
The Role of Gut Microbiota in Orthopedic Surgery: A Systematic Review

 , , and
, , and
Abstract
1. Introduction
2. Methodology
2.1. Identification and Selection of Studies
2.2. Search Strategy
2.3. Study Selection
2.3.1. Eligibility Criteria
- Population (P): patients undergoing orthopedic surgeries.
- Intervention (I): gut microbiota.
- Comparison (C): placebo groups.
- Primary outcomes (O): pinfection rates, bone healing, microbiota composition changes, incidence of postoperative cognitive dysfunction, and bone mineral density.
- Study Design (S): randomized controlled trials (RCTs), prospective and retrospective cohort studies, case-control studies, observational cohort studies, and any other suitable study designs.
2.3.2. Inclusion Criteria
2.3.3. Exclusion Criteria
2.4. Methodological Quality Assessment
2.5. Data Selection and Extraction
2.6. Data Analysis
3. Results
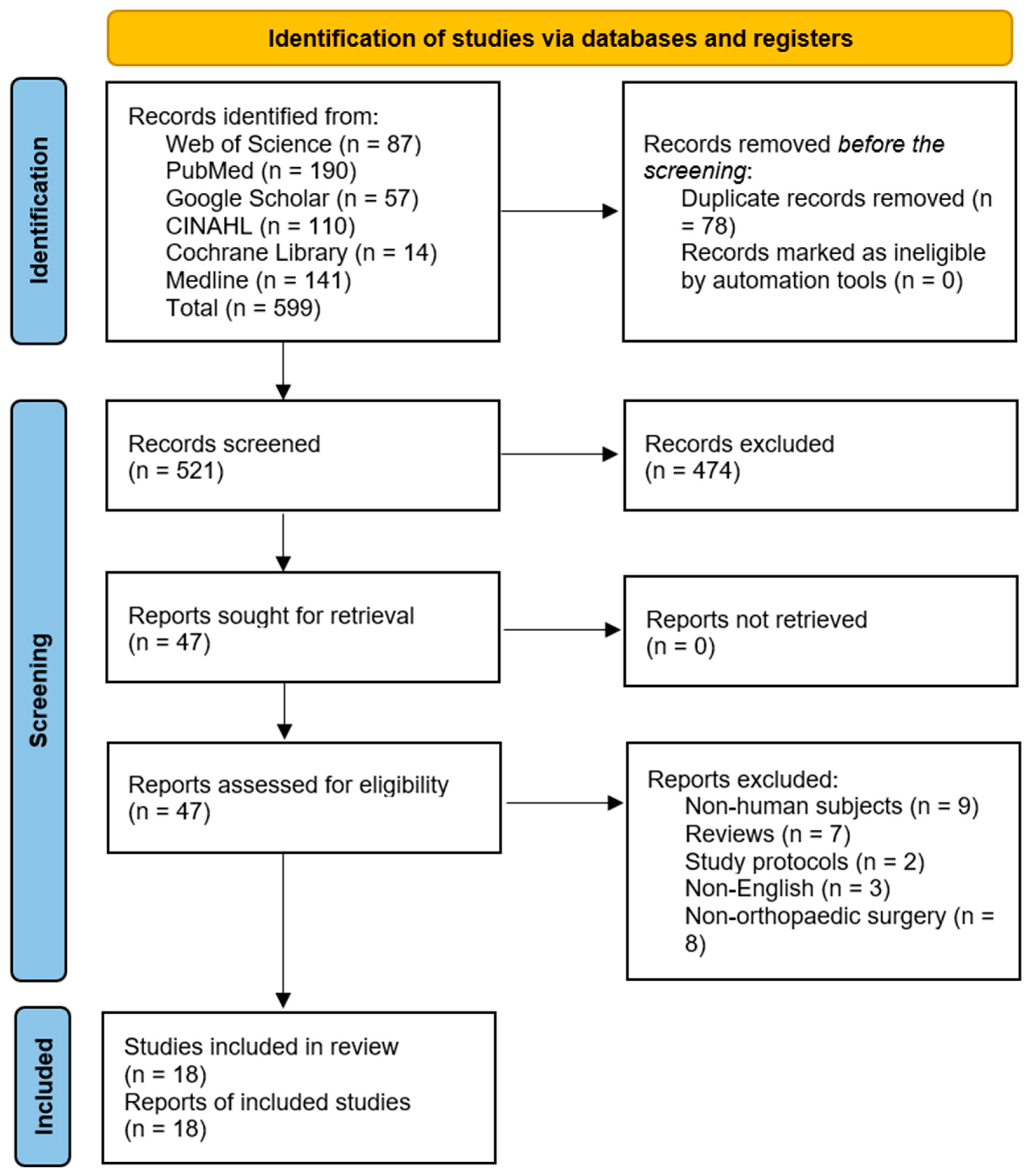
3.1. Study Selection
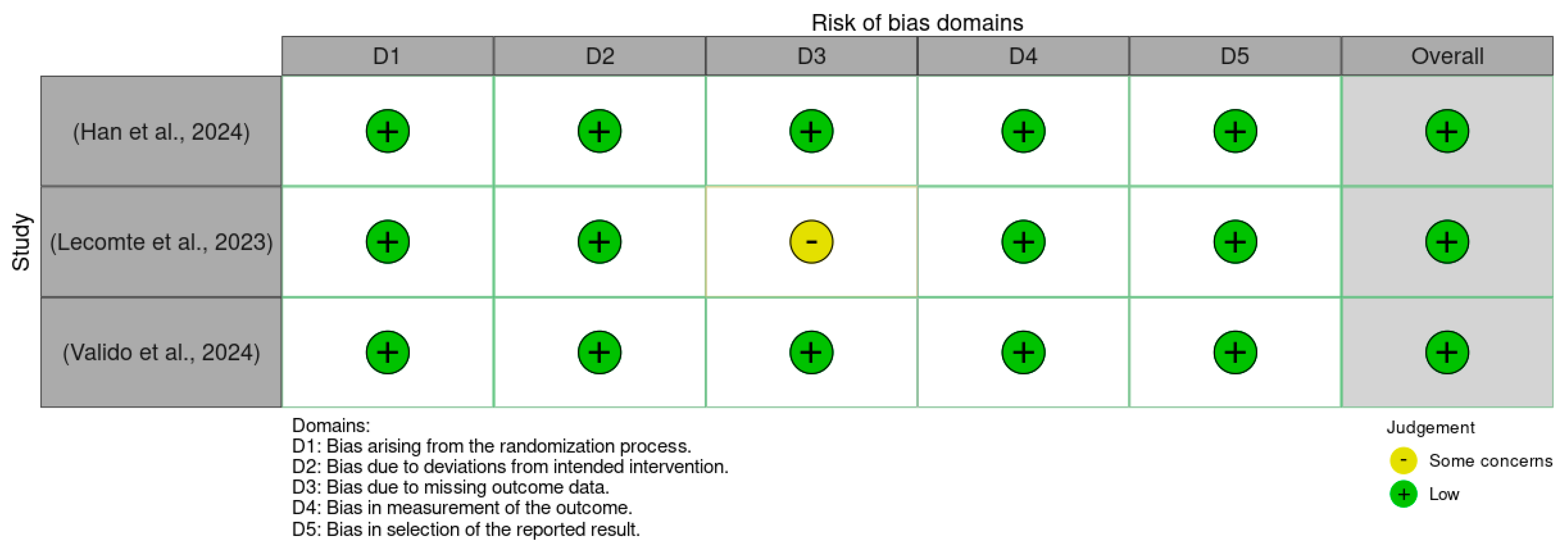
3.2. Methodological Quality Assessment
3.3. Data Selection and Extraction
3.4. Thematic Analysis of Outcomes
3.4.1. Gut Microbiota and Surgical Outcomes
3.4.2. Antibiotic Use and Resistance in Orthopedic Surgery
3.4.3. Probiotic and Prebiotic Interventions
4. Discussion
4.1. Implications for Orthopedic Surgeons
4.1.1. Preoperative Considerations
4.1.2. Postoperative Considerations
4.1.3. Microbiome Testing Protocols: Current Practices and Future Directions
4.2. Study Strengths and Limitations
4.3. Future Directions
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Anwar, H.; Iftikhar, A.; Muzaffar, H.; Almatroudi, A.; Allemailem, K.S.; Navaid, S.; Saleem, S.; Khurshid, M. Biodiversity of Gut Microbiota: Impact of Various Host and Environmental Factors. BioMed Res. Int. 2021, 2021, 5575245. [Google Scholar] [CrossRef] [PubMed]
- Guzzo, G.L.; Andrews, J.M.; Weyrich, L.S. The Neglected Gut Microbiome: Fungi, Protozoa, and Bacteriophages in Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2022, 28, 1112–1122. [Google Scholar] [CrossRef]
- Mani, I.; Singh, V. Multi-omics in Gut Microbiome. In Multi-Omics Analysis of the Human Microbiome; ResearchGate: Berlin, Germany, 2024. [Google Scholar] [CrossRef]
- Pant, A.; Maiti, T.K.; Mahajan, D.; Das, B. Human Gut Microbiota and Drug Metabolism. Microb. Ecol. 2023, 86, 97–111. [Google Scholar] [CrossRef]
- Khan, I.; Bai, Y.; Zha, L.; Ullah, N.; Ullah, H.; Shah, S.R.H.; Sun, H.; Zhang, C. Mechanism of the gut microbiota colonization resistance and enteric pathogen infection. Front. Cell. Infect. Microbiol. 2021, 11, 716299. [Google Scholar] [CrossRef]
- Fakhoury, H.M.A.; Kvietys, P.R.; AlKattan, W.; Anouti, F.A.; Elahi, M.A.; Karras, S.N.; Grant, W.B. Vitamin D and intestinal homeostasis: Barrier, microbiota, and immune modulation. J. Steroid Biochem. Mol. Biol. 2020, 200, 105663. [Google Scholar] [CrossRef] [PubMed]
- Amoroso, C.; Perillo, F.; Strati, F.; Fantini, M.; Caprioli, F.; Facciotti, F. The Role of Gut Microbiota Biomodulators on Mucosal Immunity and Intestinal Inflammation. Cells 2020, 9, 1234. [Google Scholar] [CrossRef] [PubMed]
- Kho, Z.Y.; Lal, S.K. The Human Gut Microbiome—A Potential Controller of Wellness and Disease. Front. Microbiol. 2018, 9, 356589. [Google Scholar] [CrossRef]
- Parizadeh, M.; Arrieta, M.C. The global human gut microbiome: Genes, lifestyles, and diet. Trends Mol. Med. 2023, 29, 789–801. [Google Scholar] [CrossRef]
- Seely, K.D.; Kotelko, C.A.; Douglas, H.; Bealer, B.; Brooks, A.E. The Human Gut Microbiota: A Key Mediator of Osteoporosis and Osteogenesis. Int. J. Mol. Sci. 2021, 22, 9452. [Google Scholar] [CrossRef]
- Vernocchi, P.; Del Chierico, F.; Putignani, L. Gut Microbiota Metabolism and Interaction with Food Components. Int. J. Mol. Sci. 2020, 21, 3688. [Google Scholar] [CrossRef]
- Wiertsema, S.P.; van Bergenhenegouwen, J.; Garssen, J.; Knippels, L.M.J. The Interplay between the Gut Microbiome and the Immune System in the Context of Infectious Diseases throughout Life and the Role of Nutrition in Optimizing Treatment Strategies. Nutrients 2021, 13, 886. [Google Scholar] [CrossRef] [PubMed]
- Chidambaram, S.B.; Essa, M.M.; Rathipriya, A.G.; Bishir, M.; Ray, B.; Mahalakshmi, A.M.; Tousif, A.H.; Sakharkar, M.K.; Kashyap, R.S.; Friedland, R.P.; et al. Gut dysbiosis, defective autophagy and altered immune responses in neurodegenerative diseases: Tales of a vicious cycle. Pharmacol. Ther. 2022, 231, 107988. [Google Scholar] [CrossRef]
- Jones, R.M.; Mulle, J.G.; Pacifici, R. Osteomicrobiology: The influence of gut microbiota on bone in health and disease. Bone 2018, 115, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Shavandi, A.; Saeedi, P.; Gérard, P.; Jalalvandi, E.; Cannella, D.; Bekhit, A.E.D. The role of microbiota in tissue repair and regeneration. J. Tissue Eng. Regen. Med. 2020, 14, 539–555. [Google Scholar] [CrossRef] [PubMed]
- Hussain, Z.; Park, H. Inflammation and Impaired Gut Physiology in Post-operative Ileus: Mechanisms and the Treatment Options. J. Neurogastroenterol. Motil. 2022, 28, 517–530. [Google Scholar] [CrossRef]
- Mustansir Dawoodbhoy, F.; Patel, B.K.; Patel, K.; Bhatia, M.; Lee, C.N.; Moochhala, S.M. Gut Microbiota Dysbiosis as a Target for Improved Post-Surgical Outcomes and Improved Patient Care: A Review of Current Literature. Shock 2021, 55, 441–454. [Google Scholar] [CrossRef]
- Al Bander, Z.; Nitert, M.D.; Mousa, A.; Naderpoor, N. The Gut Microbiota and Inflammation: An Overview. Int. J. Environ. Res. Public Health 2020, 17, 7618. [Google Scholar] [CrossRef]
- Koliarakis, I.; Athanasakis, E.; Sgantzos, M.; Mariolis-Sapsakos, T.; Xynos, E.; Chrysos, E.; Souglakos, J.; Tsiaoussis, J. Intestinal microbiota in colorectal cancer surgery. Cancers 2020, 12, 3011. [Google Scholar] [CrossRef]
- Stavrou, G.; Kotzampassi, K. Gut microbiome, surgical complications and probiotics. Ann. Gastroenterol. 2017, 30, 45–53. [Google Scholar] [CrossRef]
- Long, D.R.; Alverdy, J.C.; Vavilala, M.S. Emerging Paradigms in the Prevention of Surgical Site Infection: The Patient Microbiome and Antimicrobial Resistance. Anesthesiology 2022, 137, 252–262. [Google Scholar] [CrossRef]
- Buis, N.; Esfandiari, H.; Hoch, A.; Fürnstahl, P. Overview of Methods to Quantify Invasiveness of Surgical Approaches in Orthopedic Surgery—A Scoping Review. Front. Surg. 2022, 8, 771275. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, M.; Yan, Z.; Ji, S.; Xiao, S.; Gao, J. Metal nanoparticle hybrid hydrogels: The state-of-the-art of combining hard and soft materials to promote wound healing. Theranostics 2024, 14, 1534–1560. [Google Scholar] [CrossRef] [PubMed]
- Lederer, A.K.; Chikhladze, S.; Kohnert, E.; Huber, R.; Müller, A. Current Insights: The Impact of Gut Microbiota on Postoperative Complications in Visceral Surgery—A Narrative Review. Diagnostics 2021, 11, 2099. [Google Scholar] [CrossRef]
- Porcari, S.; Mullish, B.H.; Asnicar, F.; Ng, S.C.; Zhao, L.; Hansen, R.; O’Toole, P.W.; Raes, J.; Hold, G.; Putignani, L.; et al. International consensus statement on microbiome testing in clinical practice. Lancet Gastroenterol. Hepatol. 2025, 10, 154–167. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef]
- Ma, L.L.; Wang, Y.Y.; Yang, Z.H.; Huang, D.; Weng, H.; Zeng, X.T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 7. [Google Scholar] [CrossRef] [PubMed]
- Clarke, V.; Braun, V. Thematic analysis. J. Posit. Psychol. 2017, 12, 297–298. [Google Scholar] [CrossRef]
- Han, Y.; Zhou, Y.; Xu, X.; Chen, S.; Zhang, S.; Jiang, N.; Liu, Z.; Zhang, J.; Luo, Z.; Zhang, X.; et al. Improvement of post-surgery constipation in patients with fractures by Lactobacillus rhamnosus JYLR-127: A single-blind randomized controlled trial. Nutrients 2024, 16, 1505. [Google Scholar] [CrossRef]
- Valido, E.; Capossela, S.; Glisic, M.; Hertig-Godeschalk, A.; Bertolo, A.; Stucki, G.; Flueck, J.L.; Stoyanov, J. Gut microbiome and inflammation among athletes in wheelchair in a crossover randomized pilot trial of probiotic and prebiotic interventions. Sci. Rep. 2024, 14, 12838. [Google Scholar] [CrossRef]
- Lecomte, M.; Tomassi, D.; Rizzoli, R.; Tenon, M.; Berton, T.; Harney, S.; Fança-Berthon, P. Effect of a hop extract standardized in 8-prenylnaringenin on bone health and gut microbiome in postmenopausal women with osteopenia: A one-year randomized, double-blind, placebo-controlled trial. Nutrients 2023, 15, 2688. [Google Scholar] [CrossRef]
- Aboushaala, K.; Chee, A.V.; Adnan, D.; Toro, S.J.; Singh, H.; Savoia, A.; Dhillon, E.S.; Yuh, C.; Dourdourekas, J.; Patel, I.K.; et al. Gut microbiome dysbiosis is associated with lumbar degenerative spondylolisthesis in symptomatic patients. JOR Spine 2024, 7, e70005. [Google Scholar] [CrossRef] [PubMed]
- Chisari, E.; Cho, J.; Wouthuyzen-Bakker, M.; Parvizi, J. Gut permeability may be associated with periprosthetic joint infection after total hip and knee arthroplasty. Sci. Rep. 2022, 12, 15094. [Google Scholar] [CrossRef] [PubMed]
- Ganta, A.; Tong, Y.; Boadi, B.I.; Konda, S.R.; Egol, K.A. Microbiome of infected fracture nonunion: Does it affect outcomes? J. Orthop. Sci. 2024, 29, 1270–1273. [Google Scholar] [CrossRef] [PubMed]
- Kong, G.; Zhang, W.; Zhang, S.; Chen, J.; He, K.; Zhang, C.; Yuan, X.; Xie, B. The gut microbiota and metabolite profiles are altered in patients with spinal cord injury. Mol. Brain 2023, 16, 26. [Google Scholar] [CrossRef]
- Li, H.; Fu, J.; Erlong, N.; Li, R.; Xu, C.; Hao, L.; Chen, J.; Chai, W. Characterization of periprosthetic environment microbiome in patients after total joint arthroplasty and its potential correlation with inflammation. BMC Infect. Dis. 2023, 23, 423. [Google Scholar] [CrossRef]
- Liu, F.; Duan, M.; Fu, H.; Zhao, G.; Han, Y.; Lan, F.; Ahmed, Z.; Cao, G.; Li, Z.; Ma, D.; et al. Orthopedic Surgery Causes Gut Microbiome Dysbiosis and Intestinal Barrier Dysfunction in Prodromal Alzheimer Disease Patients: A Prospective Observational Cohort Study. Ann. Surg. 2022, 276, 270–280. [Google Scholar] [CrossRef]
- Cyphert, E.L.; Clare, S.; Dash, A.; Nixon, J.C.; Raphael, J.; Harrison, J.; Heilbronner, A.; Kim, H.J.; Cunningham, M.; Lebl, D.; et al. A pilot study of the gut microbiota in spine fusion surgery patients. HSS J. 2025, 21, 65–72. [Google Scholar] [CrossRef]
- Lin, H.; Liu, T.; Li, X.; Gao, X.; Wu, T.; Li, P. The role of gut microbiota metabolite trimethylamine N-oxide in functional impairment of bone marrow mesenchymal stem cells in osteoporosis disease. Ann. Transl. Med. 2020, 8, 1009. [Google Scholar] [CrossRef]
- Li, J.; Liu, C.; Xu, Y.; Ling, C.; Tang, Z.; Kiram, A.; Hu, Z.; Zhu, Z.; Qiu, Y.; Liu, Z. Gut microbiota alterations in adolescent idiopathic scoliosis are associated with aberrant bone homeostasis. Orthop. Surg. 2024, 16, 965–975. [Google Scholar] [CrossRef]
- Baek, Y.J.; Lee, Y.J.; Lee, J.A.; Kim, S.Y.; Park, J.H.; Choi, H.J.; Lim, J.Y.; Han, S.H.; Park, Y.S.; Kim, Y.H.; et al. Role of α-defensin and the microbiome in prosthetic joint infection: A prospective cohort study in Korea. J. Clin. Med. 2023, 12, 5964. [Google Scholar] [CrossRef]
- Das, M.; Cronin, O.; Keohane, D.M.; Cormac, E.M.; Nugent, H.; Nugent, M.; Molloy, C.; O’Toole, P.W.; Shanahan, F.; Molloy, M.G.; et al. Gut microbiota alterations associated with reduced bone mineral density in older adults. Rheumatology 2019, 58, 2295–2304. [Google Scholar] [CrossRef] [PubMed]
- Ma, S.; Wang, N.; Zhang, P.; Wu, W.; Fu, L. Fecal microbiota transplantation mitigates bone loss by improving gut microbiome composition and gut barrier function in aged rats. PeerJ 2021, 9, e12293. [Google Scholar] [CrossRef]
- Duan, M.; Liu, F.; Fu, H.; Lu, S.; Wang, T. Preoperative Microbiomes and Intestinal Barrier Function Can Differentiate Prodromal Alzheimer’s Disease From Normal Neurocognition in Elderly Patients Scheduled to Undergo Orthopedic Surgery. Front. Cell. Infect. Microbiol. 2021, 11, 592842. [Google Scholar] [CrossRef] [PubMed]
- Bi, J.; Xu, Y.; Li, S.; Zhan, G.; Hua, D.; Tan, J.; Chi, X.; Xiang, H.; Guo, F.; Luo, A. Contribution of preoperative gut microbiota in postoperative neurocognitive dysfunction in elderly patients undergoing orthopedic surgery. Front. Aging Neurosci. 2023, 15, 1108205. [Google Scholar] [CrossRef] [PubMed]
- Roselló-Añón, A.; Chiappe, C.; Valverde-Vázquez, M.R.; Sangüesa-Nebot, M.J.; Gómez-Cabrera, M.C.; Pérez-Martínez, G.; Doménech-Fernández, J. Pilot study to determine the association between gut microbiota and fragility hip fracture. Evista Esp. Cir. Ortop. Traumatol. 2023, 67, 279–289. [Google Scholar] [CrossRef]
- Chen, Y.; Wang, X.; Zhang, C.; Liu, Z.; Li, C.; Ren, Z. Gut Microbiota and Bone Diseases: A Growing Partnership. Front. Microbiol. 2022, 13, 877776. [Google Scholar] [CrossRef]
- Morales, F.; Montserrat-de la Paz, S.; Leon, M.J.; Rivero-Pino, F. Effects of Malnutrition on the Immune System and Infection and the Role of Nutritional Strategies Regarding Improvements in Children’s Health Status: A Literature Review. Nutrients 2024, 16, 1. [Google Scholar] [CrossRef]
- L Bishop, E.; Ismailova, A.; Dimeloe, S.; Hewison, M.; White, J.H. Vitamin D and Immune Regulation: Antibacterial, Antiviral, Anti-Inflammatory. JBMR Plus 2020, 5, e10405. [Google Scholar] [CrossRef]
- Moise, A.; Balescu-Arion, C. Vitamin D and the Immune System. When? Why? How? Cent. Eur. Ann. Clin. Res. 2020, 2, 1. [Google Scholar] [CrossRef]
- Schwalfenberg, G.K. A review of the critical role of vitamin D in the functioning of the immune system and the clinical implications of vitamin D deficiency. Mol. Nutr. Food Res. 2011, 55, 96–108. [Google Scholar] [CrossRef]
- Yan, H.; Chen, Y.; Zhu, H.; Huang, W.H.; Cai, X.H.; Li, D.; Lv, Y.J.; Zhao, -S.; Zhou, H.H.; Luo, F.Y.; et al. The relationship among intestinal bacteria, vitamin K and response of vitamin K antagonist: A review of evidence and potential mechanism. Front. Med. 2022, 9, 829304. [Google Scholar] [CrossRef]
- Conly, J.M.; Stein, K.; Worobetz, L.; Rutledge-Harding, S. The contribution of vitamin K2 (menaquinones) produced by the intestinal microflora to human nutritional requirements for vitamin K. Am. J. Gastroenterol. 1994, 89, 915–923. [Google Scholar]
- Shearer, M.J. Role of vitamin K and Gla proteins in the pathophysiology of osteoporosis and vascular calcification. Curr. Opin. Clin. Nutr. Metab. Care 2000, 3, 433–438. [Google Scholar] [CrossRef]
- Merra, G.; Dominici, F.; Gualtieri, P.; Capacci, A.; Cenname, G.; Esposito, E.; Dri, M.; Di Renzo, L.; Marchetti, M. Role of vitamin K2 in bone-vascular crosstalk. Int. J. Vitam. Nutr. Res. 2024, 94, 143–152. [Google Scholar] [CrossRef]
- Weber, P. Vitamin K and bone health. Nutrition 2001, 17, 880–887. [Google Scholar] [CrossRef]
- Luna, M.; Guss, J.D.; Vasquez-Bolanos, L.S.; Castaneda, M.; Rojas, M.V.; Strong, J.M.; Alabi, D.A.; Dornevil, S.D.; Nixon, J.C.; Taylor, E.A.; et al. Components of the gut microbiome that influence bone tissue-level strength. J. Bone Miner. Res. 2021, 36, 1823–1834. [Google Scholar] [CrossRef]
- George, S.; Leasure, A.R.; Horstmanshof, D. Effectiveness of Decolonization With Chlorhexidine and Mupirocin in Reducing Surgical Site Infections: A Systematic Review. Dimens. Crit. Care Nurs. 2016, 35, 204–222. [Google Scholar] [CrossRef]
- Zukowska, A.; Zukowski, M. Surgical Site Infection in Cardiac Surgery. J. Clin. Med. 2022, 11, 6991. [Google Scholar] [CrossRef]
- Wei, X.; Xing, F.; Xu, Y.; Zhang, F.; Cheng, D.; Zhou, Y.; Zheng, F.; Zhao, J.; Wang, Y.; Chen, L.; et al. Preoperative gut microbiota of POCD patients induces pre- and postoperative cognitive impairment and systemic inflammation in rats. J. Neuroinflamm. 2024, 21, 221. [Google Scholar] [CrossRef]
- Weaver, L.; Troester, A.; Jahansouz, C. The Impact of Surgical Bowel Preparation on the Microbiome in Colon and Rectal Surgery. Antibiotics 2024, 13, 580. [Google Scholar] [CrossRef] [PubMed]
- Bratzler, D.W.; Dellinger, E.P.; Olsen, K.M.; Perl, T.M.; Auwaerter, P.G.; Bolon, M.K.; Fish, D.N.; Napolitano, L.M.; Sawyer, R.G.; Slain, D.; et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Am. J. Health Syst. Pharm. 2013, 70, 195–283. [Google Scholar] [CrossRef] [PubMed]
- Ontario Health (Quality). Pre-surgical Nasal Decolonization of Staphylococcus aureus: A Health Technology Assessment. Ont. Health Technol. Assess. Ser. 2022, 22, 1–165. [Google Scholar]
- Guerrero, M.A.; Anderson, B.; Carr, G.; Snyder, K.L.; Boyle, P.; Ugwu, S.A.; Davis, M.; Bohnenkamp, S.K.; Nfonsam, V.; Riall, T.S. Adherence to a standardized infection reduction bundle decreases surgical site infections after colon surgery: A retrospective cohort study on 526 patients. Patient Saf. Surg. 2021, 15, 15. [Google Scholar] [CrossRef]
- Song, D.W.; Park, B.K.; Suh, S.W.; Lee, S.E.; Kim, J.W.; Park, J.M.; Kim, H.R.; Lee, M.K.; Choi, Y.S.; Kim, B.G.; et al. Bacterial culture and antibiotic susceptibility in patients with acute appendicitis. Int. J. Colorectal Dis. 2018, 33, 441–447. [Google Scholar] [CrossRef]
- Effenberger, M.; Al-Zoairy, R.; Gstir, R.; Graziadei, I.; Schwaighofer, H.; Tilg, H.; Zoller, H. Transmission of oral microbiota to the biliary tract during endoscopic retrograde cholangiography. BMC Gastroenterol. 2023, 23, 103. [Google Scholar] [CrossRef]
- Khoury, F.; Pezzone, M.; Aijazi, M.; Fons, I.; Araujo, D.; Kondaveeti, B.; Ahuja, A.; Yassin, M. Gastrointestinal endoscopy 30-day-associated bacteremia: Nonoutbreak 5-year review in an inner-city, tertiary-care hospital. Am. J. Infect. Control. 2024, 52, 1166–1169. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Selection | Comparability | Outcome | ||
|---|---|---|---|---|---|
| Representativeness of Cohort | Ascertainment of Exposure | Comparability of Cohorts | Assessment of Outcome | Follow Up | |
| (Aboushaal a et al., 2024) [33] | * | * | * | * | * |
| (Chisari et al., 2022) [34] | * | * | * | * | * |
| (Ganta et al., 2023) [35] | * | * | * | * | * |
| (Kong et al., 2023) [36] | * | * | * | * | * |
| (Li et al., 2023) [37] | * | * | * | * | * |
| (Liu et al., 2022) [38] | * | * | * | * | * |
| (Cyphert et al., 2023) [39] | * | * | * | * | * |
| (Lin et al., 2020) [40] | * | * | * | * | * |
| (Li et al., 2024) [41] | * | * | * | * | * |
| (Baek et al., 2023) [42] | * | * | * | * | * |
| (Das et al., 2019) [43] | * | * | * | * | * |
| (Ma et al., 2021) [44] | * | * | * | * | * |
| Study | Was the Research Objective Clearly Stated? | Was the Study Population Clearly Specified and Defined? | Was the Participation Rate of Eligible Persons at Least 50%? | Were All the Subjects Selected or Recruited from the Same or Similar Populations? | Were Effect Estimates Provided? | Were the Outcome Measures Clearly Defined, Valid, Reliable, and Implemented Consistently Across All Study Participants? | Were the Outcome Assessors Blinded to the Exposure Status of Participants? | Were Key Potential Confounding Variables Measured and Adjusted Statistically for Their Impact on the Relationship between Exposures and Outcomes? | Quality Rating |
|---|---|---|---|---|---|---|---|---|---|
| (Duan et al., 2021) [45] | Yes | Yes | Yes | Yes | Yes | Yes | Not mentioned | Not mentioned | Good |
| (Bi et al., 2023) [46] | Yes | Yes | Yes | Yes | Yes | Yes | Not mentioned | Not mentioned | Good |
| (Rosello-A non et al., 2023) [47] | Yes | Yes | Yes | Yes | Yes | Yes | Not mentioned | Not mentioned | Good |
| Authors | Region | Sample Size, Demographics | Study Design | Intervention | Primary Outcomes: Infection Rates, Bone Healing | Secondary Outcomes: Pain, Inflammation, Hospital Stay | Objectives | Findings |
|---|---|---|---|---|---|---|---|---|
| (Abousha ala et al., 2024) [33] | USA | 33 adults (21 with lumbar degenerative spondylolisthesis (LDS) and 12 without LDS), ages 18–80 years | Prospective cohort study | Observational study assessing gut microbiota and spinal health | LDS group shows higher disc degeneration severity (p = 0.018) and altered microbial diversity (p = 0.002–0.0046), with elevated proinflammatory bacteria (Dialister, CAG0352) and reduced anti-inflammatory bacteria (Slackia, Escherichia-Shigella) | No significant differences in pain profiles | To assess the association between gut microbiota dysbiosis and LDS in symptomatic patients. | Gut microbiome dysbiosis is significantly associated with LDS, characterized by higher Firmicutes-to-Bacteroidota ratio (p = 0.003) and shifts in pro-and anti-inflammatory bacterial taxa. |
| (Bi et al., 2023) [46] | China | 40 elderly orthopedic patients | Prospective case-control study | Gut microbiota determined by 16S rRNA MiSeq sequencing | Preoperative gut microbiota composition | Neuropsychological assessments, postoperative pain scores, inflammatory markers, and hospital stay duration | Investigate the role of gut microbiota and metabolites in POCD in elderly orthopedic patients. | Preoperative gut microbiota differences identified in POCD patients; diagnostic efficiency demonstrated in 6 genera via ROC analysis; specific pathways impacting cognition function enriched. |
| (Chisari et al., 2022) [34] | USA | 134 patients | Prospective cohort study | Zonulin, sCD14, LPS | Infection Rates: 44 PJI cases identified | Pain, Inflammation | Investigate the relationship between gut permeability and periprosthetic joint infection (PJI) through Zonulin, sCD14, and LPS biomarkers. | Zonulin and sCD14 were significantly elevated in PJI patients compared to non-infected. Acute PJI showed higher Zonulin levels than chronic PJI. |
| (Duan et al., 2021) [45] | China | 80 patients | Case-control study | Intestinal microbiota using 16S rRNA | IM dysbiosis and barrier dysfunction were observed preoperatively in SCD and aMCI patients; elevated plasma LPS and CRP in SCD patients | Reduced levels of short-chain fatty acids-producing bacteria | Investigate preoperative differences in intestinal microbiota and barrier function in NC, SCD, and aMCI patients. | SCD patients had a lower Chao1 index, higher Bacteroidetes, and elevated plasma LPS/CRP. -aMCI patients exhibited increased Firmicutes and plasma occludin. |
| (Ganta et al., 2023) [35] | USA | 551 adult patients | Retrospective cohort analysis | Culture-directed antibiotic treatment. | Time to fracture union: longer in gram-negative (662.3 days vs. 446.8 in gram-positive) | Number of reoperations, reconstructive surgeries | Assess bacterial microbiome affecting infected nonunions; Evaluate effects of bacterial speciation on fracture healing outcomes. | Gram-negative infections were associated with delayed union compared to gram-positive, though not statistically significant. Staphylococcus species were the most common isolates; reoperation rates were similar between groups. |
| (Kong et al., 2023) [36] | China | 21: 11-spinal cord injury (SCI) and 10-healthy controls | Observational cohort study | Serum metabolites | Gut dysbiosis correlated with metabolic disorders, injury duration, and motor dysfunction severity | To examine changes in gut microbiota and metabolites in SCI patients. Analyze correlations between gut microbiota, metabolites, and clinical parameters. | SCI patients exhibited gut dysbiosis and distinct serum metabolite profiles. Microbial shifts correlated with neurological grade and injury duration. | |
| (Li et al., 2023) [37] | China | 77 patients | Prospective cohort study | Leukocyte esterase | Staphylococcus and Pseudomonas types showed higher inflammatory responses | Diagnostic value of microbiota typing for PJI confirmation | To characterize the periprosthetic microbiota in patients with suspected PJI. | Significant differences in periprosthetic microbiota between PJI and non-PJI groups. |
| (Liu et al., 2022) [38] | China | 135 patients | Prospective observational cohort study | Measurement of gut microbiota, bacterial endotoxin, tight junction proteins. Knee arthroplasty or lumbar fusion. | Microbiota dysbiosis and intestinal barrier dysfunction | Increased level of inflammatory markers (CRP, IL-6, IL-10 levels monitored postoperatively) | To investigate changes in gut microbiota and intestinal barrier function after orthopedic surgery in patients with normal cognition vs. Alzheimer’s disease. | Gut dysbiosis linked with perioperative metabolic stress and inflammation. |
| (Cyphert et al., 2023) [39] | USA | 31 patients undergoing spinal fusion surgery | Observational cohort study | Microbiome composition and bone mineral density (BMD). | Association between gut microbiota composition and bone mineral density (BMD) in spinal fusion patients | No secondary outcomes were specified | To investigate the relationship between microbiome composition and bone health in spinal fusion surgery patients. | A significant difference in microbiota composition between patients with low BMD (T-score ≤ −1.0) and those with normal BMD (p = 0.03). No significant changes in microbiome composition postoperatively. |
| (Han et al., 2024) [30] | China | 100 fracture patients | RCT | Oral administration of Lactobacillus rhamnosus JYLR-127 | Infection Rates: Decreased C-reactive protein level (p = 0.030) | Pain/Inflammation: Decreased abdominal PAC-SYM scores (p < 0.001); reduced inflammatory markers | To assess the efficacy of L. rhamnosus JYLR-127 in alleviating post-surgery constipation, reducing inflammation and improving gastrointestinal health. | Altered gut microbiota: Increased Firmicutes (p < 0.01), decreased Bacteroidetes (p < 0.05). Potential anti-infection and anti-inflammatory effects post-fracture surgery. |
| (Lecomte et al., 2023) [32] | Ireland | 100 postmenopausal women | RCT | 8-prenylarin genin (8-PN) and calcium and vitamin D3 supplements | Bone Healing/BMD: Total body BMD increased significantly in the HE group (1.8 ± 0.4% vs. baseline, p < 0.0001). The proportion of women with ≥ 1% BMD increases higher in the HE group (OR: 2.41, p < 0.05) | Quality of Life: Improvement in SF-36 physical functioning score (p = 0.05) | To assess the effect of an 8-PN standardized hop extract on bone status and understand the role of gut microbiome in postmenopausal osteopenic women. | HE supplementation increased total body BMD, improved physical functioning scores, and altered the abundance of gut microbiota genera. |
| (Lin et al., 2020) [40] | China | 20 patients | Observational cohort study | Serum trimethylamine N-oxide | Elevated trimethylamine N-oxide levels in OP; promoted BMSCs | Increased ROS, IL-1β, IL-6, TNF-α; inhibited BMSCs proliferation activation of NF-κB pathway | To investigate the effect of trimethylamine N-oxide on bone metabolism in OP and elucidate mechanisms underlying these effects. | Elevated trimethylamine N-oxide negatively correlated with BMD in OP; NF-κB activation linked to trimethylamine N-oxide-induced ROS, inflammation, and altered BMSCs differentiation leading to bone loss. |
| (Li et al., 2024) [41] | China | 126 patients | Retrospective cohort study | BMD assessment by DXA scan | OPN group showed elevated serum β-CTX levels, reduced α diversity, altered GM composition | Increased Escherichia-Shigella and Faecalibacterium | To investigate the GM profile in AIS patients with differing BMD and investigate the association between GM, osteopenia, and bone turnover. | Altered GM profile in the OPN group, with reduced diversity and specific genus-level changes; Escherichia-Shigella negatively correlated with femur BMD and positively with β-CTX. |
| (Valido et al., 2024) [31] | Switzerland | 14 | RCT | Multispecies-multistrain probiotic or prebiotic | Decrease inflammatory markers: probiotics led to a decrease in 83% (25/30) of inflammatory markers compared to prebiotics. Increased gut microbiome alpha diversity (Chao1 index higher post-probiotic use) | Increased GIQLI scores post-probiotic (not significant). Enterococcus faecium W54 increased after probiotic use | Investigate the effects of probiotics vs. prebiotics on inflammatory status and gut microbiome composition. | Probiotics showed the potential to reduce inflammation and improve gut microbiome diversity more effectively than prebiotics. |
| (Baek et al., 2023) [42] | Republic of Korea | 37 patients (age: 62–83 years) | Prospective cohort study | Diagnostic analysis using α-defensive (AD), leukocyte esterase (LE) and metagenomic sequencing | Infection Rates 48.6% (18/37) classified as prosthetic joint infection (PJI) | Pain and Inflammation: The PJI group had higher ESR, CRP, synovial WBC, and PMN levels | To evaluate diagnostic biomarkers for PJI and investigate microbiome roles in synovial fluid. | PJI is associated with reduced microbial richness and pro-inflammatory taxa. |
| (Das et al., 2019) [43] | Ireland | 181 participants | Retrospective cohort study | 16S rRNA (V3–V4 region) amplicon sequencing of fecal microbiota | Bone Homeostasis: Altered microbiota associated with reduced bone mineral density (BMD) | Inflammation indirectly inferred via altered microbiota composition | Investigate the relationship between gut microbiota, bone homeostasis, and fracture risk in older adults. | BMD reduction is significantly associated with specific microbiota changes. |
| (Ma et al., 2024) [44] | USA | 770,075 patients | Retrospective cohort study | Exposure history of C. difficile infection within 2 years before THA | Infection Rates: Higher odds of PJI within 2 years post-THA associated with prior C. difficile infection. Risk increased with closer proximity of infection to THA | Not directly assessed | To evaluate the effect of prior C. difficile infection on the risk of PJI following THA and explore proximity-related risk variations. | Prior C. difficile infection is an independent risk factor for PJI (OR: 1.49%, 95% CI: 1.09–2.02). -Closer proximity of C. difficile infection to THA increases PJI risk. |
| (Roselló-Añón et al., 2023) [47] | Spain | 50 elderly patients | Case-control study | Analysis of gut | Elevated levels of Bacteroidales (p < 0.001) and Peptostreptococcales-Tissierellales (p < 0.005) in fracture patients | Alpha diversity indicated higher estimators at the taxonomic class level in fracture patients | To identify associations between gut microbiota composition and fragility of hip fractures in elderly patients. | Specific microbiota patterns were associated with the fragility of hip fractures. |
| Evidence-Based Surgical Interventions | Rationale | Clinical Recommendations | Specific Products/Tests |
|---|---|---|---|
| Probiotic Supplementation | Certain probiotics (Lactobacillus rhamnosus, Bifidobacterium longum, Lactobacillus acidophilus), cognitive dysfunction, systemic inflammation, and surgical site infections. | Use probiotics preoperatively and postoperatively to support gut microbial balance and reduce infection risks. Consider probiotic supplementation in patients receiving broad-spectrum antibiotics to mitigate microbiome disruption. Monitor and educate patients on probiotic use before and after surgery. | (Lactobacillus rhamnosus GG), (Bifidobacterium longum), Saccharomyhces boulardii |
| Prebiotic Supplementation and Fiber-Rich Diets | Prebiotic intake (fermentable fibers) supports SCFA production, which enhances gut barrier integrity and reduces systemic inflammation. | Recommend a high-fiber, prebiotic-rich diet (<30 g/day) at least 2 weeks before surgery Encourage consumption of fermented foods (yogurt, kefir, kimchi, sauerkraut) for microbiome diversity Increase fiber intake through plant-based sources (legumes, whole grains, flaxseeds, leafy greens). | Inulin, Psyllium Husk, Fructooligosaccharides (FOS), Partially Hydrolyzed Guar Gum |
| Microbiome Testing | Testing for markers such as zonulin and soluble CD14 provides insight into gut permeability and inflammation. | Utilize microbiome sequencing to evaluate microbial diversity in high-risk patients. Screen at-risk patients for microbiome-related complications, such as those with recurrent infections, or gastrointestinal issues. | Microbiome sequencing tests Biomarkers: Zonulin (gut permeability), Soluble CD14 (systemic inflammation), Calprotectin (gut inflammation) |
| Targeted Antibiotic Use | Selective use of antibiotics can minimize microbiome disruption and preserve beneficial bacterial populations while preventing infections. | Use narrow-spectrum antibiotics when clinically appropriate to preserve gut microbiota. Consider microbiome-sparing antibiotics for prolonged perioperative prophylaxis. Monitor patients for antibiotic-induced dysbiosis and recommend probiotic co-administration where indicated. | Various microbiome sparing antibiotics |
| Gut Barrier Protection Strategies | Strategies like perioperative enteral nutrition help maintain gut integrity and prevent bacterial translocation, reducing infection risks. | Avoid prolonged fasting and ensure early enteral nutrition in critically ill patients. Reduce reliance on total parenteral nutrition when possible to maintain gut microbiome stability. Encourage hydration and electrolyte balance to support intestinal barrier function. | Immunonutrition Formulas (arginine, omega-3s, nucleotides) |
| Authors | Study | Year | Surgical Context | Microbiome Focus | Main Findings | Clinical Relevance |
|---|---|---|---|---|---|---|
| (Wei et al., 2024) [61] | Preoperative gut microbiota of POCD patients induces pre- and postoperative cognitive impairment and systemic inflammation in rats | 2024 | Orthopaedic surgery | Analyzing the preoperative gut microbiota of patients with postoperative cognitive dysfunction (POCD). | The gut microbiota of POCD patients exhibited dysbiosis preoperatively | Targeting the microbiota preoperatively could improve postoperative cognitive function. |
| (Guerrero et al., 2021) [65] | Adherence to a standardized infection reduction bundle decreases surgical site infections after colon surgery: a retrospective cohort study on 526 patients | 2016–2017 | Colon Surgery | Emphasis on minimizing colon surgical site infections (SSI), indirectly impacting microbiome balance. | Implementing a perioperative SSI prevention bundle lowered SSI rates from 8.7% to 1.2%. Standard infection rate was reduced by 85.4% after introducing the prevention bundle | Advocates for implementing standardized SSI prevention bundles to improve patient safety and decrease infection rates in colon surgery. |
| (Song et al., 2018) [66] | Bacterial culture and antibiotic susceptibility in patients with acute appendicitis | 2006–2015 | Appendectomy for acute appendicitis | Detection of pathogens in appendicitis and their antibiotic resistance profiles. | Escherichia coli (64.6%) and Pseudomonas aeruginosa (16.4%) were the most common microorganisms for SSI. Pseudomonas aeruginosa was a significant microorganism associated with SSI (OR = 2.128, 95% CI = 1.077–4.206, p = 0.030) | Emphasizes the need for proper empirical antibiotic selection, particularly for P. aeruginosa infections, to minimize postoperative complications. |
| (Effenberger et al., 2023) [67] | Transmission of oral microbiota to the biliary tract during endoscopic retrograde cholangiography | 2010–2011 | Endoscopic retrograde cholangiography (ERC) | Microbial contamination of bile from the oral cavity and endoscopic equipment. | Bacteroides fragilis was significantly associated with cholangitis (p = 0.015). Microbial translocation from the throat and endoscope to bile was common, clinical outcomes not affected | Microbial contamination during ERC is frequent; it does not necessarily lead to adverse patient outcomes. |
| (Khoury et al., 2024) [68] | Gastrointestinal endoscopy 30-day-associated bacteremia: Nonoutbreak 5-year review in an inner-city, tertiary-care hospital | 2018–2022 | Gastrointestinal endoscopic procedures (GIEPs) | Incidence and associated factors of bacteremia associated with GIEPs. | Bacteremia rate was highest after endoscopic retrograde cholangiopancreatography (2.84%) and lowest after colonoscopy (0.08%) | Emphasizes the importance of clinical surveillance to reduce infection risk after GIEPs. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nadeem-Tariq, A.; Kazemeini, S.; Michelberger, M.; Fang, C.; Maitra, S.; Nelson, K. The Role of Gut Microbiota in Orthopedic Surgery: A Systematic Review. Microorganisms 2025, 13, 1048. https://doi.org/10.3390/microorganisms13051048
Nadeem-Tariq A, Kazemeini S, Michelberger M, Fang C, Maitra S, Nelson K. The Role of Gut Microbiota in Orthopedic Surgery: A Systematic Review. Microorganisms. 2025; 13(5):1048. https://doi.org/10.3390/microorganisms13051048
Chicago/Turabian StyleNadeem-Tariq, Ahmed, Sarah Kazemeini, Matthew Michelberger, Christopher Fang, Sukanta Maitra, and Karen Nelson. 2025. "The Role of Gut Microbiota in Orthopedic Surgery: A Systematic Review" Microorganisms 13, no. 5: 1048. https://doi.org/10.3390/microorganisms13051048
APA StyleNadeem-Tariq, A., Kazemeini, S., Michelberger, M., Fang, C., Maitra, S., & Nelson, K. (2025). The Role of Gut Microbiota in Orthopedic Surgery: A Systematic Review. Microorganisms, 13(5), 1048. https://doi.org/10.3390/microorganisms13051048