
Agreement of High-Definition Oscillometry (HDO) and Invasive Blood Pressure Measurements at a Metatarsal Artery in Isoflurane-Anaesthetised Horses
by
 ,
,
Lara Twele
1,*, 
Stephan Neudeck
2,
Julien Delarocque
1,
Nicole Verhaar
1,
Julia Reiners
3,
Mike Noll
4,
Julia Tünsmeyer
2 and
Sabine B. R. Kästner
2,* 1
Clinic for Horses, University of Veterinary Medicine Hannover, Foundation, Bünteweg 9, 30559 Hannover, Germany
2
Small Animal Clinic, University of Veterinary Medicine Hannover, Foundation, Bünteweg 9, 30559 Hannover, Germany
3
AniCura Duisburg-Asterlagen Gmbh, Dr.-Detlev-Karsten-Rohwedder-Str. 11, 47228 Duisburg, Germany
4
Evidensia Tierärztliche Klinik für Kleintiere Norderstedt GmbH, Kabels Stieg 41, 22850 Norderstedt, Germany
*
Authors to whom correspondence should be addressed.
Animals 2022, 12(3), 363; https://doi.org/10.3390/ani12030363
Submission received: 11 January 2022
/
Revised: 29 January 2022
/
Accepted: 31 January 2022
/
Published: 2 February 2022
(This article belongs to the Special Issue Anesthesia and Analgesia in Equids)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Simple Summary
In equine anaesthesia, valid and reliable blood pressure monitoring is crucial for adequate blood pressure management. Various non-invasive blood pressure monitors have been studied with varying results. High-definition oscillometry (HDO) promises greater accuracy than conventional oscillometric devices. With the cuff placed at the tail, the monitor gives satisfactory readings in normotensive anaesthetised horses, while for measuring low and high blood pressure, reliability was inadequate. To date, high-definition oscillometry has not been evaluated at the easily accessible equine metatarsal area. Therefore, the objective of this study was to assess agreement between HDO and invasive blood pressure, both obtained at a metatarsal artery at different blood pressure ranges in anaesthetised horses. Additionally, compliance with the American College of Veterinary Internal Medicine consensus guidelines was assessed. Agreement of HDO and invasive blood pressure was acceptable for mean arterial blood pressure during normotension only. During hypotension and hypertension, measurements were not valid. The monitor failed to meet most of the consensus validation criteria. Consequently, invasive blood pressure measurement remains preferable in haemodynamically unstable patients.
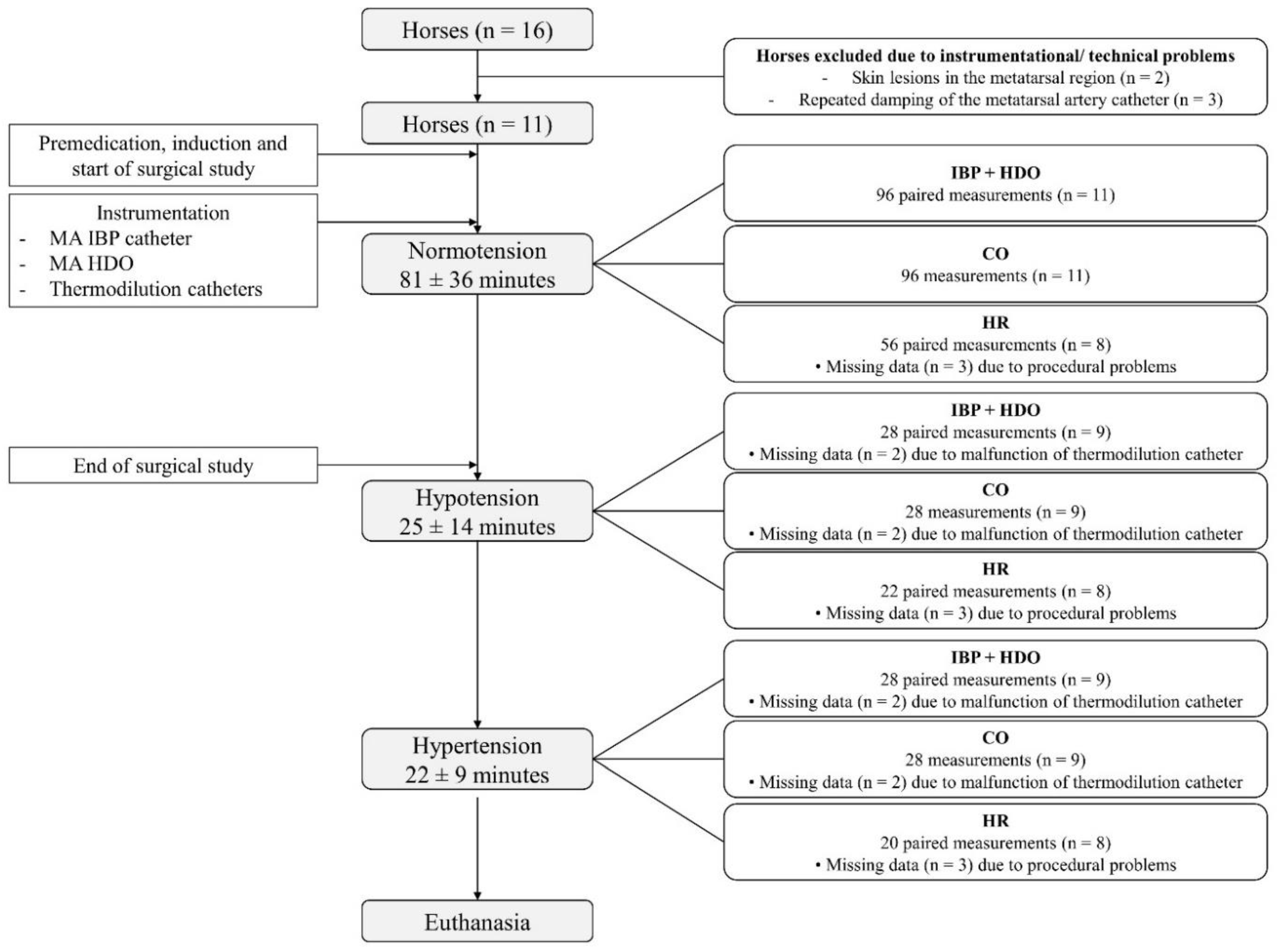
Abstract
High-definition oscillometry (HDO) over the metatarsal artery (MA) in anaesthetised horses has not yet been evaluated. This study aimed to assess agreement between HDO and invasive blood pressure (IBP) at the metatarsal artery, and to evaluate compliance with the American College of Veterinary Internal Medicine (ACVIM) consensus guidelines. In this experimental study, 11 horses underwent general anaesthesia for an unrelated, terminal surgical trial. Instrumentation included an IBP catheter in one and an HDO cuff placed over the contralateral MA, as well as thermodilution catheters. Systolic arterial pressure (SAP), mean arterial pressure (MAP), diastolic arterial pressure (DAP), and cardiac output were measured simultaneously. Normotension (MAP 61–119 mmHg) was maintained during the surgical study. Subsequently, hypotension (MAP ≤ 60 mmHg) and hypertension (MAP ≥ 120 mmHg) were induced pharmacologically. For MAP, the agreement between HDO and IBP was acceptable during normotension, while during hypotension and hypertension, IBP was overestimated and underestimated by HDO, respectively. The monitor failed to meet most ACVIM validation criteria. Consequently, if haemodynamic compromise or rapid blood pressure changes are anticipated, IBP remains preferable.