
Case Report: Heart Transplantation for Refractory Candida tropicalis Endocarditis: A Case Report and Literature Review

 , , ,
, , ,
Abstract
1. Introduction
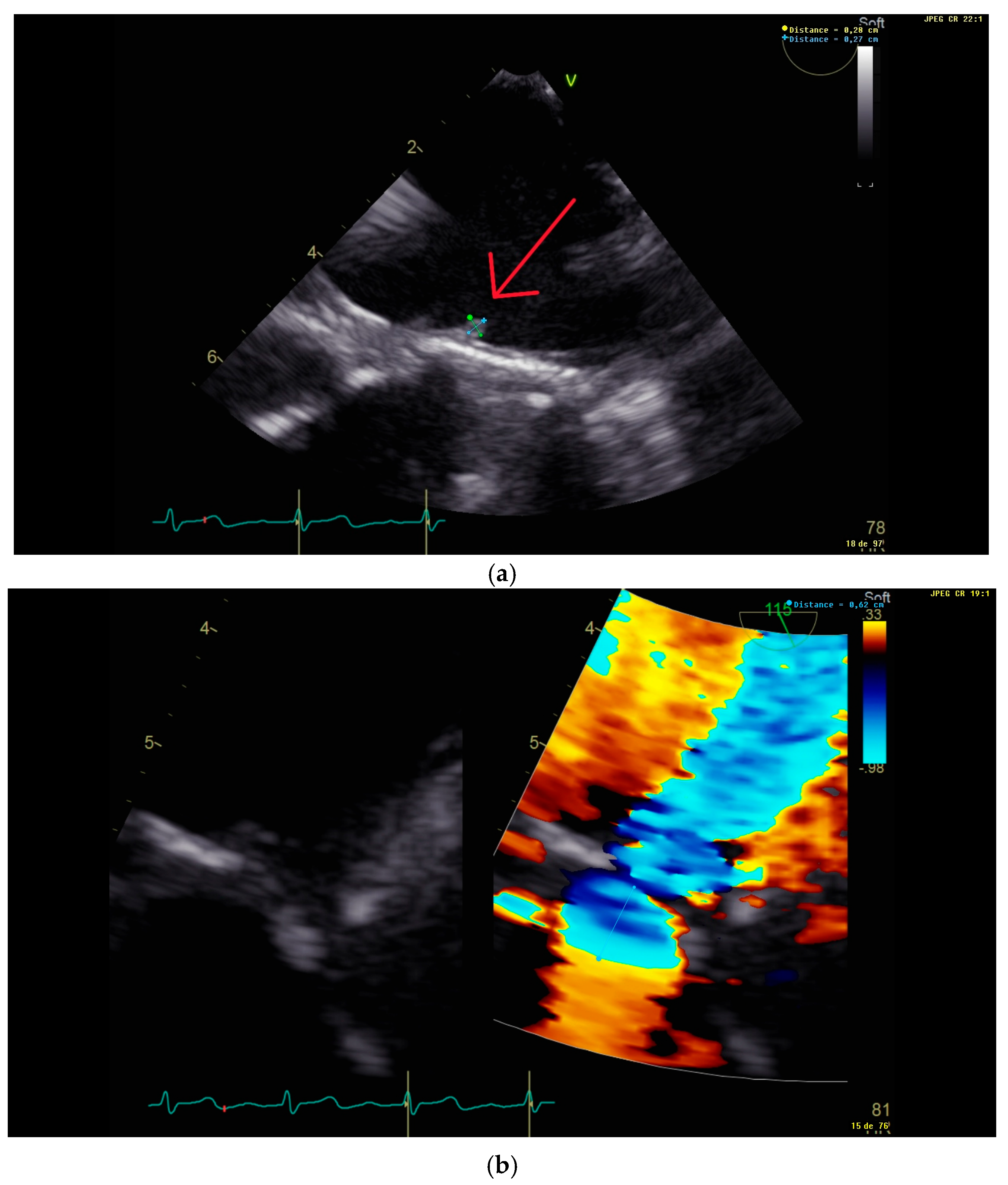
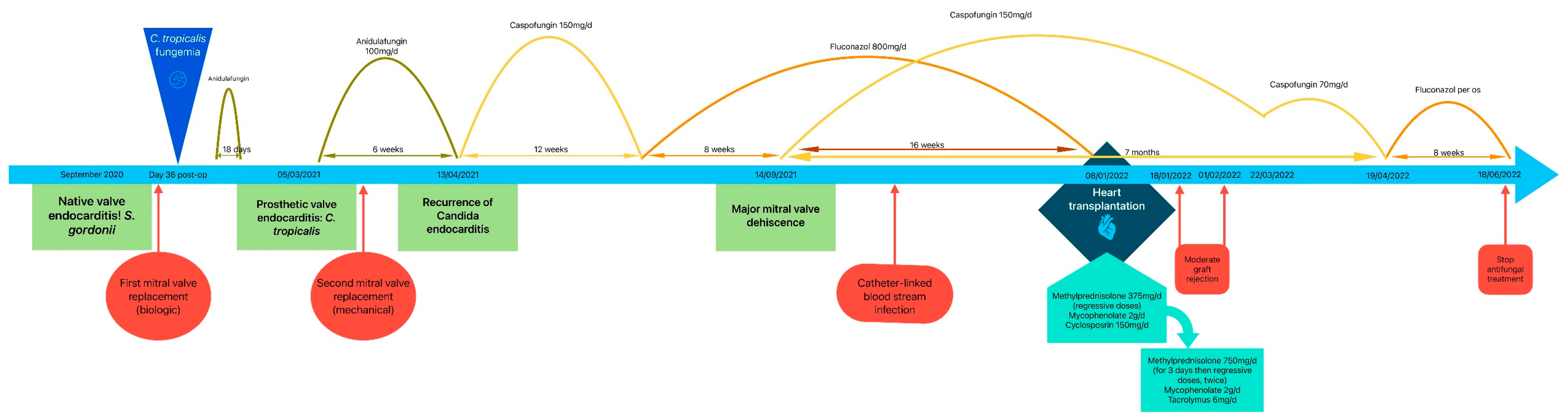
2. Case Presentation
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Deorukhkar, S.C.; Saini, S.; Mathew, S. Virulence Factors Contributing to Pathogenicity of Candida tropicalis and Its Antifungal Susceptibility Profile. Int. J. Microbiol. 2014, 2014, 456878. [Google Scholar] [CrossRef] [PubMed]
- Delgado, V.; Ajmone Marsan, N.; de Waha, S.; Bonaros, N.; Brida, M.; Burri, H.; Caselli, S.; Doenst, T.; Ederhy, S.; Erba, P.A.; et al. 2023 ESC Guidelines for the management of endocarditis: Developed by the task force on the management of endocarditis of the European Society of Cardiology (ESC) Endorsed by the European Association for Cardio-Thoracic Surgery (EACTS) and the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2023, 44, 3948–4042. [Google Scholar] [PubMed]
- Mycology|University of Adelaide [Internet]. CLSI Break Points. Available online: https://www.adelaide.edu.au/mycology/clsi-break-points (accessed on 13 February 2025).
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J.; et al. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2016, 62, e1–e50. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, D.M.; George, T.; Chandra, J.; Mukherjee, P.K.; Ghannoum, M.A. Antifungal Susceptibility of Candida Biofilms: Unique Efficacy of Amphotericin B Lipid Formulations and Echinocandins. Antimicrob. Agents Chemother. 2002, 46, 1773–1780. [Google Scholar] [CrossRef] [PubMed]
- Andes, D.; Diekema, D.J.; Pfaller, M.A.; Bohrmuller, J.; Marchillo, K.; Lepak, A. In Vivo Comparison of the Pharmacodynamic Targets for Echinocandin Drugs against Candida Species. Antimicrob. Agents Chemother. 2010, 54, 2497–2506. [Google Scholar] [CrossRef] [PubMed]
- Lepak, A.J.; Andes, D.R. Antifungal Pharmacokinetics and Pharmacodynamics. Cold Spring Harb. Perspect. Med. 2015, 5, a019653. [Google Scholar] [CrossRef] [PubMed]
- Betts, R.F.; Nucci, M.; Talwar, D.; Gareca, M.; Queiroz-Telles, F.; Bedimo, R.J.; Herbrecht, R.; Ruiz-Palacios, G.; Young, J.-A.H.; Baddley, J.W.; et al. A Multicenter, Double-Blind Trial of a High-Dose Caspofungin Treatment Regimen versus a Standard Caspofungin Treatment Regimen for Adult Patients with Invasive Candidiasis. Clin. Infect. Dis. 2009, 48, 1676–1684. [Google Scholar] [CrossRef] [PubMed]
- Tumbarello, M.; Posteraro, B.; Trecarichi, E.M.; Fiori, B.; Rossi, M.; Porta, R.; Donati, K.d.G.; La Sorda, M.; Spanu, T.; Fadda, G.; et al. Biofilm production by Candida species and inadequate antifungal therapy as predictors of mortality for patients with candidemia. J. Clin. Microbiol. 2007, 45, 1843–1850. [Google Scholar] [CrossRef] [PubMed]
- Checchia, T.; Moura, L.; Colatusso, C.; Veiga, S.; Fortes, J.; Tuon, F. Heart transplantation and Candida endocarditis. Transpl. Infect. Dis. 2016, 18, 483–484. [Google Scholar] [CrossRef] [PubMed]
- Tattevin, P.; Muñoz, P.; Moreno, A.; Hékimian, G.; Delahaye, F.; Duval, X.; Castel, M.Á.; Hasse, B.; Jaramillo, N.; Vincelj, J.; et al. Heart transplantation as salvage treatment of intractable infective endocarditis. Infect. Dis. Lond. Engl. 2023, 55, 370–374. [Google Scholar] [CrossRef] [PubMed]
- Guerrero, M.L.F.; Aldámiz, G.; Bayón, J.; Cohen, V.A.; Fraile, J. Long-term survival of salvage cardiac transplantation for infective endocarditis. Ann. Thorac. Surg. 2011, 92, e93–e94. [Google Scholar] [CrossRef] [PubMed]
- Murphy, K.M.; Vikram, H.R. Heart transplantation for infective endocarditis: Viable option for a limited few? Transpl. Infect. Dis. Off. J. Transplant. Soc. 2019, 21, e13006. [Google Scholar] [CrossRef] [PubMed]
- Givone, F.; Peghin, M.; Vendramin, I.; Carletti, S.; Tursi, V.; Pasciuta, R.; Livi, U.; Bassetti, M. Salvage heart transplantation for Mycoplasma hominis prosthetic valve endocarditis: A case report and review of the literature. Transpl. Infect. Dis. Off. J. Transplant. Soc. 2020, 22, e13249. [Google Scholar] [CrossRef] [PubMed]
- Rzucidło-Resil, J.; Golińska-Grzybała, K.; Przybylski, R.; Kapelak, B.; Gajos, G.; Gackowski, A. A complicated course of Salmonella endocarditis leading to heart transplantation. Pol. Heart J. Kardiol. Pol. 2022, 80, 945–946. [Google Scholar] [CrossRef] [PubMed]
- van ‘t Veer, M.; Otterspoor, L.; De Regt, M.; Peels, K.; Evens, J.; Vink, A.; de Jonge, N. Heart transplantation for end-stage heart failure combined with Q fever isolated to the heart: A case report. Eur. Heart J. Case Rep. 2020, 4, 1–4. [Google Scholar] [CrossRef]
- Beliaev, A.M.; Ruygrok, P.; Bergin, C.; Haydock, D.A.; Sibal, A.K. Heart transplantation for recurrent Cutibacterium (Propionibacterium) acnes prosthetic heart valve endocarditis. ANZ J. Surg. 2021, 91, 196–197. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Report | Sex & Age | Comorbidities | Valve(s) Involved | Responsible Microorganism | Medical Treatment & Duration | Timing of Transplantation | Outcome |
|---|---|---|---|---|---|---|---|
| Rzucidło-Resil et al., 2022. [15] | F; 39 | severe mitral regurgitation due to myxoid valve disease | Mitral and aortic | Salmonella enterica ssp | Ceftriaxone and trimethoprim/sulfamethoxazole | Several months after the diagnosis (unspecified) | Alive 2 years after transplantation |
| Van’t Veer et al., 2020. [16] | M; 33 | congenital corrected transposition of the great arteries, congenital atrioventricular block, tricuspid valve replacement, and progressive heart failure | Tricuspid | Coxiella brunetii | Doxycycline and hydroxychloroquine, then doxycycline and rifadine, then doxycycline and moxifloxacine, then doxycycline alone | Two years after diagnosis | Alive 5 years after transplantation |
| Beliaev et al., 2021. [17] | M; 59 | rhumatic heart disease, 7 cardiac operations including 6 redo prosthetic heart valve replacements for C. acnes endocarditis | Mitral and aortic, and left atrium | Cutibacterium acnes | Lifelong penicillin prophylaxis after transplantation. | Six years after the last prosthetic valve replacement | Alive 11 months after transplantation |
| Report | Sex & Age | Comorbidities | Valve(s) Involved | Responsible Microorganism | Medical Treatment & Duration | Timing of Transplantation | Outcome |
|---|---|---|---|---|---|---|---|
| Checchia et al., 2016. [10] | M; 56 | Advanced heart failure, diabetes mellitus, arterial hypertension, dyslipidemia, coronary artery disease | Tricuspid | Candida krusei | Amphotericin B 4 weeks, switched to anidulafungin for 6 weeks | Four weeks after initiation of amphotericin B | Alive |
| Tattevin et al., 2023. [11] | UK; 50–60 | Unspecified | Mitral | Candida albicans | Unspecified | One hundred and sixty-one days after onset of infective endocarditis | Alive |
| Our case report | M; 63 | hemochromatosis, arterial hypertension, hypercholesterolemia, malignant melanoma, chronic kidney disease | Mitral | Candida tropicalis | Anidulafungin for 6 weeks, caspofungin for 12 weeks, then fluconazole for 8 weeks, combined then with caspofungin for 16 weeks, then caspofungin alone for 14 weeks, then fluconazole for 8 weeks | Ten months after onset of infective Candida endocarditis | Alive |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El Nouwar, R.; Larranaga Lapique, E.; Vanden Eynden, F.; Martiny, D.; Remmelink, M.; Roussoulières, A.; Hites, M. Case Report: Heart Transplantation for Refractory Candida tropicalis Endocarditis: A Case Report and Literature Review. Microorganisms 2025, 13, 580. https://doi.org/10.3390/microorganisms13030580
El Nouwar R, Larranaga Lapique E, Vanden Eynden F, Martiny D, Remmelink M, Roussoulières A, Hites M. Case Report: Heart Transplantation for Refractory Candida tropicalis Endocarditis: A Case Report and Literature Review. Microorganisms. 2025; 13(3):580. https://doi.org/10.3390/microorganisms13030580
Chicago/Turabian StyleEl Nouwar, Ricardo, Eva Larranaga Lapique, Frédéric Vanden Eynden, Delphine Martiny, Myriam Remmelink, Ana Roussoulières, and Maya Hites. 2025. "Case Report: Heart Transplantation for Refractory Candida tropicalis Endocarditis: A Case Report and Literature Review" Microorganisms 13, no. 3: 580. https://doi.org/10.3390/microorganisms13030580
APA StyleEl Nouwar, R., Larranaga Lapique, E., Vanden Eynden, F., Martiny, D., Remmelink, M., Roussoulières, A., & Hites, M. (2025). Case Report: Heart Transplantation for Refractory Candida tropicalis Endocarditis: A Case Report and Literature Review. Microorganisms, 13(3), 580. https://doi.org/10.3390/microorganisms13030580