68, 179–182. [Google Scholar] [CrossRef] [PubMed]
- Sabatier, M.J.; Redmon, N.; Schwartz, G.; English, A.W. Treadmill training promotes axon regeneration in injured peripheral nerves. Exp. Neurol. 2008, 211, 489–493. [Google Scholar] [CrossRef]
- Asensio-Pinilla, E.; Udina, E.; Jaramillo, J.; Navarro, X. Electrical stimulation combined with exercise increase axonal regeneration after peripheral nerve injury. Exp. Neurol. 2009, 219, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Hartley, R.A.; Kordecki, M.E. Rehabilitation of chronic brachial plexus neuropraxia and loss of cervical extension in a high school football player: A case report. Int. J. Sports Phys. Ther. 2018, 13, 1061–1072. [Google Scholar] [CrossRef] [PubMed]
- Cui, J.; Blaha, C.; Moradkhan, R.; Gray, K.S.; Sinoway, L.I. Muscle sympathetic nerve activity responses to dynamic passive muscle stretch in humans. J. Physiol. 2006, 576, 625. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, M.J.; da Paz, M.G.D.S.; Bina, M.T.; Santos, S.N.; Raicher, I.; Galhardoni, R.; Fernandes, D.T.; Yeng, L.T.; Baptista, A.F.; de Andrade, D.C. Neuropathic pain after brachial plexus avulsion-central and peripheral mechanisms. BMC Neurol. 2015, 15, 73. [Google Scholar] [CrossRef] [PubMed]
- Treede, R.-D.; Jensen, T.S.; Campbell, J.N.; Cruccu, G.; Dostrovsky, J.O.; Griffin, J.W.; Hansson, P.; Hughes, R.; Nurmikko, T.; Serra, J. Neuropathic pain: Redefinition and a grading system for clinical and research purposes. Neurology 2008, 70, 1630–1635. [Google Scholar] [CrossRef]
- Vannier, J.L.; Belkheyar, Z.; Oberlin, C.; Montravers, P. Management of neuropathic pain after brachial plexus injury in adult patients: A report of 60 cases. Ann. Fr. Anesth. Reanim. 2008, 27, 890–895. [Google Scholar] [CrossRef]
- Abdel-Aziz, S.; Ghaleb, A.H. Cervical Spinal Cord Stimulation for the Management of Pain from Brachial Plexus Avulsion. Pain Med. 2014, 15, 712–714. [Google Scholar] [CrossRef][Green Version]
- Ciaramitaro, P.; Mondelli, M.; Logullo, F.; Grimaldi, S.; Battiston, B.; Sard, A.; Scarinzi, C.; Migliaretti, G.; Faccani, G.; Cocito, D.; et al. Traumatic peripheral nerve injuries: Epidemiological findings, neuropathic pain and quality of life in 158 patients. J. Peripher. Nerv. Syst. 2010, 15, 120–127. [Google Scholar] [CrossRef]
- Zhou, Y.; Liu, P.; Rui, J.; Zhao, X.; Lao, J. The clinical characteristics of neuropathic pain in patients with total brachial plexus avulsion: A 30-case study. Injury 2016, 47, 1719–1724. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, L.; Meng, C.; Zhou, Y.; Lao, J.; Zhao, X. A new model for the study of neuropathic pain after brachial plexus injury. Injury 2017, 48, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Lovaglio, A.; Socolovsky, M.; Di Masi, G.; Bonilla, G. Treatment of neuropathic pain after peripheral nerve and brachial plexus traumatic injury. Neurol. India 2019, 67, 32. [Google Scholar] [CrossRef] [PubMed]
- Emamhadi, M.; Andalib, S. Successful recovery of sensation loss in upper brachial plexus injuries. Acta Neurochir. 2018, 160, 2019–2023. [Google Scholar] [CrossRef] [PubMed]
- Sadosky, A.; McDermott, A. A review of the epidemiology of painful diabetic peripheral neuropathy, postherpetic neuralgia, and less commonly studied neuropathic pain conditions. Pain Pract. 2008, 8, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Ehde, D.M.; Czerniecki, J.M.; Smith, D.G.; Campbell, K.M.; Edwards, W.T.; Jensen, M.P.; Robinson, L.R. Chronic phantom sensations, phantom pain, residual limb pain, and other regional pain after lower limb amputation. Arch. Phys. Med. Rehabil. 2000, 81, 1039–1044. [Google Scholar] [CrossRef]
- Melzack, R. Phantom limbs. Sci. Am. 1992, 266, 120–126. [Google Scholar] [CrossRef]
- Jensen, T.S.; Krebs, B.; Nielsen, J.; Rasmussen, P. Immediate and long-term phantom limb pain in amputees: Incidence, clinical characteristics and relationship to pre-amputation limb pain. Pain 1985, 21, 267–278. [Google Scholar] [CrossRef]
- Menchetti, M.; Gandini, G.; Gallucci, A.; Della Rocca, G.; Matiasek, L.; Matiasek, K.; Gentilini, F.; Rosati, M. Approaching phantom complex after limb amputation in the canine species. J. Vet. Behav. 2017, 22, 24–28. [Google Scholar] [CrossRef]
- Probstner, D.; Thuler, L.C.; Ishikawa, N.M.; Alvarenga, R.M. Phantom limb phenomena in cancer amputees. Pain Pract. 2010, 10, 249–256. [Google Scholar] [CrossRef]
- Menchetti, M.; Rocca, G.D.; Tartari, I.; Gandini, G.; Di Salvo, A.; Rosati, M. Approaching phantom complex after limb amputation in cats. J. Vet. Behav. 2022, 50, 23–29. [Google Scholar] [CrossRef]











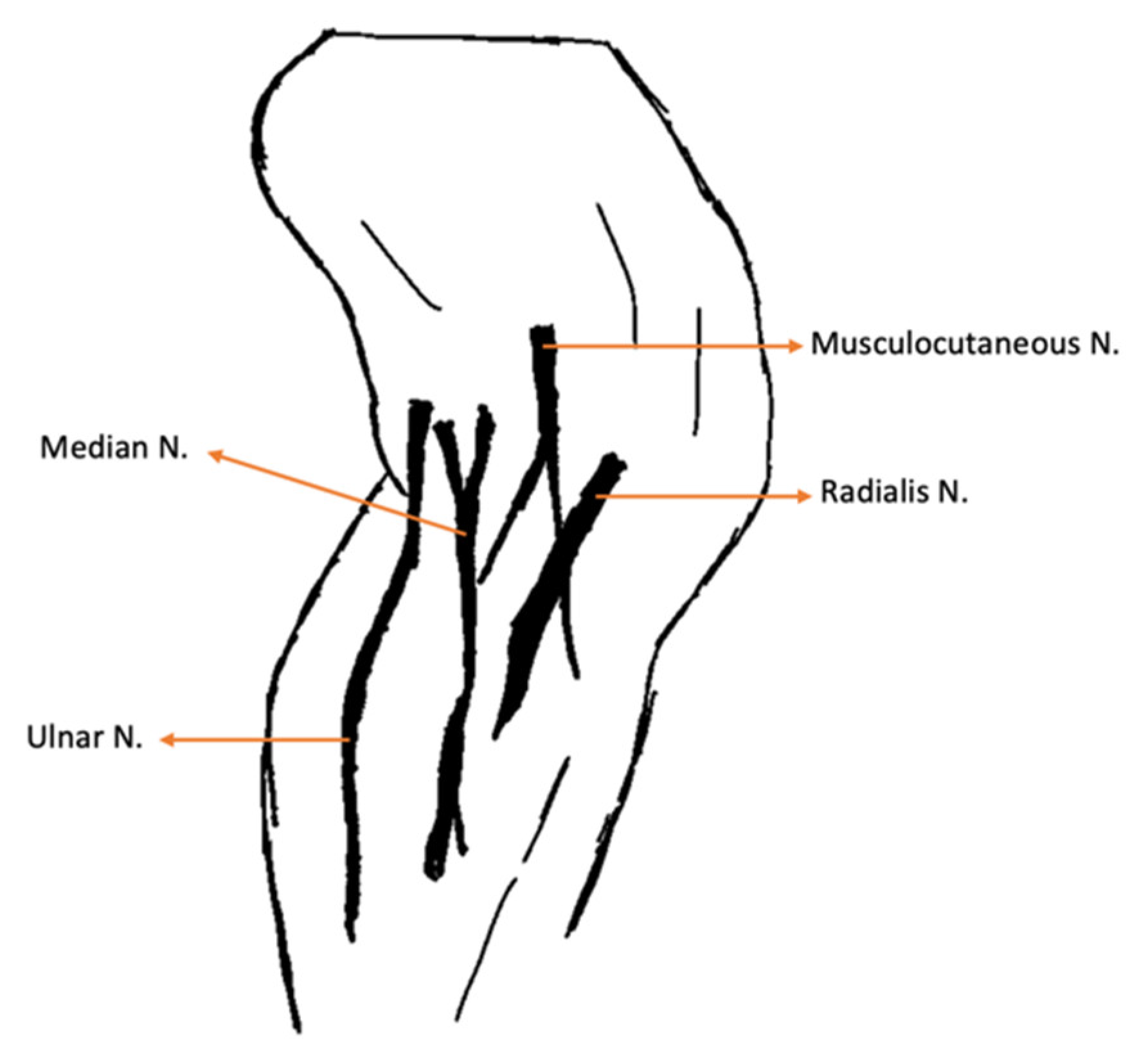
| Nerve | Origin | Innervated Muscles |
|---|---|---|
| Radial | C6, C7, C8, T1, T2 | Extensor carpi ulnaris; Triceps brachialis; Extensor carpi radialis; Lateral and common digital extensor |
| Ulnar | C8, T1, T2 | Deep digital flexor; Flexor carpi ulnaris |
| Median | C7, C8, T1 | Superficial digital flexor; flexor carpi radialis |
| Lateral thoracic | C8, T1 | Cutaneous trunci |
| Nerve | |
|---|---|
| Radial |
|
| Ulnar |
|
| Median |
|
| Type of Variable | Variable Name | Description |
|---|---|---|
| Continuous quantitative |
|
|
|
| |
|
| |
|
| |
| Categorical nominal |
|
|
|
| |
|
| |
|
| |
|
| |
|
| |
|
| |
|
| |
|
| |
|
| |
|
| |
|
| |
|
| |
|
| |
|
|
| Variable | Category | Percentage of Individuals (n = 22) | Mean ± SE (SWNT) |
|---|---|---|---|
| Age | <7 years old ≥7 years old | 72.7 27.3 | 4.86 ± 0.467 (0.021) |
| Weight | <5 kg ≥5 kg | 45.5 54.5 | 4.73 ± 0.239 (0.071) |
| Sex | Male Female | 68.2 31.8 | - |
| Breed | Mixed | 86.4 | - |
| Persian | 13.6 | ||
| Knuckling | Forelimb | Absent: 100 | - |
| Hindlimb | Absent: 90.9 Present: 9.1 | ||
| DPP | 1–4th Digits | Absent: 45.5 Doubtful: 54.5 | - |
| fifth Digit | Present: 40.9 Doubtful: 59.1 | ||
| Withdrawal reflex | Absent: 100 | ||
| Reflexes | Extensor carpi radialis reflex | Absent: 100 | - |
| Cutaneous trunci reflex | Absent: 27.3 Present: 72.7 | ||
| Horner syndrome | Absent: 86.4 Present: 13.6 | ||
| - | |||
| Up to the elbow | Absent: 13.6 Present: 86.4 | - | |
| Dermatomes | Between elbow and carpus | Absent:100 | |
| Between carpus and digits | Absent: 100 | ||
| Joint motion | Shoulder | Absent: 13.6 Present: 86.4 | - |
| Elbow | Absent: 100 | ||
| Carpus | Absent: 100 | ||
| Muscle atrophy | Triceps brachialis | Absent: 86.4 Present: 13.6 | - |
| Extensor carpi radialis | Absent: 100 | ||
| Carpal contracture | Absent: 100 | - | |
| Standing position | Absent: 100 | - | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gouveia, D.; Cardoso, A.; Carvalho, C.; Rijo, I.; Almeida, A.; Gamboa, Ó.; Lopes, B.; Sousa, P.; Coelho, A.; Balça, M.M.; et al. The Role of Early Rehabilitation and Functional Electrical Stimulation in Rehabilitation for Cats with Partial Traumatic Brachial Plexus Injury: A Pilot Study on Domestic Cats in Portugal. Animals 2024, 14, 323. https://doi.org/10.3390/ani14020323
Gouveia D, Cardoso A, Carvalho C, Rijo I, Almeida A, Gamboa Ó, Lopes B, Sousa P, Coelho A, Balça MM, et al. The Role of Early Rehabilitation and Functional Electrical Stimulation in Rehabilitation for Cats with Partial Traumatic Brachial Plexus Injury: A Pilot Study on Domestic Cats in Portugal. Animals. 2024; 14(2):323. https://doi.org/10.3390/ani14020323
Chicago/Turabian StyleGouveia, Débora, Ana Cardoso, Carla Carvalho, Inês Rijo, António Almeida, Óscar Gamboa, Bruna Lopes, Patrícia Sousa, André Coelho, Maria Manuel Balça, and et al. 2024. "The Role of Early Rehabilitation and Functional Electrical Stimulation in Rehabilitation for Cats with Partial Traumatic Brachial Plexus Injury: A Pilot Study on Domestic Cats in Portugal" Animals 14, no. 2: 323. https://doi.org/10.3390/ani14020323
APA StyleGouveia, D., Cardoso, A., Carvalho, C., Rijo, I., Almeida, A., Gamboa, Ó., Lopes, B., Sousa, P., Coelho, A., Balça, M. M., Salgado, A. J., Alvites, R., Varejão, A. S. P., Maurício, A. C., Ferreira, A., & Martins, Â. (2024). The Role of Early Rehabilitation and Functional Electrical Stimulation in Rehabilitation for Cats with Partial Traumatic Brachial Plexus Injury: A Pilot Study on Domestic Cats in Portugal. Animals, 14(2), 323. https://doi.org/10.3390/ani14020323