
Leaky Gut Syndrome Is Associated with Endotoxemia and Serum (1→3)-β-D-Glucan in Severe Dengue Infection

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
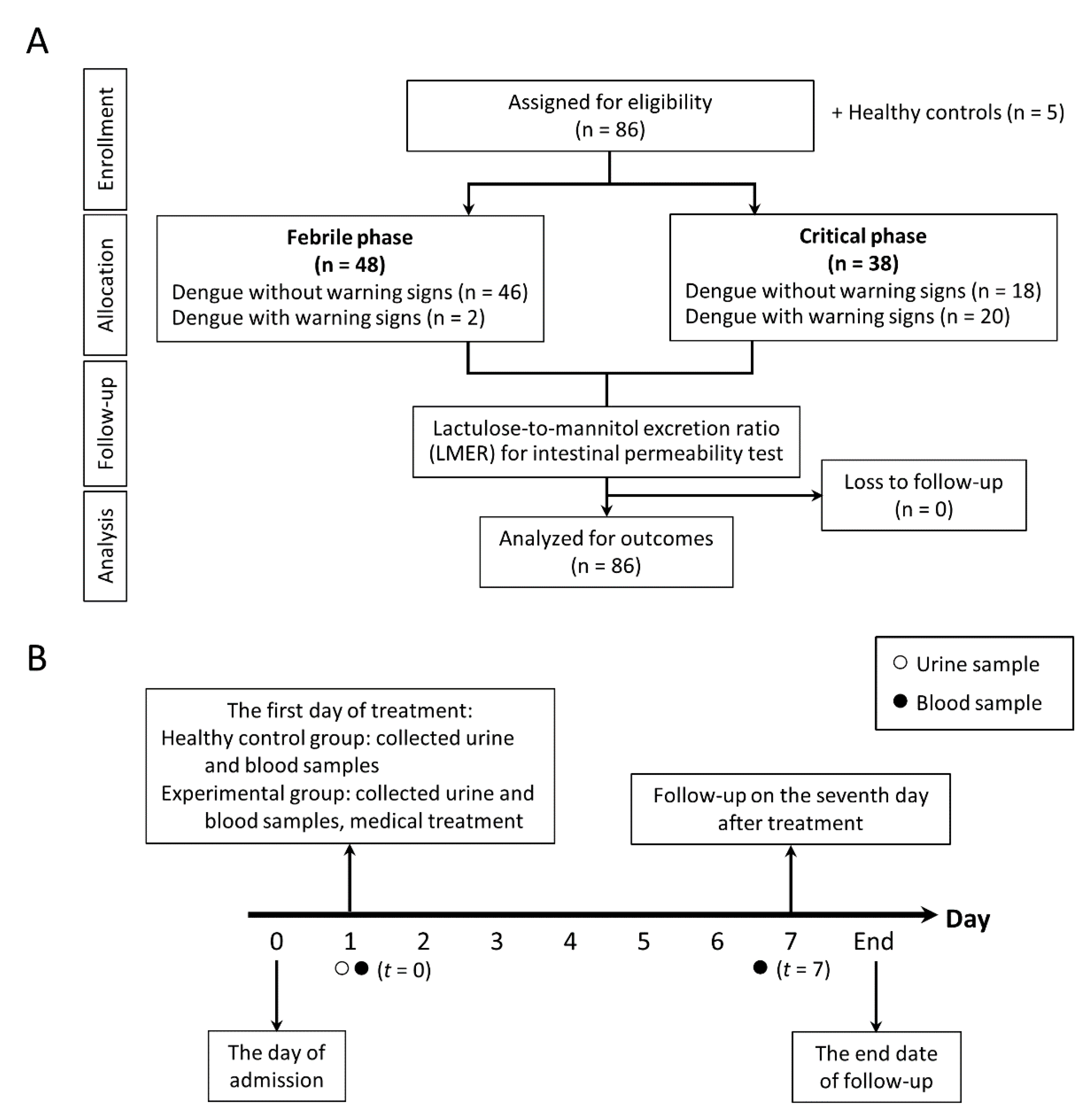
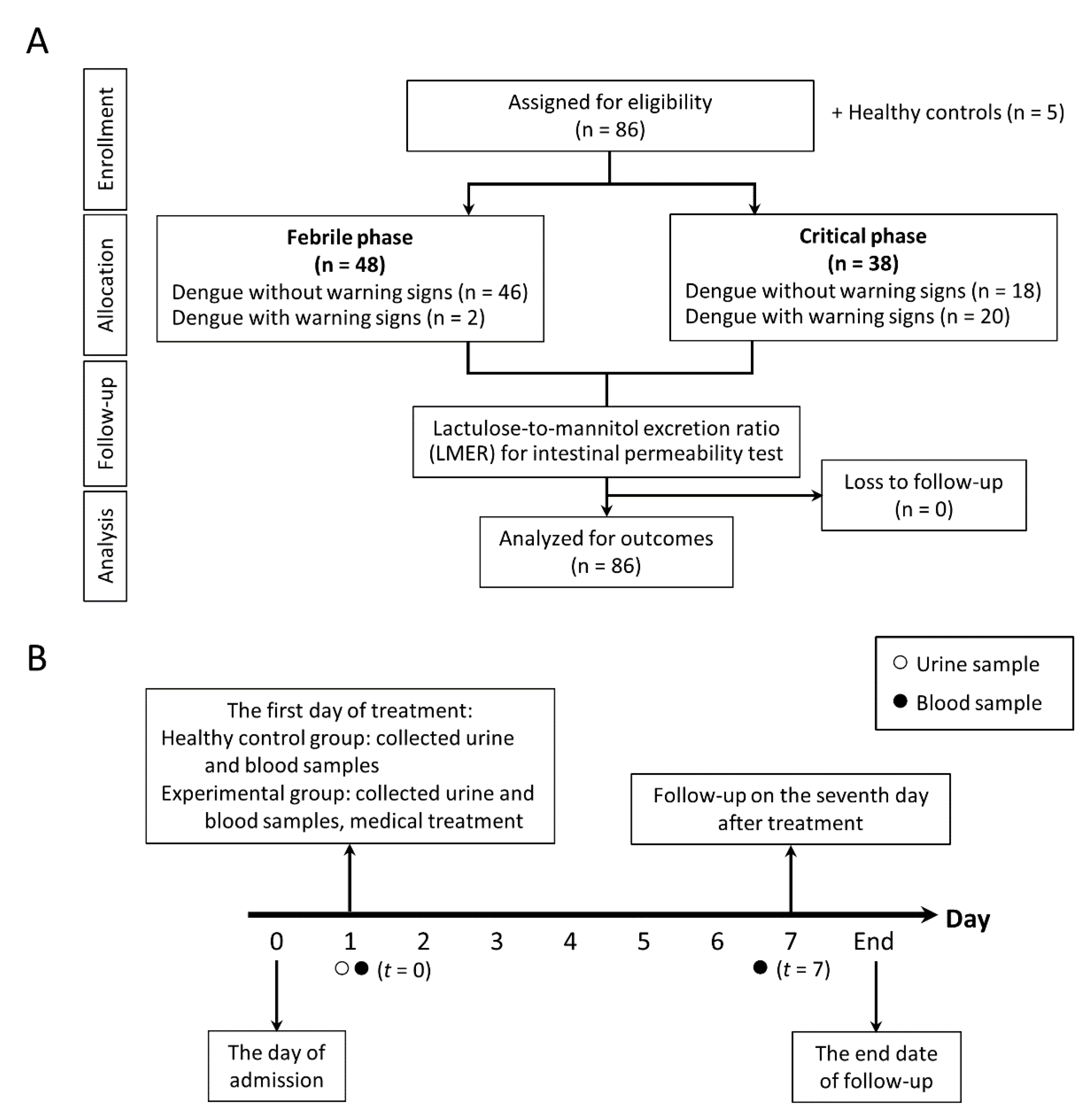
2.1. Enrolled Participants and Study Designs
2.2. Definition
2.3. Gut Permeability Analysis
2.4. Serum Parameters
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Participants
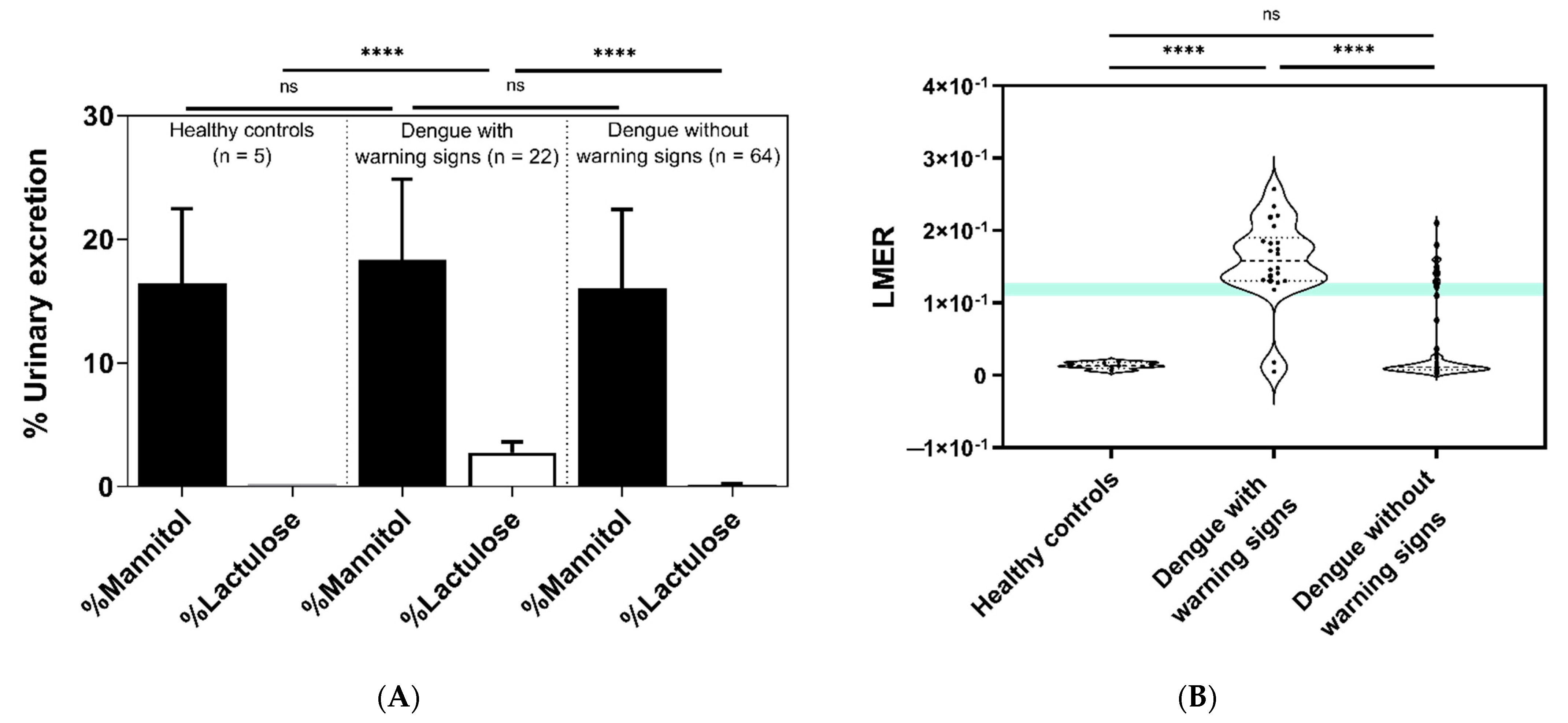
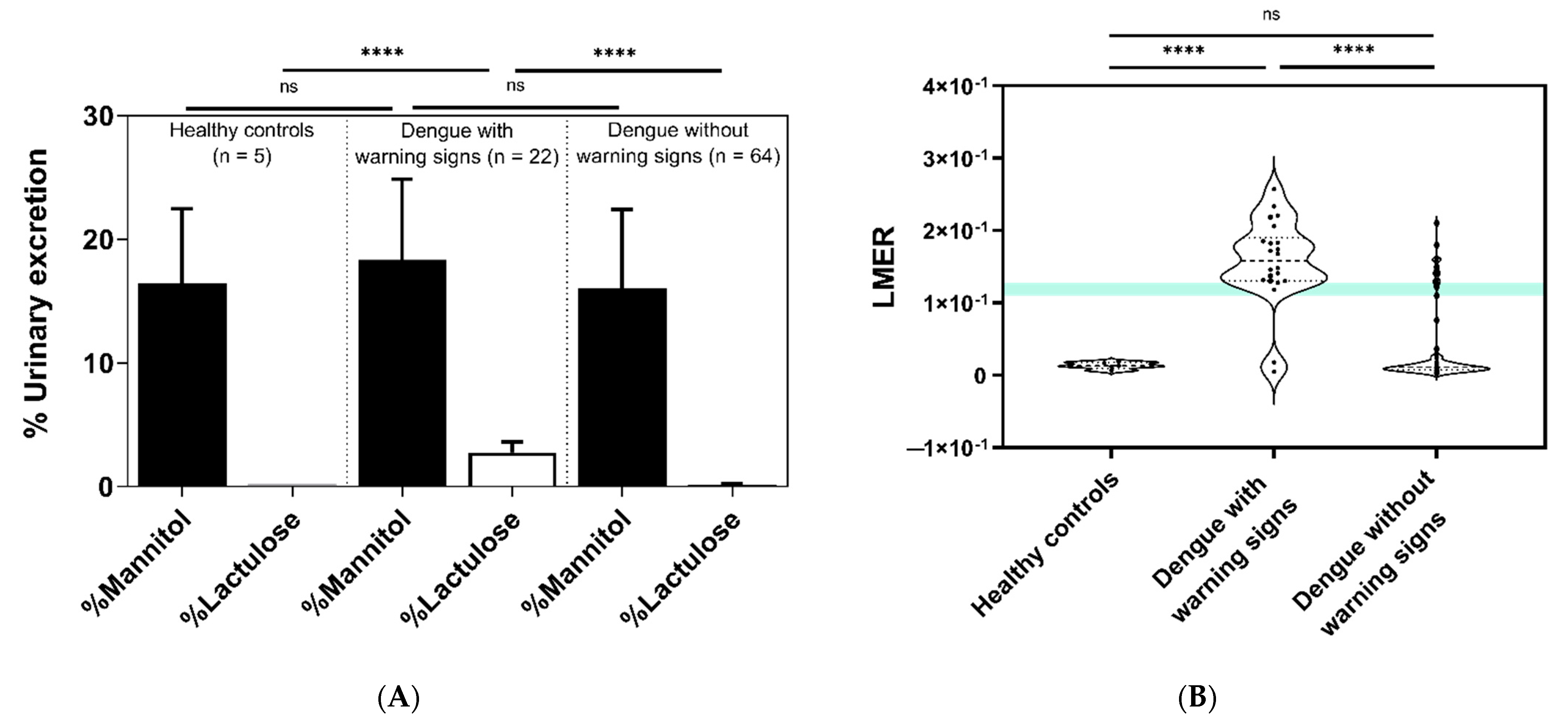
3.2. Comparisons of Intestinal Permeability among Groups Using the Lactulose-to-Mannitol Excretion Ratio (LMER)
3.3. The Progression to Severe Dengue Infection as Stratified by the Lactulose-to-Mannitol Excretion Ratio (LMER) Test and Warning Signs of Dengue Infection
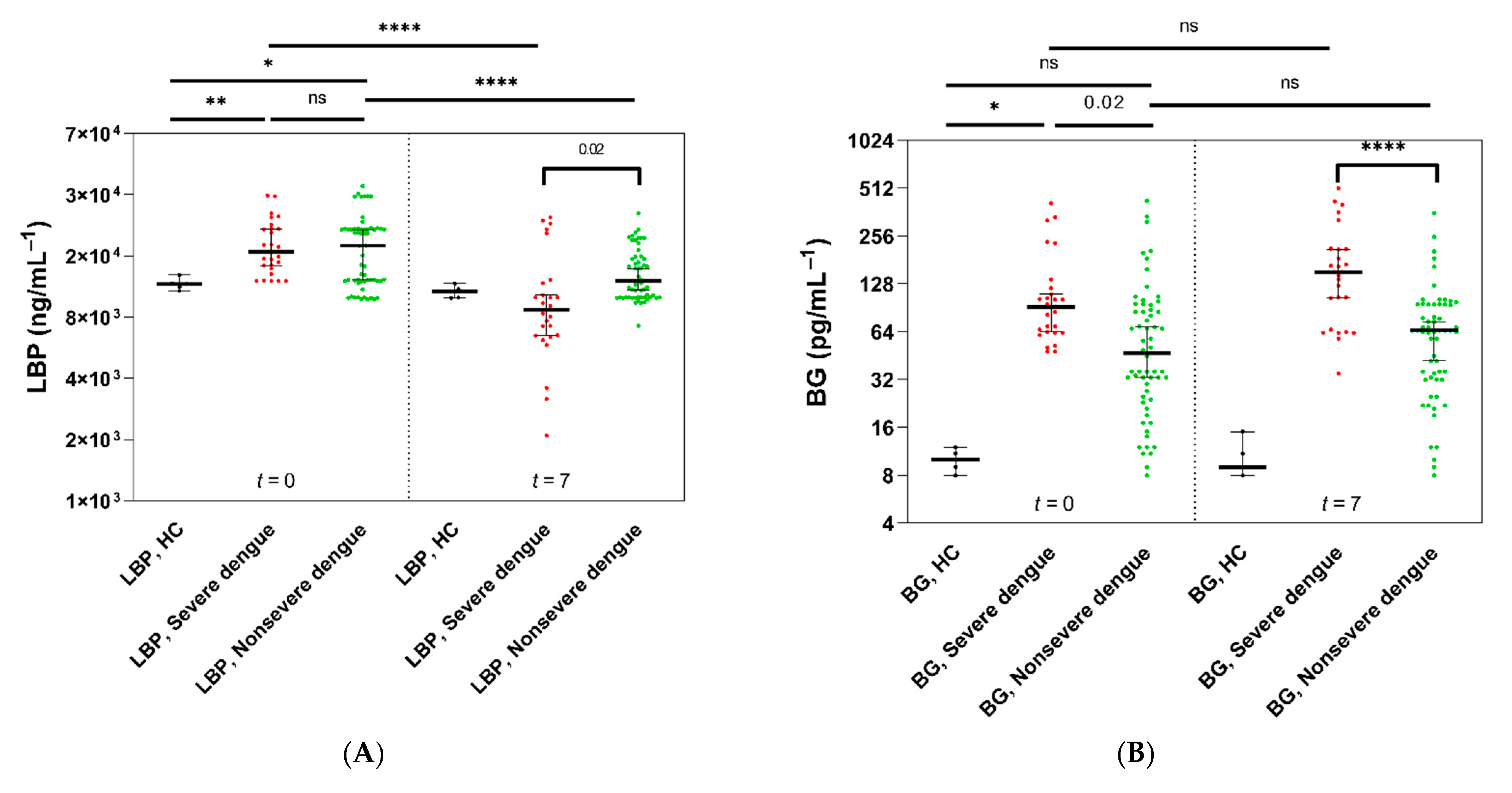
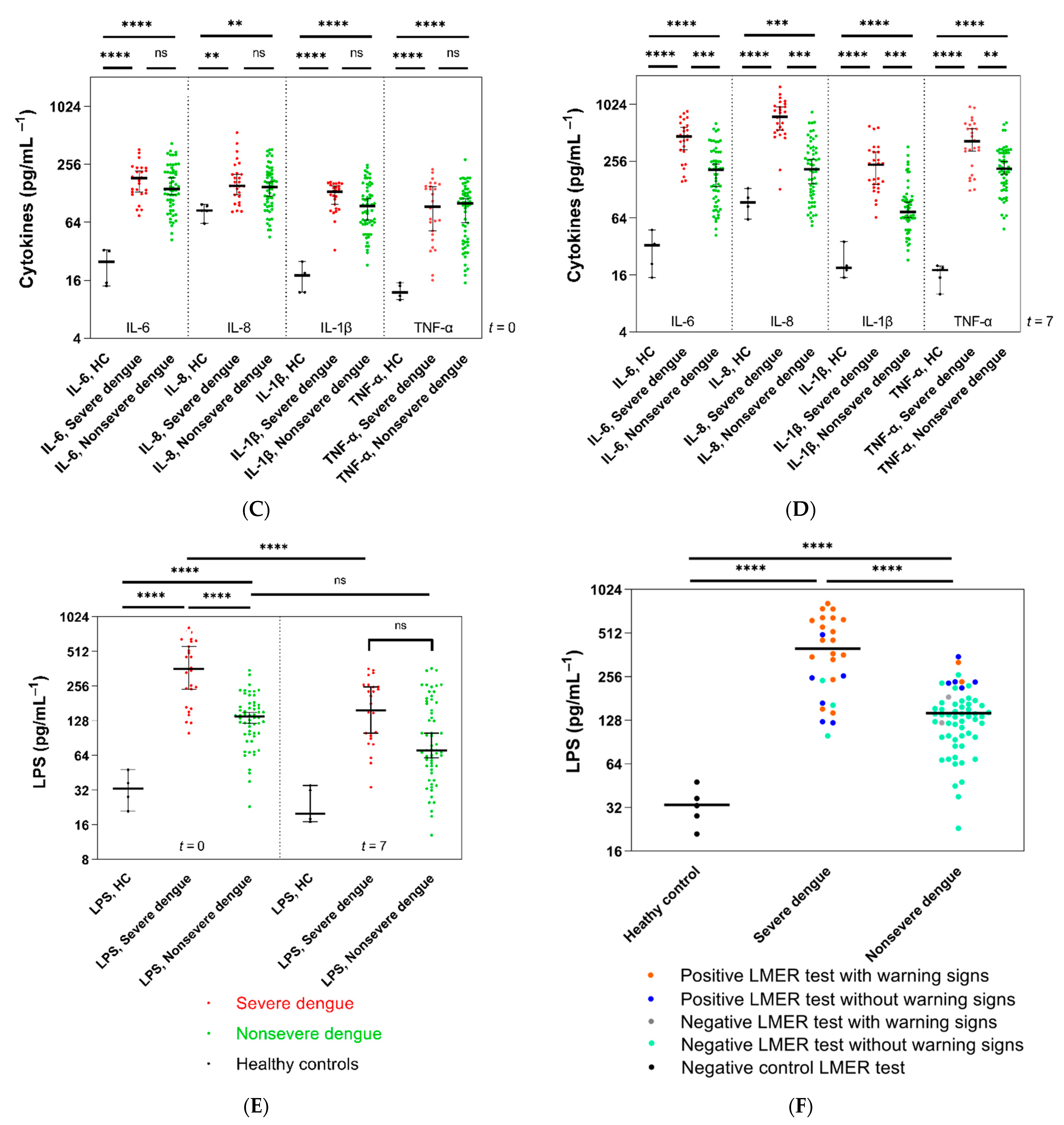
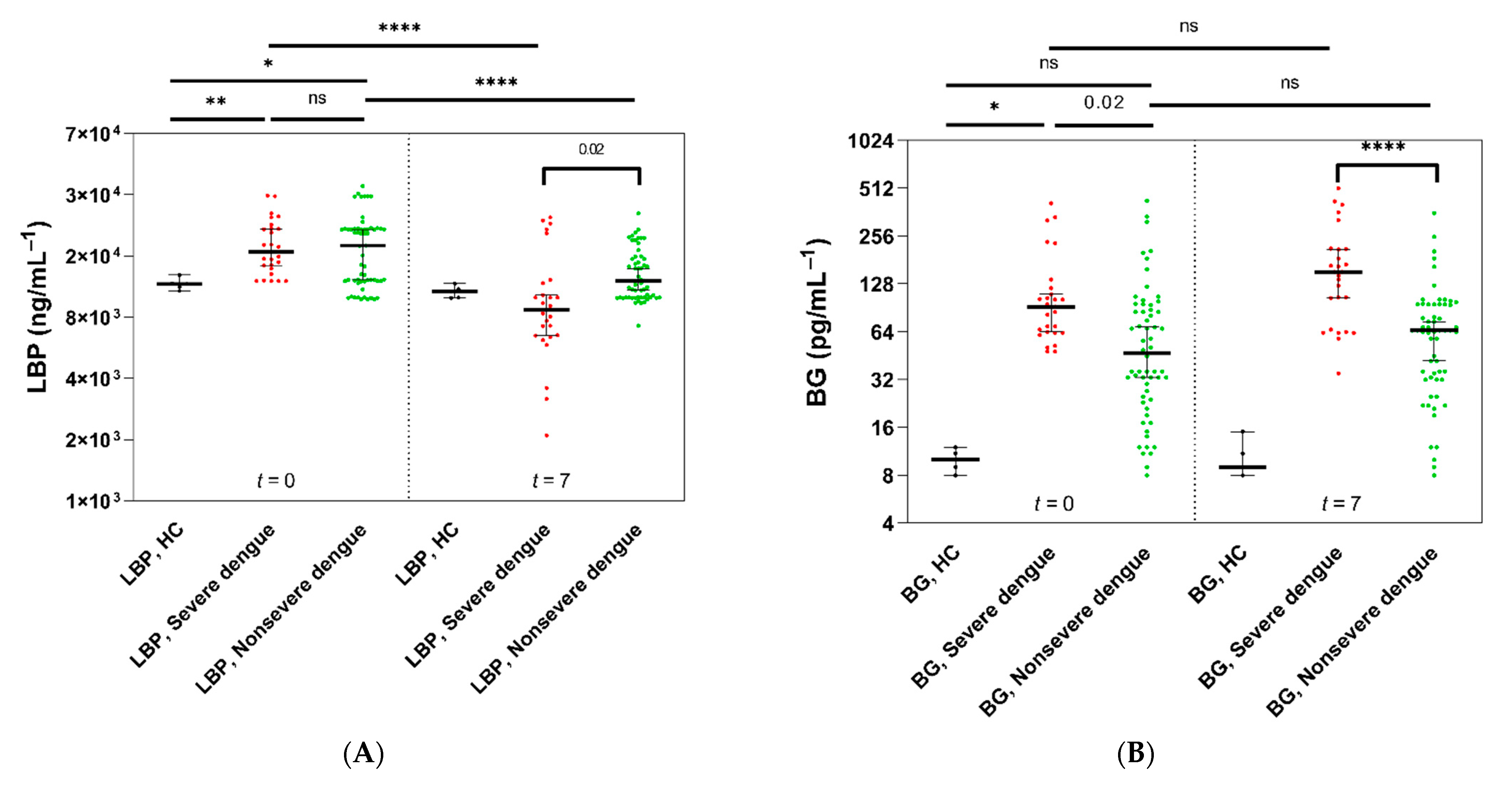
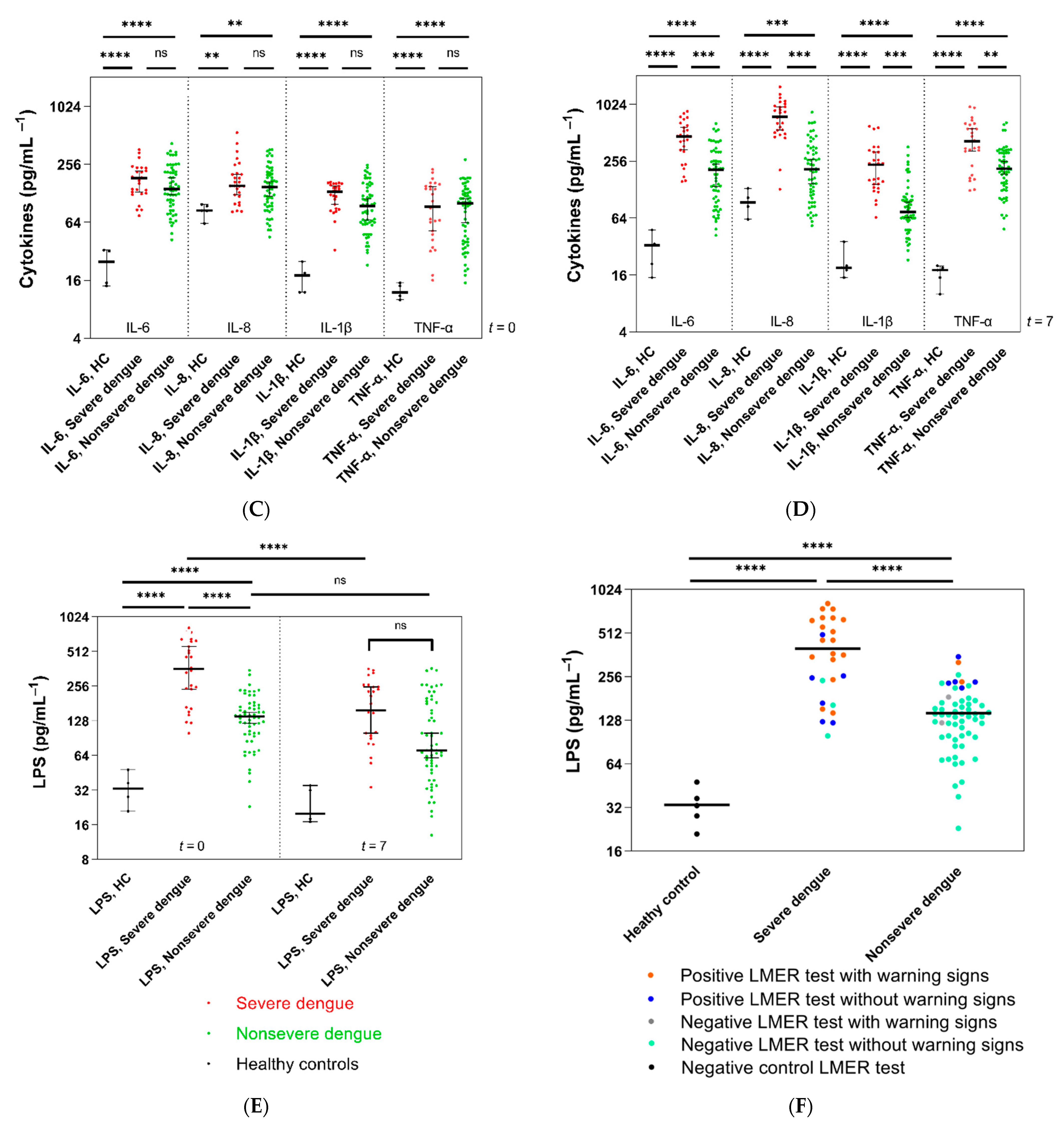
3.4. Intestinal Damage, Lipopolysaccharides (LPS), and Inflammatory Markers
3.5. Increased Lipopolysaccharides (LPS) and (1→3)-β-D-Glucan (BG) in Serum in Parallel with a Positive LMER Test in Patients with Dengue
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 10 August 2021).
- Cattarino, L.; Rodriguez-Barraquer, I.; Imai, N.; Cummings, D.; Ferguson, N.M. Mapping global variation in dengue trans-mission intensity. Sci. Transl. Med. 2020, 12, eaax4144. [Google Scholar] [CrossRef] [PubMed]
- Messina, J.P.; Brady, O.J.; Golding, N.; Kraemer, M.U.G.; Wint, G.R.W.; Ray, S.E.; Pigott, D.M.; Shearer, F.M.; Johnson, K.; Earl, L.; et al. The current and future global distribution and population at risk of dengue. Nat. Microbiol. 2019, 4, 1508–1515. [Google Scholar] [CrossRef]
- World Health Organization. Dengue and Severe Dengue. Available online: https://www.who.int/en/news-room/fact-sheets/detail/dengue-and-severe-dengue (accessed on 11 August 2021).
- Zheng, B.; Wang, H.; Cui, G.; Guo, Q.; Si, L.; Yan, H.; Fang, D.; Jiang, L.; Jiang, Z.; Zhou, J. ERG-Associated lncRNA (ERGAL) Promotes the Stability and Integrity of Vascular Endothelial Barrier During Dengue Viral Infection via Interaction With miR-183-5p. Front. Cell. Infect. Microbiol. 2020, 10, 477. [Google Scholar] [CrossRef]
- Douglas, K.O.; Samuels, T.A.; Hilaire, M.G.-S. Serum LPS Associated with Hantavirus and Dengue Disease Severity in Barbados. Viruses 2019, 11, 838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shyamali, N.L.A.; Mahapatuna, S.D.; Gomes, L.; Wijewickrama, A.; Ogg, G.S.; Malavige, G.N. Risk Factors for Elevated Serum Lipopolysaccharide in Acute Dengue and Association with Clinical Disease Severity. Trop. Med. Infect. Dis. 2020, 5, 170. [Google Scholar] [CrossRef]
- van de Weg, C.A.; Koraka, P.; van Gorp, E.C.; Mairuhu, A.T.; Supriatna, M.; Soemantri, A.; van de Vijver, D.A.; Osterhaus, A.D.; Martina, B.E. Lipopolysaccharide levels are elevated in dengue virus infected patients and correlate with disease severity. J. Clin. Virol. 2012, 53, 38–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van De Weg, C.A.M.; Pannuti, C.S.; De Araújo, E.S.A.; Ham, H.-J.V.D.; Andeweg, A.C.; Boas, L.S.V.; Felix, A.C.; Carvalho, K.; De Matos, A.M.; Levi, J.E.; et al. Microbial Translocation Is Associated with Extensive Immune Activation in Dengue Virus Infected Patients with Severe Disease. PLoS Negl. Trop. Dis. 2013, 7, e2236. [Google Scholar] [CrossRef]
- Rossol, M.; Heine, H.; Meusch, U.; Quandt, D.; Klein, C.; Sweet, M.; Hauschildt, S. LPS-induced Cytokine Production in Human Monocytes and Macrophages. Crit. Rev. Immunol. 2011, 31, 379–446. [Google Scholar] [CrossRef]
- Kamaladasa, A.; Gomes, L.; Jeewandara, C.; Shyamali, N.; Ogg, G.S.; Malavige, G.N. Lipopolysaccharide acts synergistically with the dengue virus to induce monocyte production of platelet activating factor and other inflammatory mediators. Antivir. Res. 2016, 133, 183–190. [Google Scholar] [CrossRef] [Green Version]
- Issara-Amphorn, J.; Surawut, S.; Worasilchai, N.; Thim-Uam, A.; Finkelman, M.; Chindamporn, A.; Palaga, T.; Hirankarn, N.; Pisitkun, P.; Leelahavanichkul, A. The Synergy of Endotoxin and (1→3)-β-D-Glucan, from Gut Translocation, Worsens Sepsis Severity in a Lupus Model of Fc Gamma Receptor IIb-Deficient Mice. J. Innate Immun. 2018, 10, 189–201. [Google Scholar] [CrossRef]
- Panpetch, W.; Chancharoenthana, W.; Bootdee, K.; Nilgate, S.; Finkelman, M.; Tumwasorn, S.; Leelahavanichkul, A. Lacto-bacillus rhamnosus L34 attenuates gut translocation-induced bacterial sepsis in murine models of leaky gut. Infect. Immun. 2017, 86, e00700-17. [Google Scholar]
- Chopyk, D.M.; Grakoui, A. Contribution of the Intestinal Microbiome and Gut Barrier to Hepatic Disorders. Gastroenterology 2020, 159, 849–863. [Google Scholar] [CrossRef] [PubMed]
- Thim-Uam, A.; Surawut, S.; Issara-Amphorn, J.; Jaroonwitchawan, T.; Hiengrach, P.; Chatthanathon, P.; Wilantho, A.; Somboonna, N.; Palaga, T.; Pisitkun, P.; et al. Leaky-gut enhanced lupus progression in the Fc gamma re-ceptor-IIb deficient and pristane-induced mouse models of lupus. Sci. Rep. 2020, 10, 777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uil, J.J.; Van Elburg, R.M.; Van Overbeek, F.M.; Mulder, C.J.; Vanberge-Henegouwen, G.P.; Heymans, H.S. Clinical implications of the sugar absorption test: Intestinal permeability test to assess mucosal barrier function. Scand. J. Gastroenterol. Suppl. 1997, 223, 70–78. [Google Scholar] [PubMed]
- World Health Organization. Dengue: Guidelines for Diagnosis, Treatment, Prevention and Control. New Edition; World Health Organization: Geneva, Switzerland, 2009; pp. 1–147. [Google Scholar]
- Johnston, S.D.; Smye, M.; Watson, R.G.; McMillan, S.A.; Trimble, E.R.; Love, A.H. Lactulose-mannitol intestinal permeability test: A useful screening test for adult coeliac disease. Ann. Clin. Biochem. 2000, 37, 512–519. [Google Scholar] [PubMed] [Green Version]
- Mishra, A.; Makharia, G.K. Techniques of Functional and Motility Test: How to Perform and Interpret Intestinal Permeability. J. Neurogastroenterol. Motil. 2012, 18, 443–447. [Google Scholar] [CrossRef] [Green Version]
- Romaschin, A.D.; Harris, D.M.; Ribeiro, M.B.; Paice, J.; Foster, D.M.; Walker, P.M.; Marshall, J.C. A rapid assay of endotoxin in whole blood using autologous neutrophil dependent chemiluminescence. J. Immunol. Methods 1998, 212, 169–185. [Google Scholar] [CrossRef]
- Marshall, J.C.; Foster, D.M.; Vincent, J.-L.; Cook, D.J.; Cohen, J.; Dellinger, R.P.; Opal, S.M.; Abraham, E.H.; Brett, S.J.; Smith, T.J.; et al. Diagnostic and Prognostic Implications of Endotoxemia in Critical Illness: Results of the MEDIC Study. J. Infect. Dis. 2004, 190, 527–534. [Google Scholar] [CrossRef] [Green Version]
- Scaldaferri, F.; Lopetuso, L.R.; Petito, V.; Cufino, V.; Bilotta, M.; Arena, V.; Stigliano, E.; Maulucci, G.; Papi, M.; Emiliana, C.M.; et al. Gelatin tannate ameliorates acute colitis in mice by reinforcing mucus layer and modulating gut microbiota composition: Emerging role for ‘gut barrier protectors’ in IBD? United Eur. Gastroenterol. J. 2014, 2, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Yousef, M.; Pichyangkura, R.; Soodvilai, S.; Chatsudthipong, V.; Muanprasat, C. Chitosan oligosaccharide as potential therapy of inflammatory bowel disease: Therapeutic efficacy and possible mechanisms of action. Pharmacol. Res. 2012, 66, 66–79. [Google Scholar] [CrossRef]
- Ellis, M.; Al-Ramadi, B.; Finkelman, M.; Hedstrom, U.; Kristensen, J.; Ali-Zadeh, H.; Klingspor, L. Assessment of the clinical utility of serial β-d-glucan concentrations in patients with persistent neutropenic fever. J. Med Microbiol. 2008, 57, 287–295. [Google Scholar] [CrossRef]
- Di Lorenzo, F.; De Castro, C.; Silipo, A.; Molinaro, A. Lipopolysaccharide structures of Gram-negative populations in the gut mi-crobiota and effects on host interactions. FEMS. Microbiol. Rev. 2019, 43, 257–272. [Google Scholar] [CrossRef]
- Marshall, J.C. Lipopolysaccharide: An endotoxin or an exogenous hormone? Clin. Infect. Dis. 2005, 41, S470–S480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teshima, C.W.; Goodman, K.J.; El-Kalla, M.; Turk, S.; El-Matary, W.; Valcheva, R.; Danchak, R.; Gordon, M.; Ho, P.; Mullins, A.; et al. Increased Intestinal Permeability in Relatives of Patients With Crohn’s Disease Is Not Associated With Small Bowel Ulcerations. Clin. Gastroenterol. Hepatol. 2017, 15, 1413–1418.e1. [Google Scholar] [CrossRef] [PubMed]
- Power, N.; Turpin, W.; Espin-Garcia, O.; Smith, M.I.; Croitoru, K. Serum zonulin measured by commercial kit fails to correlate with physiologic measures of altered gut permeability in first degree relatives of Crohn’s disease patients. Front. Physiol. 2021, 12, 645303. [Google Scholar] [CrossRef] [PubMed]
- Turpin, W.; Lee, S.H.; Raygoza Garay, J.A.; Madsen, K.L.; Meddings, J.B.; Bedrani, L.; Power, N.; Espin-Garcia, O.; Xu, W.; Smith, M.I.; et al. Increased intestinal permeability is associated with later development of Crohn’s disease. Gastroenterology 2020, 159, 2092.e2095–2100.e2095. [Google Scholar] [CrossRef]
- Kevans, D.; Turpin, W.; Madsen, K.; Meddings, J.; Shestopaloff, K.; Xu, W.; Moreno-Hagelsieb, G.; Griffiths, A.; Silverberg, M.S.; Paterson, A.; et al. Determinants of intestinal permeability in healthy first-degree relatives of indi-viduals with Crohn’s disease. Inflamm. Bowel Dis. 2015, 21, 879–887. [Google Scholar] [CrossRef]
- Che, P.; Tang, H.; Li, Q. The interaction between claudin-1 and dengue viral prM/M protein for its entry. Virology 2013, 446, 303–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanlaya, R.; Pattanakitsakul, S.N.; Sinchaikul, S.; Chen, S.T.; Thongboonkerd, V. Alterations in actin cytoskeletal assembly and junctional protein complexes in human endothelial cells induced by dengue virus infection and mimicry of leukocyte tran-sendothelial migration. J. Proteome Res. 2009, 8, 2551–2562. [Google Scholar] [CrossRef]
- Leelahavanichkul, A.; Worasilchai, N.; Wannalerdsakun, S.; Jutivorakool, K.; Somparn, P.; Issara-Amphorn, J.; Tachaboon, S.; Srisawat, N.; Finkelman, M.; Chindamporn, A. Gastrointestinal Leakage Detected by Serum (1→3)-β-D-Glucan in Mouse Models and a Pilot Study in Patients with Sepsis. Shock 2016, 46, 506–518. [Google Scholar] [CrossRef] [PubMed]
- Ramendra, R.; Isnard, S.; Mehraj, V.; Chen, J.; Zhang, Y.; Finkelman, M.; Routy, J.P. Circulating LPS and (1→3)-β-D-glucan: A Folie à Deux contributing to HIV-associated immune activation. Front. Immunol. 2019, 10, 465. [Google Scholar] [CrossRef]
- Legentil, L.; Paris, F.; Ballet, C.; Trouvelot, S.; Daire, X.; Vetvicka, V.; Ferrières, V. Molecular interactions of β-(1→3)-glucans with their receptors. Molecules 2015, 20, 9745–9766. [Google Scholar] [CrossRef]
- Finkelman, M.A. Specificity Influences in (1→3)-β-d-Glucan-Supported Diagnosis of Invasive Fungal Disease. J. Fungi 2021, 7, 14. [Google Scholar] [CrossRef] [PubMed]
- Meng, L.; Song, Z.; Liu, A.; Dahmen, U.; Yang, X.; Fang, H. Effects of Lipopolysaccharide-Binding Protein (LBP) Single Nucleotide Polymorphism (SNP) in Infections, Inflammatory Diseases, Metabolic Disorders and Cancers. Front. Immunol. 2021, 12, 2469. [Google Scholar] [CrossRef] [PubMed]
- Blairon, L.; Wittebole, X.; Laterre, P. Lipopolysaccharide-Binding Protein Serum Levels in Patients with Severe Sepsis Due to Gram-Positive and Fungal Infections. J. Infect. Dis. 2003, 187, 287–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prucha, M.; Herold, I.; Zazula, R.; Dubska, L.; Dostal, M.; Hildebrand, T.; Hyanek, J. Significance of lipopolysaccharide-binding protein (an acute phase protein) in monitoring critically ill patients. Crit. Care 2003, 7, R154–R159. [Google Scholar] [CrossRef] [Green Version]
- Ghosh, S.S.; Wang, J.; Yannie, P.J.; Ghosh, S. Intestinal barrier dysfunction, LPS translocation, and disease development. J. Endocr. Soc. 2020, 4, bvz039. [Google Scholar] [CrossRef] [Green Version]
- Pålsson-McDermott, E.M.; O’Neill, L.A. Signal transduction by the lipopolysaccharide receptor, Toll-like receptor-4. Immunology 2004, 113, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Marshall, J.C.; Walker, P.M.; Foster, D.M.; Harris, D.; Ribeiro, M.; Paice, J.; Romaschin, A.D.; Derzko, A.N. Measurement of endotoxin activity in critically ill patients using whole blood neutrophil dependent chemiluminescence. Crit. Care 2002, 6, 342–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rowe, E.K.; Leo, Y.S.; Wong, J.G.; Thein, T.L.; Gan, V.C.; Lee, L.K.; Lye, D.C. Challenges in dengue fever in the elderly: Atypical presentation and risk of severe dengue and hospital-acquired infection. PLoS. Negl. Trop. Dis. 2014, 8, e2777. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Group (n = 5) | Dengue with Warning Signs (n = 22) | Dengue without Warning Signs (n = 64) | p Value 1 | |
|---|---|---|---|---|
| Age, years | 36.4 ± 8.2 | 41.4 ± 10.6 | 40.1 ± 9.8 | 0.60 |
| Female, n (%) | 3 (60.0) | 16 (72.7) | 44 (68.8) | 0.73 |
| Day of illness at enrollment | 5.2 ± 0.4 | 3.4 ± 0.5 | <0.0001 | |
| NS1 positive, n (%) | 22 (100.0) | 64 (100.0) | - | |
| PCR positive, n (%) | 22 (100.0) | 52 (81.3) | 0.03 | |
| Serotype DENV-1 | 1 (4.5) | 22 (42.3) | 0.001 | |
| Serotype DENV-2 | 15 (68.2) | 20 (38.5) | 0.02 | |
| Serotype DENV-3 | 0 (0) | 0 (0) | - | |
| Serotype DENV-4 | 6 (27.3) | 10 (19.2) | 0.43 | |
| Comorbidities, n (%) | 5 (22.7) | 11 (17.2) | 0.57 | |
| Diabetes | 1 (4.5) | 3 (4.7) | 0.97 | |
| Hypertension | 5 (22.7) | 10 (15.6) | 0.45 | |
| Symptoms, n (%) | ||||
| Fever | 22 (100.0) | 64 (100.0) | - | |
| Anorexia | 22 (100.0) | 55 (85.9) | 0.06 | |
| Nausea | 22 (100.0) | 41 (64.1) | 0.001 | |
| Vomiting | 12 (54.5) | 0 (0) | <0.0001 | |
| Abdominal pain | 19 (86.4) | 0 (0) | <0.0001 | |
| Diarrhea | 7 (31.8) | 0 (0) | <0.0001 | |
| Myalgia | 22 (100.0) | 14 (21.9) | <0.0001 | |
| Rash | 11 (50.0) | 16 (25.0) | 0.03 | |
| Mucosal bleeding | 7 (31.8) | 0 (0) | <0.0001 | |
| Clinical fluid accumulation | 5 (22.7) | 0 (0) | 0.0001 | |
| Hemoglobin (g/dL) | 14.6 ± 0.9 | 13.3 ± 1.1 | <0.0001 | |
| Hematocrit (%) | 43.1 ± 2.2 | 40.2 ± 0.7 | <0.0001 | |
| White blood cell count (×109/L) | 3.83 ± 1.4 | 5.28 ± 2.1 | 0.003 | |
| Platelet count (×109/L) | 93.2 ± 11.6 | 121.2 ± 14.5 | <0.0001 | |
| Albumin (g/L) | 40.8 ± 1.5 | 41.8 ± 2.2 | 0.05 | |
| Aspartate transaminase (AST) (U/L) | 134.5 ± 16.2 | 68.8 ± 10.7 | <0.0001 | |
| Alanine transaminase (ALT) (U/L) | 50.1 ± 6.9 | 41.9 ± 10.4 | 0.001 | |
| Positive cases of bacterial isolation from blood, n (%) 2 | 0 (0) | 0 (0) | - | |
| LMER, median (range) | 0.013 (0.01) | 0.158 (0.25) | 0.011 (0.21) | <0.0001 |
| Endotoxins (pg/mL) | 33.4 ± 10.1 | 332.8 ± 263.2 | 103.4 ± 66.3 | <0.0001 |
| Lipopolysaccharide-binding protein (LBP) (ng/mL) | 10,070 ± 109.6 | 15,550 ± 4916.4 | 16,336 ± 7246.8 | 0.64 |
| (1→3)-β-D-glucan (BG) (pg/mL) | 10.0 ± 1.6 | 103.0 ± 96.9 | 53.8 ± 33.1 | 0.0007 |
| IL-6 (pg/mL) | 24.2 ± 10.8 | 408.0 ± 203.5 | 202.7 ± 146.3 | <0.0001 |
| IL-8 (pg/mL) | 78.6 ± 15.7 | 772.5 ± 330.5 | 192.3 ± 109.3 | <0.0001 |
| IL-1β (pg/mL) | 18.6 ± 8.3 | 215.4 ± 147.3 | 78.8 ± 68.0 | <0.0001 |
| TNF-α (pg/mL) | 14.4 ± 4.0 | 342.8 ± 235.4 | 206.5 ± 130.5 | 0.001 |
| Febrile Phase | Critical Phase | |||
|---|---|---|---|---|
| Dengue with Warning Signs (n = 2) | Dengue without Warning Signs (n = 46) | Dengue with Warning Signs (n = 20) | Dengue without Warning Signs (n = 18) | |
| Positive LMER test, n (%) | 2 (100.0) | 6 (13.0) | 18 (90.0) | 5 (27.8) |
| Negative LMER test, n (%) | 0 (0) | 40 (87.0) | 2 (10.0) | 13 (72.2) |
| For Severe Dengue Infection Prediction | |||||
|---|---|---|---|---|---|
| Cutoff | Sensitivity (%) | 95% CI 1 | Specificity (%) | 95% CI | Likelihood Ratio |
| LMER | |||||
| 0.1382 | 62.5 | 43–79% | 42.9 | 16–75% | 1.10 |
| 0.1401 | 62.5 | 43–79% | 57.1 | 25–84% | 1.46 |
| 0.1420 | 58.3 | 39–76% | 57.1 | 25–84% | 1.36 |
| 0.1444 | 58.3 | 39–76% | 71.4 | 36–95% | 2.04 |
| 0.1470 | 54.2 | 35–72% | 71.4 | 36–95% | 1.90 |
| 0.1580 | 50.0 | 31–69% | 71.4 | 36–95% | 1.75 |
| 0.1698 | 45.8 | 28–65% | 71.4 | 36–95% | 1.60 |
| LPS (pg/mL) | |||||
| 233.0 | 74.1 | 55–87% | 89.8 | 80–95% | 7.28 |
| 235.5 | 74.1 | 55–87% | 91.5 | 82–96% | 8.74 |
| 238.5 | 74.1 | 55–87% | 94.9 | 86–99% | 14.57 |
| 242.5 | 70.4 | 52–84% | 94.9 | 86–99% | 13.84 |
| 247.5 | 66.7 | 48–81% | 94.9 | 86–99% | 13.11 |
| 255.0 | 63.0 | 44–78% | 94.9 | 86–99% | 12.38 |
| 261.5 | 59.3 | 41–75% | 94.9 | 86–99% | 11.65 |
| BG (pg/mL) | |||||
| 50.0 | 93.0 | 77–99% | 51.7 | 39–64% | 1.92 |
| 51.5 | 88.9 | 72–96% | 53.3 | 41–65% | 1.91 |
| 54.0 | 85.2 | 68–94% | 53.3 | 41–65% | 1.83 |
| 57.0 | 85.2 | 68–94% | 55.0 | 42–67% | 1.90 |
| 59.5 | 85.2 | 68–94% | 57.0 | 44–68% | 1.97 |
| 62.0 | 81.4 | 63–92% | 57.0 | 44–68% | 1.88 |
| 63.5 | 74.1 | 55–87% | 57.0 | 44–68% | 1.71 |
| For Severe Dengue Infection Diagnosis | |||||
| Cutoff | Sensitivity (%) | 95% CI | Specificity (%) | 95% CI | Likelihood Ratio |
| LPS (pg/mL) | |||||
| 128.5 | 63.0 | 44–78% | 66.1 | 53–77% | 1.86 |
| 132.5 | 63.0 | 44–78% | 67.8 | 55–78% | 1.96 |
| 142.5 | 63.0 | 44–78% | 69.5 | 57–80% | 2.06 |
| 149.5 | 63.0 | 44–78% | 71.2 | 57–80% | 2.19 |
| 151.0 | 59.3 | 41–75% | 71.2 | 57–80% | 2.06 |
| 155.0 | 55.6 | 37–72% | 71.2 | 57–80% | 1.93 |
| 169.0 | 48.2 | 31–66% | 72.9 | 60–83% | 1.78 |
| BG (pg/mL) | |||||
| 97.0 | 74.1 | 55–87% | 81.7 | 70–89% | 4.04 |
| 99.0 | 74.1 | 55–87% | 83.3 | 72–91% | 4.44 |
| 101.0 | 74.1 | 55–87% | 85.0 | 74–92% | 4.94 |
| 103.0 | 74.1 | 55–87% | 90.0 | 80–95% | 7.41 |
| 104.5 | 70.4 | 52–84% | 90.0 | 80–95% | 7.04 |
| 115.0 | 63.0 | 44–78% | 90.0 | 80–95% | 6.30 |
| 130.5 | 59.2 | 41–75% | 91.7 | 82–96% | 7.11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chancharoenthana, W.; Leelahavanichkul, A.; Ariyanon, W.; Vadcharavivad, S.; Phatcharophaswattanakul, S.; Kamolratanakul, S.; Leaungwutiwong, P.; Phumratanaprapin, W.; Wilairatana, P. Leaky Gut Syndrome Is Associated with Endotoxemia and Serum (1→3)-β-D-Glucan in Severe Dengue Infection. Microorganisms 2021, 9, 2390. https://doi.org/10.3390/microorganisms9112390
Chancharoenthana W, Leelahavanichkul A, Ariyanon W, Vadcharavivad S, Phatcharophaswattanakul S, Kamolratanakul S, Leaungwutiwong P, Phumratanaprapin W, Wilairatana P. Leaky Gut Syndrome Is Associated with Endotoxemia and Serum (1→3)-β-D-Glucan in Severe Dengue Infection. Microorganisms. 2021; 9(11):2390. https://doi.org/10.3390/microorganisms9112390
Chicago/Turabian StyleChancharoenthana, Wiwat, Asada Leelahavanichkul, Wassawon Ariyanon, Somratai Vadcharavivad, Suphasit Phatcharophaswattanakul, Supitcha Kamolratanakul, Pornsawan Leaungwutiwong, Weerapong Phumratanaprapin, and Polrat Wilairatana. 2021. "Leaky Gut Syndrome Is Associated with Endotoxemia and Serum (1→3)-β-D-Glucan in Severe Dengue Infection" Microorganisms 9, no. 11: 2390. https://doi.org/10.3390/microorganisms9112390
APA StyleChancharoenthana, W., Leelahavanichkul, A., Ariyanon, W., Vadcharavivad, S., Phatcharophaswattanakul, S., Kamolratanakul, S., Leaungwutiwong, P., Phumratanaprapin, W., & Wilairatana, P. (2021). Leaky Gut Syndrome Is Associated with Endotoxemia and Serum (1→3)-β-D-Glucan in Severe Dengue Infection. Microorganisms, 9(11), 2390. https://doi.org/10.3390/microorganisms9112390