Antibiotic-Loaded Hydrogel Coating to Reduce Early Postsurgical Infections in Aseptic Hip Revision Surgery: A Retrospective, Matched Case-Control Study

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
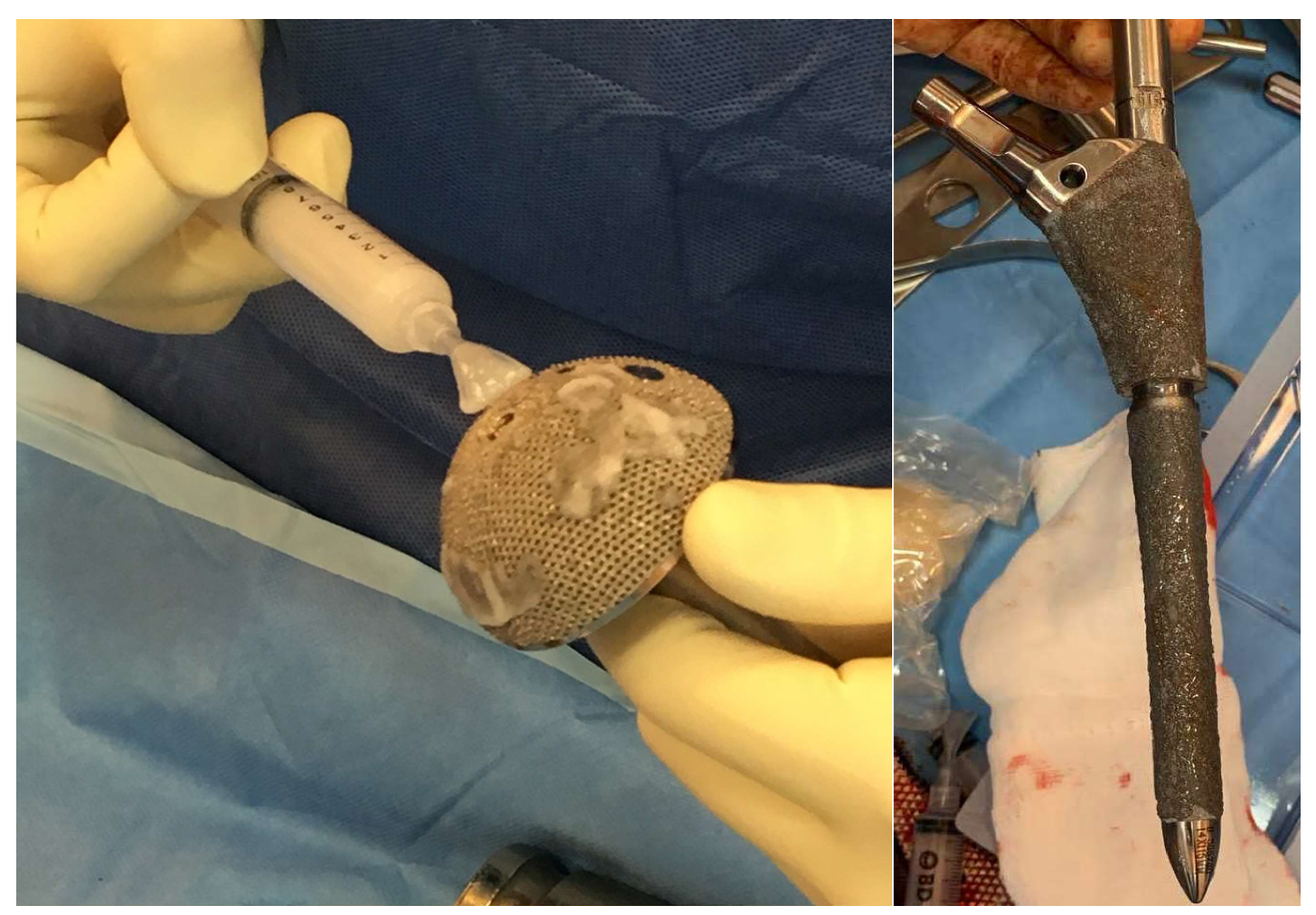
2.2. Surgical Treatment and Hydrogel Preparation
2.3. End-Points and Follow-Up
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Torre, M.; Carrani, E.; Luzi, I.; Laricchiuta, P.; Ceccarelli, S. (Eds.) Progetto Registro Italiano Artroprotesi. Quarto Report. Potenziare la Qualità dei Dati per Migliorare la Sicurezza dei Pazienti; Il Pensiero Scientifico Editore: Rome, Italy, 2017. [Google Scholar]
- Kenney, C.; Dick, S.; Lea, J.; Liu, J.; Ebraheim, N.A. A systematic review of the causes of failure of Revision Total Hip Arthroplasty. J. Orthop. 2019, 16, 393–395. [Google Scholar] [CrossRef] [PubMed]
- Badarudeen, S.; Shu, A.C.; Ong, K.L.; Baykal, D.; Lau, E.; Malkani, A.L. Complications After Revision Total Hip Arthroplasty in the Medicare Population. J. Arthroplast. 2017, 32, 1954–1958. [Google Scholar] [CrossRef] [PubMed]
- Romano, C.L.; Scarponi, S.; Gallazzi, E.; Romanò, D.; Drago, L. Antibacterial coating of implants in orthopaedics and trauma: A classification proposal in an evolving panorama. J. Orthop. Surg. Res. 2015, 10, 157. [Google Scholar] [CrossRef] [PubMed]
- Pitarresi, G.; Palumbo, F.S.; Calascibetta, F.; Fiorica, C.; Di Stefano, M.; Giammona, G. Medicated hydrogels of hyaluronic acid derivatives for use in orthopedic field. Int. J. Pharm. 2013, 449, 84–94. [Google Scholar] [CrossRef] [PubMed]
- Overstreet, D.; McLaren, A.; Calara, F.; Vernon, B.L.; McLemore, R. Local Gentamicin Delivery From Resorbable Viscous Hydrogels Is Therapeutically Effective. Clin. Orthop. Relat. Res. 2014, 473, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Harris, L.; Richards, R.G. Staphylococci and implant surfaces: A review. Injury 2006, 37, S3–S14. [Google Scholar] [CrossRef]
- Gasik, M.; Van Mellaert, L.; Pierron, D.; Braem, A.; Hofmans, D.; De Waelheyns, E.; Anné, J.; Harmand, M.F.; Vleugel, J. Reduction of Biofilm Infection Risks and Promotion of Osteointegration for Optimized Surfaces of Titanium Implants. Adv. Healthc. Mater. 2012, 1, 117–127. [Google Scholar] [CrossRef]
- Carlson, G.A.; Dragoo, J.L.; Samimi, B.; Bruckner, D.A.; Bernard, G.W.; Hedrick, M.; Benhaim, P. Bacteriostatic properties of biomatrices against common orthopaedic pathogens. Biochem. Biophys. Res. Commun. 2004, 321, 472–478. [Google Scholar] [CrossRef]
- Pirnazar, P.; Wolinsky, L.; Nachnani, S.; Haake, S.; Pilloni, A.; Bernard, G.W. Bacteriostatic Effects of Hyaluronic Acid. J. Periodontol. 1999, 70, 370–374. [Google Scholar] [CrossRef]
- Drago, L.; Boot, W.; Dimas, K.; Malizos, K.; Hänsch, G.M.; Stuyck, J.; Gawlitta, D.; Romano, C.L. Does implant coating with antibacterial-loaded hydrogel reduce bacterial colonization and biofilm formation in vitro? Clin. Orthop. Relat. Res. 2014, 472, 3311–3323. [Google Scholar] [CrossRef]
- Giavaresi, G.; Meani, E.; Sartori, M.; Ferrari, A.; Bellini, D.; Sacchetta, A.C.; Meraner, J.; Sambri, A.; Vocale, C.; Sambri, V.; et al. Efficacy of antibacterial-loaded coating in an in vivo model of acutely highly contaminated implant. Int. Orthop. 2013, 38, 1505–1512. [Google Scholar] [CrossRef] [PubMed]
- Tan, T.L.; Maltenfort, M.G.; Chen, A.F.; Shahi, A.; Higuera, C.A.; Siqueira, M.; Parvizi, J. Development and Evaluation of a Preoperative Risk Calculator for Periprosthetic Joint Infection Following Total Joint Arthroplasty. J. Bone Jt. Surg. 2018, 100, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Inacio, M.C.; Chen, Y.; Paxton, E.W.; Namba, R.S.; Kurtz, S.M.; Cafri, G. Statistics in Brief: An Introduction to the Use of Propensity Scores. Clin. Orthop. Relat. Res. 2015, 473, 2722–2726. [Google Scholar] [CrossRef] [PubMed]
- Tande, A.J.; Patel, R. Prosthetic joint infection. Clin. Microbiol. Rev. 2014, 27, 302–345. [Google Scholar] [CrossRef]
- Izakovicova, P.; Borens, O.; Trampuz, A. Periprosthetic joint infection: Current concepts and outlook. EFORT Open Rev. 2019, 4, 482–494. [Google Scholar] [CrossRef]
- Baeza, J.; Cury, M.B.; Fleischman, A.; Ferrando, A.; Fuertes, M.; Goswami, K.; Lidgren, L.; Linke, P.; Manrique, J.; Bs, G.S.M.; et al. General Assembly, Prevention, Local Antimicrobials: Proceedings of International Consensus on Orthopedic Infections. J. Arthroplast. 2019, 34, S75–S84. [Google Scholar] [CrossRef]
- Craig, W.A. Pharmacokinetic/pharmacodynamic parameters: Rationale for antibacterial dosing of mice and men. Clin. Infect. Dis. 1998, 26, 1–10. [Google Scholar] [CrossRef]
- Gunderson, B.W.; Ross, G.H.; Ibrahim, K.H.; Rotschafer, J.C. What Do We Really Know About Antibiotic Pharmacodynamics? Pharmacother. J. Hum. Pharmacol. Drug Ther. 2001, 21, 302S–318S. [Google Scholar] [CrossRef]
- Mouton, J.W.; Theuretzbacher, U.; Craig, W.A.; Tulkens, P.M.; Derendorf, H.; Cars, O. Tissue concentrations: Do we ever learn? J. Antimicrob. Chemother. 2007, 61, 235–237. [Google Scholar] [CrossRef]
- Romano, C.L.; Malizos, K.; Capuano, N.; Mezzoprete, R.; D’Arienzo, M.; Van Der Straeten, C.; Scarponi, S.; Drago, L. Does an Antibiotic-Loaded Hydrogel Coating Reduce Early Post-Surgical Infection After Joint Arthroplasty? J. Bone Jt. Infect. 2016, 1, 34–41. [Google Scholar] [CrossRef]
- Zagra, L.; Gallazzi, E.; Romanò, D.; Scarponi, S.; Romanò, C. Two-stage cementless hip revision for peri-prosthetic infection with an antibacterial hydrogel coating: Results of a comparative series. Int. Orthop. 2018, 43, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Capuano, N.; Logoluso, N.; Gallazzi, E.; Drago, L.; Romano, C.L. One-stage exchange with antibacterial hydrogel coated implants provides similar results to two-stage revision, without the coating, for the treatment of peri-prosthetic infection. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 3362–3367. [Google Scholar] [CrossRef] [PubMed]
- Malizos, K.N.; Blauth, M.; Danita, A.; Capuano, N.; Mezzoprete, R.; Logoluso, N.; Drago, L.; Romano, C.L. Fast-resorbable antibiotic-loaded hydrogel coating to reduce post-surgical infection after internal osteosynthesis: A multicenter randomized controlled trial. J. Orthop. Traumatol. 2017, 18, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Bini, S.A.; Chan, P.H.; Inacio, M.C.; Paxton, E.W.; Khatod, M. Antibiotic cement was associated with half the risk of re-revision in 1,154 aseptic revision total knee arthroplasties. Acta Orthop. 2015, 87, 55–59. [Google Scholar] [CrossRef] [PubMed]
- British Medical Association; Australian Medical Association. The Medical Journal of Australia. Australasian Medical Pub. Available online: https://www.researchgate.net/publication/8684538_The_Australian_Orthopedic_Association_National_Joint_Replacement_Registry (accessed on 9 July 2019).
- Cai, X.-Z.; Chen, X.-Z.; Yan, S.; Parvizi, J.; Saleh, K.; Mont, M. Efficacy of antibiotic-impregnated cement in total hip replacement. Acta Orthop. 2008, 79, 870–872. [Google Scholar] [CrossRef] [PubMed]
- Ensing, G.T.; van Horn, J.R.; van der Mei, H.C.; Busscher, H.J.; Neut, D. Copal bone cement is more effective in preventing biofilm formation than Palacos R-G. Clin. Orthop. Relat. Res. 2008, 466, 1492–1498. [Google Scholar] [CrossRef]
- Schmolders, J.; Hischebeth, G.T.; Friedrich, M.; Randau, T.M.; Wimmer, M.; Kohlhof, H.; Molitor, E.; Gravius, S. Evidence of MRSE on a gentamicin and vancomycin impregnated polymethyl-methacrylate (PMMA) bone cement spacer after two-stage exchange arthroplasty due to periprosthetic joint infection of the knee. BMC Infect. Dis. 2014, 14, 144. [Google Scholar] [CrossRef]
- Wafa, H.; Grimer, R.J.; Reddy, K.; Jeys, L.; Abudu, A.; Carter, S.; Tillman, R.M. Retrospective evaluation of the incidence of early periprosthetic infection with silver-treated endoprostheses in high-risk patients. Bone Jt. J. 2015, 97, 252–257. [Google Scholar] [CrossRef]
- Tsuchiya, H.; Shirai, T.; Nishida, H.; Murakami, H.; Kabata, T.; Yamamoto, N.; Watanabe, K.; Nakase, J. Innovative antimicrobial coating of titanium implants with iodine. J. Orthop. Sci. 2012, 17, 595–604. [Google Scholar] [CrossRef]
- Kallala, R.; Harris, W.E.; Ibrahim, M.; Dipane, M.; McPherson, E. Use of Stimulan absorbable calcium sulphate beads in revision lower limb arthroplasty. Bone Jt. Res. 2018, 7, 570–579. [Google Scholar] [CrossRef]
- Barrack, R.L.; Brumfield, C.S.; Rorabeck, C.H.; Cleland, D.; Myers, L. Heterotopic Ossification After Revision Total Knee Arthroplasty. Clin. Orthop. Relat. Res. 2002, 404, 208–213. [Google Scholar] [CrossRef] [PubMed]
- McPherson, F.E.; Dipane, B.M.; Sherif, S. Dissolvable Antibiotic Beads in Treatment of Periprosthetic Joint Infection and Revision Arthroplasty—The Use of Synthetic Pure Calcium Sulfate (Stimulan®) Impregnated with Vancomycin & Tobramycin. Reconstr. Rev. 2013, 3, 32–43. [Google Scholar]
- Ziran, B.H.; Smith, W.R.; Morgan, S.J. Use of Calcium-Based Demineralized Bone Matrix/Allograft for Nonunions and Posttraumatic Reconstruction of the Appendicular Skeleton: Preliminary Results and Complications. J. Trauma 2007, 63, 1324–1328. [Google Scholar] [CrossRef]
- Trentinaglia, M.T.; Van Der Straeten, C.; Morelli, I.; Logoluso, N.; Drago, L.; Romanò, C.L. Economic Evaluation of Antibacterial Coatings on Healthcare Costs in First Year Following Total Joint Arthroplasty. J. Arthroplast. 2018, 33, 1656–1662. [Google Scholar] [CrossRef] [PubMed]
- Schwarzkopf, R.; Baghoolizadeh, M. Conversion total hip arthroplasty: Primary or revision total hip arthroplasty. World J. Orthop. 2015, 6, 750–753. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Demographic Data | ALH | Controls | p Value |
|---|---|---|---|
| Age | 74.9 ± 11.5 | 75.9 ± 9.6 | 0.7973 |
| Sex (F) | 11 | 10 | 1 |
| BMI | 27.1 ± 5.1 | 24.9 ± 4.9 | 0.1801 |
| CCI | 4.4 ± 1.7 | 4.4 ± 2.2 | 1 |
| PJI risk score | 25.2 ± 16.1 | 22.6 ± 19.8 | 0.6795 |
| Operative time (min) | 168.2 ± 56.9 | 166.8 ± 42.4 | 0.9348 |
| ALH | Controls | p Value | |
|---|---|---|---|
| Periprosthetic Fracture | 5 | 7 | 0.7207 |
| Aseptic Loosening | 4 | 4 | 1 |
| Dislocation | 3 | 1 | 0.6012 |
| Wear | 1 | 2 | 1 |
| ARMD 1 | 0 | 1 | 1 |
| Fixation Failure | 4 | 2 | 0.6562 |
| Time-To-Failure (month) | 103.7 ± 108.3 | 112.1 ± 96.8 | 0.8150 |
| Surgical Intervention | ALH | Controls | p Value |
|---|---|---|---|
| Stem or shell revision | 5 | 9 | 0.2960 |
| Stem and shell revision | 1 | 0 | 1 |
| Mobile components revision | 1 | 2 | 1 |
| Osteosynthesis (only) | 5 | 4 | 1 |
| Conversion THA | 4 | 2 | 0.6562 |
| + Bone grafting | 3 | 1 | 0.6012 |
| Outcome | ALH | Controls | p Value |
|---|---|---|---|
| Total complications | 3 | 11 | 0.0134 |
| Infection | 0 | 6 | 0.0001 |
| Dislocation | 0 | 1 | 1 |
| Prolonged wound discharge | 2 | 1 | 1 |
| Nerve deficit | 0 | 1 | 1 |
| Systemics | 1 | 2 | 1 |
| Deceased | 1 | 4 | 0.3353 |
| Functional Outcome | ALH | Controls | p Value |
|---|---|---|---|
| HHS pre | 34.1 ± 29.8 | 38.4 ± 13.7 | 0.7291 |
| HHS post | 72.9 ± 12.9 | 57.6 ± 23.8 | 0.0687 |
| HOOS post | 73.6 ± 15.8 | 57.9 ± 26.3 | 0.0988 |
| Pz | Age | Sex | Diagnosis | Treatment | Prophylaxis | Time to Infection | Type of Infection | Infection Treatment | Complication | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 66 | M | Aseptic Loosening | Revision | Cefazolin 2000 mg | 2 d | MRSA | DAIR then TSE | Cerclage Breakage | Cured |
| 2 | 79 | F | ARMD | Revision | Vancomycin 1000 mg | 35 d | Klebsiella P. | DAIR then TSE | Sepsis, MOF | Death |
| 3 | 86 | F | PPFX | ORIF | Cefazolin 2000 mg | 5 m | E. Faecalis, MRSA | DAIR | Sepsis, MOF | Death |
| 4 | 86 | M | PPFX | ORIF | Cefazolin 2000 mg | 14 d | E. Coli, MSSA | DAIR | NONE | Cured |
| 5 | 86 | M | Wear | Revision | Cefazolin 2000 mg | 6 m | Culture Negative | DAIR | P.E. | Death |
| 6 | 72 | M | Fixation Failure | Conversion | Cefazolin 2000 mg | 4 m | MSSA | TSE | NONE | Cured |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Meo, D.; Calogero, V.; Are, L.; Cavallo, A.U.; Persiani, P.; Villani, C. Antibiotic-Loaded Hydrogel Coating to Reduce Early Postsurgical Infections in Aseptic Hip Revision Surgery: A Retrospective, Matched Case-Control Study. Microorganisms 2020, 8, 571. https://doi.org/10.3390/microorganisms8040571
De Meo D, Calogero V, Are L, Cavallo AU, Persiani P, Villani C. Antibiotic-Loaded Hydrogel Coating to Reduce Early Postsurgical Infections in Aseptic Hip Revision Surgery: A Retrospective, Matched Case-Control Study. Microorganisms. 2020; 8(4):571. https://doi.org/10.3390/microorganisms8040571
Chicago/Turabian StyleDe Meo, Daniele, Valeria Calogero, Lorenzo Are, Armando U. Cavallo, Pietro Persiani, and Ciro Villani. 2020. "Antibiotic-Loaded Hydrogel Coating to Reduce Early Postsurgical Infections in Aseptic Hip Revision Surgery: A Retrospective, Matched Case-Control Study" Microorganisms 8, no. 4: 571. https://doi.org/10.3390/microorganisms8040571
APA StyleDe Meo, D., Calogero, V., Are, L., Cavallo, A. U., Persiani, P., & Villani, C. (2020). Antibiotic-Loaded Hydrogel Coating to Reduce Early Postsurgical Infections in Aseptic Hip Revision Surgery: A Retrospective, Matched Case-Control Study. Microorganisms, 8(4), 571. https://doi.org/10.3390/microorganisms8040571