Predictive Values of Serum Chlamydia trachomatis TroA and HtrA IgG Antibodies as Markers of Persistent Infection in the Detection of Pelvic Adhesions and Tubal Occlusion

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
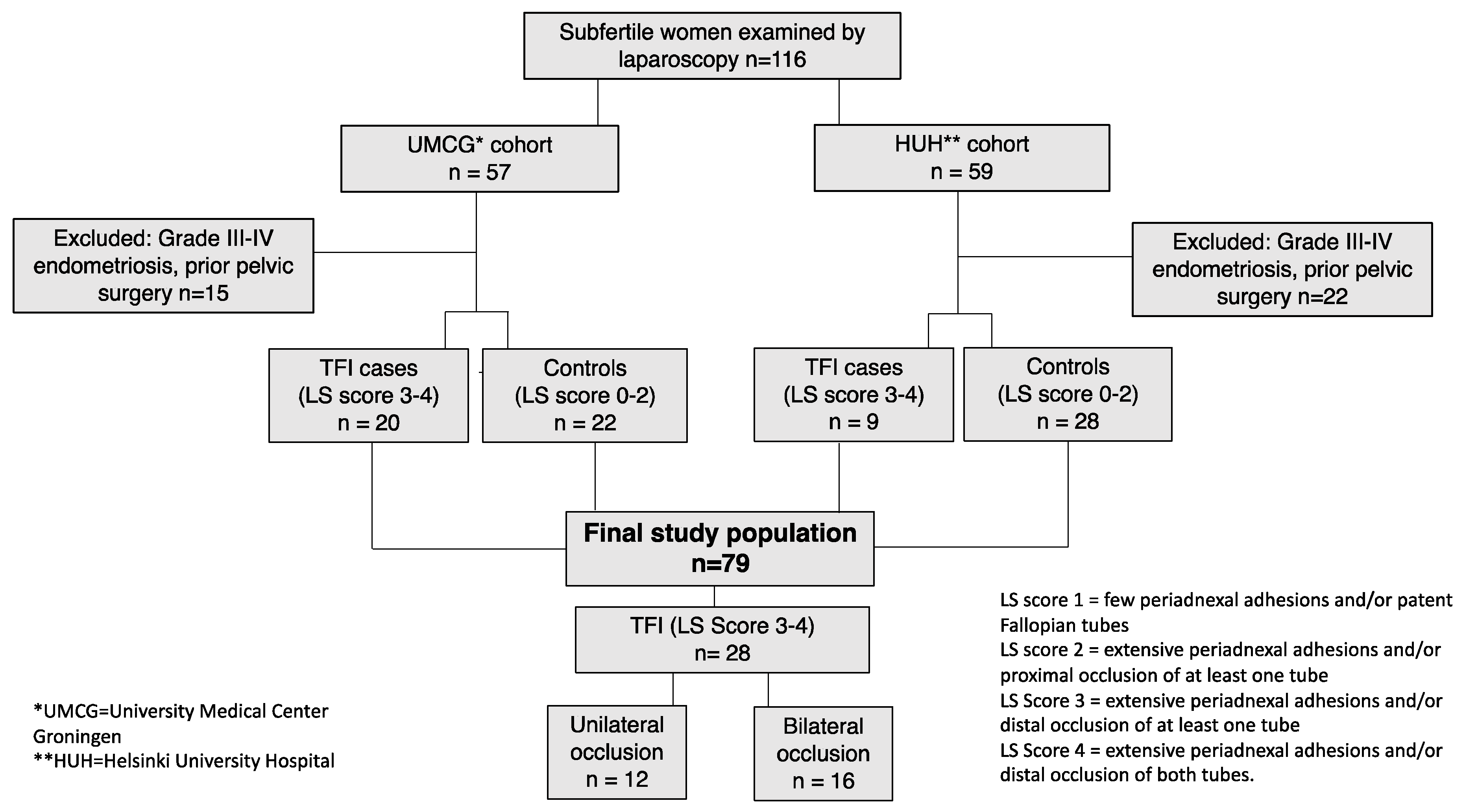
2.1. Study Population
2.2. Serological Methods
2.3. Statistical Methods
2.4. Ethical Approval
3. Results
3.1. Tubal Factor Infertility (TFI) in the Study Population
3.2. Serological Results
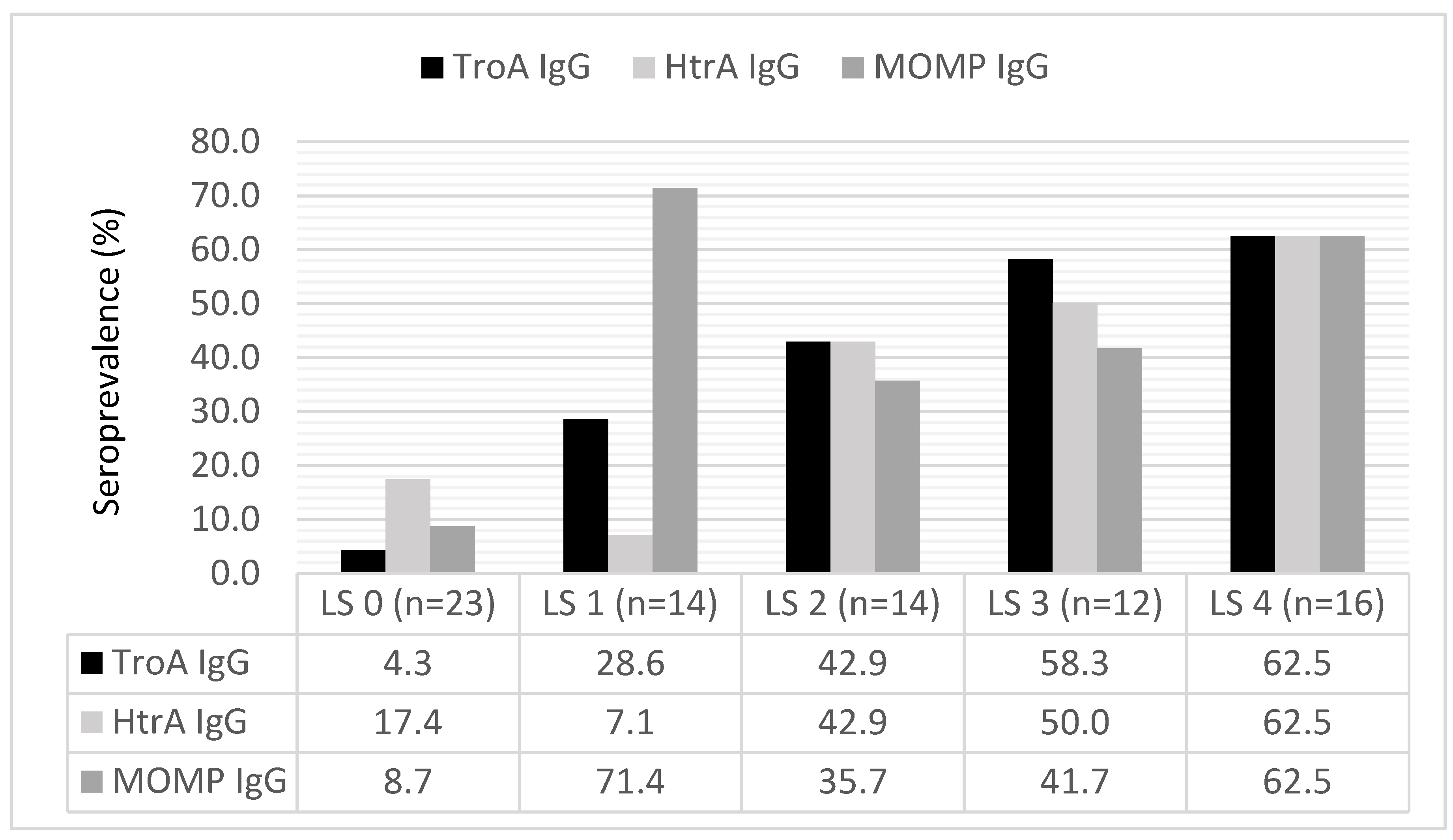
3.3. Serum Antibody Levels by the Severity of TFI
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Newman, L.; Rowley, J.; Vander Hoorn, S.; Wijesooriya, N.S.; Unemo, M.; Low, N.; Stevens, G.; Gottlieb, S.; Kiarie, J.; Temmerman, M. Global Estimates of the Prevalence and Incidence of Four Curable Sexually Transmitted Infections in 2012 Based on Systematic Review and Global Reporting. PLoS ONE 2015, 10, e0143304. [Google Scholar] [CrossRef] [PubMed]
- Geisler, W.M. Duration of untreated, uncomplicated Chlamydia trachomatis genital infection and factors associated with chlamydia resolution: A review of human studies. J. Infect. Dis. 2010, 201, S104–S113. [Google Scholar] [CrossRef] [PubMed]
- Paavonen, J.; Eggert-Kruse, W. Chlamydia trachomatis: Impact on human reproduction. Hum. Reprod. Update 1999, 5, 433–447. [Google Scholar] [CrossRef] [PubMed]
- Mardh, P.A. Tubal factor infertility, with special regard to chlamydial salpingitis. Curr. Opin. Infect. Dis. 2004, 17, 49–52. [Google Scholar] [CrossRef] [PubMed]
- National Collaborating Centre for Women’s and Children’s Health. National Institute for Health and Clinical Excellence: Guidance. In Fertility: Assessment and Treatment for People with Fertility Problems; Royal College of Obstetricians & Gynaecologists: London, UK, 2013. [Google Scholar]
- Maheux-Lacroix, S.; Boutin, A.; Moore, L.; Bergeron, M.E.; Bujold, E.; Laberge, P.; Lemyre, M.; Dodin, S. Hysterosalpingosonography for diagnosing tubal occlusion in subfertile women: a systematic review with meta-analysis. Hum. Reprod. 2014, 29, 953–963. [Google Scholar] [CrossRef]
- Den Hartog, J.E.; Land, J.A.; Stassen, F.R.; Kessels, A.G.; Bruggeman, C.A. Serological markers of persistent C. trachomatis infections in women with tubal factor subfertility. Hum. Reprod. 2005, 20, 986–990. [Google Scholar] [CrossRef]
- Tiitinen, A.; Surcel, H.M.; Halttunen, M.; Birkelund, S.; Bloigu, A.; Christiansen, G.; Koskela, P.; Morrison, S.G.; Morrison, R.P.; Paavonen, J. Chlamydia trachomatis and chlamydial heat shock protein 60-specific antibody and cell-mediated responses predict tubal factor infertility. Hum. Reprod. 2006, 21, 1533–1538. [Google Scholar] [CrossRef]
- Broeze, K.A.; Opmeer, B.C.; Coppus, S.F.; Van Geloven, N.; Alves, M.F.; Anestad, G.; Bhattacharya, S.; Allan, J.; Guerra-Infante, M.F.; Den Hartog, J.E.; et al. Chlamydia antibody testing and diagnosing tubal pathology in subfertile women: an individual patient data meta-analysis. Hum. Reprod. Update 2011, 17, 301–310. [Google Scholar] [CrossRef]
- Den Hartog, J.E.; Lardenoije, C.M.; Severens, J.L.; Land, J.A.; Evers, J.L.; Kessels, A.G. Screening strategies for tubal factor subfertility. Hum. Reprod. 2008, 23, 1840–1848. [Google Scholar] [CrossRef]
- Menon, S.; Timms, P.; Allan, J.A.; Alexander, K.; Rombauts, L.; Horner, P.; Keltz, M.; Hocking, J.; Huston, W.M. Human and Pathogen Factors Associated with Chlamydia trachomatis-Related Infertility in Women. Clin. Microbiol. Rev. 2015, 28, 969–985. [Google Scholar] [CrossRef]
- Huston, W.M.; Swedberg, J.E.; Harris, J.M.; Walsh, T.P.; Mathews, S.A.; Timms, P. The temperature activated HtrA protease from pathogen Chlamydia trachomatis acts as both a chaperone and protease at 37 degrees C. FEBS Lett. 2007, 581, 3382–3386. [Google Scholar] [CrossRef]
- Miller, J.D.; Sal, M.S.; Schell, M.; Whittimore, J.D.; Raulston, J.E. Chlamydia trachomatis YtgA is an iron-binding periplasmic protein induced by iron restriction. Microbiology 2009, 155, 2884–2894. [Google Scholar] [CrossRef] [PubMed]
- Wyrick, P.B. Chlamydia trachomatis persistence in vitro: An overview. J. Infect. Dis. 2010, 201, S88–S95. [Google Scholar] [CrossRef] [PubMed]
- Hokynar, K.; Korhonen, S.; Norja, P.; Paavonen, J.; Puolakkainen, M. Antibody to Chlamydia trachomatis proteins, TroA and HtrA, as a biomarker for Chlamydia trachomatis infection. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Rantsi, T.; Joki-Korpela, P.; Hokynar, K.; Kalliala, I.; Öhman, H.; Surcel, H.M.; Paavonen, J.; Tiitinen, A.; Puolakkainen, M. Serum antibody response to Chlamydia trachomatis TroA and HtrA in women with tubal factor infertility. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 1499–1502. [Google Scholar] [CrossRef] [PubMed]
- Rantsi, T.; Öhman, H.; Puolakkainen, M.; Bloigu, A.; Paavonen, J.; Surcel, H.M.; Tiitinen, A.; Joki-Korpela, P. Predicting tubal factor infertility by using markers of humoral and cell-mediated immune response against Chlamydia trachomatis. Am. J. Reprod. Immunol. 2018, 80, e13051. [Google Scholar] [CrossRef] [PubMed]
- Land, J.A.; Evers, J.L.; Goossens, V.J. How to use Chlamydia antibody testing in subfertility patients. Hum. Reprod. 1998, 13, 1094–1098. [Google Scholar] [CrossRef] [PubMed]
- Rock, J.A. The revised American Fertility Society classification of endometriosis: reproducibility of scoring. ZOLADEX Endometriosis Study Group. Fertil. Steril. 1995, 63, 1108–1110. [Google Scholar] [CrossRef]
- Mol, B.W.; Dijkman, B.; Wertheim, P.; Lijmer, J.; van der Veen, F.; Bossuyt, P.M. The accuracy of serum chlamydial antibodies in the diagnosis of tubal pathology: A meta-analysis. Fertil. Steril. 1997, 67, 1031–1037. [Google Scholar] [CrossRef]
- Akande, V.A.; Hunt, L.P.; Cahill, D.J.; Caul, E.O.; Ford, W.C.; Jenkins, J.M. Tubal damage in infertile women: Prediction using chlamydia serology. Hum. Reprod. 2003, 18, 1841–1847. [Google Scholar] [CrossRef]
- El Hakim, E.A.; Gordon, U.D.; Akande, V.A. The relationship between serum Chlamydia antibody levels and severity of disease in infertile women with tubal damage. Arch. Gynecol. Obstet. 2010, 281, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Tsevat, D.G.; Wiesenfeld, H.C.; Parks, C.; Peipert, J.F. Sexually transmitted diseases and infertility. Am. J. Gynecol. Obstet. 2017, 216, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Den Hartog, J.E.; Morre, S.A.; Land, J.A. Chlamydia trachomatis-associated tubal factor subfertility: Immunogenetic aspects and serological screening. Hum. Reprod. Update 2006, 12, 719–730. [Google Scholar] [CrossRef] [PubMed]
- Öhman, H.; Tiitinen, A.; Halttunen, M.; Lehtinen, M.; Paavonen, J.; Surcel, H.M. Cytokine polymorphisms and severity of tubal damage in women with Chlamydia-associated infertility. J. Infect. Dis. 2009, 199, 1353–1359. [Google Scholar] [CrossRef] [PubMed]
- Byrne, G.I. Chlamydia trachomatis strains and virulence: Rethinking links to infection prevalence and disease severity. J. Infect. Dis. 2010, 201, S126–S133. [Google Scholar] [CrossRef] [PubMed]
- Coppus, S.F.; Land, J.A.; Opmeer, B.C.; Steures, P.; Eijkemans, M.J.; Hompes, P.G.; Bossuyt, P.M.; van der Veen, F.; Mol, B.W.; van der Steeg, J.W. Chlamydia trachomatis IgG seropositivity is associated with lower natural conception rates in ovulatory subfertile women without visible tubal pathology. Hum. Reprod. 2011, 26, 3061–3067. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| TFI (N = 28) | Controls (N = 51) | p-Value | |
|---|---|---|---|
| TroA IgG (%) | 60.7 (17/28) | 21.6 (11/51) | 0.001 |
| HtrA IgG (%) | 57.1 (16/28) | 21.6 (11/51) | 0.001 |
| MOMP IgG (%) | 53.6 (15/28) | 33.3 (17/51) | 0.08 |
| Antibody Test | Sensitivity (%, 95% CI) | Specificity (%, 95% CI) | Accuracy (%, 95% CI) | PPV (%, 95% CI) | NPV (%, 95% CI) |
|---|---|---|---|---|---|
| TroA IgG | 60.7 (40.6⎯78.5) | 78.4 (64.7⎯88.7) | 72.2 (60.9⎯81.7) | 60.7 (45.8⎯73.8) | 78.4 (69.2⎯85.5) |
| HtrA IgG | 57.1 (37.2⎯75.5) | 78.4 (64.7⎯88.7) | 70.9 (59.6⎯80.6) | 59.3 (44.1⎯72.9) | 76.9 (68.0⎯84.0) |
| MOMP IgG | 53.6 (33.9⎯72.5) | 66.7 (52.1⎯79.2) | 62.0 (50.4⎯72.7) | 46.9 (34.4⎯59.7) | 72.3 (62.7⎯80.3) |
| Test combinations | |||||
| TroA + HtrA IgG | 53.6 (33.9⎯72.5) | 86.3 (73.7⎯94.3) | 74.7 (63.6⎯83.8) | 68.2 (49.8⎯82.2) | 77.2 (69.1⎯83.6) |
| TroA + MOMP IgG | 39.3 (21.5⎯59.4) | 84.3 (71.4⎯92.3) | 68.4 (56.9⎯78.4) | 57.9 (38.5⎯75.1) | 71.7 (64.7⎯77.7) |
| HtrA + MOMP IgG | 32.1 (15.9⎯52.4) | 90.2 (78.6⎯96.7) | 69.6 (58.3⎯79.5) | 64.3 (40.1⎯82.9) | 70.8 (64.9⎯76.0) |
| TroA + HtrA + MOMP IgG | 35.7 (18.6⎯55.9) | 88.2 (76.1⎯95.6) | 69.6 (58.3⎯79.5) | 62.5 (40.4⎯80.4) | 71.4 (65.1⎯77.0) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rantsi, T.; Land, J.A.; Joki-Korpela, P.; Ouburg, S.; Hokynar, K.; Paavonen, J.; Tiitinen, A.; Puolakkainen, M. Predictive Values of Serum Chlamydia trachomatis TroA and HtrA IgG Antibodies as Markers of Persistent Infection in the Detection of Pelvic Adhesions and Tubal Occlusion. Microorganisms 2019, 7, 391. https://doi.org/10.3390/microorganisms7100391
Rantsi T, Land JA, Joki-Korpela P, Ouburg S, Hokynar K, Paavonen J, Tiitinen A, Puolakkainen M. Predictive Values of Serum Chlamydia trachomatis TroA and HtrA IgG Antibodies as Markers of Persistent Infection in the Detection of Pelvic Adhesions and Tubal Occlusion. Microorganisms. 2019; 7(10):391. https://doi.org/10.3390/microorganisms7100391
Chicago/Turabian StyleRantsi, Tiina, Jolande A. Land, Päivi Joki-Korpela, Sander Ouburg, Kati Hokynar, Jorma Paavonen, Aila Tiitinen, and Mirja Puolakkainen. 2019. "Predictive Values of Serum Chlamydia trachomatis TroA and HtrA IgG Antibodies as Markers of Persistent Infection in the Detection of Pelvic Adhesions and Tubal Occlusion" Microorganisms 7, no. 10: 391. https://doi.org/10.3390/microorganisms7100391
APA StyleRantsi, T., Land, J. A., Joki-Korpela, P., Ouburg, S., Hokynar, K., Paavonen, J., Tiitinen, A., & Puolakkainen, M. (2019). Predictive Values of Serum Chlamydia trachomatis TroA and HtrA IgG Antibodies as Markers of Persistent Infection in the Detection of Pelvic Adhesions and Tubal Occlusion. Microorganisms, 7(10), 391. https://doi.org/10.3390/microorganisms7100391