
Biomarkers of Coagulation and Inflammation in Dogs after Randomized Administration of 6% Hydroxyethyl Starch 130/0.4 or Hartmann’s Solution

 , ,
, ,  ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials & Methods
2.1. Study Design
2.2. Sample Collection
2.3. Coagulation Biomarker Measurement
2.4. Inflammation Biomarker Measurement
2.5. Sample Size Calculation
2.6. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yozova, I.D.; Howard, J.; Sigrist, N.E.; Adamik, K.N. Current Trends in Volume Replacement Therapy and the Use of Synthetic Colloids in Small Animals—An Internet-Based Survey (2016). Front. Vet. Sci. 2017, 4, 140. [Google Scholar] [CrossRef] [PubMed]
- Hopper, K.; Garcia Rojas, A.; Barter, L. An Online Survey of Small Animal Veterinarians Regarding Current Fluid Therapy Practices in Dogs and Cats. J. Am. Vet. Med. Assoc. 2018, 252, 553–559. [Google Scholar] [CrossRef] [PubMed]
- Lobo, D.N.; Stanga, Z.; Aloysius, M.M.; Wicks, C.; Nunes, Q.M.; Ingram, K.L.; Risch, L.; Allison, S.P. Effect of Volume Loading with 1 Liter Intravenous Infusions of 0.9% Saline, 4% Succinylated Gelatine (Gelofusine) and 6% Hydroxyethyl Starch (Voluven) on Blood Volume and Endocrine Responses: A Randomized, Three-Way Crossover Study in Healthy Volunteers. Crit. Care Med. 2010, 38, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Lewis, S.R.; Pritchard, M.W.; Evans, D.J.; Butler, A.R.; Alderson, P.; Smith, A.F.; Roberts, I. Colloids Versus Crystalloids for Fluid Resuscitation in Critically Ill People. Cochrane Database Syst. Rev. 2018, 8, CD000567. [Google Scholar] [CrossRef]
- Rasmussen, K.C.; Secher, N.H.; Pedersen, T. Effect of Perioperative Crystalloid or Colloid Fluid Therapy on Hemorrhage, Coagulation Competence, and Outcome: A Systematic Review and Stratified Meta-Analysis. Medicine 2016, 95, e4498. [Google Scholar] [CrossRef]
- Spahn, D.R.; Bouillon, B.; Cerny, V.; Duranteau, J.; Filipescu, D.; Hunt, B.J.; Komadina, R.; Maegele, M.; Nardi, G.; Riddez, L. The European Guideline on Management of Major Bleeding and Coagulopathy Following Trauma. Crit. Care 2019, 23, 98. [Google Scholar] [CrossRef]
- Boyd, C.J.; Brainard, B.M.; Smart, L. Intravenous Fluid Administration and the Coagulation System. Front. Vet. Sci. 2021, 8, 326. [Google Scholar] [CrossRef]
- Falco, S.; Bruno, B.; Maurella, C.; Bellino, C.; D’Angelo, A.; Gianella, P.; Tarducci, A.; Zanatta, R.; Borrelli, A. In Vitro Evaluation of Canine Hemostasis Following Dilution with Hydroxyethyl Starch (130/0.4) Via Thromboelastometry. J. Vet. Emerg. Crit. Care 2012, 22, 640–645. [Google Scholar] [CrossRef]
- Wurlod, V.A.; Howard, J.; Francey, T.; Schweighauser, A.; Adamik, K.N. Comparison of the in Vitro Effects of Saline, Hypertonic Hydroxyethyl Starch, Hypertonic Saline, and Two Forms of Hydroxyethyl Starch on Whole Blood Coagulation and Platelet Function in Dogs. J. Vet. Emerg. Crit. Care 2015, 25, 474–487. [Google Scholar] [CrossRef]
- Boyd, C.; Claus, M.; Raisis, A.; Hosgood, G.; Sharp, C.; Smart, L. Hypocoagulability and Platelet Dysfunction Are Exacerbated by Synthetic Colloids in a Canine Hemorrhagic Shock Model. Front. Vet. Sci. 2018, 5, 279. [Google Scholar] [CrossRef]
- Gauthier, V.; Holowaychuk, M.; Kerr, C.; Bersenas, A.; Darren Wood, R. Effect of Synthetic Colloid Administration on Coagulation in Healthy Dogs and Dogs with Systemic Inflammation. J. Vet. Intern. Med. 2015, 29, 276–285. [Google Scholar] [CrossRef]
- Iannucci, C.; Dirkmann, D.; Howard, J.; Adamik, K.N. A Prospective Randomized Open-Label Trial on the Comparative Effects of 6% Hydroxyethyl Starch 130/0.4 Versus Polyionic Isotonic Crystalloids on Coagulation Parameters in Dogs with Spontaneous Hemoperitoneum. J. Vet. Emerg. Crit. Care 2020, 31, 32–42. [Google Scholar] [CrossRef]
- Treib, J.; Haass, A.; Pindur, G.; Miyachita, C.; Grauer, M.T.; Jung, F.; Wenzel, E.; Schimrigk, K. Highly Substituted Hydroxyethyl Starch (Hes 200/0.62) Leads to Type-L Von Willebrand Syndrome after Repeated Administration. Pathophysiol. Haemost. Thromb. 1996, 26, 210–213. [Google Scholar] [CrossRef]
- Tsai, M.-C.; Chen, W.-J.; Ching, C.-H.; Chuang, J.-I. Resuscitation with Hydroxyethyl Starch Solution Prevents Nuclear Factor Κb Activation and Oxidative Stress after Hemorrhagic Shock and Resuscitation in Rats. Shock 2007, 27, 527–533. [Google Scholar] [CrossRef]
- Xie, J.; Lv, R.; Yu, L.; Huang, W. Hydroxyethyl Starch 130/0.4 Inhibits Production of Plasma Proinflammatory Cytokines and Attenuates Nuclear Factor-Κb Activation and Toll-Like Receptors Expression in Monocytes During Sepsis. J. Surg. Res. 2010, 160, 133–138. [Google Scholar] [CrossRef]
- Smart, L.; Boyd, C.J.; Claus, M.A.; Bosio, E.; Hosgood, G.; Raisis, A. Large-Volume Crystalloid Fluid Is Associated with Increased Hyaluronan Shedding and Inflammation in a Canine Hemorrhagic Shock Model. Inflammation 2018, 41, 1515–1523. [Google Scholar] [CrossRef]
- Boyd, C.J.; Sharp, C.R.; Claus, M.A.; Raisis, A.L.; Hosgood, G.; Smart, L. Prospective Randomized Controlled Blinded Clinical Trial Evaluating Biomarkers of Acute Kidney Injury Following 6% Hydroxyethyl Starch 130/0.4 or Hartmann’s Solution in Dogs. J. Vet. Emerg. Crit. Care 2021, 31, 306–314. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D.; The Consort Group. Consort 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. BMC Med. 2010, 8, 18. [Google Scholar] [CrossRef]
- Turner, K.; Boyd, C.J.; Rossi, G.; Sharp, C.R.; Claus, M.A.; Francis, A.; Smart, L. Allergy, inflammation, hepatopathy and coagulation biomarkers in dogs with suspected anaphylaxis due to insect envenomation. Front. Vet. Sci. 2022, 9, 875339. [Google Scholar] [CrossRef]
- Chee, W.; Sharp, C.R.; Boyd, C.J.; Claus, M.A.; Smart, L. Stability of Ex Vivo Coagulation Factor Activity in Never-Frozen and Thawed Refrigerated Canine Plasma Stored for 42 Days. J. Vet. Emerg. Crit. Care 2022, 32, 189–195. [Google Scholar] [CrossRef]
- Sharkey, L.C.; Little, K.J.; Williams, K.D.; Todd, J.M.; Richardson, R.; Gwynn, A.D.; Rendahl, A. Performance Characteristics of the Turbidimetric Acl-Top Cts 300 Coagulation Analyzer in Dogs and Cats. J. Vet. Emerg. Crit. Care 2018, 28, 317–325. [Google Scholar] [CrossRef]
- Hayes, G.; Mathews, K.; Doig, G.; Kruth, S.; Boston, S.; Nykamp, S.; Poljak, Z.; Dewey, C. The Acute Patient Physiologic and Laboratory Evaluation (Apple) Score: A Severity of Illness Stratification System for Hospitalized Dogs. J. Vet. Intern. Med. 2010, 24, 1034–1047. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, D.C.; Aldrich, J.; Haskins, S.C.; Drobatz, K.J.; Cowgill, L.D. Assessment of Changes in Blood Volume in Response to Resuscitative Fluid Administration in Dogs. J. Vet. Emerg. Crit. Care 2005, 15, 185–192. [Google Scholar] [CrossRef]
- Brunkhorst, F.M.; Engel, C.; Bloos, F.; Meier-Hellmann, A.; Ragaller, M.; Weiler, N.; Moerer, O.; Gruendling, M.; Oppert, M.; Grond, S. Intensive Insulin Therapy and Pentastarch Resuscitation in Severe Sepsis. N. Engl. J. Med. 2008, 358, 125–139. [Google Scholar] [CrossRef] [PubMed]
- Myburgh, J.A.; Finfer, S.; Bellomo, R.; Billot, L.; Cass, A.; Gattas, D.; Glass, P.; Lipman, J.; Liu, B.; McArthur, C. Hydroxyethyl Starch or Saline for Fluid Resuscitation in Intensive Care. N. Engl. J. Med. 2012, 367, 1901–1911. [Google Scholar] [CrossRef] [PubMed]
- Perner, A.; Haase, N.; Guttormsen, A.B.; Tenhunen, J.; Klemenzson, G.; Åneman, A.; Madsen, K.R.; Møller, M.H.; Elkjær, J.M.; Poulsen, L.M. Hydroxyethyl Starch 130/0.42 Versus Ringer’s Acetate in Severe Sepsis. N. Engl. J. Med. 2012, 367, 124–134. [Google Scholar] [CrossRef] [PubMed]
- Franz, A.; Bräunlich, P.; Gamsjäger, T.; Felfernig, M.; Gustorff, B.; Kozek-Langenecker, S.A. The Effects of Hydroxyethyl Starches of Varying Molecular Weights on Platelet Function. Anesth. Analg. 2001, 92, 1402–1407. [Google Scholar] [CrossRef] [PubMed]
- Lucas, C.E.; Denis, R.; Ledgerwood, A.M.; Grabow, D. The Effects of Hespan on Serum and Lymphatic Albumin, Globulin, and Coagulant Protein. Ann. Surg. 1988, 207, 416. [Google Scholar] [CrossRef]
- Carr, M.E. Effect of Hydroxyethyl Starch on the Structure of Thrombin-and Reptilase-Induced Fibrin Gels. J. Lab. Clin. Med. 1986, 108, 556–561. [Google Scholar]
- Nielsen, V.G. Effects of Hextend Hemodilution on Plasma Coagulation Kinetics in the Rabbit: Role of Factor XIII-Mediated Fibrin Polymer Crosslinking. J. Surg. Res. 2006, 132, 17–22. [Google Scholar] [CrossRef]
- Strauss, R.; Stump, D.; Henriksen, R.; Saunders, R. Effects of Hydroxyethyl Starch on Fibrinogen, Fibrin Clot Formation, and Fibrinolysis. Transfusion 1985, 25, 230–234. [Google Scholar] [CrossRef]
- De Laforcade, A.M.; Freeman, L.M.; Shaw, S.P.; Brooks, M.B.; Rozanski, E.A.; Rush, J.E. Hemostatic Changes in Dogs with Naturally Occurring Sepsis. J. Vet. Intern. Med. 2003, 17, 674–679. [Google Scholar] [CrossRef]
- Gottlieb, D.L.; Prittie, J.; Buriko, Y.; Lamb, K.E. Evaluation of Acute Traumatic Coagulopathy in Dogs and Cats Following Blunt Force Trauma. J. Vet. Emerg. Crit. Care 2017, 27, 35–43. [Google Scholar] [CrossRef]
- Holowaychuk, M.K.; Hanel, R.M.; Darren Wood, R.; Rogers, L.; O’Keefe, K.; Monteith, G. Prospective Multicenter Evaluation of Coagulation Abnormalities in Dogs Following Severe Acute Trauma. J. Vet. Emerg. Crit. Care 2014, 24, 93–104. [Google Scholar] [CrossRef]
- Obradovic, M.; Kurz, A.; Kabon, B.; Roth, G.; Kimberger, O.; Zotti, O.; Bayoumi, A.; Reiterer, C.; Stift, A.; Fleischmann, E. The Effect of Intraoperative Goal-Directed Crystalloid Versus Colloid Administration on Perioperative Inflammatory Markers-a Substudy of a Randomized Controlled Trial. BMC Anesthesiol. 2020, 20, 210. [Google Scholar] [CrossRef]
- Anthon, C.; Müller, R.; Haase, N.; Hjortrup, P.; Møller, K.; Lange, T.; Wetterslev, J.; Perner, A. Effects of Hydroxyethyl Starch 130/0.42 Vs. Ringer’s Acetate on Cytokine Levels in Severe Sepsis. Acta Anaesthesiol. Scand. 2017, 61, 904–913. [Google Scholar] [CrossRef]
- Voigtsberger, S.; Urner, M.; Hasler, M.; Roth Z’Graggen, B.; Booy, C.; Spahn, D.R.; Beck-Schimmer, B. Modulation of Early Inflammatory Response by Different Balanced and Non-Balanced Colloids and Crystalloids in a Rodent Model of Endotoxemia. PLoS ONE 2014, 9, e93863. [Google Scholar] [CrossRef]
- Fletcher, D.J.; Rozanski, E.A.; Brainard, B.M.; Laforcade, A.M.; Brooks, M.B. Assessment of the Relationships among Coagulopathy, Hyperfibrinolysis, Plasma Lactate, and Protein C in Dogs with Spontaneous Hemoperitoneum. J. Vet. Emerg. Crit. Care 2016, 26, 41–51. [Google Scholar] [CrossRef]
- Smith, M.R.; Wurlod, V.A.; Ralph, A.G.; Daniels, E.R.; Mitchell, M. Mortality Rate and Prognostic Factors for Dogs with Severe Anaphylaxis: 67 Cases (2016–2018). J. Am. Vet. Med. Assoc. 2020, 256, 1137–1144. [Google Scholar] [CrossRef]
- Kelley, D.; Lester, C.; Shaw, S.; de Laforcade, A.; Webster, C. Thromboelastographic Evaluation of Dogs with Acute Liver Disease. J. Vet. Intern. Med. 2015, 29, 1053–1062. [Google Scholar] [CrossRef]
- Larsson, A.; Tynngård, N.; Kander, T.; Bonnevier, J.; Schött, U. Comparison of Point-of-Care Hemostatic Assays, Routine Coagulation Tests, and Outcome Scores in Critically Ill Patients. J. Crit. Care 2015, 30, 1032–1038. [Google Scholar] [CrossRef]
- Yates, D.; Davies, S.; Milner, H.; Wilson, R. Crystalloid or Colloid for Goal-Directed Fluid Therapy in Colorectal Surgery. Br. J. Anaesth. 2014, 112, 281–289. [Google Scholar] [CrossRef]
- McBride, D.; Hosgood, G.L.; Mansfield, C.S.; Smart, L. Effect of Hydroxyethyl Starch 130/0.4 and 200/0.5 Solutions on Canine Platelet Function in Vitro. Am. J. Vet. Res. 2013, 74, 1133–1137. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Transfusion Type | HES | CRYST |
|---|---|---|
| No transfusion (n) | 16 | 16 |
| Packed red blood cells only (n) | 1 | 0 |
| Plasma only (n) | 2 | 0 |
| Both packed red blood cells and plasma (n) | 2 * | 2 # |
| Biomarker | Time Main Effect | Treatment Main Effect | Treatment-by-Time Interaction Effect |
|---|---|---|---|
| Prothrombin time | 0.002 | 0.53 | 0.68 |
| Activated partial thromboplastin time | 0.12 | 0.025 | 0.72 |
| Thrombin time | 0.39 | 0.24 | 0.68 |
| Fibrinogen concentration | 0.029 | 0.54 | 0.24 |
| Factor V activity | <0.001 | 0.87 | 0.46 |
| Factor VII activity | <0.001 | 0.94 | 0.36 |
| Factor VIII activity | 0.006 | 0.15 | 0.16 |
| Factor IX activity | <0.001 | 0.49 | 0.76 |
| Factor X activity | <0.001 | 0.81 | 0.45 |
| von Willebrand factor antigen | 0.028 | 0.74 | 0.39 |
| Antithrombin activity | <0.001 | 0.92 | 0.42 |
| Protein C activity | <0.001 | 0.75 | 0.08 |
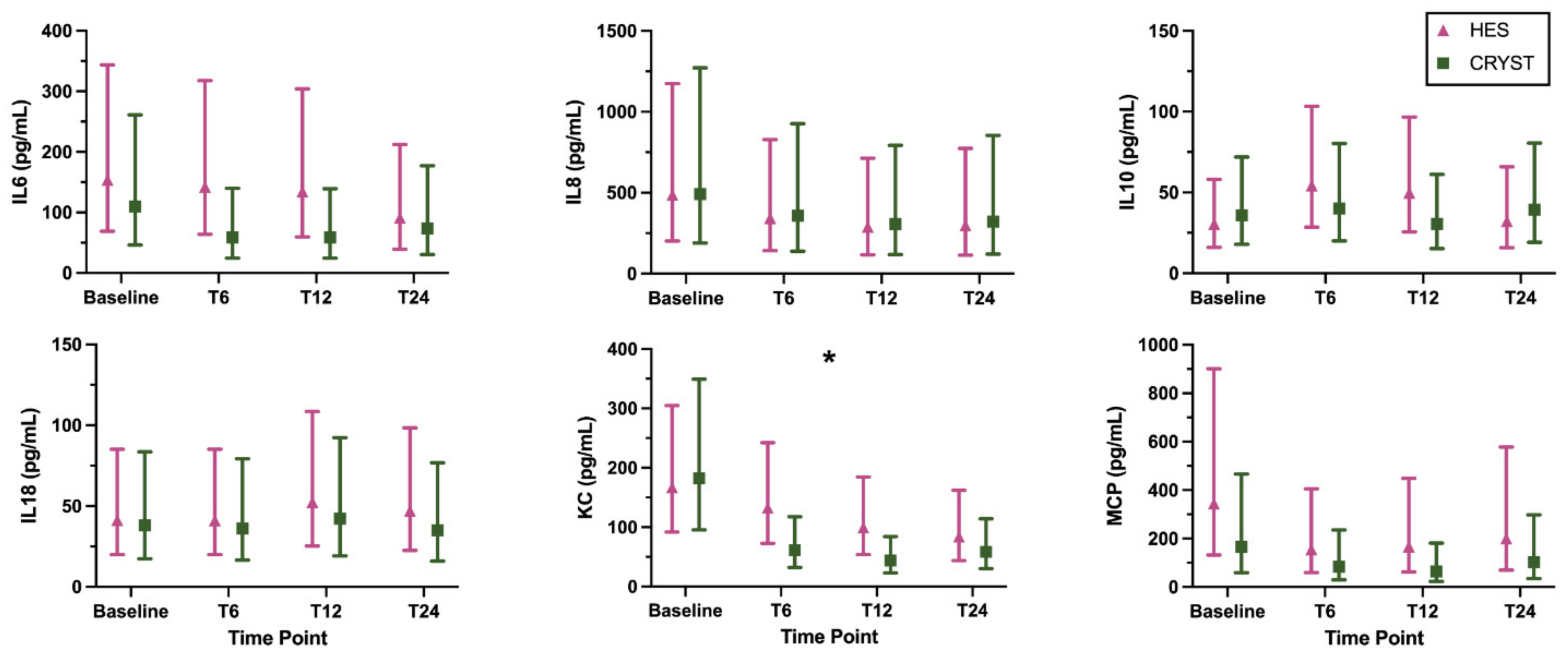
| Interleukin 6 * | 0.09 | 0.31 | 0.22 |
| Interleukin 8 * | 0.27 | 0.93 | 1.00 |
| Interleukin 10 * | 0.47 | 0.78 | 0.37 |
| Interleukin 18 * | 0.17 | 0.73 | 0.69 |
| Keratinocyte-derived chemokine * | <0.001 | 0.23 | 0.06 |
| Monocyte chemoattractant protein-1 * | 0.053 | 0.22 | 0.96 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boyd, C.J.; Raisis, A.L.; Sharp, C.R.; Claus, M.A.; Hosgood, G.; Smart, L. Biomarkers of Coagulation and Inflammation in Dogs after Randomized Administration of 6% Hydroxyethyl Starch 130/0.4 or Hartmann’s Solution. Animals 2022, 12, 2691. https://doi.org/10.3390/ani12192691
Boyd CJ, Raisis AL, Sharp CR, Claus MA, Hosgood G, Smart L. Biomarkers of Coagulation and Inflammation in Dogs after Randomized Administration of 6% Hydroxyethyl Starch 130/0.4 or Hartmann’s Solution. Animals. 2022; 12(19):2691. https://doi.org/10.3390/ani12192691
Chicago/Turabian StyleBoyd, Corrin J., Anthea L. Raisis, Claire R. Sharp, Melissa A. Claus, Giselle Hosgood, and Lisa Smart. 2022. "Biomarkers of Coagulation and Inflammation in Dogs after Randomized Administration of 6% Hydroxyethyl Starch 130/0.4 or Hartmann’s Solution" Animals 12, no. 19: 2691. https://doi.org/10.3390/ani12192691
APA StyleBoyd, C. J., Raisis, A. L., Sharp, C. R., Claus, M. A., Hosgood, G., & Smart, L. (2022). Biomarkers of Coagulation and Inflammation in Dogs after Randomized Administration of 6% Hydroxyethyl Starch 130/0.4 or Hartmann’s Solution. Animals, 12(19), 2691. https://doi.org/10.3390/ani12192691