1. Introduction
Nosebands may be used in horse-riding for an aesthetic effect (so-called framing of the horse’s face) and to keep the horse’s mouth closed [
1]. By doing so, they may stabilise the bit in a preferred position and prevent the horse attempting to avoid bit pressure by putting the tongue out of the mouth or over the bit [
2]. These behaviours are sometimes called evasions because they reduce the rider’s control of the horse and even attract penalties in some disciplines, notably dressage.
Historically, an informal guideline for gauging noseband tightness has been to check if two adult fingers can be fitted between horse’s nose and the noseband [
3]. The origin of this standard is unknown, but it has been appearing in equestrian texts since 1956 [
4], up until the present [
5,
6,
7,
8,
9]. However, perhaps as the perceived competitive advantages that were anticipated from tight nosebands became more broadly recognised, manual checking alone was questioned because of its imprecision [
10]. One solution was the use of a standardised taper gauge such as that produced by the International Society for Equitation Science (ISES, [
11]).
A recent European study of 750 eventing, dressage, and performance hunter horses [
12] assessed the prevalence of tight nosebands in various equestrian disciplines. It found that 7% had space to accommodate 0.5 of a finger, 23% had space for 1 finger, 19% for 1.5 fingers, and 44% wore nosebands that allowed no space between the noseband and the skin over the nasal plane. Only 7% of nosebands would have passed the historic test and allowed for the placement of at least 2 fingers.
Concern has been expressed globally that nosebands in some equestrian disciplines, such as eventing, have become progressively tighter over the past two decades to the point that their current tightness may now compromise horse welfare [
10,
13]. There is evidence that vascular perfusion may be compromised distal to restrictive nosebands, as a result of a tourniquet effect [
14]. In naïve horses, tight nosebands are associated with transient stress responses and a post inhibitory rebound of behaviours, such as yawning, lip-licking, and chewing, that they restrict [
15]. It has been shown that excessive noseband tightness is associated with lip abrasions and/or blood at the commissures of the lips [
16]. Indeed, it has been suggested that that horses may bear evidence of remodelling of the nasal bones as a result of pressure from nosebands [
10].
A pilot study using archived radiographs of horses’ heads (
n = 60) [
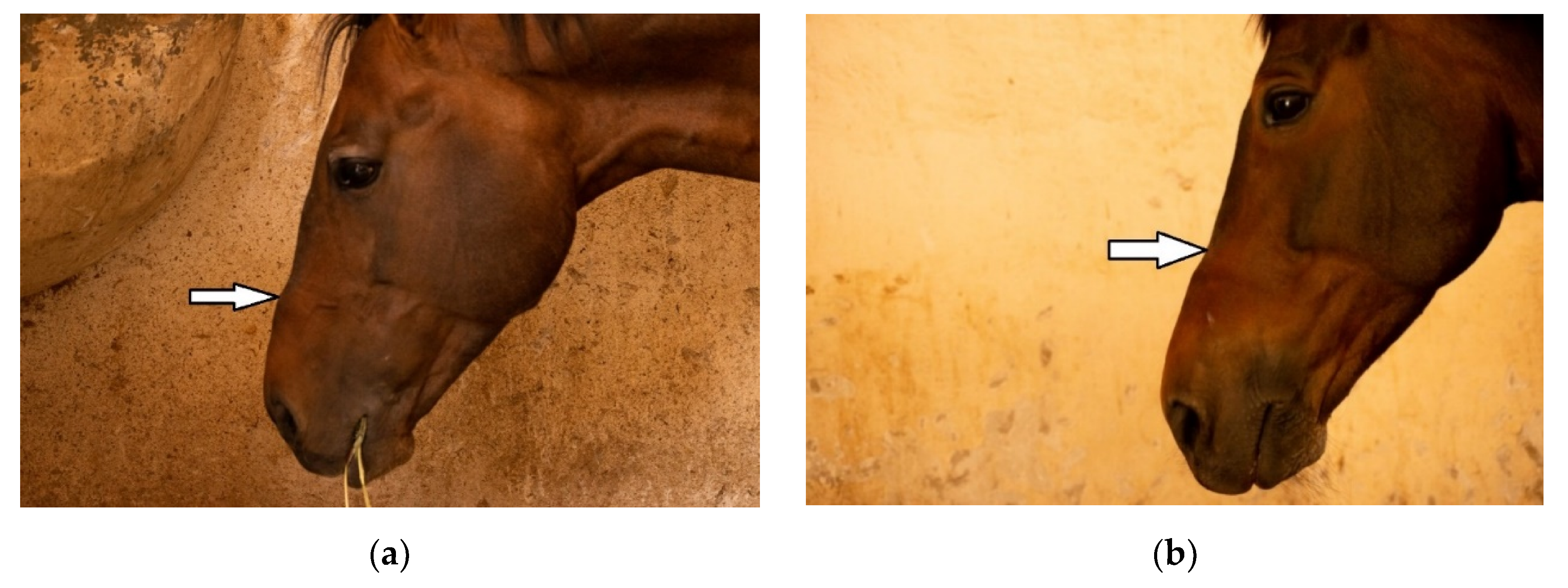
17] revealed that little is known about what constitutes normal appearance of the nasal bones radiographically. The relationships among palpable, visual, and radiologically confirmed changes, including exostoses and concavities, are of particular importance to the discussion about restrictive tightening of nosebands, since the changes detectable without radiography may provide warning signs that encourage carers to loosen nosebands before bony changes develop. It is possible that that both exostoses and concavities may occur in the same horse at the same time as simultaneous forms of remodelling. For example, it is possible that the apparent concavity is the result of remodelling of the bone distally. It is also possible that exostoses may visually and palpably accentuate a neighbouring minor morphological depression. Therefore, when a concavity arises adjacent to an exostosis, it may appear larger than were it to arise alone.
This article describes a non-invasive study of cavalry horses to determine what radiographic changes, if any, arise in equine nasal bones and mandibles at the point of contact with restrictive nosebands and how these changes relate to any palpable or visible changes at these sites.
4. Discussion
We note that the current study provides no evidence of a causal link between any piece of gear or its putative tightness and the lesions in these anatomical locations. It is anticipated that the same cohort of horses will be studied to provide relevant data as we develop the design of a follow-up study. This will move from the current study, that is confined to prevalence and distribution at these anatomical locations, to risk factors for the various lesions reported here. It is expected that the follow-up study will explore the interactive role of multiple putative causal variables including: horse age; horse breed; horse sex; main equestrian disciplines (historic and current) as well as the 97 items of behavioural, management, and training data collected through the nascent Equine Behaviour Assessment Research Questionnaire (E-BARQ) instrument [
21].
The risks of comprised welfare in horses wearing restrictive nosebands are widely recognised by equine welfare scientists [
22]. The current opportunistic study is the first to reveal that physically detectable and radiographic lesions occur in areas of the nasal bones and mandibles likely to be subjected to pressure from restrictive nosebands. These findings are critical to the advance of ethical equitation [
23] that advocates a three-step process for equestrian stakeholders who seek to retain the social license to operate [
24]. It demands that we identify the causes of distress in the horses we ride, that we mitigate these stressors as much as possible, and we justify the retention of those that cannot be mitigated.
A recent survey of horse owners revealed that 9% had observed swelling of the area under the noseband, 14.3% had observed soreness in the area under the noseband, and 39.9% had observed hair loss in the area under the noseband [
25]. Of the subset of current horses suitably pigmented for assessment, 64.5% had white hairs in the nasal bone region, and 15.7% in the mandibular region. This suggests that the hairs of the nasal bones are more vulnerable than those over the mandibles to the type of injury that causes pigment changes. In both sites, the association between white hairs and a palpation finding was weak. Therefore, the presence of white hairs alone should be considered a poor indicator of lesions in these areas.
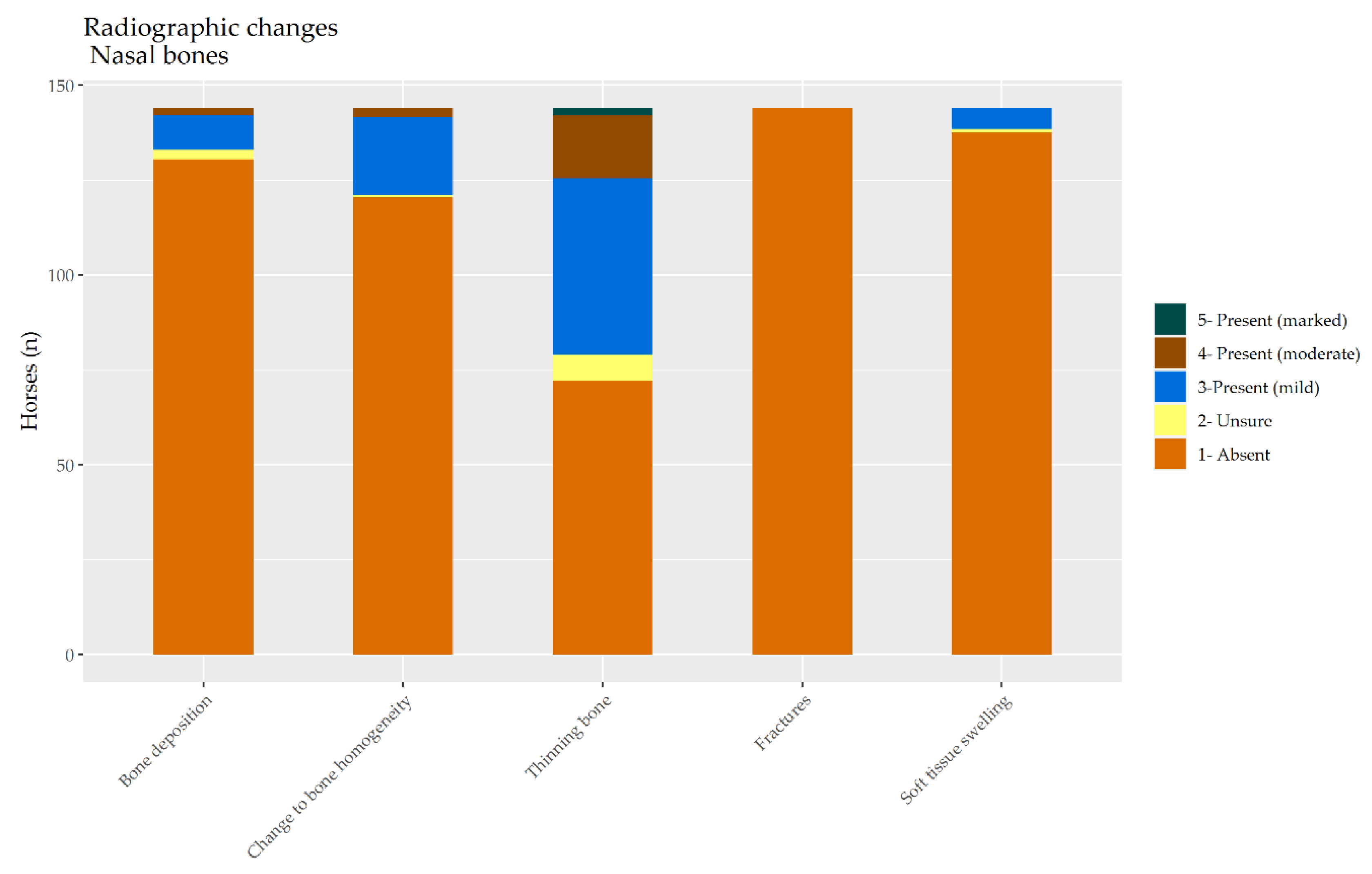
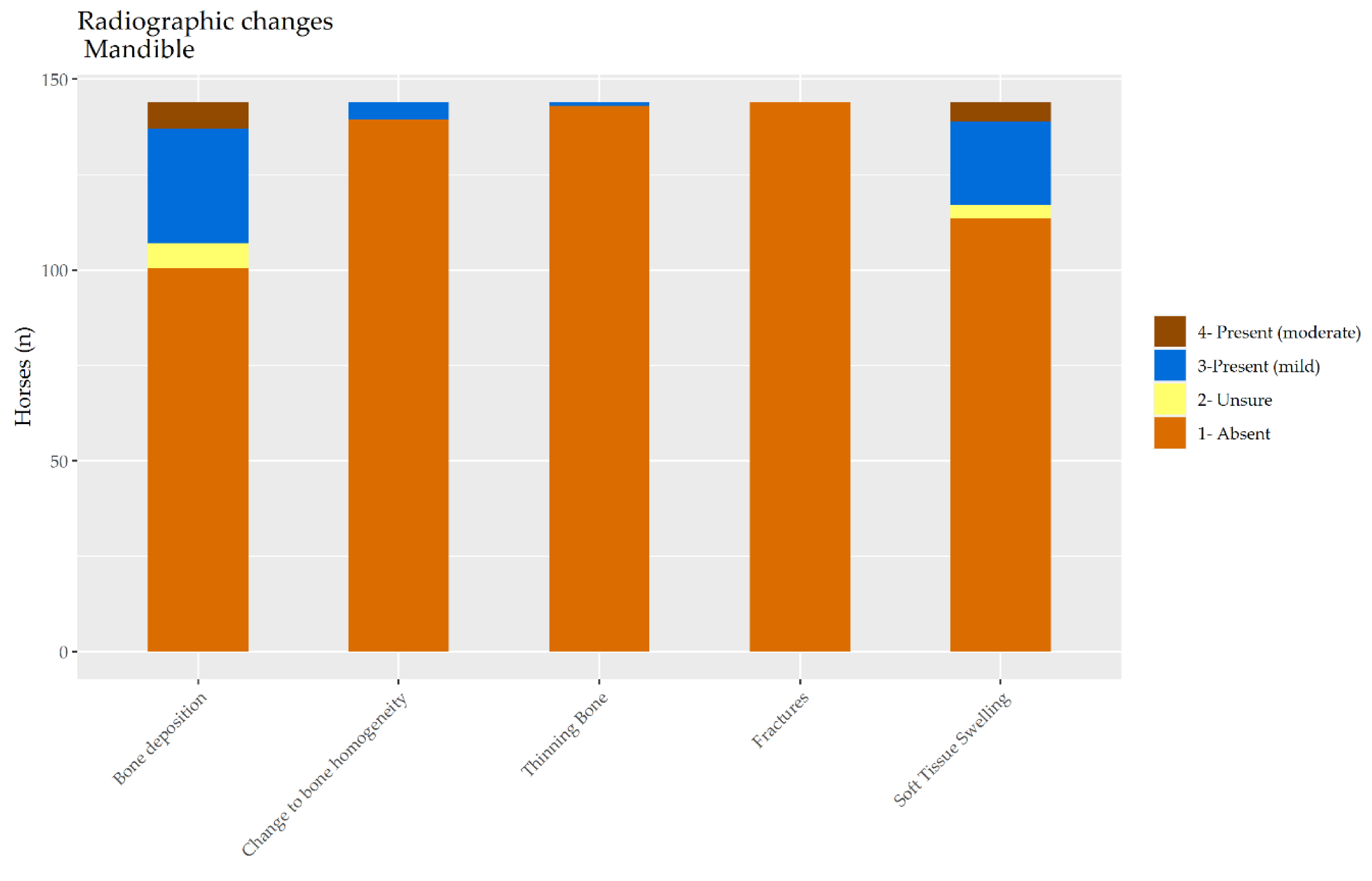
Among the current population, 37.5% had one or more radiographic changes to the nasal bones according to both radiologists, and 13.8% had one or more radiographic changes to the mandible. This indicates that the nasal bones are likely to be more vulnerable to changes. This may reflect the direction of the trauma that leads to these changes or the relative strength of mandibular bone.
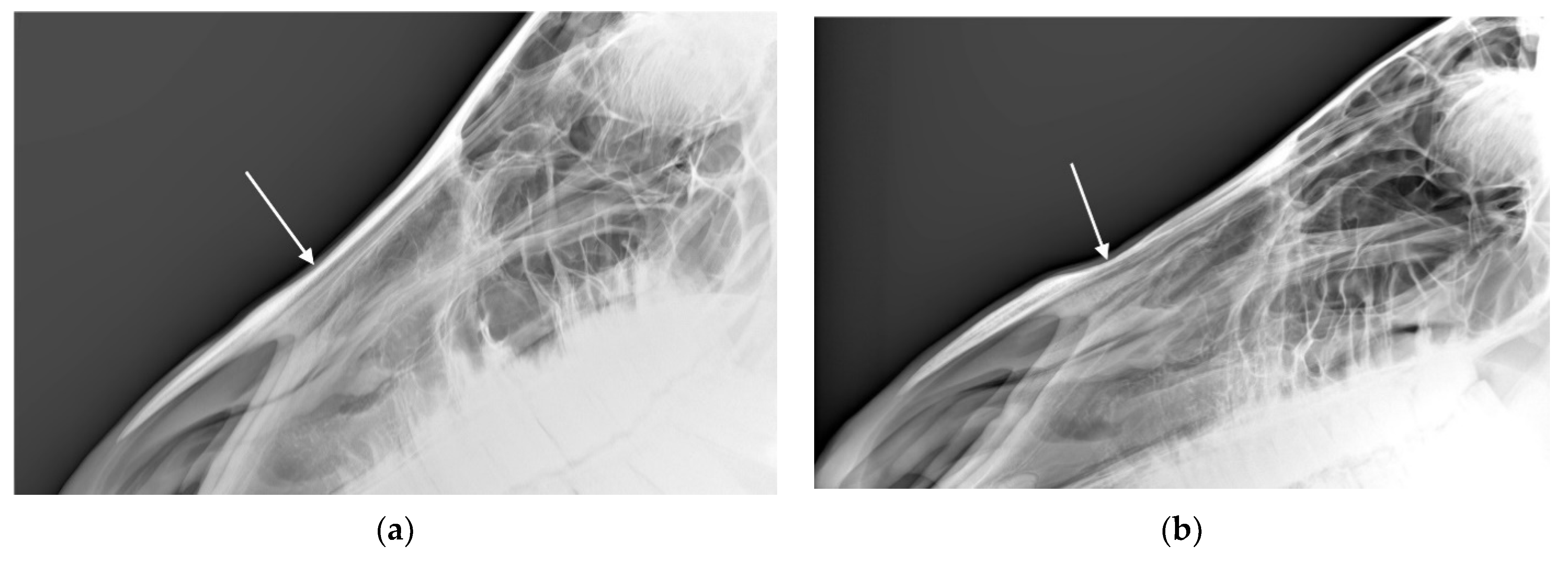
It is worth noting that when considering the nasal bones, exostosis was a more common finding on physical examination, yet, when examined by radiograph, bone thinning was generally more common than new bone deposition. Taken together with the finding that physical examination findings of exostosis were associated with one or more radiographic lesions in the nasal bone whereas physical examination findings of concavity were not, it may be that practitioners who believe they see or palpate exostosis on the nasal bones should have a higher index of suspicion for disease severe enough to cause radiographic lesions than those who believe they see or palpate concavity.
For both the nasal bones and mandibles, agreement on visual appraisal and palpation between observers was moderate and significantly greater than zero. We recommend that visual appraisal and palpation alone should not be relied upon diagnostically. As clinical indicators, they may well lead to imaging but there is evidence that radiological lesions are more profound.
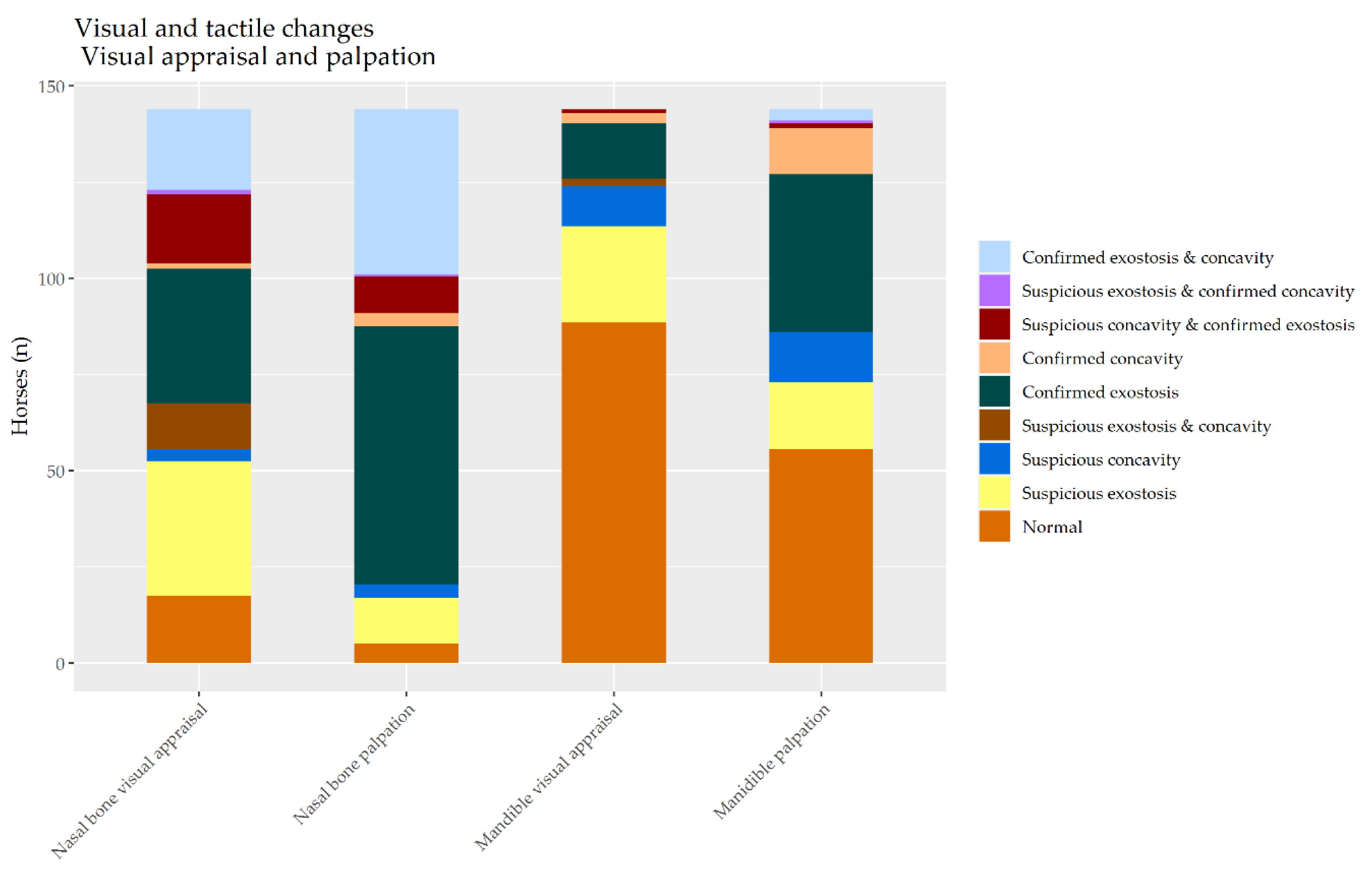
For both the nasal bones and the mandibles, visual appraisal was more likely to detect increases in bone profiles than decreases. However, whereas at least 34% of the horses (depending on the examiner) were at least suspicious for both kinds of change in nasal bones, only up to 3.5% were suspicious for both kinds of change in the mandible. This suggests that observers are generally more familiar with normal appearance of the nasal bones than the mandible.
Palpation appears to be more sensitive to changes on both of these sites than visual appraisal, resulting in more findings of exostosis. Palpation confirmed exostosis in at least 45% of the nasal bones and 27% of the mandibles. Palpation confirmed concavity in at least 2.1% of the nasal bones and 8% of the mandibles. The proportion of horses assessed to be at least suspicious for both sorts of change was at least 36% but again depended on the examiner.
Where there was agreement between the radiologists, 83% of agreement was about bone thinning in the nasal bones and 94% in the mandibles. In contrast, where there was disagreement between the radiologists about bone thinning, 10% of consensus was about bone thinning in the nasal bones and 100% in the mandibles. For bone deposition, where there was disagreement between the radiologists, 90% of consensus was about bone deposition in the nasal bones and 10% in the mandibles. Disagreement about bone thinning in the nasal bones was noticeably the most important source of dispute for these more equivocally affected horses. For the mandibles, disagreement about bone deposition and also soft tissue hypertrophy was the source of dispute for these more equivocally affected horses. This suggests that bone deposition is easier to detect with confidence in the nasal bones than in the mandible.
The limitations of the current study include its reliance on data from veterinary students who were not working in equine practice. That said, it is possible that seasoned equine practitioners may be inured to the presence of lesions at these sites in riding horses. Therefore, the two students who provided visual and palpation data for the current study may have benefited from approaching the question of normality without this possible habituation.
The authors considered calculation of the negative predictive value (NPV) and positive predictive value (PPV) of the physical examination findings for radiographic change but ultimately, rejected them for two main reasons. Firstly, the NPV and PPV are affected by disease prevalence and the horses in the current study represent a unique population subject to unique equitation uses and husbandry that do not necessarily reflect the uses and husbandry of horses more broadly. Secondly, although radiography may be considered prima facie to be somehow ‘more objective’ than physical exam, it does not necessarily follow that radiology should be considered the ‘gold standard’ assessment tool for these lesions, and particularly, that horses who do not show radiographic disease should be considered unaffected by noseband injury. It is not uncommon, as a general principle for clinical signs to precede the development of radiographic change [
26], and the lag between radiology and physical exam was up to several months, meaning that disease may have progressed between assessment by radiology and by physical exam.
Equine skulls are complex structures and so the current focus on the nasal bones meant that mA, kVp, exposure time, and focal spot–film distance were optimised for the nasal bones, not the mandibles. Future studies may benefit from treating the two sites separately. Longitudinal studies will be needed to reveal the role of various risk factors in the ontogeny of these lesions. There may be merit in separating the lesions of the mandible and nasal bones for such an exercise.

 ,
, 










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}