
Herpesvirus Infections of the Corneal Endothelium

 , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Methods
3. Results
3.1. Cytomegalovirus (CMV)
3.1.1. Epidemiology and Pathophysiology of CMV Endotheliitis
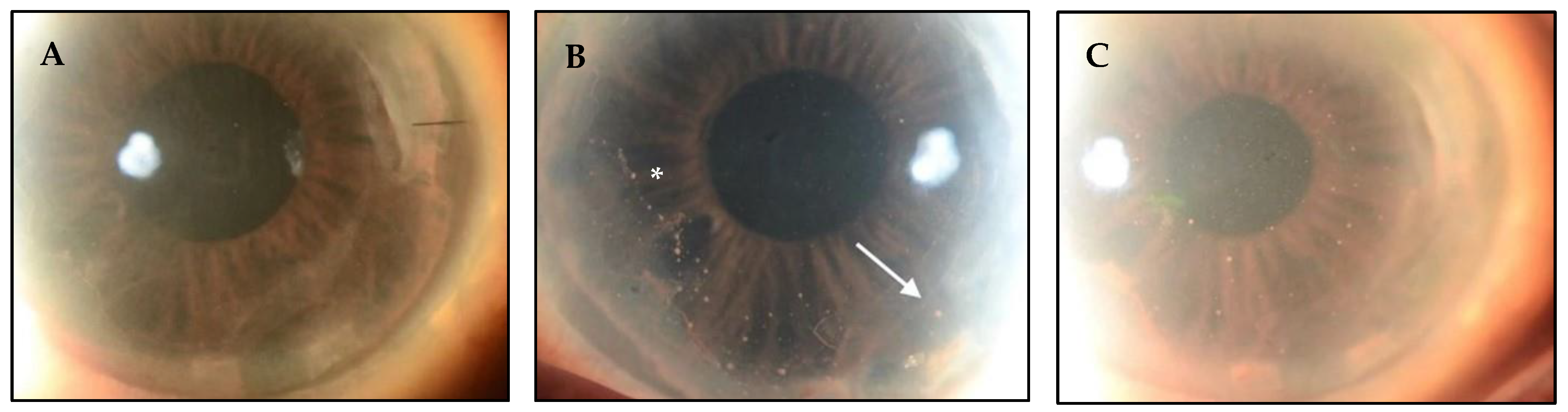
3.1.2. Clinical Manifestations of CMV Endotheliitis
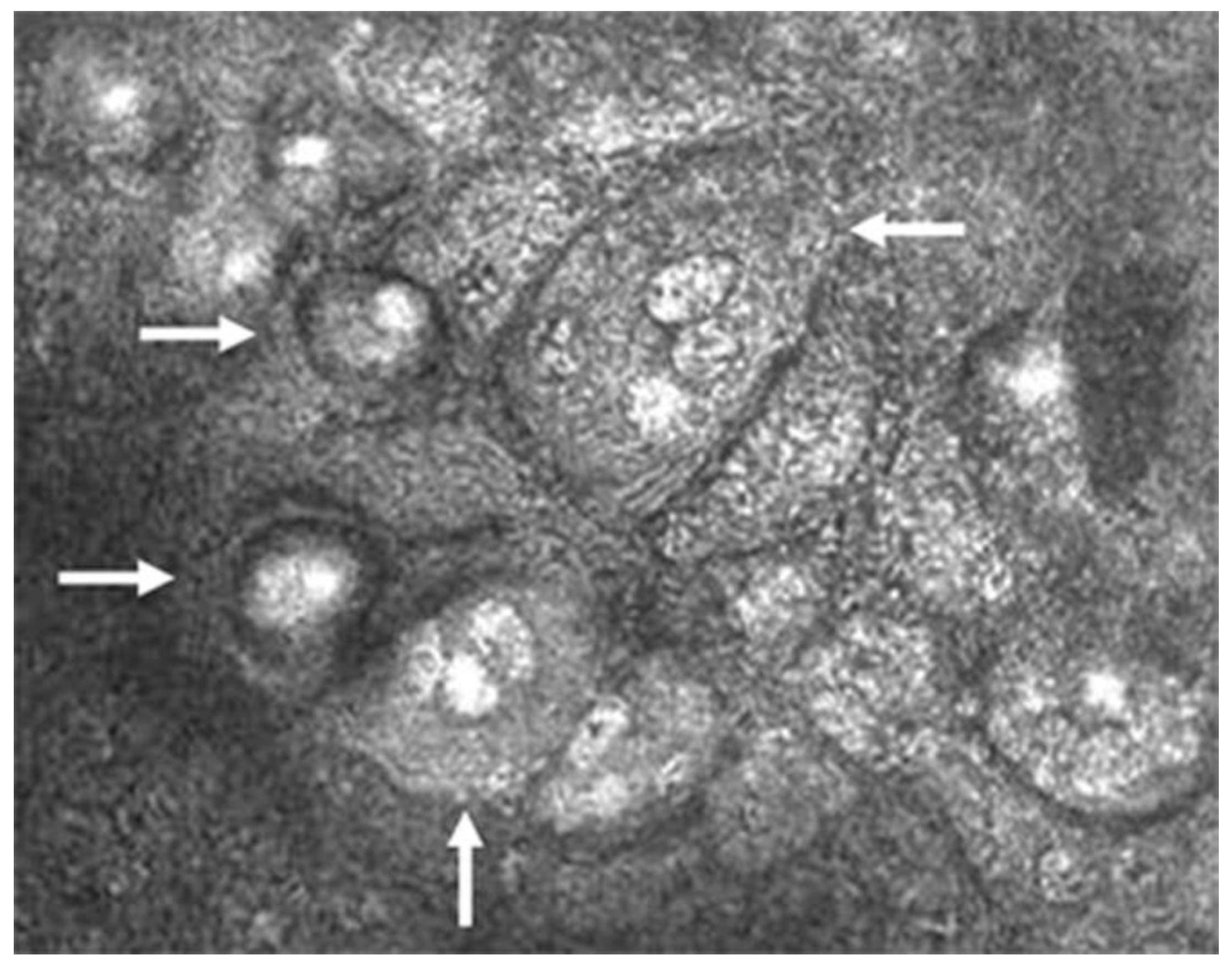
3.1.3. Diagnostic Techniques of CMV Endotheliitis
3.1.4. Treatment of CMV Endotheliitis
3.2. Varicella Zoster Virus (VZV)
3.2.1. Epidemiology and Pathophysiology of VZV Endotheliitis
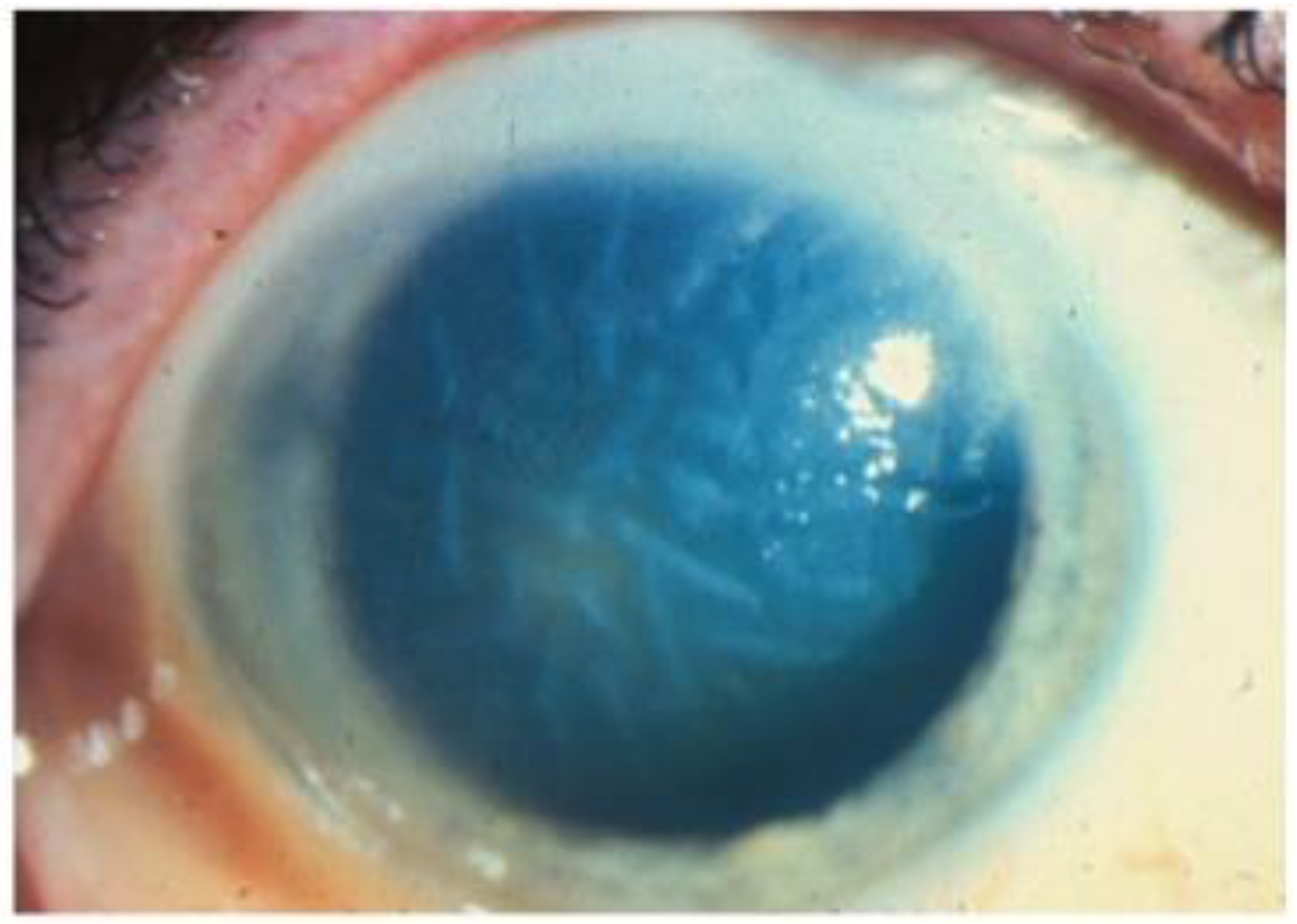
3.2.2. Clinical Manifestations of VZV Endotheliitis
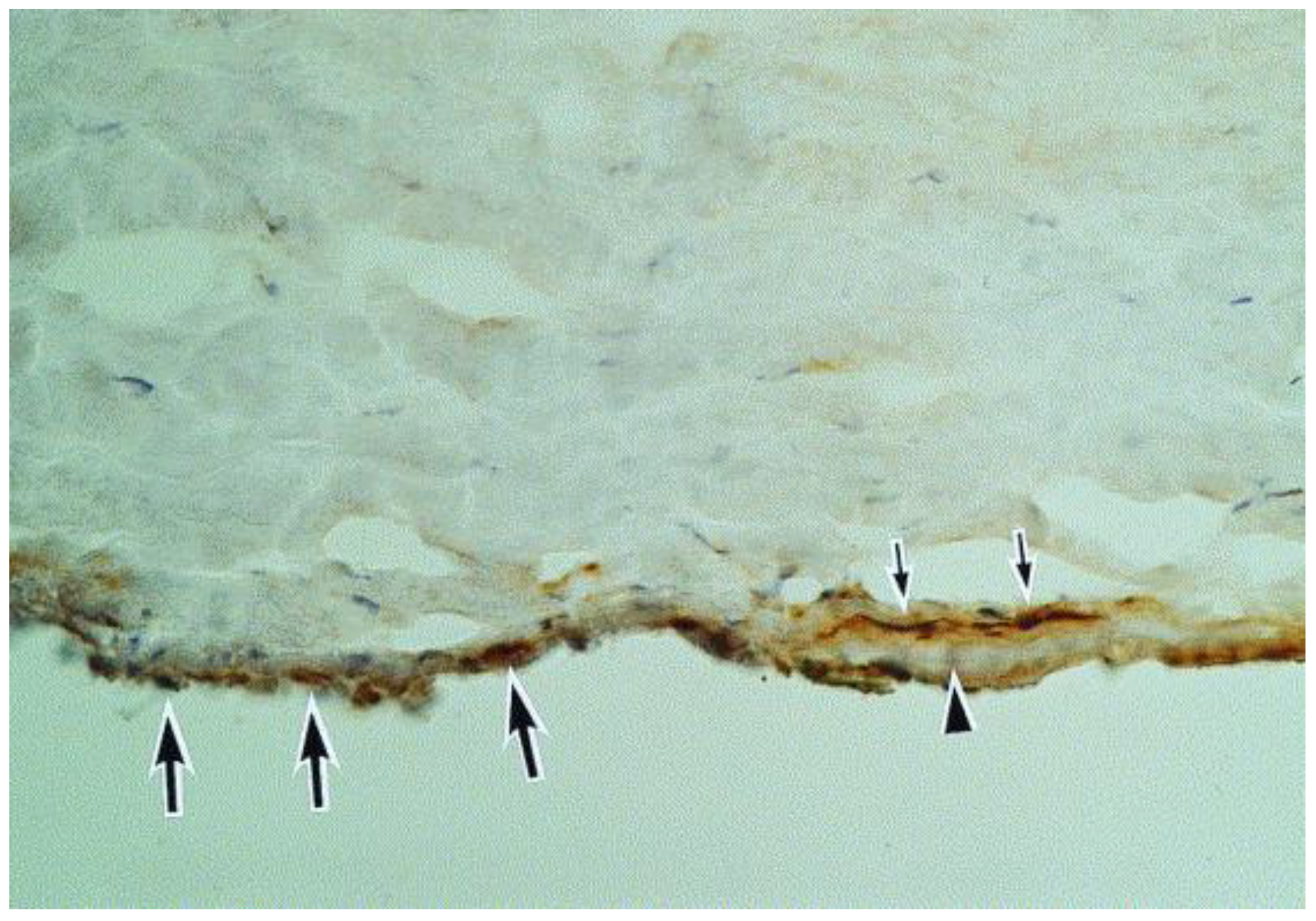
3.2.3. Diagnostic Techniques of VZV Endotheliitis
3.2.4. Treatment of VZV Endotheliitis
3.3. Herpes Simplex Virus (HSV)
3.3.1. Epidemiology and Pathophysiology of HSV Endotheliitis
3.3.2. Clinical Manifestations of HSV Endotheliitis
3.3.3. Diagnostic Techniques of HSV Endotheliitis
3.3.4. Treatment of HSV Endotheliitis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moshirfar, M.; Murri, M.S.; Shah, T.J.; Skanchy, D.F.; Tuckfield, J.Q.; Ronquillo, Y.C.; Birdsong, O.C.; Hofstedt, D.; Hoopes, P.C. A review of corneal endotheliitis and endotheliopathy: Differential diagnosis, evaluation, and treatment. Ophthalmol. Ther. 2019, 8, 195–213. [Google Scholar] [PubMed]
- Alfawaz, A. Cytomegalovirus-related corneal endotheliitis: A review article. Saudi J. Ophthalmol. 2013, 27, 47–49. [Google Scholar] [PubMed]
- Pepose, J.S.; Keadle, T.L.; Morrison, L.A. Ocular herpes simplex: Changing epidemiology, emerging disease patterns, and the potential of vaccine prevention and therapy. Am. J. Ophthalmol. 2006, 141, 547–557.e2. [Google Scholar] [PubMed]
- Xu, F.; Sternberg, M.R.; Kottiri, B.J.; McQuillan, G.M.; Lee, F.K.; Nahmias, A.J.; Berman, S.M.; Markowitz, L.E. Trends in herpes simplex virus type 1 and type 2 seroprevalence in the United States. JAMA 2006, 296, 964–973. [Google Scholar]
- Inoue, Y. Review of clinical and basic approaches to corneal endotheliitis. Cornea 2014, 33, S3–S8. [Google Scholar]
- Suzuki, T.; Ohashi, Y. (Eds.) Corneal endotheliitis. In Seminars in Ophthalmology; Taylor & Francis: Abingdon, UK, 2008. [Google Scholar]
- Singh, K.; Sodhi, P.K. Mumps-induced corneal endotheliitis. Cornea 2004, 23, 400–402. [Google Scholar] [CrossRef]
- Rouhbakhshzaeri, M.; Rabiee, B.; Azar, N.; Ghahari, E.; Putra, I.; Eslani, M.; Djalilian, A.R. New ex vivo model of corneal endothelial phacoemulsification injury and rescue therapy with mesenchymal stromal cell secretome. J. Cataract Refract. Surg. 2019, 45, 361–366. [Google Scholar]
- Cannon, M.J.; Schmid, D.S.; Hyde, T.B. Review of cytomegalovirus seroprevalence and demographic characteristics associated with infection. Rev. Med. Virol. 2010, 20, 202–213. [Google Scholar]
- Koizumi, N.; Inatomi, T.; Suzuki, T.; Shiraishi, A.; Ohashi, Y.; Kandori, M.; Miyazaki, D.; Inoue, Y.; Soma, T.; Nishida, K.; et al. Clinical features and management of cytomegalovirus corneal endotheliitis: Analysis of 106 cases from the Japan corneal endotheliitis study. Br. J. Ophthalmol. 2015, 99, 54–58. [Google Scholar]
- Kumar, A.; Mehta, J.S. Diagnosis and Management of CMV Endotheliitis. Curr. Ophthalmol. Rep. 2019, 7, 98–109. [Google Scholar]
- Schottstedt, V.; Blümel, J.; Burger, R.; Drosten, C.; Gröner, A.; Gürtler, L.; Heiden, M.; Hildebrandt, M.; Jansen, B.; Montag-Lessing, T.; et al. Human Cytomegalovirus (HCMV)—Revised. Transfus. Med. Hemother. 2010, 37, 365–375. [Google Scholar] [PubMed]
- Maier, A.-K.; Gundlach, E.; Gonnermann, J.; Klamann, M.; Bertelmann, E.; Rieck, P.; Joussen, A.M.; Torun, N. Retrospective contralateral study comparing Descemet membrane endothelial keratoplasty with Descemet stripping automated endothelial keratoplasty. Eye 2015, 29, 327–332. [Google Scholar] [PubMed]
- Kitazawa, K.; Jongkhajornpong, P.; Inatomi, T.; Koizumi, N.; Kayukawa, K.; Wakimasu, K.; Sotozono, C.; Kinoshita, S. Topical ganciclovir treatment post-Descemet’s stripping automated endothelial keratoplasty for patients with bullous keratopathy induced by cytomegalovirus. Br. J. Ophthalmol. 2018, 102, 1293–1297. [Google Scholar] [PubMed]
- Hillenaar, T.; Weenen, C.; Wubbels, R.J.; Remeijer, L. Endothelial involvement in herpes simplex virus keratitis: An in vivo confocal microscopy study. Ophthalmology 2009, 116, 2077–2086.e2. [Google Scholar]
- Bronner, A. The pathogens of corneal infection: Know your enemy. Rev. Optom. 2014, 151, 68–80. [Google Scholar]
- Zarei-Ghanavati, S.; Alizadeh, R.; Yoo, S.H. Herpes simplex virus endotheliitis following Descemet’s membrane endothelial keratoplasty. J. Ophthalmic Vis. Res. 2015, 10, 184. [Google Scholar] [CrossRef]
- Murthy, S.I.; Sangwan, V.S.; Tejwani, S.; Atmanathan, S.; Rao, G.N. Manifestations of Progressive Herpes Simplex Virus Endotheliitis. Asian J. Ophthalmol. 2007, 9, 76–81. [Google Scholar]
- Zhu, L.; Zhu, H. Ocular herpes: The pathophysiology, management and treatment of herpetic eye diseases. Virol. Sin. 2014, 29, 327–342. [Google Scholar] [CrossRef]
- Carrillo-Arroyo, I.; Gutierrez-Diaz, E.; Mencia-Gutierrez, E.; Gomez-Perez, P.; Montero-Rodriguez, M. Herpetic endotheliitis and trabeculitis with delayed corneal involvement. Arch. Soc. Esp. Oftalmol. (Engl. Ed.) 2012, 87, 47–49. [Google Scholar]
- Ahmad, F.; Deshmukh, N.; Webel, A.; Johnson, S.; Suleiman, A.; Mohan, R.R.; Fraunfelder, F.; Singh, P.K. Viral infections and pathogenesis of glaucoma: A comprehensive review. Clin. Microbiol. Rev. 2023, 36, e0005723. [Google Scholar]
- Kakimaru-Hasegawa, A.; Kuo, C.-H.; Komatsu, N.; Komatsu, K.; Miyazaki, D.; Inoue, Y. Clinical application of real-time polymerase chain reaction for diagnosis of herpetic diseases of the anterior segment of the eye. Jpn. J. Ophthalmol. 2008, 52, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Guda, S.J.M.; Sontam, B.; Bagga, B.; Ranjith, K.; Sharma, S.; Joseph, J. Evaluation of multiplex real-time polymerase chain reaction for the detection of herpes simplex virus-1 and 2 and varicella-zoster virus in corneal cells from normal subjects and patients with keratitis in India. Indian J. Ophthalmol. 2019, 67, 1040. [Google Scholar]
- Corey, L.; Huang, M.L.; Selke, S.; Wald, A. Differentiation of herpes simplex virus types 1 and 2 in clinical samples by a real-time taqman PCR assay. J. Med. Virol. 2005, 76, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, M.; Deai, T.; Hibino, T.; Higaki, S.; Hayashi, K.; Shimomura, Y. Quantitative analysis of herpes simplex virus genome in tears from patients with herpetic keratitis. Cornea 2003, 22, S55–S60. [Google Scholar] [CrossRef]
- Shoji, J.; Sakimoto, T.; Inada, N.; Kamei, Y.; Matsubara, M.; Takamura, E.; Sawa, M. A diagnostic method for herpes simplex keratitis by simultaneous measurement of viral DNA and virus-specific secretory IgA in tears: An evaluation. Jpn. J. Ophthalmol. 2016, 60, 294–301. [Google Scholar] [CrossRef]
- Das, S.; D’Souza, S.; Gorimanipalli, B.; Shetty, R.; Ghosh, A.; Deshpande, V. Ocular Surface Infection Mediated Molecular Stress Responses: A Review. Int. J. Mol. Sci. 2022, 23, 3111. [Google Scholar] [CrossRef]
- Kaye, S.B.; Baker, K.; Bonshek, R.; Maseruka, H.; Grinfeld, E.; Tullo, A.; Easty, D.L.; Hart, C.A. Human herpesviruses in the cornea. Br. J. Ophthalmol. 2000, 84, 563–571. [Google Scholar] [CrossRef] [PubMed]
- Lobo, A.-M.; Agelidis, A.M.; Shukla, D. Pathogenesis of herpes simplex keratitis: The host cell response and ocular surface sequelae to infection and inflammation. Ocul. Surf. 2019, 17, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Chodosh, J.; Ung, L. Adoption of Innovation in Herpes Simplex Virus Keratitis. Cornea 2020, 39 (Suppl. 1), S7–S18. [Google Scholar] [CrossRef]
- Friehmann, A.; Myerscough, J.; Giannaccare, G.; Mazzoni, M.; Bovone, C.; Busin, M. Successful descemet membrane endothelial keratoplasty in proven herpetic endothelial decompensation requires intensive antiviral therapy. Cornea 2020, 39, 196–199. [Google Scholar] [CrossRef]
- Singh, A.; Zarei-Ghanavati, M.; Avadhanam, V.; Liu, C. Systematic review and meta-analysis of clinical outcomes of Descemet membrane endothelial keratoplasty versus Descemet stripping endothelial keratoplasty/Descemet stripping automated endothelial keratoplasty. Cornea 2017, 36, 1437–1443. [Google Scholar]
- Chee, S.-P.; Bacsal, K.; Jap, A.; Se-Thoe, S.-Y.; Cheng, C.L.; Tan, B.H. Corneal endotheliitis associated with evidence of cytomegalovirus infection. Ophthalmology 2007, 114, 798–803. [Google Scholar]
- Chee, S.-P.; Jap, A. Presumed fuchs heterochromic iridocyclitis and Posner-Schlossman syndrome: Comparison of cytomegalovirus-positive and negative eyes. Am. J. Ophthalmol. 2008, 146, 883–889.e1. [Google Scholar]
- Jap, A.; Chee, S.-P. Cytomegalovirus-associated anterior segment infection. Expert Rev. Ophthalmol. 2011, 6, 517–528. [Google Scholar]
- Shahrudin, N.A.; Zahidin, A.Z.M.; Noh, U.K.M.; Halim, W.H.W.A.; Din, N.M. CMV endotheliitis: A cause for recurrent failed corneal transplant. GMS Ophthalmol. Cases 2017, 7, Doc31. [Google Scholar]
- Foster, C.S.; Vitale, A.T. Diagnosis & Treatment of Uveitis; JP Medical Ltd.: London, UK, 2013. [Google Scholar]
- Anwar, Z.; Galor, A.; Albini, T.A.; Miller, D.; Perez, V.; Davis, J.L. The diagnostic utility of anterior chamber paracentesis with polymerase chain reaction in anterior uveitis. Am. J. Ophthalmol. 2013, 155, 781–786.e2. [Google Scholar] [CrossRef] [PubMed]
- Relvas, L.J.M.; Antoun, J.; de Groot-Mijnes, J.D.; Motulsky, E.; Ten Dam-Van Loon, N.H.; Makhoul, D.; Willermain, F.; Caspers, L. Diagnosis of cytomegalovirus anterior uveitis in two European referral centers. Ocul. Immunol. Inflamm. 2018, 26, 116–121. [Google Scholar]
- Shiraishi, A.; Hara, Y.; Takahashi, M.; Oka, N.; Yamaguchi, M.; Suzuki, T.; Uno, T.; Ohashi, Y. Demonstration of “owl’s eye” morphology by confocal microscopy in a patient with presumed cytomegalovirus corneal endotheliitis. Am. J. Ophthalmol. 2007, 143, 715–717. [Google Scholar]
- Kobayashi, R.; Hashida, N.; Soma, T.; Koh, S.; Miki, A.; Usui, S.; Maeda, N.; Nishida, K. Clinical findings of anterior segment spectral domain optical coherence tomography images in cytomegalovirus corneal endotheliitis. Cornea 2016, 36, 411–414. [Google Scholar] [CrossRef]
- Yoo, W.S.; Kwon, L.H.; Eom, Y.; Thng, Z.X.; Or, C.; Nguyen, Q.D.; Kim, S.J. Cytomegalovirus Corneal Endotheliitis: A Comprehensive Review. Ocul. Immunol. Inflamm. 2024, 32, 2228–2237. [Google Scholar] [CrossRef]
- Fan, N.-W.; Chung, Y.-C.; Liu, Y.-C.; Liu, C.J.-L.; Kuo, Y.-S.; Lin, P.-Y. Long-term topical ganciclovir and corticosteroids preserve corneal endothelial function in cytomegalovirus corneal endotheliitis. Cornea 2016, 35, 596–601. [Google Scholar]
- Gilbert, C.; Boivin, G. Human cytomegalovirus resistance to antiviral drugs. Antimicrob. Agents Chemother. 2005, 49, 873–883. [Google Scholar]
- Hwang, J.-H.; Ha, M.; Park, Y.; Chung, S.-H. The effect of topical ganciclovir and corticosteroid on cytomegalovirus corneal endotheliitis in Korean patients. Ocul. Immunol. Inflamm. 2019, 27, 338–344. [Google Scholar]
- Strasfeld, L.; Lee, I.; Tatarowicz, W.; Villano, S.; Chou, S. Virologic characterization of multidrug-resistant cytomegalovirus infection in 2 transplant recipients treated with maribavir. J. Infect. Dis. 2010, 202, 104–108. [Google Scholar]
- Koizumi, N.; Miyazaki, D.; Inoue, T.; Ohtani, F.; Kandori-Inoue, M.; Inatomi, T.; Sotozono, C.; Nakagawa, H.; Horikiri, T.; Ueta, M.; et al. The effect of topical application of 0.15% ganciclovir gel on cytomegalovirus corneal endotheliitis. Br. J. Ophthalmol. 2017, 101, 114–119. [Google Scholar]
- Cho, A.-R.; Hong, S.-U. A case report of alopecia treated by Gagamsunbangpaedok-tang (Jiājiǎnxiānfángbàidú-tāng)-focused on multi-patched alopecia Areata with lymphadenopathy. J. Korean Med. Ophthalmol. Otolaryngol. Dermatol. 2014, 27, 130–139. [Google Scholar]
- Basilious, A.; Chew, H.F. Topical ganciclovir for prophylaxis of cytomegalovirus endotheliitis in endothelial keratoplasty. Cornea 2019, 38, 120–122. [Google Scholar]
- Yu, T.; Peng, R.-M.; Xiao, G.-G.; Feng, L.-N.; Hong, J. Clinical evaluation of intravitreal injection of ganciclovir in refractory corneal endotheliitis. Ocul. Immunol. Inflamm. 2020, 28, 270–280. [Google Scholar]
- Kaufman, A.R.; Kaufman, A.H. Pediatric herpes virus anterior segment infections. In Practical Management of Pediatric Ocular Disorders and Strabismus; Springer: Berlin/Heidelberg, Germany, 2016; pp. 119–128. [Google Scholar]
- Khodabande, A. Varicella endotheliitis: A case report. Eur. J. Ophthalmol. 2009, 19, 1076–1078. [Google Scholar]
- De Freitas, D.; Sato, E.H.; Kelly, L.D.; Pavan-Langston, D. Delayed onset of varicella keratitis. Cornea 1992, 11, 471–474. [Google Scholar]
- Li, J.Y. Herpes zoster ophthalmicus: Acute keratitis. Curr. Opin. Ophthalmol. 2018, 29, 328–333. [Google Scholar]
- De Castro, L.E.F.; Al Sarraf, O.; Hawthorne, K.M.; Solomon, K.D.; Vroman, D.T. Ocular manifestations after primary varicella infection. Cornea 2006, 25, 866–867. [Google Scholar]
- Arvin, A.M. (Ed.) Antiviral therapy for varicella and herpes zoster. In Seminars in Pediatric Infectious Diseases; Elsevier: Amsterdam, The Netherlands, 2002. [Google Scholar]
- Colin, J.; Prisant, O.; Cochener, B.; Lescale, O.; Rolland, B.; Hoang-Xuan, T. Comparison of the efficacy and safety of valaciclovir and acyclovir for the treatment of herpes zoster ophthalmicus. Ophthalmology 2000, 107, 1507–1511. [Google Scholar] [PubMed]
- Kaufman, S.C. Anterior segment complications of herpes zoster ophthalmicus. Ophthalmology 2008, 115, S24–S32. [Google Scholar]
- Liesegang, T.J. Herpes zoster ophthalmicus: Natural history, risk factors, clinical presentation, and morbidity. Ophthalmology 2008, 115, S3–S12. [Google Scholar]
- Morishige, N.; Morita, Y.; Yamada, N.; Sonoda, K.-H. Differential changes in intraocular pressure and corneal manifestations in individuals with viral endotheliitis after keratoplasty. Cornea 2016, 35, 602–606. [Google Scholar] [PubMed]
- Kedar, S.; Jayagopal, L.N.; Berger, J.R. Neurological and ophthalmological manifestations of varicella zoster virus. J. Neuro-Ophthalmol. 2019, 39, 220–231. [Google Scholar]
- Sauerbrei, A. Diagnosis, antiviral therapy, and prophylaxis of varicella-zoster virus infections. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 723–734. [Google Scholar]
- Cohen, J.I. Clinical practice: Herpes zoster. N. Engl. J. Med. 2013, 369, 255–263. [Google Scholar]
- Otani, N.; Tanaka, M.; Maeda, K.; Gomi, Y.; Nakajima, K.; Tanimura, S.; Takesue, Y.; Shima, M.; Okuno, T. Varicella zoster virus antibody detection: A comparison of four commonly used techniques. J. Infect. Chemother. 2016, 22, 225–228. [Google Scholar]
- Breuer, J.; Schmid, D.S.; Gershon, A.A. Use and limitations of varicella-zoster virus-specific serological testing to evaluate breakthrough disease in vaccinees and to screen for susceptibility to varicella. J. Infect. Dis. 2008, 197 (Suppl. 2), S147–S151. [Google Scholar]
- Tuft, S. How to manage herpes zoster ophthalmicus. Community Eye Health 2020, 33, 71. [Google Scholar]
- Voelker, R. Increasing cases of Shingles in the eye raise key questions. JAMA 2019, 322, 712–714. [Google Scholar] [CrossRef]
- Borkar, D.S.; Tham, V.M.; Esterberg, E.; Ray, K.J.; Vinoya, A.C.; Parker, J.V.; Uchida, A.; Acharya, N.R. Incidence of herpes zoster ophthalmicus: Results from the Pacific Ocular Inflammation Study. Ophthalmology 2013, 120, 451–456. [Google Scholar]
- Tran, K.D.; Falcone, M.M.; Choi, D.S.; Goldhardt, R.; Karp, C.L.; Davis, J.L.; Galor, A. Epidemiology of herpes zoster ophthalmicus: Recurrence and chronicity. Ophthalmology 2016, 123, 1469–1475. [Google Scholar]
- Rousseau, A.; Bourcier, T.; Colin, J.; Labetoulle, M. Herpes Zoster Ophthalmicus–Diagnosis and Management. US Ophthalmic Rev. 2013, 6, 119–124. [Google Scholar]
- Al Somali, A.I.; Otaif, W. Concomitant Varicella Zoster Virus and Cytomegalovirus Corneal Endotheliitis in an Immunocompetent Patient. Ocul. Immunol. Inflamm. 2020, 30, 638–640. [Google Scholar]
- Wu, W.; Jiang, H.; Zhang, Y.; Zhou, Y.; Bai, G.; Shen, L.; Zhou, H.; Chen, X.; Hu, L. Clinical Metagenomic Next-Generation Sequencing for Diagnosis of Secondary Glaucoma in Patients with Cytomegalovirus-Induced Corneal Endotheliitis. Front. Microbiol. 2022, 13, 940818. [Google Scholar]
- Abdelmassih, Y.; Dubrulle, P.; Sitbon, C.; El-Khoury, S.; Guindolet, D.; Doan, S.; Labetoulle, M.; Cochereau, I.; Gabison, E.E. Therapeutic Challenges and Prognosis of Descemet’s Membrane Endothelial Keratoplasty in Herpes Simplex Eye Disease. Cornea 2019, 38, 553–558. [Google Scholar] [CrossRef]
- Sonoyama, H.; Araki-Sasaki, K.; Osakabe, Y.; Nakamura, M.; Amano, S.; Koizumi, N.; Kinoshita, S.; Ideta, H. Detection of cytomegalovirus DNA from cytomegalovirus corneal endotheliitis after penetrating keratoplasty. Cornea 2010, 29, 683–685. [Google Scholar]
- Matar, C.; Seitz, B.; Daas, L. Rezidivierendes DMEK-Versagen [Recurrent DMEK failure]. Ophthalmologe 2021, 118, 719–723. (In German) [Google Scholar]
- Anshu, A.; Chee, S.P.; Mehta, J.S.; Tan, D.T. Cytomegalovirus endotheliitis in Descemet’s stripping endothelial keratoplasty. Ophthalmology 2009, 116, 624–630. [Google Scholar]
- Sakai, J.I.; Usui, Y.; Suzuki, J.; Kezuka, T.; Goto, H. Clinical features of anterior uveitis caused by three different herpes viruses. Int. Ophthalmol. 2019, 39, 2785–2795. [Google Scholar]
- Liesegang, T.J. Biology and molecular aspects of herpes simplex and varicella-zoster virus infections. Ophthalmology 1992, 99, 781–799. [Google Scholar]
- Valerio, G.S.; Lin, C.C. Ocular manifestations of herpes simplex virus. Curr. Opin. Ophthalmol. 2019, 30, 525–531. [Google Scholar]
- Sinzger, C. Entry route of HCMV into endothelial cells. J. Clin. Virol. 2008, 41, 174–179. [Google Scholar]
- Wang, D.; Yu, Q.C.; Schröer, J.; Murphy, E.; Shenk, T. Human cytomegalovirus uses two distinct pathways to enter retinal pigmented epithelial cells. Proc. Natl. Acad. Sci. USA 2007, 104, 20037–20042. [Google Scholar]
- Farooq, A.V.; Valyi-Nagy, T.; Shukla, D. Mediators and mechanisms of herpes simplex virus entry into ocular cells. Curr. Eye Res. 2010, 35, 445–450. [Google Scholar]
- Reynolds, M.A. Varicella seroprevalence in the U.S.: Data from the National Health and Nutrition Examination Survey, 1999–2004. Public Health Rep. 2010, 125, 860–869. [Google Scholar]
- Schmader, K. Herpes Zoster. Clin. Geriatr. Med. 2016, 32, 539–553. [Google Scholar]
- Kawai, K. Increasing Incidence of Herpes Zoster Over a 60-year Period from a Population-based Study. Clin. Infect. Dis. 2016, 63, 221–226. [Google Scholar] [CrossRef]
- Yawn, B.P. Herpes zoster eye complications: Rates and trends. Mayo Clin. Proc. 2013, 88, 562–570. [Google Scholar] [CrossRef]
- Chan, A.Y. Factors associated with age of onset of herpes zoster ophthalmicus. Cornea 2015, 34, 535–540. [Google Scholar] [CrossRef]
- Gilden, D.; Nagel, M.A.; Cohrs, R.J. Varicella-zoster. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2014; Volume 123, pp. 265–283. [Google Scholar]
- Gilden, D.; Mahalingam, R.; Nagel, M.A.; Pugazhenthi, S.; Cohrs, R.J. Review: The neurobiology of varicella zoster virus infection. Neuropathol. Appl. Neurobiol. 2011, 37, 441–463. [Google Scholar] [CrossRef]
- Young, R.C.; Hodge, D.O.; Liesegang, T.J.; Baratz, K.H. Incidence, recurrence, and outcomes of herpes simplex virus eye disease in Olmsted County, Minnesota, 1976–2007: The effect of oral antiviral prophylaxis. Arch. Ophthalmol. 2010, 128, 1178–1183. [Google Scholar] [CrossRef]
- Kennedy, D.P.; Clement, C.; Arceneaux, R.L.; Bhattacharjee, P.S.; Huq, T.S.; Hill, J.M. Ocular herpes simplex virus type 1: Is the cornea a reservoir for viral latency or a fast pit stop? Cornea 2011, 30, 251–259. [Google Scholar] [CrossRef]
- Kobayashi, R.; Hashida, N. Overview of Cytomegalovirus Ocular Diseases: Retinitis, Corneal Endotheliitis, and Iridocyclitis. Viruses 2024, 16, 1110. [Google Scholar] [CrossRef]
- Kim, J.H.; Collins-McMillen, D.; Buehler, J.C.; Goodrum, F.D.; Yurochko, A.D. Human Cytomegalovirus Requires Epidermal Growth Factor Receptor Signaling to Enter and Initiate the Early Steps in the Establishment of Latency in CD34+ Human Progenitor Cells. J. Virol. 2017, 91, e01206-16. [Google Scholar] [CrossRef]
- Li, Q.; Wilkie, A.R.; Weller, M.; Liu, X.; Cohen, J.I. THY-1 Cell Surface Antigen (CD90) Has an Important Role in the Initial Stage of Human Cytomegalovirus Infection. PLoS Pathog. 2015, 11, e1004999. [Google Scholar] [CrossRef]
- Martinez-Martin, N.; Marcandalli, J.; Huang, C.S.; Arthur, C.P.; Perotti, M.; Foglierini, M.; Ho, H.; Dosey, A.M.; Shriver, S.; Payandeh, J.; et al. An Unbiased Screen for Human Cytomegalovirus Identifies Neuropilin-2 as a Central Viral Receptor. Cell 2018, 174, 1158–1171. [Google Scholar] [CrossRef]
- Agelidis, A.; Shukla, D. Heparanase, Heparan Sulfate and Viral Infection. In Heparanase: From Basic Research to Clinical Applications (Advances in Experimental Medicine and Biology); Vlodavsky, I., Sanderson, R., Ilan, N., Eds.; Springer: Cham, Switzerland, 2020; Volume 1221. [Google Scholar]
- Oliver, S.L.; Yang, E.; Arvin, A.M. Varicella-Zoster Virus Glycoproteins: Entry, Replication, and Pathogenesis. Curr. Clin. Microbiol. Rep. 2016, 3, 204–215. [Google Scholar]
- Shukla, D.; Spear, P.G. Herpesviruses and heparan sulfate: An intimate relationship in aid of viral entry. J. Clin. Investig. 2001, 108, 503–510. [Google Scholar]
- Welder, J.; Vislisel, J. Varicella-Zoster Virus (VZV) Epithelial Keratitis, Pseudodendrites; University of Iowa: Iowa City, IA, USA, 2019. [Google Scholar]
- Koujah, L.; Suryawanshi, R.K.; Shukla, D. Pathological processes activated by herpes simplex virus-1 (HSV-1) infection in the cornea. Cell. Mol. Life Sci. 2019, 76, 405–419. [Google Scholar]
- Grinage, E.; Shukla, D. Optineurin in ocular herpes infection. Exp. Eye Res. 2022, 219, 109059. [Google Scholar] [CrossRef]
- Akhtar, J.; Tiwari, V.; Oh, M.J.; Kovacs, M.; Jani, A.; Kovacs, S.K.; Valyi-Nagy, T.; Shukla, D. HVEM and nectin-1 are the major mediators of herpes simplex virus 1 (HSV-1) entry into human conjunctival epithelium. Investig. Ophthalmol. Vis. Sci. 2008, 49, 4026–4035. [Google Scholar] [CrossRef]
- Agelidis, A.M.; Hadigal, S.R.; Jaishankar, D.; Shukla, D. Viral Activation of Heparanase Drives Pathogenesis of Herpes Simplex Virus-1. Cell Rep. 2017, 20, 439–450. [Google Scholar]
- Hadigal, S.R.; Agelidis, A.M.; Karasneh, G.A.; Antoine, T.E.; Yakoub, A.M.; Ramani, V.C.; Djalilian, A.R.; Sanderson, R.D.; Shukla, D. Heparanase is a host enzyme required for herpes simplex virus-1 release from cells. Nat. Commun. 2015, 6, 6985. [Google Scholar]
- Sharma, P.; Kapoor, D.; Shukla, D. Role of Heparanase and Syndecan-1 in HSV-1 Release from Infected Cells. Viruses 2022, 14, 2156. [Google Scholar] [CrossRef]
- Agelidis, A.; Turturice, B.A.; Suryawanshi, R.K.; Yadavalli, T.; Jaishankar, D.; Ames, J.; Hopkins, J.; Koujah, L.; Patil, C.D.; Hadigal, S.R.; et al. Disruption of innate defense responses by endoglycosidase HPSE promotes cell survival. JCI Insight 2021, 6, e144255. [Google Scholar] [CrossRef]
- Suryawanshi, R.K.; Patil, C.D.; Agelidis, A.; Koganti, R.; Yadavalli, T.; Ames, J.M.; Borase, H.; Shukla, D. Pathophysiology of reinfection by exogenous HSV-1 is driven by heparanase dysfunction. Sci. Adv. 2023, 9, eadf3977. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Epidemiology | Clinical Manifestation | Diagnosis | Treatment | |
|---|---|---|---|---|
| Cytomegalovirus (CMV) |
|
|
|
|
| Varicella Zoster Virus (VZV) |
|
|
|
|
| Herpes Simplex Virus (HSV) |
|
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.; Rabiee, B.; Patel, C.; Jafri, M.; Hussain, H.; Chaudhry, A.; Chaudhry, I.; Kamoun, L.; Chaudhry, I.; Oh, L.; et al. Herpesvirus Infections of the Corneal Endothelium. Microorganisms 2025, 13, 778. https://doi.org/10.3390/microorganisms13040778
Wang J, Rabiee B, Patel C, Jafri M, Hussain H, Chaudhry A, Chaudhry I, Kamoun L, Chaudhry I, Oh L, et al. Herpesvirus Infections of the Corneal Endothelium. Microorganisms. 2025; 13(4):778. https://doi.org/10.3390/microorganisms13040778
Chicago/Turabian StyleWang, Jessie, Behnam Rabiee, Chandani Patel, Mansab Jafri, Hamad Hussain, Aaila Chaudhry, Imtiaz Chaudhry, Layla Kamoun, Iftikhar Chaudhry, Lewis Oh, and et al. 2025. "Herpesvirus Infections of the Corneal Endothelium" Microorganisms 13, no. 4: 778. https://doi.org/10.3390/microorganisms13040778
APA StyleWang, J., Rabiee, B., Patel, C., Jafri, M., Hussain, H., Chaudhry, A., Chaudhry, I., Kamoun, L., Chaudhry, I., Oh, L., Bobat, F. I., Shukla, D., & Farooq, A. V. (2025). Herpesvirus Infections of the Corneal Endothelium. Microorganisms, 13(4), 778. https://doi.org/10.3390/microorganisms13040778