In-Person Caretaker Visits Disrupt Ongoing Discomfort Behavior in Hospitalized Equine Orthopedic Surgical Patients

Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Case Selection
2.2. Data Collection
2.3. Data Analysis
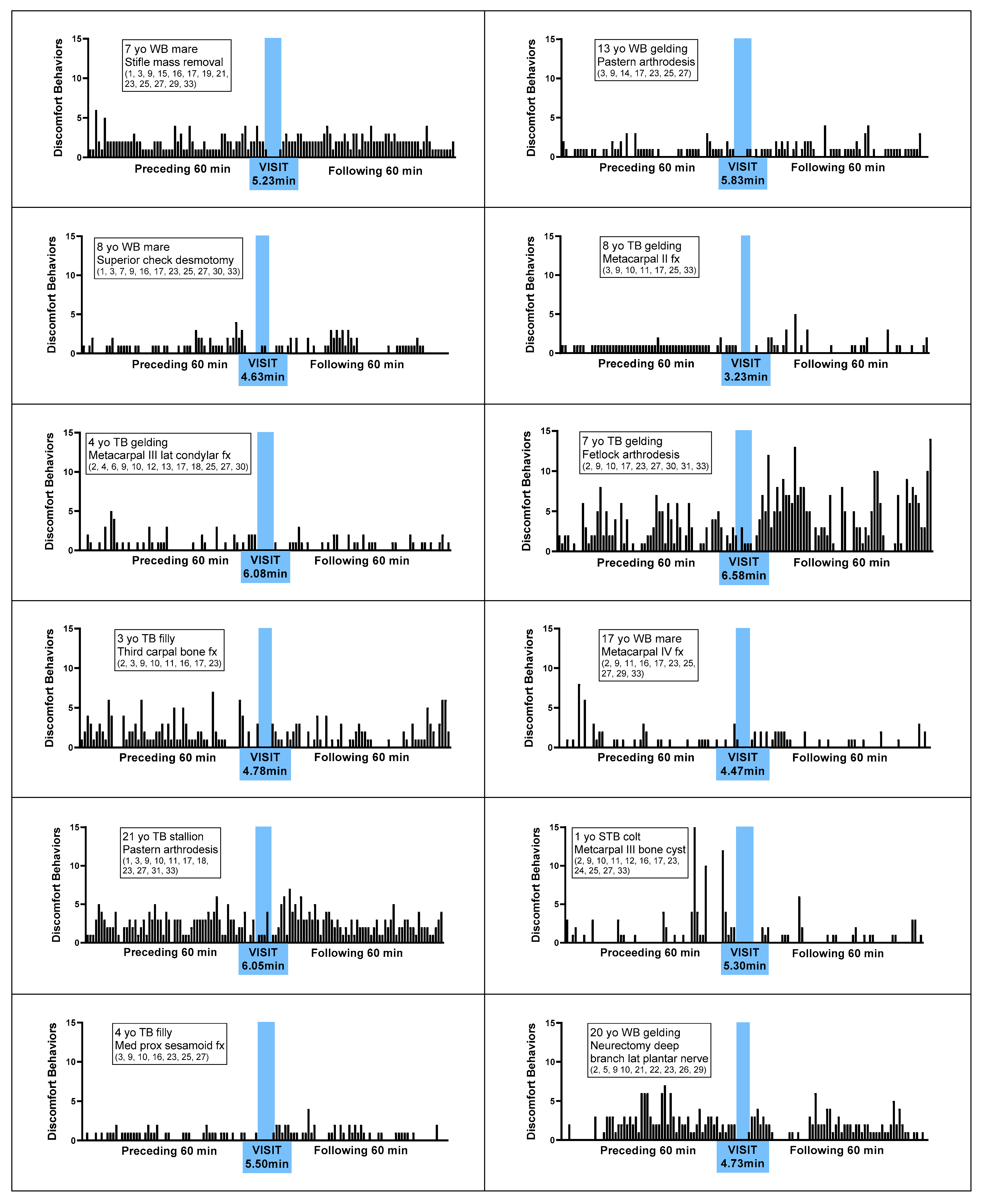
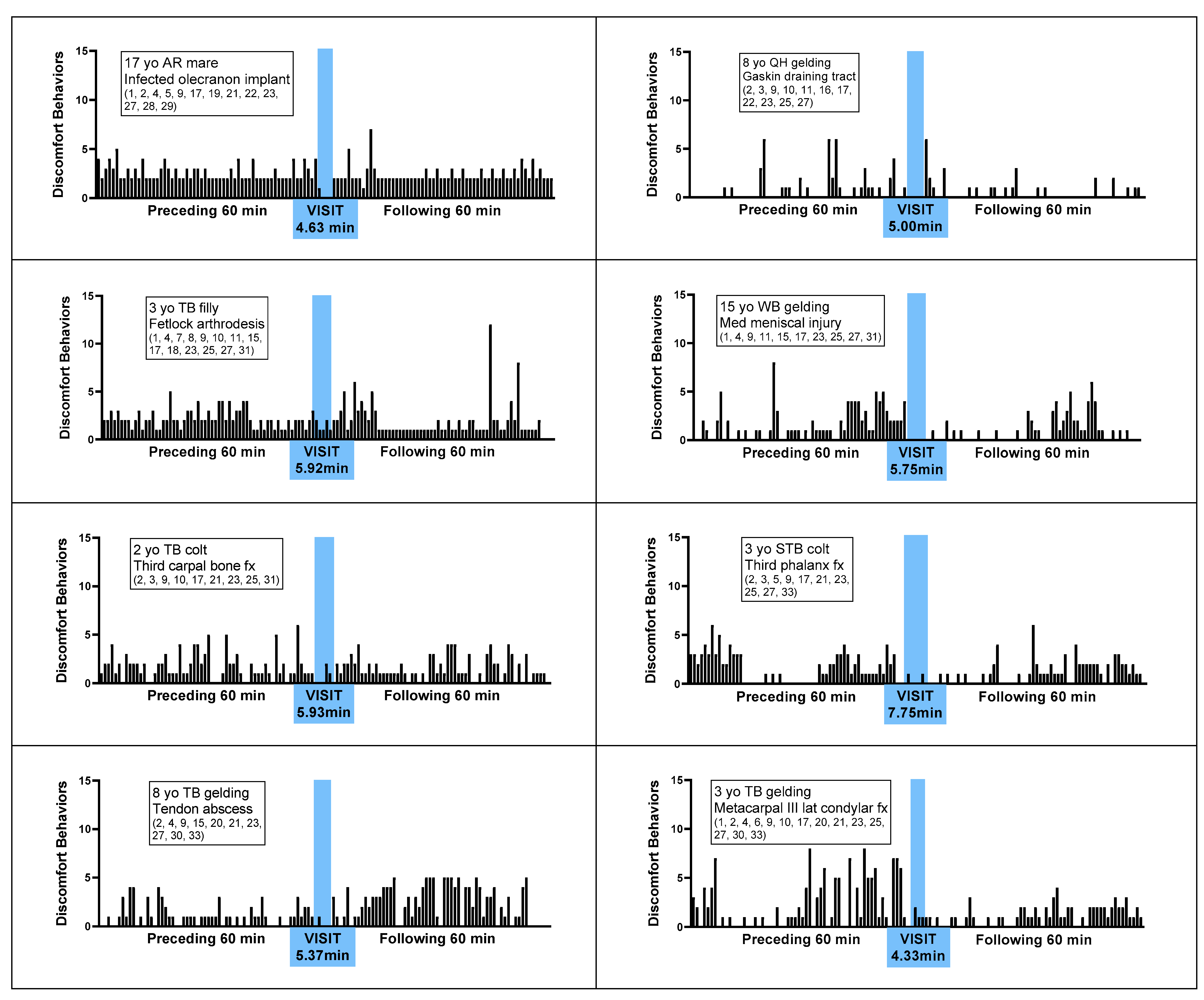
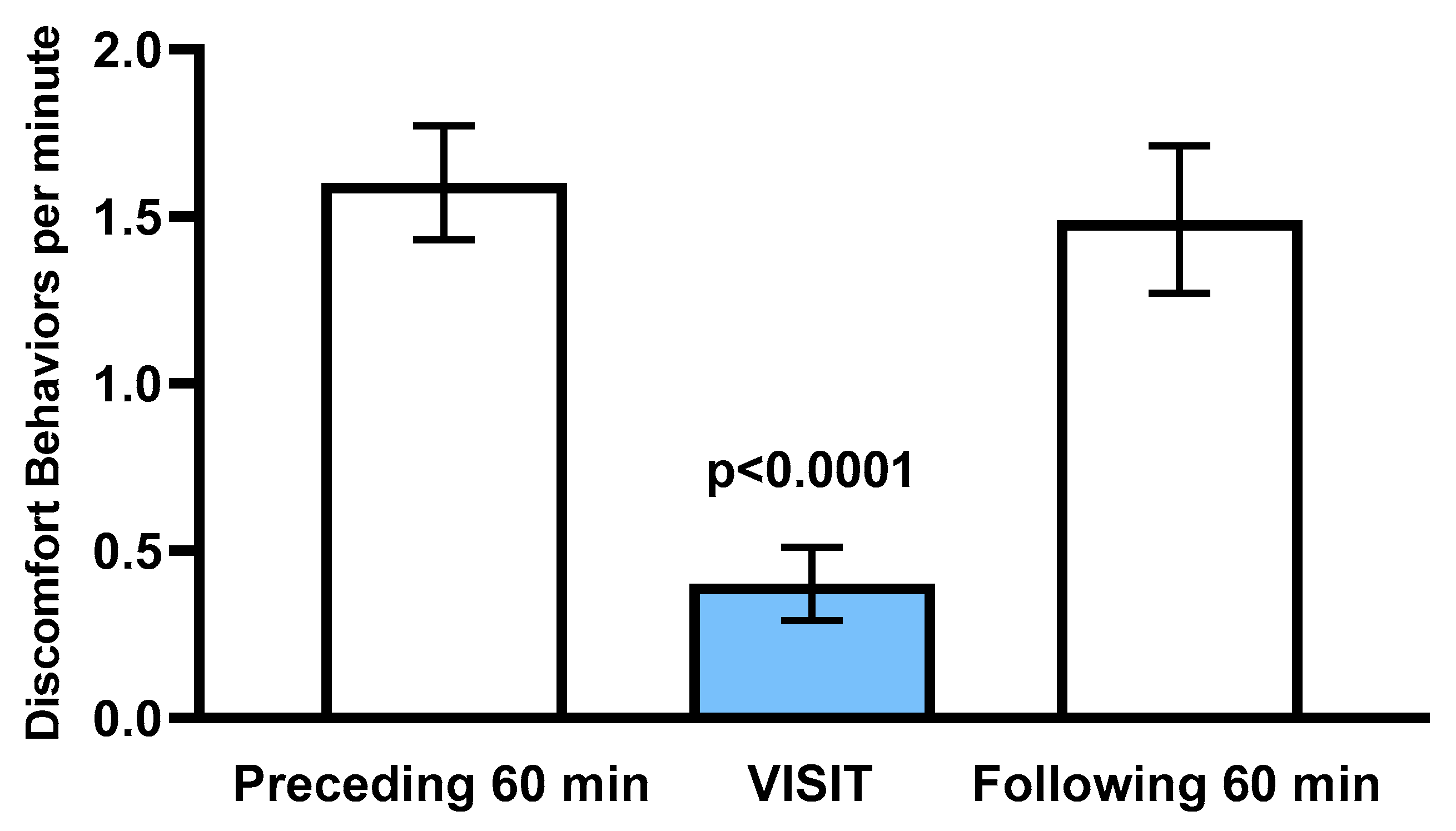
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Behavioral Indicators of Discomfort | ||
| Posture and weight bearing | ||
| 1. Non-physiologic locomotion | Lameness, including altered stride, impact, and weight bearing; may include altered limb placement, head and neck movements that suggest off-loading, and/or limited range of motion of a limb |  |
| 2. Shifting weight | Frequent shifting of the primary weight bearing limb or limbs |   |
| 3. Pointing | Consistent extension of one forelimb, reducing weight bearing on that limb |  |
| 4. Prolonged resting of limb | Flexing a fore or hind limb, resting the toe of the hoof on the substrate for a prolonged period |  |
| 5. Base narrow or wide | Standing or moving with fore and/or hind limbs placed either more medially or laterally than is normal for the horse’s conformation |   |
| 6. Leaning against objects | Supporting weight and/or stabilizing balance against a wall or fence, usually during standing rest |  |
| 7. Atypical recumbency | Prolonged or frequent interrupted recumbent rests and/or increased recumbent resting time budget |   |
| 8. Difficulty rising | Failing to rise gracefully, requiring increased effort and/or attempts to rise |  |
| Limb and body movements | ||
| 9. Stepping in place | Repeated flexing of a limb, briefly relieving weight bearing on that limb |  |
| 10. Lifting/holding limb up | Flexing a limb, lifting the hoof off of the substrate (usually 20cm or more) and then placing it back down |  |
| 11. Pawing | Reaching a forelimb cranially and dragging the hoof along or above the substrate while sweeping the limb caudally, often in rhythmic series |  |
| 12. Kicking out or back | Lifting and extending one or both hind limbs caudally, either straight back or arching laterally |  |
| 13. Romping/Bucking | Alternate rearing and kicking out, often repeatedly in rapid succession |   |
| 14. Rolling | Lying down to sternal recumbency and then rotating from sternal to dorsal recumbency, sometimes from one side to the other |  |
| 15. Flinching | Sudden reflexive contraction of muscles |  |
| 16. Stretching | Extending or straightening part of the body to its full extent, can take multiple forms |   |
| Head, neck, mouth, and lip movements | ||
| 17. Rotational shaking head or whole body | Rapid, rhythmic rotation of the whole body or just the head and neck along the long axis |  |
| 18. Frustration head tossing | Quick rotational toss of the head, similar to a head threat |  |
| 19. Head bobbing | Repetitive rhythmic nodding of the head and neck |  |
| 20. Abbreviated weaving | Rhythmic side-to-side swaying of the head and neck |  |
| 21. Sympathetic surge resolution signs: extending tongue, licking, chewing, itching | Cluster of autonomic responses following an acute sympathetic surge, including salivation (leading to chewing movements, swallowing, tongue extensions) and or/autogrooming (typically rubbing face against forelimb) |   |
| 22. Frequent yawning bouts | Frequent bouts of yawning, often with a greater number of yawns per bout than is characteristic (>3–5) |  |
| Attention to an area | ||
| 23. Looking | Repeated glancing or gazing at a particular area of the body |  |
| 24. Swatting | Swinging the head and neck to bat at a particular area of the body |  |
| 25. Autogrooming | Nibbling, nuzzling, biting at and area of the body, or rubbing one part of the body against another or against an object |   |
| Ear and tail movements | ||
| 26. Moving/focusing ear caudally | Rotating ears to focus caudally, or laying ears back against neck |  |
| 27.Swishing/flicking tail | Moving tail suddenly from side to side |  |
| Overall demeanor | ||
| 28. Changing activities frequently | Uncharacteristically changing major activity (foraging, standing rest, standing alert) more frequently than expected, as often as from minute to minute with other accompanying signs of discomfort | |
| 29. Conservative movement | Less than typical movement about the stall, with apparent hesitation to walk |  |
| 30. Circling/Pacing | Walking in circle usually along a perimeter |  |
| 31. Abandoning recumbency or elimination attempts | Repeated posturing as if intending to lie down, urinate, or defecate that appears interrupted by discomfort |  |
| 32. Nibbling aimlessly | Reduced interest in hay or feed, but continued nominal foraging gestures, often directed at non-food objects |  |
| 33. Fidgeting | Biting, mouthing, or rubbing against objects (e.g., stall walls, feed/water containers) |  |
References
- McDonnell, S. Is it Psychological, Physical or Both? In Proceedings of the 51st AAEP Annual Convention, Seattle, WA, USA, 3–7 December 2005; pp. 231–238. [Google Scholar]
- Gleerup, K.B.; Lindegaard, C. Recognition and quantification of pain in horses: A tutorial review. Equine Vet. Educ. 2016, 28, 47–57. [Google Scholar] [CrossRef]
- Bussières, G.; Jacques, C.; Lainay, O.; Beauchamp, G.; Leblond, A.; Cadoré, J.L.; Desmaizières, L.M.; Cuvelliez, S.G.; Troncy, E. Development of a composite orthopaedic pain scale in horses. Res. Vet. Sci. 2008, 85, 294–306. [Google Scholar] [CrossRef] [PubMed]
- Price, J.; Catriona, S.; Welsh, E.M.; Waran, N.K. Preliminary evaluation of a behaviour-based system for assessment of post-operative pain in horses following arthroscopic surgery. Vet. Anaesth. Analg. 2003, 30, 124–137. [Google Scholar] [CrossRef] [PubMed]
- de Graw, J.C.; van Loon, J.P.A.M. Systematic pain assessment in horses. Vet. J. 2016, 209, 14–22. [Google Scholar] [CrossRef] [PubMed]
- van Loon, J.P.A.M.; van Dierendonck, M.C. Objective pain assessment in horses (2014-2018). Vet. J. 2018, 242, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Dalla Costa, E.; Minero, M.; Lebelt, D.; Stucke, D.; Canali, E.; Leach, M.C. Development of the horse grimace scale (HGS) as a pain assessment tool in horses undergoing routine castration. PLoS ONE. 2014, 9, e92281. [Google Scholar] [CrossRef] [PubMed]
- van Loon, J.P.A.M.; van Dierendonck, M.C. Monitoring acute equine visceral pain with the Equine Utrecht University Scale for Composite Pain Assessment (EQUUS-COMPASS) and the Equine Utrecht Scale for Facial Assessment of Pain (EQUUS-FAP): A scale-construction study. Vet. J. 2015, 206, 356–364. [Google Scholar] [CrossRef] [PubMed]



© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torcivia, C.; McDonnell, S. In-Person Caretaker Visits Disrupt Ongoing Discomfort Behavior in Hospitalized Equine Orthopedic Surgical Patients. Animals 2020, 10, 210. https://doi.org/10.3390/ani10020210
Torcivia C, McDonnell S. In-Person Caretaker Visits Disrupt Ongoing Discomfort Behavior in Hospitalized Equine Orthopedic Surgical Patients. Animals. 2020; 10(2):210. https://doi.org/10.3390/ani10020210
Chicago/Turabian StyleTorcivia, Catherine, and Sue McDonnell. 2020. "In-Person Caretaker Visits Disrupt Ongoing Discomfort Behavior in Hospitalized Equine Orthopedic Surgical Patients" Animals 10, no. 2: 210. https://doi.org/10.3390/ani10020210
APA StyleTorcivia, C., & McDonnell, S. (2020). In-Person Caretaker Visits Disrupt Ongoing Discomfort Behavior in Hospitalized Equine Orthopedic Surgical Patients. Animals, 10(2), 210. https://doi.org/10.3390/ani10020210