

The Yellow Fever Outbreak in Brazil (2016–2018): How a Low Vaccination Coverage Can Contribute to Emerging Disease Outbreaks

 ,
, 
 , ,
, ,  and
and {kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Yellow Fever Vaccine
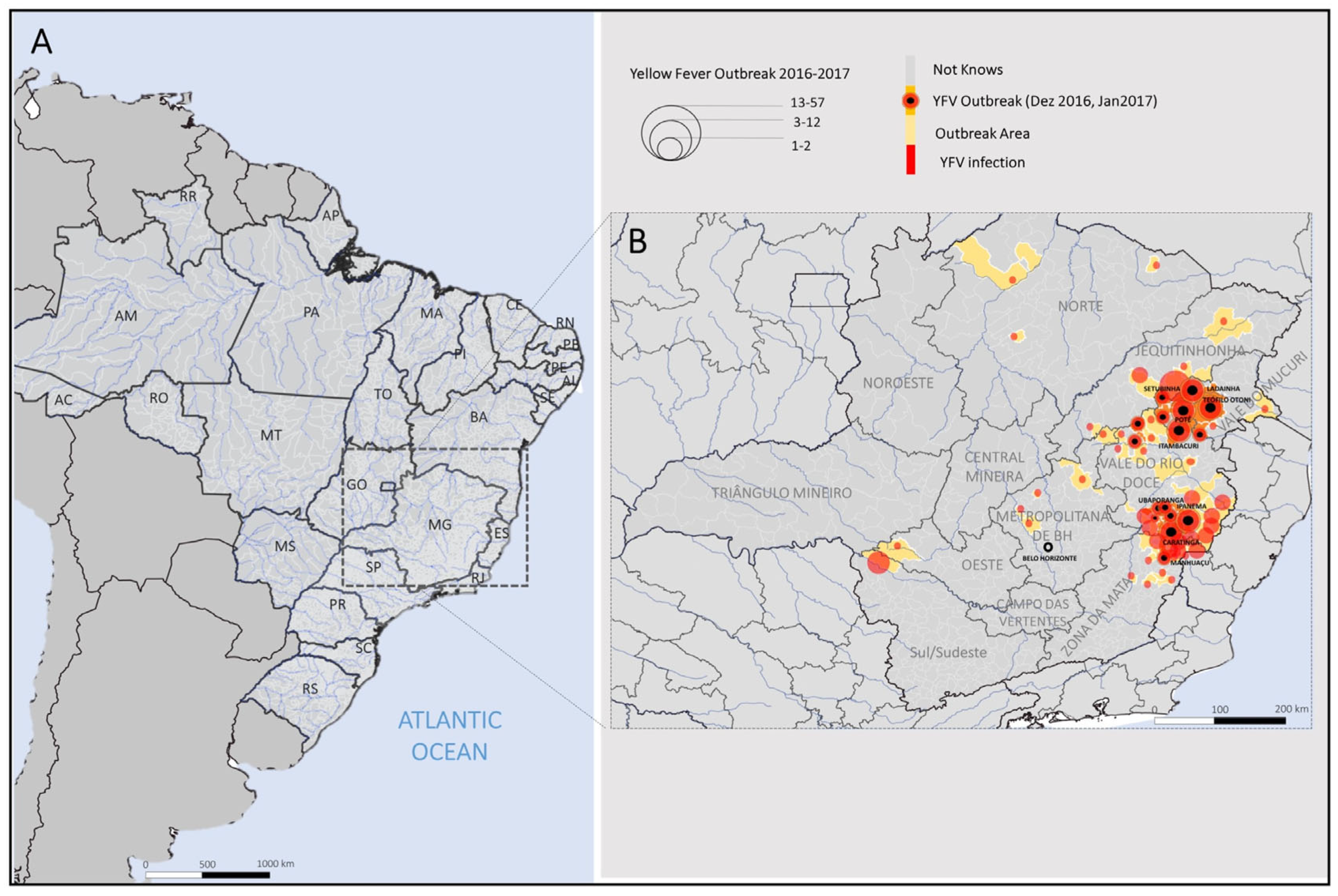
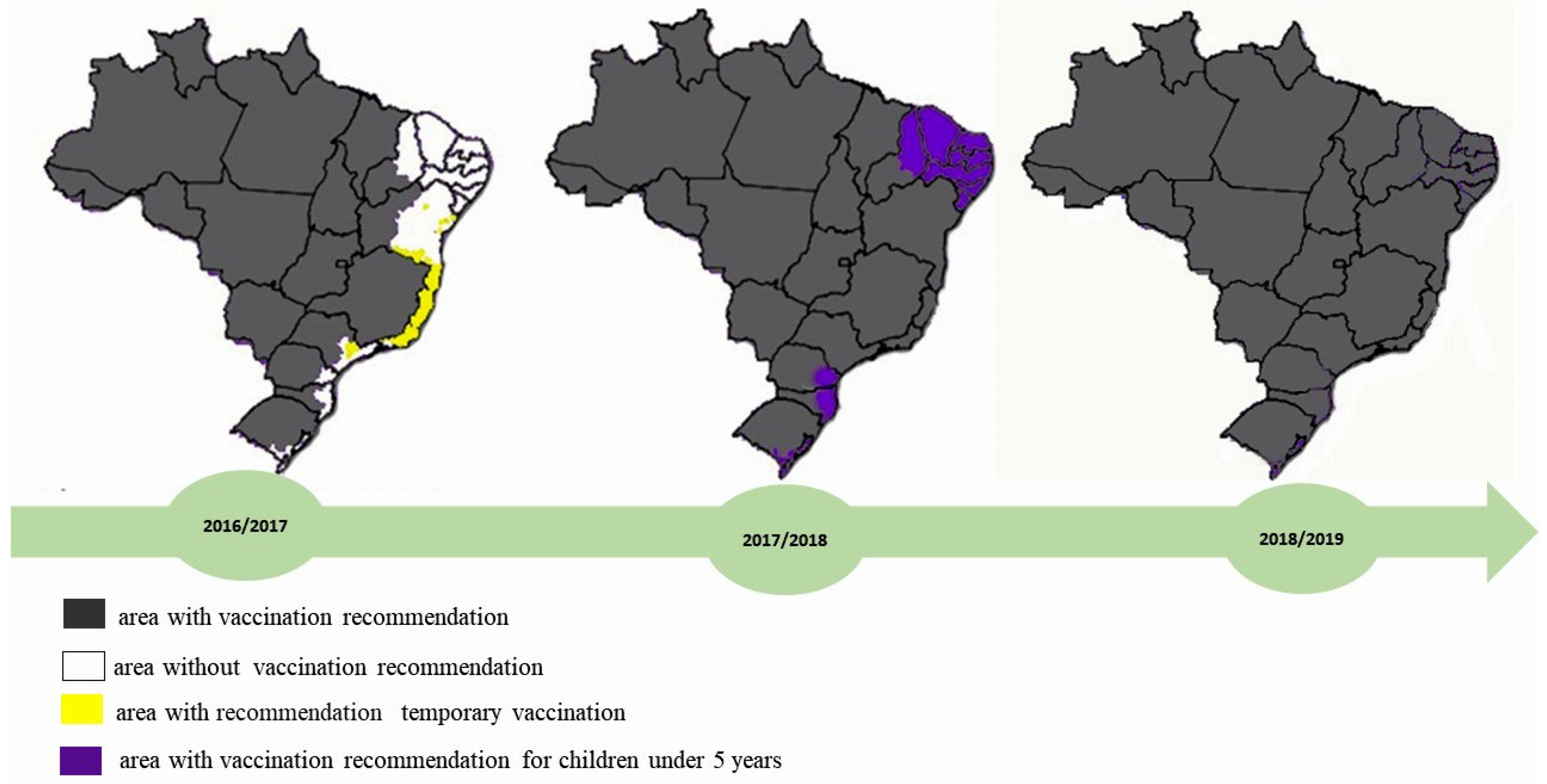
3. The Most Recent Outbreak in Brazil: From Minas Gerais State to the Country
4. The Viral Genotype Circulating in Brazil
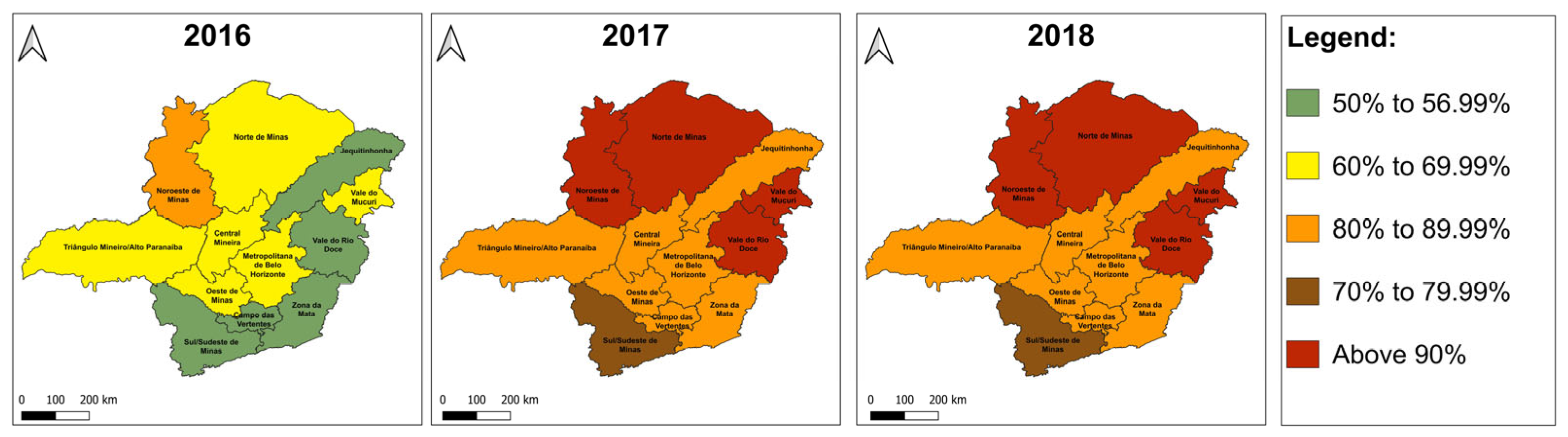
5. Low Vaccination Coverage: The Beginning of an Outbreak
6. Lessons and Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACRV | Area with vaccine recommendation |
| ASVR | Area without vaccine recommendation |
| VHF | Viral hemorrhagic fever |
| WHO | World Health Organization |
| YF | Yellow fever |
| YFV | Orthoflavivirus flavi |
References
- Monath, T.P. Yellow fever: An update. Lancet Infect. Dis. 2001, 1, 11–20. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Yellow Fever. 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/yellow-fever (accessed on 2 May 2025).
- International Committee on Taxonomy of Viruses: ICTV. Orthoflavivirus flavi. Available online: https://ictv.global/taxonomy/taxondetails?taxnode_id02403121&taxon_name=Orthoflavivirus%20flavi (accessed on 28 April 2025).
- Zanotto, P.M.; Gould, E.A.; Gao, G.F.; Harvey, P.H.; Holmes, E.C. Population dynamics of flaviviruses revealed by molecular phylogenies. Proc. Natl. Acad. Sci. USA 1996, 93, 548–553. [Google Scholar] [CrossRef] [PubMed]
- Rogers, D.J.; Wilson, A.J.; Hay, S.I.; Graham, A.J. The Global Distribution of Yellow Fever and Dengue. Adv. Parasitol. 2006, 62, 181–220. [Google Scholar] [PubMed]
- Barnett, E.D. Yellow Fever: Epidemiology and Prevention. Clin. Infect. Dis. 2007, 44, 850–856. [Google Scholar] [CrossRef]
- Monath, T.P. Yellow fever vaccine. Expert Rev. Vaccines 2005, 4, 553–574. [Google Scholar] [CrossRef]
- Monath, T.P.; Vasconcelos, P.F.C. Yellow fever. J. Clin. Virol. 2015, 64, 160–173. [Google Scholar] [CrossRef]
- Igloi, Z.; Pezzi, L.; Charrel, R.N.; Koopmans, M. Detection of yellow fever virus genome in urine following natural infection or vaccination: Review of current knowledge 1985–2023. J. Clin. Virol. 2024, 105740. [Google Scholar] [CrossRef]
- Russel, F.F. Permanent Value of Major Walter Reed’s Work on Yellow Fever. Am. J. Public Health Nations Health 1934, 24, 1–7. [Google Scholar] [CrossRef]
- Norrby, E. Yellow fever and Max Theiler: The only Nobel Prize for a virus vaccine. J. Exp. Med. 2007, 204, 2779–2784. [Google Scholar] [CrossRef]
- Bollati, M. Structure and functionality in flavivirus NS-proteins: Perspectives for drug design. Antivir. Res. 2010, 87, 125–148. [Google Scholar] [CrossRef]
- Hansen, C.A.; Barrett, A.D. The present and future of yellow fever vaccines. Pharmaceuticals 2021, 14, 891. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.L.; Martins, M.A.; Espírito-Santo, L.R.; Campi-Azevedo, A.C.; Silveira-Lemos, D.; Ribeiro, J.G.L.; Homma, A.; Kroon, E.G.; Teixeira-Carvalho, A.; Elói-Santos, S.M.; et al. Characterization of main cytokine sources from the innate and adaptive immune responses following primary 17DD yellow fever vaccination in adults. Vaccine 2011, 29, 583–592. [Google Scholar] [CrossRef] [PubMed]
- Staples, J.E.; O’Laughlin, K. Yellow Fever Vaccine. In CDC Yellow Book: Health Information for International Travel, 2026th ed.; CDC: Atlanta, GA, USA, 2025. Available online: https://www.cdc.gov/yellow-book/hcp/travel-associated-infections-diseases/yellow-fever.html (accessed on 2 May 2025).
- Barrett, A.D. Yellow fever live attenuated vaccine: A very successful live attenuated vaccine but still we have problems controlling the disease. Vaccine 2017, 35, 5951–5955. [Google Scholar] [CrossRef]
- de Melo, A.B.; da Paz C da Silva, M.; Magalhães, M.C.F.; Gil, L.H.V.G.; de Carvalho, E.M.F.; Braga-Neto, U.M.; Bertani, G.R.; Jr, E.T.A.M.; Cordeiro, M.T. Description of a prospective 17DD yellow fever vaccine cohort in Recife, Brazil. Am. J. Trop. Med. Hyg. 2011, 85, 739. [Google Scholar] [CrossRef]
- Pan American Health Organization. Epidemiological Update—Yellow Fever in the Region of the Americas. Available online: https://www.paho.org/en/documents/epidemiological-update-yellow-fever-region-americas-25-april-2023 (accessed on 16 May 2023).
- Poland, J.D.; Calisher, C.H.; Monath, T.P.; Downs, W.G.; Murphy, K. Persistence of neutralizing antibody 30–35 years after immunization with 17D yellow fever vaccine. Bull. World Health Organ. 1981, 59, 895–900. [Google Scholar]
- Monath, T.P.; Nichols, R.; Archambault, W.T.; Moore, L.; Marchesani, R.; Tian, J.; Shope, R.E.; Thomas, N.; Schrader, R.; Furby, D.; et al. Comparative safety and immunogenicity of two yellow fever 17D vaccines (ARILVAX and YF-VAX) in a phase III multicenter, double-blind clinical trial. Am. J. Trop. Med. Hyg. 2002, 66, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Lindsey, N.P.; Schroeder, B.A.; Miller, E.R.; Braun, M.M.; Hinckley, A.F.; Marano, N.; Slade, B.A.; Barnett, E.D.; Brunette, G.W.; Horan, K.; et al. Adverse event reports following yellow fever vaccination. Vaccine 2008, 26, 6077–6082. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Morbidity and Mortality Weekly Report (MMWR): Yellow Fever Vaccine: Recommendations of the Advisory Committee on Immunization Practices (ACIP). 2010. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/rr5907a1.htm (accessed on 2 May 2025).
- Cetron, M.S.; Marfin, A.A.; Julian, K.G.; Gubler, D.J.; Sharp, D.J.; Barwick, R.S.; Weld, L.H.; Chen, R.; Clover, R.D.; Deseda-Tous, J.; et al. Yellow fever vaccine recommendations of the Advisory Committee on Immunization Practices (ACIP), 2002. Morb. Mortal. Wkly. Rep. Recomm. Rep. 2002, 51, 1–27. [Google Scholar]
- Kelso, J.M.; Mootrey, G.T.; Tsai Theodore, F. Anaphylaxis from yellow fever vaccine. J. Allergy Clin. Immunol. 1999, 103, 698–701. [Google Scholar] [CrossRef]
- Staples, J.E.; Barrett, A.D.T.; Wilder-Smith, A.; Hombach, J. Review of data and knowledge gaps regarding yellow fever vaccine-induced immunity and duration of protection. NPJ Vaccines 2020, 5, 54. [Google Scholar] [CrossRef]
- Abdala-Torres, T.; Campi-Azevedo, A.C.; da Silva-Pereira, R.A.; Dos Santos, L.I.; Henriques, P.M.; Costa-Rocha, I.A.; Otta, D.A.; Peruhype-Magalhães, V.; Teixeira-Carvalho, A.; Araújo, M.S.S.; et al. Immune response induced by standard and fractional doses of 17DD yellow fever vaccine. NPJ Vaccines 2024, 9, 54. [Google Scholar] [CrossRef] [PubMed]
- Mir, D.; Delatorre, E.; Bonaldo, M.; Lourenço-de-Oliveira, R.; Vicente, A.C.; Bello, G. Phylodynamics of Yellow Fever Virus in the Americas: New insights into the origin of the 2017. Brazilian outbreak. Sci. Rep. 2017, 7, 7385. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, L.A. Da transmissão hídrica a culicidiana: A febre amarela na sociedade de medicina e cirurgia de São Paulo. Rev. Bras. Hist. 2001, 21, 217–242. [Google Scholar] [CrossRef]
- Vasconcelos, P.F.D.C. Febre amarela: Reflexões sobre a doença, as perspectivas para o século XXI e o risco da reurbanização. Rev. Bras. Epidemiol. 2002, 5, 244–258. [Google Scholar] [CrossRef]
- Vasconcelos, P.F.C.; Costa, Z.G.; Travassos Da Rosa, E.S.; Luna, E.; Rodrigues, S.G.; Barros, V.L.; Dias, J.P.; Monteiro, H.A.; Oliva, O.F.; Vasconcelos, H.B.; et al. Epidemic of Jungle Yellow Fever in Brazil, 2000: Implications of Climatic Alterations in Disease Spread. J. Med. Virol. 2001, 65, 598–604. [Google Scholar] [CrossRef]
- Ministry of Health (Brazil). Epidemiological Surveillance Guide. Available online: http://bvsms.saude.gov.br/bvs/publicacoes/guia_vigilancia_epidemiologica_7ed.pdf (accessed on 12 December 2018). (In Portuguese)
- Rezende, I.M.; Sacchetto, L.; Munhoz de Mello, É.; Alves, P.A.; Iani, F.C.M.; Adelino, T.É.R.; Duarte, M.M.; Cury, A.L.F.; Bernardes, A.F.L.; Santos, T.A.; et al. Persistence of Yellow Fever virus outside the Amazon Basin, causing epidemics in Southeast Brazil, from 2016 to 2018. PLoS Negl. Trop. Dis. 2018, 12, e0006538. [Google Scholar] [CrossRef]
- Ministry of Health (Brazil). Contingency Plan for Emergency Response in Public Health: Yellow Fever. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/plano_contingencia_emergencias_febre_amarela.pdf (accessed on 7 March 2023). (In Portuguese)
- Possas, C.; Lourenço-De-Oliveira, R.; Tauil, P.L.; Pinheiro, F.d.P.; Pissinatti, A.; da Cunha, R.V.; Freire, M.; Martins, R.M.; Homma, A. Yellow fever outbreak in Brazil: The puzzle of rapid viral spread and challenges for immunization. Mem. Inst. Oswaldo Cruz 2018, 113, e180278. [Google Scholar] [CrossRef]
- Silva, N.I.O.; Sacchetto, L.; de Rezende, I.M.; Trindade, G.d.S.; LaBeaud, A.D.; de Thoisy, B.; Drumond, B.P. Recent sylvatic yellow fever virus transmission in Brazil: The news from an old disease. Virol. J. 2020, 17, 9. [Google Scholar] [CrossRef]
- Douam, F.; Ploss, A. Yellow Fever Virus: Knowledge Gaps Impeding the Fight Against an Old Foe. Trends Microbiol. 2018, 26, 913–928. [Google Scholar] [CrossRef]
- Ministry of Health (Brazil). Monitoring the Seasonal Period of Yellow Fever 2017–2018. Available online: https://sbim.org.br/images/files/informe-fa-21-11abr18-c.pdf (accessed on 15 December 2018). (In Portuguese).
- Bonaldo, M.C.; Gómez, M.M.; dos Santos, A.A.; de Abreu, F.V.S.; Ferreira-De-Brito, A.; de Miranda, R.M.; de Castro, M.G.; Lourenço-De-Oliveira, R. Genome analysis of yellow fever virus of the ongoing outbreak in brazil reveals polymorphisms. Mem. Inst. Oswaldo Cruz 2017, 112, 447–451. [Google Scholar] [CrossRef]
- Ministry of Health (Brazil). Epidemiological Bulletin: Epidemiological Emergency of Yellow Fever in Brazil, from December 2016 to July 2017; Ministério da Saúde: Brasília, Brazil, 2017; Volume 48, pp. 1–22. (In Portuguese) [Google Scholar]
- Secretary of State for Health of Minas Gerais (Brazil). Epidemiological Bulletin 26/08/2018: Wild Yellow Fever in Minas Gerais; Secretária do Estado de Saúde de Minas Gerais: Belo Horizonte, Brazil, 2018; pp. 1–12. (In Portuguese) [Google Scholar]
- Romano, A.P.M.; Costa, Z.G.A.; Ramos, D.G.; Andrade, M.A.; Jayme, V.d.S.; de Almeida, M.A.B.; Vettorello, K.C.; Mascheretti, M.; Flannery, B. Yellow Fever outbreaks in unvaccinated populations, Brazil, 2008–2009. PLoS Negl. Trop. Dis. 2014, 8, e2740. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health (Brazil). Yellow Fever: Confirmed Cases Notified in the Notification Aggregation Information System—Minas Gerais. Available online: http://tabnet.datasus.gov.br/cgi/deftohtm.exe?sinanwin/cnv/febreamarelabr.def (accessed on 20 December 2018). (In Portuguese)
- Secretary of State for Health of Minas Gerais (Brazil). State Health Plan 2020–2023. Available online: https://www.conass.org.br/wp-content/uploads/2021/04/08-02-Plano-Estadual-de-Saude-de-Minas-Gerais-2020-2023.pdf (accessed on 7 March 2023). (In Portuguese).
- Beck, A.; Guzman, H.; Li, L.; Ellis, B.; Tesh, R.B.; Barrett, A.D. Phylogeographic reconstruction of African yellow fever virus isolates indicates recent simultaneous dispersal into east and west Africa. PLoS Neglected Trop. Dis. 2013, 7, e1910. [Google Scholar] [CrossRef] [PubMed]
- Bryant, J.E.; Barrett, A.D. Comparative phylogenies of yellow fever isolates from Peru and Brazil. FEMS Immunol. Med. Microbol 2003, 39, 103–118. [Google Scholar] [CrossRef]
- Auguste, A.J.; Lemey, P.; Pybus, O.G.; Suchard, M.A.; Salas, R.A.; Adesiyun, A.A.; Barrett, A.D.; Tesh, R.B.; Weaver, S.C.; Carrington, C.V.F. Yellow fever virus maintenance in Trinidad and its dispersal throughout the Americas. J. Virol. 2010, 84, 9967–9977. [Google Scholar] [CrossRef] [PubMed]
- Delatorre, E.; de Abreu, F.V.S.; Ribeiro, I.P.; Gómez, M.M.; dos Santos, A.A.C.; Ferreira-De-Brito, A.; Neves, M.S.A.S.; Bonelly, I.; de Miranda, R.M.; Furtado, N.D.; et al. Distinct YFV Lineages Co-circulated in the Central-Western and Southeastern Brazilian Regions From 2015 to 2018. Front. Microbiol. 2019, 10, 1079. [Google Scholar] [CrossRef]
- Faria, N.R.; Kraemer, M.U.G.; Hill, S.C.; De Jesus, J.G.; Aguiar, R.S.; Iani, F.C.M.; Xavier, J.; Quick, J.; Du Plessis, L.; Dellicour, S.; et al. Genomic and epidemiological monitoring of yellow fever virus transmission potential. Science 2018, 361, 894–899. [Google Scholar] [CrossRef]
- Ministry of Health (Brazil). Health Surveillance Guide. Available online: http://bvsms.saude.gov.br/bvs/publicacoes/guia_vigilancia_saude_unificado.pdf (accessed on 9 January 2019). (In Portuguese)
- Ministry of Health (Brazil). Yellow Fever Vaccine to Be Extended to All of Brazil. Available online: https://www.gov.br/saude/pt-br/assuntos/noticias/2018/marco/vacina-de-febre-amarela-sera-ampliada-para-todo-o-brasil (accessed on 4 January 2019). (In Portuguese)
- Pan American Health Organization. Control of Yellow Fever: Field Guide. Scientific and Technical Publication. Available online: https://www3.paho.org/hq/dmdocuments/2013/PAHO-fieldguide-yellowfever-2005.pdf (accessed on 14 August 2018).
- Juan-Giner, A.; Kimathi, D.; Grantz, K.H.; Hamaluba, M.; Kazooba, P.; Njuguna, P.; Fall, G.; Dia, M.; Bob, N.S.; Monath, T.P.; et al. Immunogenicity and safety of fractional doses of yellow fever vaccines: A randomised, double-blind, non-inferiority trial. Lancet 2021, 397, 119–127. [Google Scholar] [CrossRef]
- Vasconcelos, P.F.D.C. Febre amarela. Rev. Soc. Bras. Med. Trop. 2003, 36, 275–293. [Google Scholar] [CrossRef]
- Ministry of Health (Brazil). Immunizations, Roof, Technical Notes. Available online: http://tabnet.datasus.gov.br/cgi/dhdat.exe?bd_pni/cpnibr.def (accessed on 7 March 2023). (In Portuguese)
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos, J.D.; Rocha, K.L.S.; Amaral, C.D.; Dutra, A.G.S.; Figueiredo, P.d.O.; Rocha-Vieira, E.; de Abreu, F.V.S.; Trindade, G.d.S.; de Oliveira, D.B. The Yellow Fever Outbreak in Brazil (2016–2018): How a Low Vaccination Coverage Can Contribute to Emerging Disease Outbreaks. Microorganisms 2025, 13, 1287. https://doi.org/10.3390/microorganisms13061287
Santos JD, Rocha KLS, Amaral CD, Dutra AGS, Figueiredo PdO, Rocha-Vieira E, de Abreu FVS, Trindade GdS, de Oliveira DB. The Yellow Fever Outbreak in Brazil (2016–2018): How a Low Vaccination Coverage Can Contribute to Emerging Disease Outbreaks. Microorganisms. 2025; 13(6):1287. https://doi.org/10.3390/microorganisms13061287
Chicago/Turabian StyleSantos, Juliane Duarte, Kamila Lorene Soares Rocha, Carolina Dourado Amaral, Ana Gabriella Stoffella Dutra, Poliana de Oliveira Figueiredo, Etel Rocha-Vieira, Filipe Vieira Santos de Abreu, Giliane de Souza Trindade, and Danilo Bretas de Oliveira. 2025. "The Yellow Fever Outbreak in Brazil (2016–2018): How a Low Vaccination Coverage Can Contribute to Emerging Disease Outbreaks" Microorganisms 13, no. 6: 1287. https://doi.org/10.3390/microorganisms13061287
APA StyleSantos, J. D., Rocha, K. L. S., Amaral, C. D., Dutra, A. G. S., Figueiredo, P. d. O., Rocha-Vieira, E., de Abreu, F. V. S., Trindade, G. d. S., & de Oliveira, D. B. (2025). The Yellow Fever Outbreak in Brazil (2016–2018): How a Low Vaccination Coverage Can Contribute to Emerging Disease Outbreaks. Microorganisms, 13(6), 1287. https://doi.org/10.3390/microorganisms13061287