
Trends in Healthcare-Acquired Infections Due to Multidrug-Resistant Organisms at a German University Medical Center Before and During the COVID-19 Pandemic



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Outcome and Definitions
2.3. Data Processing
2.4. Data Analysis
2.5. Ethical Considerations
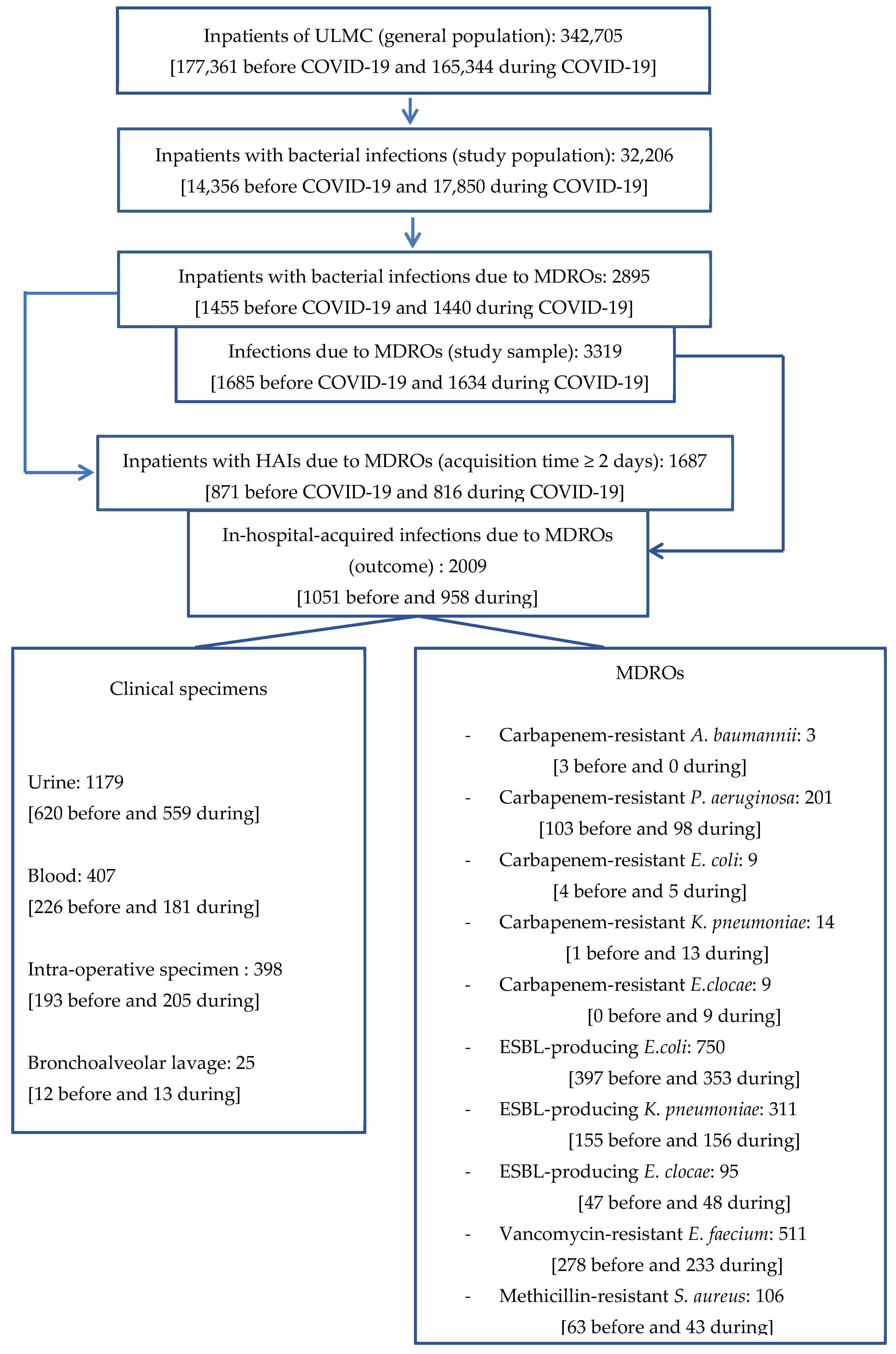
2.6. Flow Chart
3. Results
3.1. Description of the General Population
3.2. Description of the Study Population
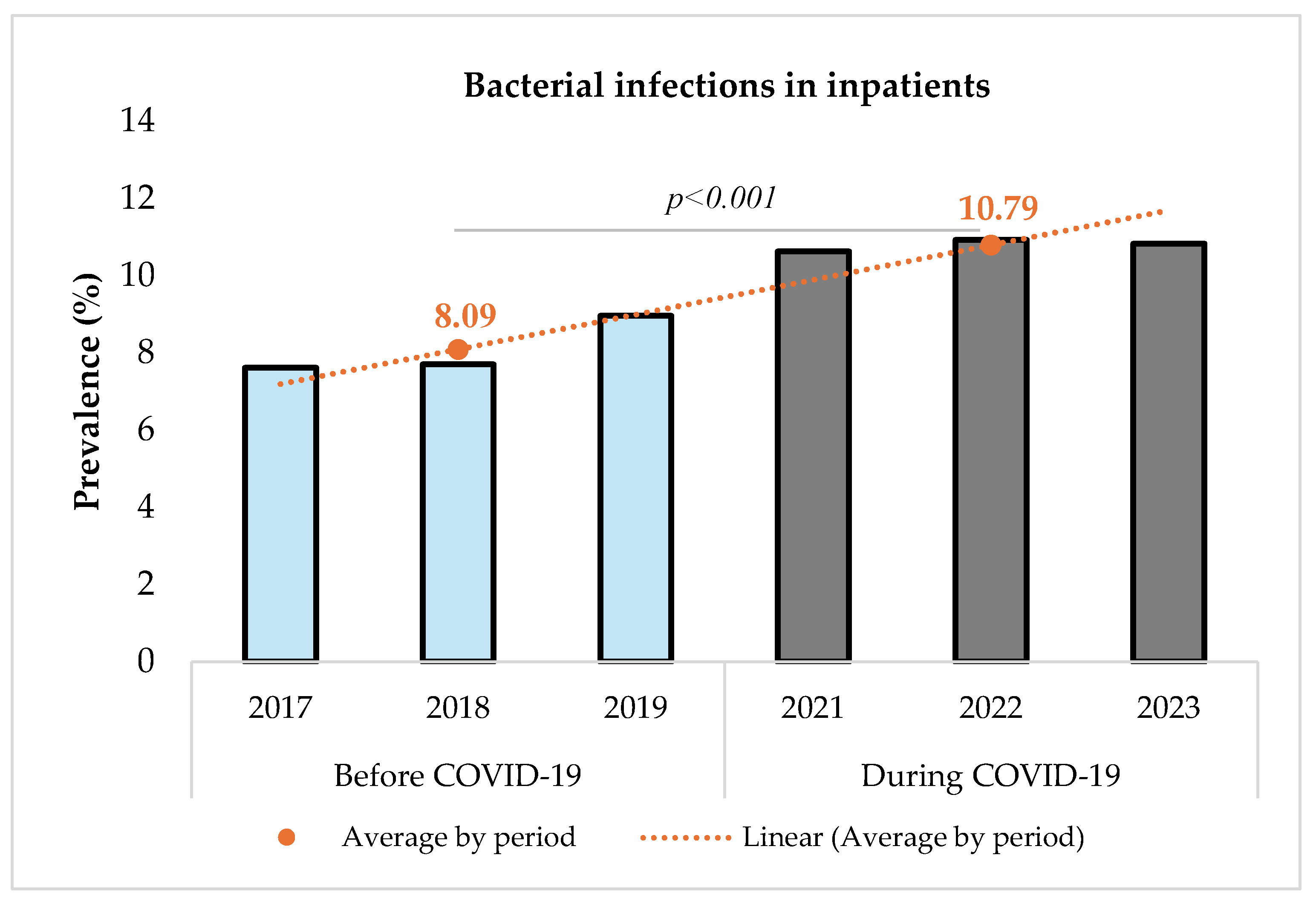
3.3. Prevalence of Bacterial Infections in Inpatients Before (2017–2019) and During (2021–2023) COVID-19
3.4. Infections Due to MDROs in Inpatients Before (2017–2019) and During (2021–2023) COVID-19
3.5. Multidrug-Resistant Healthcare-Acquired Infections (HAIs) in Inpatients Before (2017–2019) and During (2021–2023) COVID-19
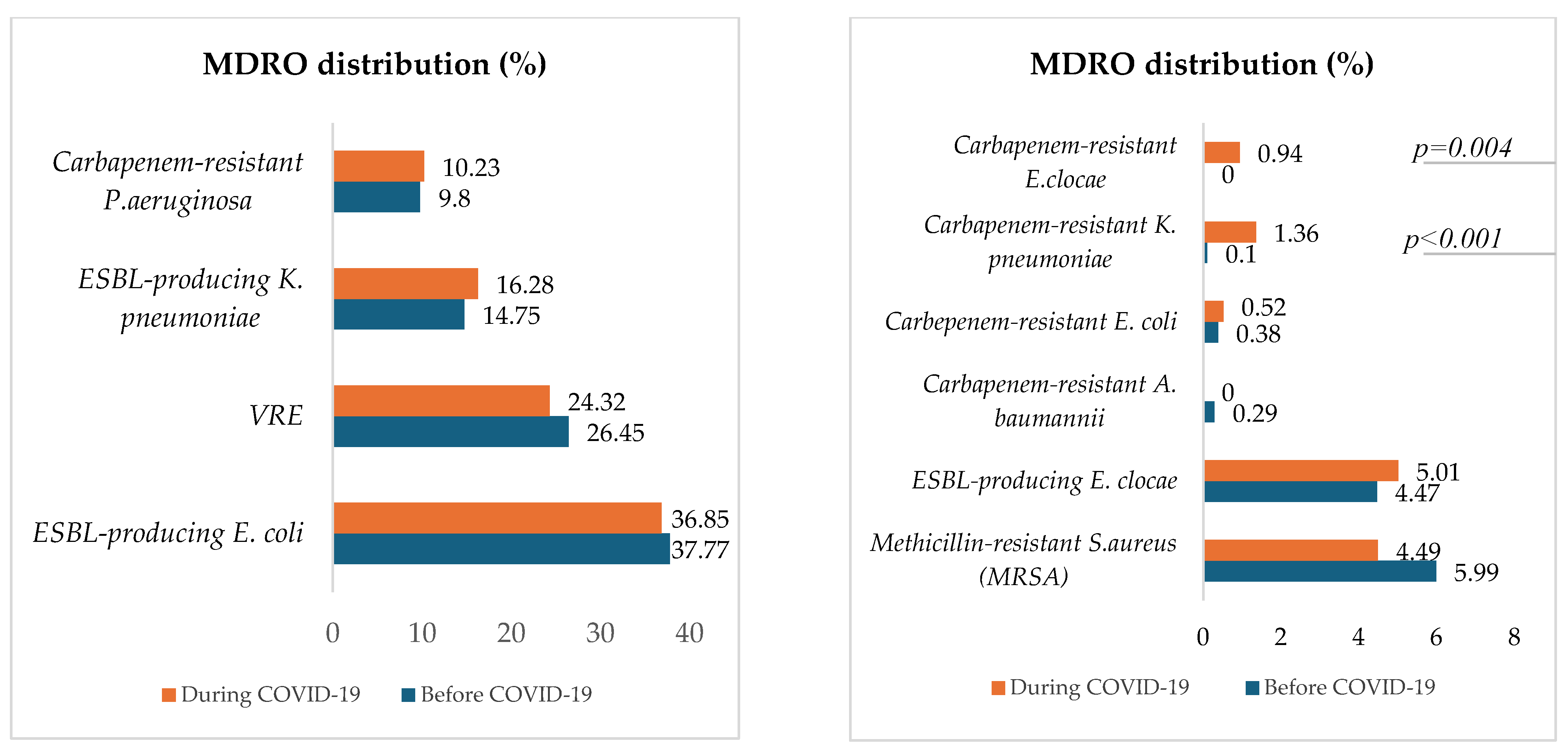
3.6. Distribution of Healthcare-Acquired MDRO
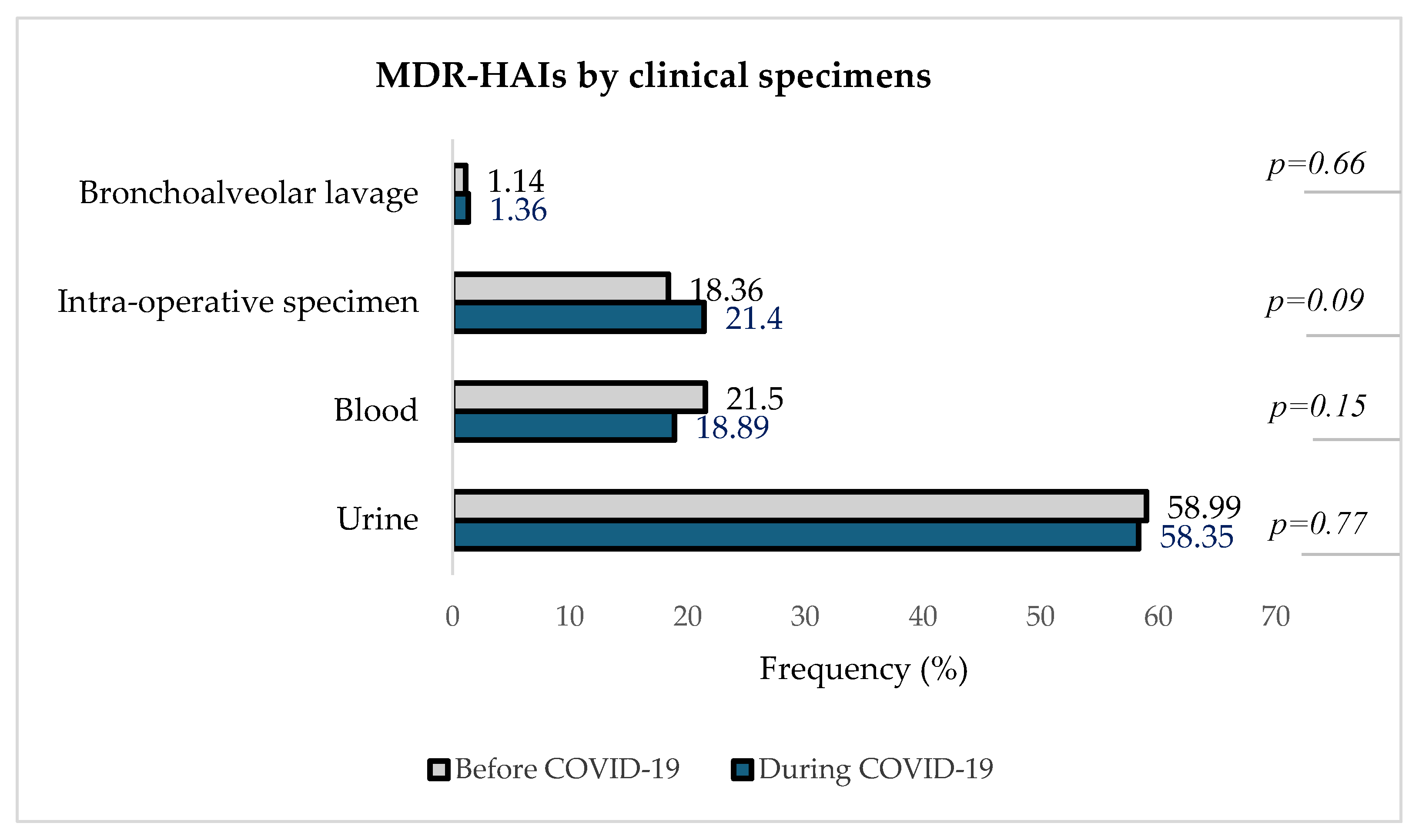
3.7. Distribution of MDR-HAIs in Clinical Specimens Before and During the COVID-19 Pandemic
3.8. Antibiotic Susceptibility Profile of Healthcare-Acquired MDRO
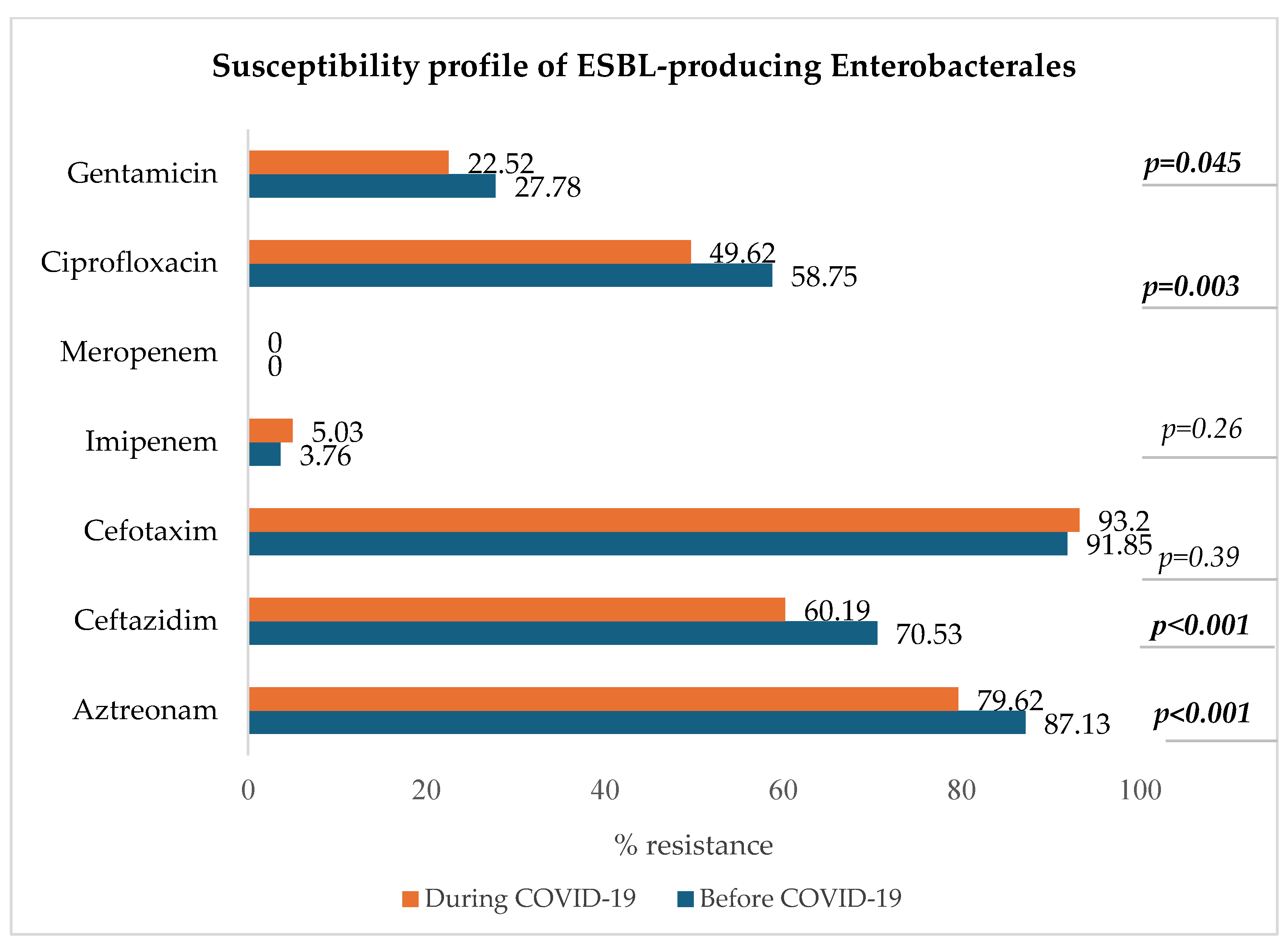
3.8.1. ESBL-Producing Enterobacterales: E. coli, K. pneumoniae, E. clocae
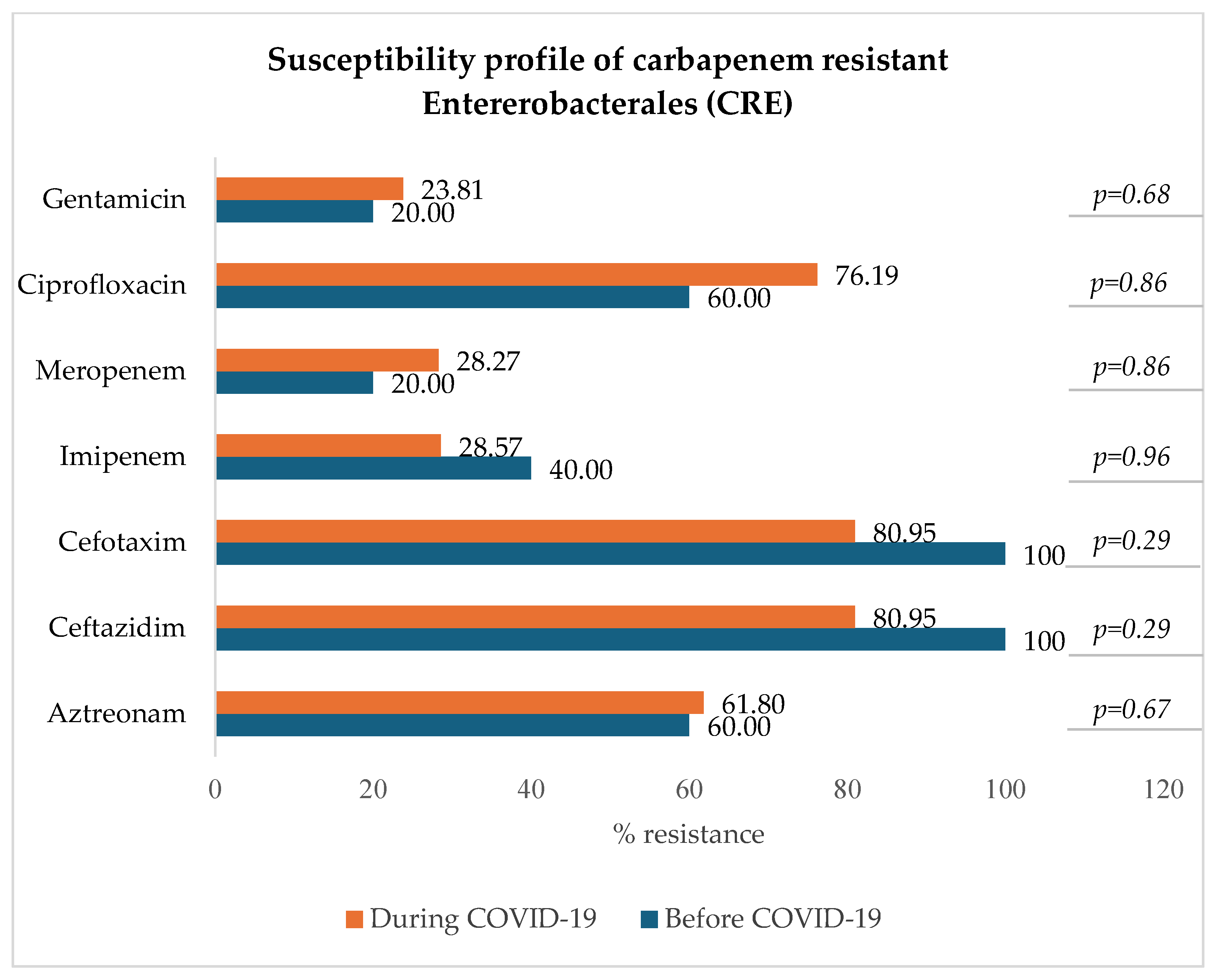
3.8.2. Carbapenem-Resistant Enterobacterales: E. coli, K. pneumoniae, E. clocae
3.8.3. Carbapenem-Resistant Acinetobacter baumannii (CRAB)
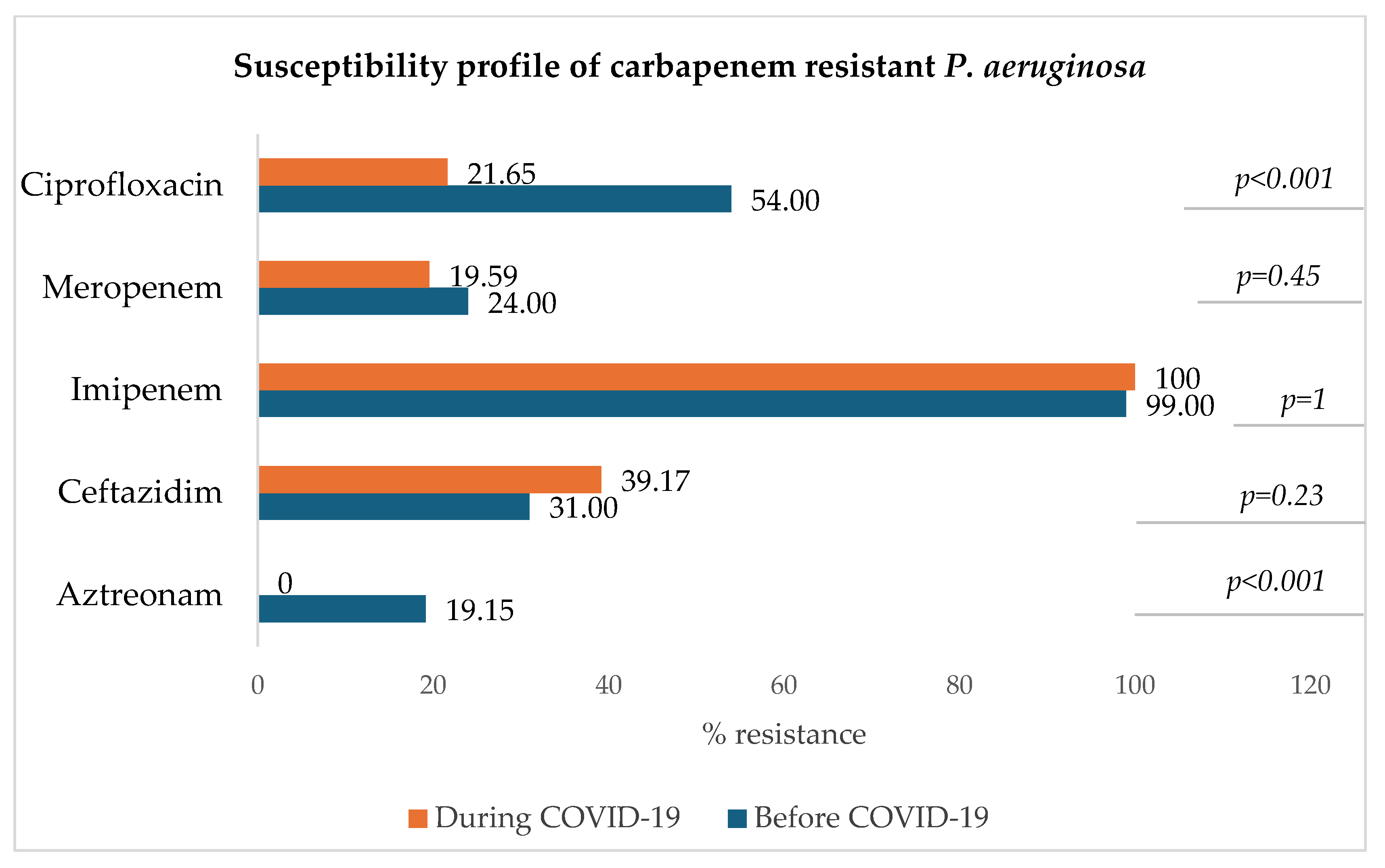
3.8.4. Carbapenem-Resistant Pseudomonas aeruginosa (CRPA)
3.8.5. Vancomycin-Resistant Enterococcus faecium (VRE)
3.8.6. Methicillin-Resistant Staphylococcus aureus (MRSA)
3.9. Factors Associated with the In-Hospital Acquisition of Infections Due to MDROs (MDR-HAIs)
3.9.1. Univariable Analysis with Interaction Terms (Variable*Period COVID-19)
- -
- Compared to adults (18–64 years), the risk of in-hospital-acquired infections due to MDROs was 0.34 times lower in infants under one year of age (p = 0.019) before the COVID-19 pandemic. This was non-significantly lower in children (p = 0.12) and the elderly group (p = 0.37). During COVID-19, there was a significant decrease in the odds ratio (OR) of the association between MDR-HAIs and the elderly group (OR = 0.66 vs 0.91 before, p = 0.03).
- -
- Compared to a length of stay (LOS) < 8 days, the risk of MDR-HAIs tended to increase (trend p < 0.001) in both periods for longer LOSs. Before the pandemic, the OR increased significantly from 2.32 (p < 0.001) for medium stays (8–14 days) to 9.45 (p < 0.001) for long stays (15–30 days) and to 33.60 (p < 0.001) for very long stays (> 30 days) compared to short stays. During COVID-19, there was also an increase in OR between all these types of stay and MDR HAIs (respectively, 2.32 to 2.69, 9.45 to 12.66, and 33.60 to 45.70). But, the additional effect of this increase was not significant.
- -
- Compared to normal care, the risk of in-hospital-acquired infections due to MDROs was 1.33 times higher in intensive care units (p = 0.03) before the pandemic. During COVID-19, although not significant (p = 0.67), the OR for this association increased to 1.44.
3.9.2. Multivariable Analysis (Logistic Regression with Interaction Terms)
- -
- During COVID-19, there was a significant decrease in the risk of MDR-HAIs among the children (OR = 1.55 to 0.31, p = 0.003) and elderly (OR = 1.17 to 0.78, p = 0.03) groups. Compared to an LOS < 8 days, the risk of MDR-HAIs tended to increase (trend p < 0.001) in both periods for longer LOSs. Before the pandemic, the LOS was a risk factor of MDR-HAIs. We therefore noted a significant increase in the risk to 2.31 [1.63–3.18] (p < 0.001) for medium stays, to 9.48 [6.87–13.36] (p < 0.001) for long stays, and to 34.27 [23.62–49.73] (p < 0.001) for very long stays compared to short stays. During COVID-19, the odds ratios (OR) for MDR-HAIs increased for medium stays (OR = 2.68), long stays (OR = 12.80), and very long stays (OR = 48.52), but these increases were not statistically significant. 3.9.3. Multivariable Analysis (Logistic Regression Without Interaction Terms)
- -
- During the COVID-19 pandemic, the risk of in-hospital acquisition of infections due to MDROs in infected inpatients at ULMC decreased to 0.82 [0.67–0.99] compared to the pre-pandemic period (p = 0.047).
- -
- The length of stay was a risk factor to MDR HAIs, with an increased risk of 2.47 [1.87–3.27] for medium stays, 10.57 [8.02–13.94] for long stays, and 34.73 [25.37–47.53] for very long stays compared to the short stays (p < 0.001). Risk increased with length of stay (trend p < 0.001).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Identifying Healthcare-Associated Infections (HAI) for NHSN Surveillance. Available online: https://www.cdc.gov/nhsn/pdfs/pscmanual/2psc_identifyinghais_nhsncurrent.pdf (accessed on 25 November 2024).
- Serra-Burriel, M.; Keys, M.; Campillo-Artero, C.; Agodi, A.; Barchitta, M.; Gikas, A.; Palos, G.; López-Casasnovas, G. Impact of multi-drug resistant bacteria on economic and clinical outcomes of healthcare-associated infections in adults: Systematic review and meta-analysis. PLoS ONE 2020, 15, e0227139. [Google Scholar] [CrossRef]
- Dobrović, K.; Škrobo, T.; Selec, K.; Jelić, M.; Čivljak, R.; Peršec, J.; Sakan, S.; Bušić, N.; Mihelčić, A.; Hleb, S.; et al. Healthcare-Associated Bloodstream Infections Due to Multidrug-Resistant Acinetobacter baumannii in COVID-19 Intensive Care Unit: A Single-Center Retrospective Study. Microorganisms 2023, 11, 774. [Google Scholar] [CrossRef] [PubMed]
- US CDC. HAI Data. May 2024. Available online: https://www.cdc.gov/healthcare-associated-infections/php/data/?CDC_AAref_Val=https://www.cdc.gov/hai/data/index.html (accessed on 24 November 2024).
- CDC. Infection Control. April 2024. Available online: https://www.cdc.gov/infection-control/hcp/mdro-management/index.html (accessed on 24 November 2024).
- World Health Organization. New Report Calls for Urgent Action to Avert Antimicrobial Resistance Crisis; WHO: Geneva, Switzerland, 2019; Available online: https://www.who.int/news/item/29-04-2019-new-report-calls-for-urgent-action-to-avert-antimicrobial-resistance-crisis (accessed on 1 January 2025).
- WHO. Antibiotic Resistance, Key Facts. 31 July 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/antibiotic-resistance (accessed on 24 April 2023).
- Blanco, N.; O’Hara, L.M.; Harris, A.D. Transmission pathways of multidrug-resistant organisms in the hospital setting: A scoping review. Infect. Control Hosp. Epidemiol. 2019, 40, 447–456. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- D’agata, E.M.C.; Varu, A.; Geffert, S.F.; Araos, R.; Mitchell, S.; Situ, A.; Cameron, C. Acquisition of Multidrug-resistant Organisms in the Absence of Antimicrobials. Clin. Infect. Dis. 2018, 67, 1437–1440. [Google Scholar] [CrossRef]
- Al-Tawfiq, J.A.; Tambyah, P.A. Healthcare associated infections (HAI) perspectives. J. Infect. Public Health 2014, 7, 339–344. [Google Scholar] [CrossRef] [PubMed]
- CDC. HAI Pathogens and Antimicrobial Resistance Report, 2018–2021. Available online: https://www.cdc.gov/nhsn/hai-report/narrative-commentary.html (accessed on 24 November 2024).
- World Health Organization. (2024). WHO Bacterial Priority Pathogens List, 2024: Bacterial Pathogens of Public Health Importance, to Guide Research, Development and Strategies to Prevent and Control Antimicrobial Resistance. World Health Organization. Available online: https://iris.who.int/handle/10665/376776 (accessed on 24 November 2024).
- CDC. COVID-19 & Antimicrobial Resistance. July 2024. Available online: https://www.cdc.gov/antimicrobial-resistance/data-research/threats/covid-19.html (accessed on 24 November 2024).
- Kariyawasam, R.M.; Julien, D.A.; Jelinski, D.C.; Larose, S.L.; Rennert-May, E.; Conly, J.M.; Dingle, T.C.; Chen, J.Z.; Tyrrell, G.J.; Ronksley, P.E.; et al. Antimicrobial resistance (AMR) in COVID-19 patients: A systematic review and meta-analysis (November 2019–June 2021). Antimicrob. Resist. Infect. Control 2022, 11, 45. [Google Scholar] [CrossRef] [PubMed]
- Chih-Cheng, L.; Shey-Ying, C.; Wen-Chien, K.; Po-Ren, H. Increased antimicrobial resistance during the COVID-19 pandemic. Int. J. Antimicrob. Agent. 2021, 57, 106324. [Google Scholar] [CrossRef]
- Lin, S.; Koh, J.J.; Aung, T.T.; Lim, F.; Li, J.; Zou, H.; Wang, L.; Lakshminarayanan, R.; Verma, C.; Wang, Y.; et al. Symmetrically Substituted Xanthone Amphiphiles Combat Gram-Positive Bacterial Resistance with Enhanced Membrane Selectivity. J. Med. Chem. 2017, 60, 1362–1378. [Google Scholar] [CrossRef]
- Farfour, E.; Lecuru, M.; Dortet, L.; Guen, M.L.; Cerf, C.; Karnycheff, F.; Lesprit, P. Carbapenemase-producing Enterobacterales outbreak: Another dark side of COVID-19. Am. J. Infect. Control 2020, 48, 1533–1536. [Google Scholar] [CrossRef] [PubMed]
- Tiri, B.; Sensi, E.; Marsiliani, V.; Cantarini, M.; Priante, G.; Vernelli, C.; Martella, L.A.; Costantini, M.; Mariottini, A.; Andreani, P.; et al. Antimicrobial stewardship program, COVID-19, and infection control: Spread of carbapenem-resistant Klebsiella pneumoniae colonization in ICU COVID-19 patients. What did not work? J. Clin. Med. 2020, 9, 2744. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wang, J.; Yang, Y.; Cai, P.; Cao, J.; Cai, X.; Zhang, Y. Etiology and antimicrobial resistance of secondary bacterial infections in patients hospitalized with COVID-19 in Wuhan, China: A retrospective analysis. Antimicrob. Resist. Infect. Control 2020, 9, 153. [Google Scholar] [CrossRef]
- Sharifipour, E.; Shams, S.; Esmkhani, M.; Khodadadi, J.; Fotouhi-Ardakani, R.; Koohpaei, A.; Doosti, Z.; Ej Golzari, S. Evaluation of bacterial co-infections of the respiratory tract in COVID-19 patients admitted to ICU. BMC Infect. Dis. 2020, 20, 646. [Google Scholar] [CrossRef] [PubMed]
- LeRose, J.; Sandhu, A.; Polistico, J.; Ellsworth, J.; Cranis, M.; Jabbo, L.; Cullen, L.; Moshos, J.; Samavati, L.; Chopra, T. The impact of coronavirus disease 2019 (COVID-19) response on central-line–associated bloodstream infections and blood culture contamination rates at a tertiary-care center in the Greater Detroit area. Infect. Control Hosp. Epidemiol. 2021, 42, 997–1000. [Google Scholar] [CrossRef]
- Baccolini, V.; Migliara, G.; Isonne, C.; Dorelli, B.; Barone, L.C.; Giannini, D.; Marotta, D.; Marte, M.; Mazzalai, E.; Alessandri, F.; et al. The impact of the COVID-19 pandemic on healthcare-associated infections in intensive care unit patients: A retrospective cohort study. Antimicrob. Resist. Infect. Control 2021, 10, 87. [Google Scholar] [CrossRef]
- Weiner-Lastinger, L.M.; Pattabiraman, V.; Konnor, R.Y.; Patel, P.R.; Wong, E.; Xu, S.Y.; Smith, B.; Edwards, J.R.; Dudeck, M.A. The impact of coronavirus disease 2019 (COVID-19) on healthcare-associated infections in 2020: A summary of data reported to the National Healthcare Safety Network. Infect. Control Hosp. Epidemiol. 2022, 43, 12–25. [Google Scholar] [CrossRef]
- Gisselø, K.L.; Rubin, I.M.C.; Knudsen, M.S.; From-Hansen, M.; Stangerup, M.; Kavalaris, C.P.; Pinholt, M.; Mollerup, S.; Westh, H.; Bartels, M.D.; et al. Substantial decrease in vancomycin-resistant Enterococcus faecium outbreak duration and number of patients during the danish COVID-19 lockdown: A prospective observational study. Microb. Drug Resist. 2022, 28, 73–80. [Google Scholar] [CrossRef]
- Wee, L.E.; Venkatachalam, I.; Sim, X.Y.J.; Tan, K.B.-K.; Wen, R.; Tham, C.K.; Gan, W.H.; Ko, K.K.K.; Ho, W.Q.; Kwek, G.T.C.; et al. Containment of COVID-19 and reduction in healthcare-associated respiratory viral infections through a multi-tiered infection control strategy. Infect. Dis. Health 2021, 26, 123–131. [Google Scholar] [CrossRef]
- Su, C.; Zhang, Z.; Zhao, X.; Peng, H.; Hong, Y.; Huang, L.; Huang, J.; Yan, X.; Wu, S.; Bai, Z. Changes in prevalence of nosocomial infection pre- and post-COVID-19 pandemic from a tertiary Hospital in China. BMC Infect. Dis. 2021, 21, 693. [Google Scholar] [CrossRef]
- Mitchell, B.G.; Stewardson, A.J.; Kerr, L.; Ferguson, J.K.; Curtis, S.; Busija, L.; Lydeamore, M.J.; Graham, K.; Russo, P.L. The incidence of nosocomial bloodstream infection and urinary tract infection in Australian hospitals before and during the COVID-19 pandemic: An interrupted time series study. Antimicrob. Resist. Infect. Control 2023, 12, 61. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Raoofi, S.; Pashazadeh Kan, F.; Rafiei, S.; Hosseinipalangi, Z.; Noorani Mejareh, Z.; Khani, S.; Abdollahi, B.; Seyghalani Talab, F.; Sanaei, M.; Zarabi, F.; et al. Global prevalence of nosocomial infection: A systematic review and meta-analysis. PLoS ONE 2023, 18, e0274248. [Google Scholar] [CrossRef]
- European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters, Version 14.0, 2024. Available online: https://www.eucast.org/clinical_breakpoints (accessed on 1 January 2025).
- Wan Nawi, N.A.R. Multinomial Logistic Regression Using SPSS. Available online: https://wnarifin.github.io/lecture/pg/mlog_spss_pg.pdf (accessed on 30 December 2024).
- World Health Organization. Report on the Burden of Healthcare-Associated Infections; WHO: Geneva, Switzerland, 2024; Available online: https://www.who.int/publications/i/item/9789240103986 (accessed on 13 January 2025).
- World Health Organization. Global Report on Infection Prevention and Control 2024; World Health Organization: Geneva, Switzerland, 2024; ISBN 978-92-4-010398-6. [Google Scholar]
- Geffers, C.; Schwab, F.; Behnke, M.; Gastmeier, P. No increase of device associated infections in German intensive care units during the start of the COVID-19 pandemic in 2020. Antimicrob. Resist. Infect. Control 2022, 11, 67. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kapsner, L.A.; Kampf, M.O.; Seuchter, S.A.; Gruendner, J.; Gulden, C.; Mate, S.; Mang, J.M.; Schüttler, C.; Deppenwiese, N.; Krause, L.; et al. Reduced Rate of Inpatient Hospital Admissions in 18 German University Hospitals During the COVID-19 Lockdown. Front. Public Health 2021, 8, 594117. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Healthcare-Associated Infections. Available online: https://www.ecdc.europa.eu/en/healthcare-associated-infections (accessed on 7 January 2025).
- Morris, S.; Cerceo, E. Trends, Epidemiology, and Management of Multi-Drug Resistant Gram-Negative Bacterial Infections in the Hospitalized Setting. Antibiotics 2020, 9, 196. [Google Scholar] [CrossRef] [PubMed]
- Djuikoue, C.I.; Yamdeu Djonkouh, W.; Epie Bekolo, C.; Kamga Wouambo, R.; Carrel Founou, R.; Djouela Djoulako, P.D.; Tonfak Temgoua, G.; Pokam, B.D.T.; Antoine-Moussiaux, N.; Apalata, T.R. Prevalence and Antibiotic Resistance Pattern of Streptococcus, Staphylococcus, Neisseria meningitidis and Enterobacteriaceae in Two Reference Hospitals of Yaoundé. Antibiotics 2023, 12, 929. [Google Scholar] [CrossRef] [PubMed]
- Langford, B.J.; Soucy, J.R.; Leung, V.; So, M.; Kwan, A.T.H.; Portnoff, J.S.; Bertagnolio, S.; Raybardhan, S.; MacFadden, D.R.; Daneman, N. Antibiotic resistance associated with the COVID-19 pandemic: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2023, 29, 302–309. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Point Prevalence Survey of Healthcare-Associated Infections and Antimicrobial Use in European Acute Care Hospitals 2022–2023. Available online: https://www.ecdc.europa.eu/en/publications-data/PPS-HAI-AMR-acute-care-europe-2022-2023 (accessed on 27 December 2024).
- Petrosillo, N.; Petersen, E.; Antoniak, S. Ukraine war and antimicrobial resistance. Lancet Infect. Dis. 2023, 23, 653–654. [Google Scholar] [CrossRef] [PubMed]
- Hermsen, E.D.; Amos, J.; Townsend, A.; Becker, T.; Hargreaves, S. Antimicrobial resistance among refugees and asylum seekers: A global systematic review and meta-analysis. Lancet Infect. Dis. 2025, 25, e34–e43. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Operational Public Health Considerations for the Prevention and Control of Infectious Diseases in the Context of Russia’s Aggression Towards Ukraine. 8 March 2022. Available online: https://www.ecdc.europa.eu/en/publications-data/operational-public-health-considerations-prevention-and-control-infectious (accessed on 13 January 2025).
- Bai, Y.; Xie, C.; Zhang, Y.; Zhang, Z.; Liu, J.; Cheng, G.; Li, Y.; Wang, D.; Cui, B.; Liu, Y.; et al. sRNA Expression Profile of KPC-2-Producing Carbapenem-Resistant Klebsiella pneumoniae: Functional Role of sRNA51. PLoS Pathog. 2024, 20, e1012187. [Google Scholar] [CrossRef]
- Ilmavirta, H.; Ollgren, J.; Räisänen, K.; Kinnunen, T.; Hakanen, A.J.; Rantakokko-Jalava, K.; Jalava, J.; Lyytikäinen, O. Impact of the COVID-19 pandemic on extended-spectrum β-lactamase producing Escherichia coli in urinary tract and blood stream infections: Results from a nationwide surveillance network, Finland, 2018 to 2022. Antimicrob. Resist. Infect. Control 2024, 13, 72. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Selected MDRO | Selected Antimicrobial Agents |
|---|---|
| ESBL-producing or carbapenem-resistant Enterobacterales: E. coli, K. pneumoniae, E. cloacae | aztreonam, ceftazidim, cefotaxim, imipenem, meropenem, ciprofloxacin, gentamicin |
| Carbapenem-resistant A. baumannii | imipenem, meropenem, ciprofloxacin, gentamicin |
| Carbapenem-resistant P. aeruginosa | aztreonam, ceftazidim, imipenem, meropenem, ciprofloxacin |
| VRE | vancomycin, linezolid |
| MRSA | vancomycin, daptomycin, linezolid |
| Characteristics | Before COVID-19 n = 177,361 (51.75%) | During COVID-19 n = 165,344 (48.25%) | Total n = 342,705 | p-Value a | ||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |||
| Sex | ||||||||
| Male | 88,608 | 49.95 | 83,722 | 50.64 | 172,330 | 50.25 | <0.001 | |
| Female | 88,232 | 49.75 | 79,017 | 47.79 | 167,249 | 48.80 | <0.001 | |
| Unknown | 0 | 0.00 | 6 | 0.004 | 6 | 0.002 | 0.03 | |
| Missing | 521 | 0.30 | 2599 | 1.57 | 3120 | 0.91 | <0.001 | |
| Age (years) | ||||||||
| * | 48 | 50 | 49 | |||||
| Infants (<1) | 12,314 | 6.94 | 11,280 | 6.82 | 23,594 | 6.88 | 0.16 | |
| Children (1–17) | 17,43 | 9.83 | 16,375 | 9.90 | 33,808 | 9.87 | 0.46 | |
| Adults (18–64) | 87,986 | 49.61 | 76,084 | 46.02 | 164,070 | 47.87 | <0.001 | |
| Elderly (65+) | 59,628 | 33.62 | 61,605 | 37.26 | 121,233 | 35.38 | <0.001 | |
| Stay (days) | ||||||||
| * | 7 | 7 | 7 | |||||
| Short stay (1–7) | 132,206 | 74.54 | 122,795 | 74.27 | 255,001 | 74.41 | 0.07 | |
| Medium stay (8–14) | 24,464 | 13.79 | 22,852 | 13.82 | 47,316 | 13.81 | 0.8 | |
| Long stay (15–30) | 13,766 | 7.76 | 13,212 | 8.00 | 26,978 | 7.87 | 0.01 | |
| Very long stay (>30) | 6925 | 3.90 | 6470 | 3.91 | 13,395 | 3.91 | 0.9 | |
| Missing | 0 | 0.00 | 15 | 0.01 | 15 | 0.004 | <0.001 | |
| Unit of care | ||||||||
| Normal care unit | 165,493 | 93.31 | 154,519 | 93.45 | 320,012 | 93.38 | 0.09 | |
| Intensive care unit | 11,868 | 6.69 | 10,825 | 6.55 | 22,693 | 6.62 | 0.09 | |
| Characteristics | Before COVID-19 n = 14,356 (44.58%) | During COVID-19 n = 17,850 (55.42%) | Total N = 32,206 | p-Value a | ||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |||
| Sex | ||||||||
| Male | 7612 | 53.02 | 9265 | 51.90 | 16,877 | 52.40 | 0.046 | |
| Female | 6741 | 46.96 | 8498 | 47.61 | 15,239 | 47.32 | 0.24 | |
| Missing | 3 | 0.02 | 87 | 0.49 | 90 | 0.28 | <0.001 | |
| Age (years) | ||||||||
| * | 62 | 62 | 62 | |||||
| Infants (<1) | 344 | 2.40 | 318 | 1.78 | 662 | 2.06 | <0.001 | |
| Children (1–17) | 523 | 3.64 | 695 | 3.89 | 1218 | 3.78 | 0.24 | |
| Adults (18–64) | 5669 | 39.49 | 6922 | 38.78 | 12,591 | 39.10 | 0.2 | |
| Elderly (≥65) | 7820 | 54.47 | 9915 | 55.55 | 17,735 | 55.07 | 0.05 | |
| Stay (days) | ||||||||
| * | 20 | 18 | 19 | |||||
| Short stay (1–7) | 4545 | 31.66 | 6111 | 34.24 | 10,656 | 33.09 | <0.001 | |
| Medium stay (8–14) | 3302 | 23.00 | 4344 | 24.34 | 7646 | 23.74 | 0.005 | |
| Long stay (15–30) | 3717 | 25.89 | 4577 | 25.64 | 8294 | 25.75 | 0.61 | |
| Very long stay (>30) | 2792 | 19.45 | 2814 | 15.76 | 5606 | 17.41 | <0.001 | |
| Missing | 0 | 0.00 | 4 | 0.02 | 4 | 0.01 | ||
| Unit of care | ||||||||
| Normal care unit | 11,167 | 77.79 | 14,155 | 79.30 | 25,322 | 78.63 | <0.001 | |
| Intensive care unit | 3189 | 22.21 | 3695 | 20.70 | 6884 | 21.37 | <0.001 | |
| Variables | In-Hospital Acquisition of MDRO | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Before COVID-19 | During COVID-19 | ||||||||||
| n | No (%) | Yes (%) | OR c | p-Value c | n | No (%) | Yes (%) | OR c | p-Value c* | ||
| Sex a | |||||||||||
| Male | 863 | 323 37.43 | 540 62.57 | Ref | 841 | 332 39.48 | 509 60.52 | Ref | |||
| Female | 822 | 311 37.83 | 511 62.17 | 0.98 | 0.86 | 788 | 343 43.53 | 445 56.47 | 0.84 | 0.29 | |
| Missing | - | - | - | 1 | - | 4 | 0 0.00 | 4 100.0 | 1 | - | |
| Age (years) b | 1685 63 * | 634 63 * | 1051 63 * | 0.51 b | 1633 61 * | 675 62 * | 958 61 * | 0.35 b | |||
| Group of age a | |||||||||||
| Adults | 698 | 250 35.82 | 448 64.18 | Ref | 740 | 262 35.41 | 478 64.59 | Ref | |||
| Infants | 21 | 13 81.90 | 8 38.10 | 0.34 | 0.019 | 17 | 7 41.18 | 10 58.83 | 0.77 | 0.22 | |
| Children | 44 | 21 47.73 | 23 52.27 | 0.61 | 0.12 | 54 | 36 66.67 | 18 33.33 | 0.27 | 0.06 | |
| Elderly | 922 | 350 37.96 | 572 62.04 | 0.91 | 0.37 | 822 | 370 45.01 | 452 54.99 | 0.66 | 0.03 | |
| Length of stay (days) b | 1685 32 * | 634 13 * | 1051 43 * | <0.001 b | 1632 30 * | 674 12 * | 958 42 * | <0.001 b | |||
| Type of stay a | <0.001 ** | ||||||||||
| Short stay | 348 | 275 79.02 | 73 20.98 | Ref | 361 | 299 82.83 | 62 17.17 | Ref | |||
| Medium stay | 273 | 169 61.90 | 104 38.1 | 2.32 | <0.001 | 344 | 221 64.24 | 123 35.76 | 2.69 | 0.57 | |
| Long stay | 449 | 128 28.51 | 321 71.49 | 9.45 | <0.001 | 362 | 100 27.62 | 262 72.38 | 12.66 | 0.24 | |
| Very long stay | 615 | 62 10.08 | 553 89.92 | 33.60 | <0.001 | 565 | 54 9.56 | 511 90.44 | 45.70 | 0.26 | |
| Unit a | |||||||||||
| Normal care unit | 1354 | 527 38.92 | 827 61.08 | Ref | 1310 | 564 43.05 | 746 56.95 | Ref | |||
| Intensive care Unit | 331 | 107 32.33 | 224 67.67 | 1.33 | 0.03 | 323 | 111 34.37 | 212 65.63 | 1.44 | 0.67 | |
| In-Hospital-Acquired MDRO (MDR HAIs) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Before COVID-19 | During COVID-19 | |||||||
| OR c | CI (95%) c | p-Value c | Additional OR c* | CI (95%) c* | OR c | p-Value c** | ||
| Group of age | ||||||||
| Adults | Ref | |||||||
| Infants | 0.70 | [0.24–2.70] | 0.52 | 1.14 | [0.22–5.85] | 0.80 | 0.88 | |
| Children | 1.55 | [0.75–3.20] | 0.23 | 0.20 | [0.07–0.58] | 0.31 | 0.003 | |
| Elderly | 1.17 | [0.91–1.50] | 0.23 | 0.67 | [0.47–0.96] | 0.78 | 0.03 | |
| Type of stay | <0.001 ** | |||||||
| Short stay | Ref | |||||||
| Medium stay | 2.31 | [1.62–3.31] | <0.001 | 1.16 | [0.70–1.92] | 2.68 | 0.55 | |
| Long stay | 9.48 | [6.87–13.36] | <0.001 | 1.35 | [0.83–2.21] | 12.80 | 0.23 | |
| Very long stay | 34.27 | [23.62–49.73] | <0.001 | 46.61 | [0.79–2.35] | 48.52 | 0.27 | |
| Unit | ||||||||
| Normal care unit | Ref | |||||||
| Intensive care unit | 1.14 | [0.83–1.55] | 0.42 | 0.66 | [0.42–1.03] | 0.75 | 0.06 | |
| Variables | In-Hospital-Acquired MDR Infections | |||||
|---|---|---|---|---|---|---|
| No n (%) | Yes n (%) | Adjusted OR | IC (95%) | p-Value | ||
| COVID-19 Era | ||||||
| Before COVID-19 | 634 (37.63) | 1051 (62.37) | Ref | |||
| During COVID-19 | 675 (41.33) | 958 (58.67) | 0.82 | [0.67–0.99] | 0.047 | |
| Type of stay | <0.001 ** | |||||
| Short stay | 574 (80.96) | 135 (19.04) | Ref | |||
| Medium stay | 390 (63.21) | 227 (36.79) | 2.47 | [1.87–3.27] | <0.001 | |
| Long stay | 228 (28.11) | 583 (71.89) | 10.57 | [8.02–13.94] | <0.001 | |
| Very long stay | 116(9.83) | 1064 (90.17) | 34.73 | [25.37–47.53] | <0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kolbe-Busch, S.; Djouela Djoulako, P.D.; Stingu, C.-S. Trends in Healthcare-Acquired Infections Due to Multidrug-Resistant Organisms at a German University Medical Center Before and During the COVID-19 Pandemic. Microorganisms 2025, 13, 274. https://doi.org/10.3390/microorganisms13020274
Kolbe-Busch S, Djouela Djoulako PD, Stingu C-S. Trends in Healthcare-Acquired Infections Due to Multidrug-Resistant Organisms at a German University Medical Center Before and During the COVID-19 Pandemic. Microorganisms. 2025; 13(2):274. https://doi.org/10.3390/microorganisms13020274
Chicago/Turabian StyleKolbe-Busch, Susanne, Paule Dana Djouela Djoulako, and Catalina-Suzana Stingu. 2025. "Trends in Healthcare-Acquired Infections Due to Multidrug-Resistant Organisms at a German University Medical Center Before and During the COVID-19 Pandemic" Microorganisms 13, no. 2: 274. https://doi.org/10.3390/microorganisms13020274
APA StyleKolbe-Busch, S., Djouela Djoulako, P. D., & Stingu, C.-S. (2025). Trends in Healthcare-Acquired Infections Due to Multidrug-Resistant Organisms at a German University Medical Center Before and During the COVID-19 Pandemic. Microorganisms, 13(2), 274. https://doi.org/10.3390/microorganisms13020274