
Association between Gut Microbiota and Muscle Strength in Japanese General Population of the Iwaki Health Promotion Project

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Measurements of Muscle Strength
2.3. Measurements of Body Composition
2.4. Measurements of the Gut Microbiota
2.5. Self-Reported Questionnaires
2.6. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Characteristics of the Gut Microbiota
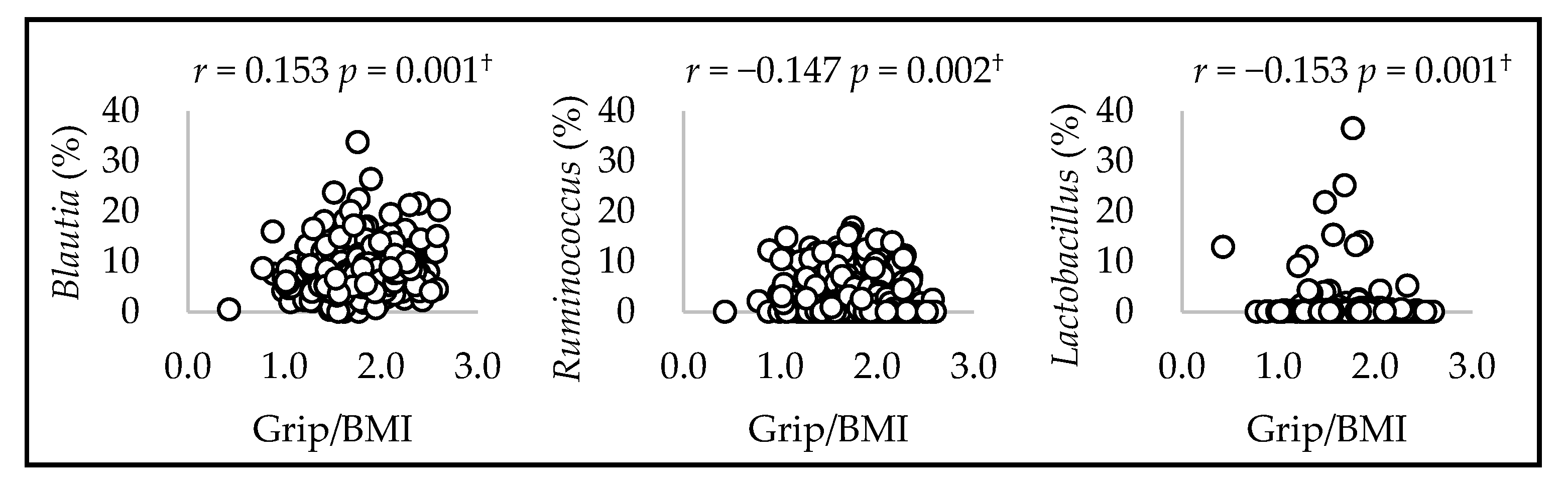
3.3. Association between Gut Microbiota and Muscle Strength
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Flint, H.J.; Duncan, S.H.; Scott, K.P.; Louis, P. Links between diet, gut microbiota composition and gut metabolism. Proc. Nutr. Soc. 2015, 74, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.; Mach, N. The Crosstalk between the Gut Microbiota and Mitochondria during Exercise. Front. Physiol. 2017, 8, 319. [Google Scholar] [CrossRef]
- Arumugam, M.; Raes, J.; Pelletier, E.; Le Paslier, D.; Yamada, T.; Mende, D.R.; Fernandes, G.R.; Tap, J.; Bruls, T.; Batto, J.M.; et al. Enterotypes of the human gut microbiome. Nature 2011, 473, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Sheng, S.; Yan, S.; Chen, J.; Zhang, Y.; Wang, Y.; Qin, Q.; Li, W.; Li, T.; Huang, M.; Ding, S.; et al. Gut microbiome is associated with metabolic syndrome accompanied by elevated gamma-glutamyl transpeptidase in men. Front. Cell. Infect. Microbiol. 2022, 12, 946757. [Google Scholar] [CrossRef]
- Jandhyala, S.M.; Talukdar, R.; Subramanyam, C.; Vuyyuru, H.; Sasikala, M.; Nageshwar Reddy, D. Role of the normal gut microbiota. World J. Gastroenterol. 2015, 21, 8787–8803. [Google Scholar] [CrossRef]
- Clarke, S.F.; Murphy, E.F.; O’Sullivan, O.; Lucey, A.J.; Humphreys, M.; Hogan, A.; Hayes, P.; O’Reilly, M.; Jeffery, I.B.; Wood-Martin, R.; et al. Exercise and associated dietary extremes impact on gut microbial diversity. Gut 2014, 63, 1913–1920. [Google Scholar] [CrossRef]
- Yang, Y.; Shi, Y.; Wiklund, P.; Tan, X.; Wu, N.; Zhang, X.; Tikkanen, O.; Zhang, C.; Munukka, E.; Cheng, S. The Association between Cardiorespiratory Fitness and Gut Microbiota Composition in Premenopausal Women. Nutrients 2017, 9, 792. [Google Scholar] [CrossRef]
- Dalton, A.; Mermier, C.; Zuhl, M. Exercise influence on the microbiome-gut-brain axis. Gut Microbes 2019, 10, 555–568. [Google Scholar] [CrossRef]
- Akazawa, N.; Nakamura, M.; Eda, N.; Murakami, H.; Nakagata, T.; Nanri, H.; Park, J.; Hosomi, K.; Mizuguchi, K.; Kunisawa, J.; et al. Gut microbiota alternation with training periodization and physical fitness in Japanese elite athletes. Front. Sports Act. Living 2023, 5, 1219345. [Google Scholar] [CrossRef]
- Houttu, V.; Boulund, U.; Nicolaou, M.; Holleboom, A.G.; Grefhorst, A.; Galenkamp, H.; van den Born, B.J.; Zwinderman, K.; Nieuwdorp, M. Physical activity and dietary composition relate to differences in gut microbial patterns in a Multi-Ethnic Cohort-The HELIUS Study. Metabolites 2021, 11, 858. [Google Scholar] [CrossRef]
- Fielding, R.A.; Reeves, A.R.; Jasuja, R.; Liu, C.; Barrett, B.B.; Lustgarten, M.S. Muscle strength is increased in mice that are colonized with microbiota from high-functioning older adults. Exp. Gerontol. 2019, 127, 110722. [Google Scholar] [CrossRef] [PubMed]
- Kang, L.; Li, P.; Wang, D.; Wang, T.; Hao, D.; Qu, X. Alterations in intestinal microbiota diversity, composition, and function in patients with sarcopenia. Sci. Rep. 2021, 11, 4628. [Google Scholar] [CrossRef] [PubMed]
- Leong, D.P.; Teo, K.K.; Rangarajan, S.; Lopez-Jaramillo, P.; Avezum, A., Jr.; Orlandini, A.; Seron, P.; Ahmed, S.H.; Rosengren, A.; Kelishadi, R.; et al. Prognostic value of grip strength: Findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet 2015, 386, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Wang DX, M.; Yao, J.; Zirek, Y.; Reijnierse, E.M.; Maier, A.B. Muscle mass, strength, and physical performance predicting activities of daily living: A meta-analysis. J. Cachexia Sarcopenia Muscle 2020, 11, 3–25. [Google Scholar] [CrossRef] [PubMed]
- Alonso, A.C.; Ribeiro, S.M.; Luna, N.M.S.; Peterson, M.D.; Bocalini, D.S.; Serra, M.M.; Brech, G.C.; Greve, J.M.D.; Garcez-Leme, L.E. Association between handgrip strength, balance, and knee flexion/extension strength in older adults. PLoS ONE 2018, 13, e0198185. [Google Scholar] [CrossRef] [PubMed]
- Fragala, M.S.; Alley, D.E.; Shardell, M.D.; Harris, T.B.; McLean, R.R.; Kiel, D.P.; Cawthon, P.M.; Dam, T.T.; Ferrucci, L.; Guralnik, J.M.; et al. Comparison of handgrip and leg extension strength in predicting slow gait speed in older adults. J. Am. Geriatr. Soc. 2016, 64, 144–150. [Google Scholar] [CrossRef]
- Porto, J.M.; Nakaishi, A.P.M.; Cangussu-Oliveira, L.M.; Freire Júnior, R.C.; Spilla, S.B.; Abreu, D.C.C. Relationship between grip strength and global muscle strength in community-dwelling older people. Arch. Gerontol. Geriatr. 2019, 82, 273–278. [Google Scholar] [CrossRef]
- Mitsionis, G.; Pakos, E.E.; Stafilas, K.S.; Paschos, N.; Papakostas, T.; Beris, A.E. Normative data on hand grip strength in a Greek adult population. Int. Orthop. 2009, 33, 713–717. [Google Scholar] [CrossRef]
- Chun, S.W.; Kim, W.; Choi, K.H. Comparison between grip strength and grip strength divided by body weight in their relationship with metabolic syndrome and quality of life in the elderly. PLoS ONE 2019, 14, e0222040. [Google Scholar] [CrossRef]
- Grosicki, G.J.; Travison, T.G.; Zhu, H.; Magaziner, J.; Binder, E.F.; Pahor, M.; Correa-de-Araujo, R.; Cawthon, P.M. Application of cut-points for low muscle strength and lean mass in mobility-limited older adults. J. Am. Geriatr. Soc. 2020, 68, 1445–1453. [Google Scholar] [CrossRef]
- Nakaji, S.; Ihara, K.; Sawada, K.; Parodi, S.; Umeda, T.; Takahashi, I.; Murashita, K.; Kurauchi, S.; Tokuda, I. Social innovation for life expectancy extension utilizing a platform-centered system used in the Iwaki health promotion project: A protocol paper. SAGE Open Med. 2021, 9, 20503121211002606. [Google Scholar]
- Mathiowetz, V. Comparison of Rolyan and Jamar dynamometers for measuring grip strength. Occup. Ther. Int. 2002, 9, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Bobos, P.; Nazari, G.; Lu, Z.; MacDermid, J.C. Measurement properties of the hand grip strength assessment: A systematic review with meta-analysis. Arch. Phys. Med. Rehabil. 2020, 101, 553–565. [Google Scholar] [PubMed]
- Hosomi, K.; Ohno, H.; Murakami, H.; Natsume-Kitatani, Y.; Tanisawa, K.; Hirata, S.; Suzuki, H.; Nagatake, T.; Nishino, T.; Mizuguchi, K.; et al. Method for preparing DNA from feces in guanidine thiocyanate solution affects 16S rRNA-based profiling of human microbiota diversity. Sci. Rep. 2017, 7, 4339. [Google Scholar] [PubMed]
- Kawada, Y.; Naito, Y.; Andoh, A.; Ozeki, M.; Inoue, R. Effect of storage and DNA extraction method on 16S rRNA-profiled fecal microbiota in Japanese adults. J. Clin. Biochem. Nutr. 2019, 64, 106–111. [Google Scholar] [CrossRef]
- Ozato, N.; Saito, S.; Yamaguchi, T.; Katashima, M.; Tokuda, I.; Sawada, K.; Katsuragi, Y.; Kakuta, M.; Imoto, S.; Ihara, K.; et al. Blautia genus associated with visceral fat accumulation in adults 20-76 years of age. NPJ Biofilms Microbiomes 2019, 5, 28. [Google Scholar]
- Takahashi, S.; Tomita, J.; Nishioka, K.; Hisada, T.; Nishijima, M. Development of a prokaryotic universal primer for simultaneous analysis of bacteria and archaea using next-generation sequencing. PLoS ONE 2014, 9, e105592. [Google Scholar]
- Hisada, T.; Endoh, K.; Kuriki, K. Inter- and intra-individual variations in seasonal and daily stabilities of the human gut microbiota in Japanese. Arch. Microbiol. 2015, 197, 919–934. [Google Scholar] [PubMed]
- Kobayashi, S.; Murakami, K.; Sasaki, S.; Okubo, H.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Comparison of relative validity of food group intakes estimated by comprehensive and brief-type self-administered diet history questionnaires against 16 d dietary records in Japanese adults. Public Health Nutr. 2011, 14, 1200–1211. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Margiotta, E.; Miragoli, F.; Callegari, M.L.; Vettoretti, S.; Caldiroli, L.; Meneghini, M.; Zanoni, F.; Messa, P. Gut microbiota composition and frailty in elderly patients with chronic kidney disease. PLoS ONE 2020, 15, e0228530. [Google Scholar] [CrossRef] [PubMed]
- Jackson, M.A.; Jeffery, I.B.; Beaumont, M.; Bell, J.T.; Clark, A.G.; Ley, R.E.; O'Toole, P.W.; Spector, T.D.; Steves, C.J. Signatures of early frailty in the gut microbiota. Genome Med. 2016, 8, 8. [Google Scholar] [CrossRef]
- Ponziani, F.R.; Picca, A.; Marzetti, E.; Calvani, R.; Conta, G.; Del Chierico, F.; Capuani, G.; Faccia, M.; Fianchi, F.; Funaro, B.; et al. Characterization of the gut-liver-muscle axis in cirrhotic patients with sarcopenia. Liver Int. Off. J. Int. Assoc. Study Liver 2021, 41, 1320–1334. [Google Scholar] [CrossRef]
- Yun, Y.; Kim, H.N.; Kim, S.E.; Heo, S.G.; Chang, Y.; Ryu, S.; Shin, H.; Kim, H.L. Comparative analysis of gut microbiota associated with body mass index in a large Korean cohort. BMC Microbiol. 2017, 17, 151. [Google Scholar] [CrossRef] [PubMed]
- Maruta, H.; Yamashita, H. Acetic acid stimulates G-protein-coupled receptor GPR43 and induces intracellular calcium influx in L6 myotube cells. PLoS ONE 2020, 15, e0239428. [Google Scholar] [CrossRef]
- Sugimura, Y.; Kanda, A.; Sawada, K.; Wai, K.M.; Tanabu, A.; Ozato, N.; Midorikawa, T.; Hisada, T.; Nakaji, S.; Ihara, K. Association between gut microbiota and body composition in Japanese general population: A focus on gut microbiota and skeletal muscle. Int. J. Environ. Res. Public Health 2022, 19, 7464. [Google Scholar] [CrossRef] [PubMed]
- Longo, P.L.; de Aquino, R.C.; Ortiz, S.R.M.; de Oliveira, R.S.; Gavioli, A.; do Amaral, J.B.; Monteiro, F.R.; de Almeida Franco, R.R.; Mereu, G.R.; Bachi, A.L.L.; et al. Effects of physical distancing by COVID-19 pandemic on diet quality, neurological and immunological markers, and fecal microbiota of Brazilian older women. Front. Nutr. 2022, 9, 972100. [Google Scholar] [CrossRef]
- Quiroga, R.; Nistal, E.; Estébanez, B.; Porras, D.; Juárez-Fernández, M.; Martínez-Flórez, S.; García-Mediavilla, M.V.; de Paz, J.A.; González-Gallego, J.; Sánchez-Campos, S.; et al. Exercise training modulates the gut microbiota profile and impairs inflammatory signaling pathways in obese children. Exp. Mol. Med. 2020, 52, 1048–1061. [Google Scholar] [CrossRef]
- Rios-Covian, D.; Gueimonde, M.; Duncan, S.H.; Flint, H.J.; de los Reyes-Gavilan, C.G. Enhanced butyrate formation by cross-feeding between Faecalibacterium prausnitzii and Bifidobacterium adolescentis. FEMS Microbiol. Lett. 2015, 362, fnv176. [Google Scholar] [CrossRef]
- Bressa, C.; Bailén-Andrino, M.; Pérez-Santiago, J.; González-Soltero, R.; Pérez, M.; Montalvo-Lominchar, M.G.; Maté-Muñoz, J.L.; Domínguez, R.; Moreno, D.; Larrosa, M. Differences in gut microbiota profile between women with active lifestyle and sedentary women. PLoS ONE 2017, 12, e0171352. [Google Scholar] [CrossRef]
- Prokopidis, K.; Giannos, P.; Kirwan, R.; Ispoglou, T.; Galli, F.; Witard, O.C.; Triantafyllidis, K.K.; Kechagias, K.S.; Morwani-Mangnani, J.; Ticinesi, A.; et al. Impact of probiotics on muscle mass, muscle strength and lean mass: A systematic review and meta-analysis of randomized controlled trials. J. Cachexia Sarcopenia Muscle 2023, 14, 30–44. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Li, J.; Zhang, Y.; Philip, A.; Shi, E.; Chi, X.; Meng, J. Influence of glucose fermentation on CO₂ assimilation to acetate in homoacetogen Blautia coccoides GA-1. J. Ind. Microbiol. Biotechnol. 2015, 42, 1217–1224. [Google Scholar] [CrossRef] [PubMed]
- Lustgarten, M.S. The Role of the Gut Microbiome on Skeletal Muscle Mass and Physical Function: 2019 Update. Front. Physiol. 2019, 10, 1435. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Men (n = 442) | Women (n = 588) | |
|---|---|---|
| Mean ± SD | Mean ± SD | |
| Age (years) | 50.5 ± 15.3 | 51.2 ± 15.9 |
| Body composition | ||
| Height (cm) | 169.4 ± 6.5 | 156.8 ± 6.3 |
| Weight (kg) | 68.9 ± 11.5 | 54.8 ± 9.2 |
| BMI (kg/m2) | 24.0 ± 3.4 | 22.3 ± 3.5 |
| Muscle strength | ||
| Grip_Ave (kg) | 41.5 ± 7.3 | 25.7 ± 4.2 |
| Grip/BMI | 1.8 ± 0.3 | 1.2 ± 0.2 |
| Nutrition | ||
| Protein (g/d) | 74.8 ± 26 | 65.8 ± 24.3 |
| Fat (g/d) | 55.3 ± 20.2 | 50.9 ± 17.8 |
| Carbohydrate (g/d) | 281.0 ± 86.0 | 218.4 ± 68.7 |
| Total dietary fiber (g/d) | 11.0 ± 4.5 | 10.6 ± 4.2 |
| Alcohol (g/d) | 23.3 ± 26.8 | 5.7 ± 12.9 |
| Lifestyle | ||
| Habitual medicine use (no, %) | 247 (55.9) | 441 (50.5) |
| (yes, %) | 195 (44.1) | 291 (49.5) |
| Exercise (no, %) | 320 (72.4) | 429 (73.0) |
| (yes, %) | 122 (27.6) | 159 (27.0) |
| Smoking (no, %) | 308 (69.7) | 544 (92.5) |
| (yes, %) | 134 (30.3) | 44 (7.5) |
| Sleep time (min/day) | 423.1 ± 69.2 | 409.4 ± 65.4 |
| Gut Microbiota | Men (n = 442) | Women (n = 588) | p-Value | |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | |||
| Read count | ||||
| Total lead | 20,395.0 ± 5244.9 | 20,505.4 ± 5536.7 | 0.989 | |
| Relative count (%) | ||||
| Akkermansia | 0.52 ± 2.38 | 0.62 ± 1.80 | <0.001 | |
| Alistipes | 1.42 ± 2.11 | 2.86 ± 3.41 | <0.001 | |
| Clostridium IV | 1.85 ± 3.16 | 3.02 ± 4.16 | <0.001 | |
| Collinsella | 5.62 ± 4.78 | 4.35 ± 4.74 | <0.001 | |
| Dorea | 0.94 ± 0.83 | 0.76 ± 0.75 | <0.001 | |
| Eggerthella | 0.14 ± 0.22 | 0.22 ± 0.30 | <0.001 | |
| Faecalibacterium | 6.48 ± 5.16 | 8.14 ± 5.47 | <0.001 | |
| Flavonifractor | 0.18 ± 0.20 | 0.25 ± 0.25 | <0.001 | |
| Fusobacterium | 0.95 ± 3.26 | 0.28 ± 1.49 | <0.001 | |
| Gemmiger | 2.11 ± 2.28 | 2.69 ± 2.58 | <0.001 | |
| Intestinibacter | 0.16 ± 0.38 | 0.21 ± 0.34 | <0.001 | |
| Lachnospiracea_incertae_sedis | 1.62 ± 1.04 | 1.96 ± 1.34 | <0.001 | |
| Oscillibacter | 0.28 ± 0.36 | 0.45 ± 0.52 | <0.001 | |
| Phascolarctobacterium | 0.71 ± 0.85 | 0.46 ± 0.67 | <0.001 | |
| Prevotella | 7.51 ± 11.89 | 3.65 ± 8.61 | <0.001 | |
| Ruminococcus | 2.45 ± 3.64 | 3.80 ± 4.77 | <0.001 | |
| Sutterella | 1.36 ± 1.62 | 0.69 ± 1.04 | <0.001 | |
| Butyricicoccus | 0.68 ± 0.51 | 0.62 ± 0.51 | 0.001 | |
| Dialister | 0.25 ± 0.51 | 0.27 ± 0.54 | 0.001 | |
| Slackia | 0.14 ± 0.38 | 0.08 ± 0.29 | 0.001 | |
| Megasphaera | 0.43 ± 1.25 | 0.28 ± 0.93 | 0.002 | |
| Odoribacter | 0.10 ± 0.22 | 0.14 ± 0.25 | 0.002 | |
| Megamonas | 1.29 ± 4.36 | 0.59 ± 2.21 | 0.004 | |
| Acidaminococcus | 0.19 ± 0.58 | 0.11 ± 0.39 | 0.010 | |
| Clostridium XlVa | 0.37 ± 0.33 | 0.43 ± 0.40 | 0.026 | |
| Mitsuokella | 0.17 ± 0.85 | 0.06 ± 0.45 | 0.051 | |
| Escherichia Shigella | 0.32 ± 1.71 | 0.40 ± 1.52 | 0.052 | |
| Bifidobacterium | 7.44 ± 8.17 | 8.10 ± 7.60 | 0.057 | |
| Erysipelotrichaceae_incertae_sedis | 0.43 ± 1.23 | 0.55 ± 1.66 | 0.061 | |
| Alloprevotella | 0.33 ± 1.34 | 0.13 ± 0.84 | 0.065 | |
| Klebsiella | 0.18 ± 1.16 | 0.04 ± 0.30 | 0.077 | |
| Paraprevotella | 0.25 ± 0.56 | 0.21 ± 0.47 | 0.089 | |
| Holdemanella | 0.87 ± 1.77 | 0.70 ± 1.68 | 0.094 | |
| Streptococcus | 1.75 ± 3.25 | 1.89 ± 3.56 | 0.100 | |
| Catenibacterium | 0.38 ± 1.37 | 0.29 ± 1.57 | 0.117 | |
| Parabacteroides | 0.96 ± 1.37 | 1.01 ± 1.17 | 0.138 | |
| Parasutterella | 0.41 ± 0.89 | 0.51 ± 0.94 | 0.264 | |
| Clostridium XlVb | 0.22 ± 0.31 | 0.19 ± 0.32 | 0.332 | |
| Ruminococcus2 | 5.78 ± 5.84 | 5.24 ± 5.37 | 0.379 | |
| Bilophila | 0.14 ± 0.20 | 0.16 ± 0.21 | 0.389 | |
| Blautia | 7.41 ± 4.16 | 7.63 ± 4.19 | 0.392 | |
| Fusicatenibacter | 2.18 ± 2.11 | 2.38 ± 2.41 | 0.408 | |
| Bacteroides | 11.32 ± 7.26 | 11.75 ± 7.40 | 0.410 | |
| Enterococcus | 0.07 ± 0.41 | 0.13 ± 0.83 | 0.431 | |
| Clostridium XVIII | 0.77 ± 1.18 | 0.70 ± 0.96 | 0.440 | |
| Veillonella | 0.64 ± 1.74 | 0.67 ± 1.43 | 0.479 | |
| Coprococcus | 0.54 ± 0.69 | 0.57 ± 0.80 | 0.482 | |
| Turicibacter | 0.30 ± 1.42 | 0.18 ± 0.43 | 0.527 | |
| Clostridium sensu stricto | 0.23 ± 0.70 | 0.17 ± 0.46 | 0.550 | |
| Barnesiella | 0.09 ± 0.25 | 0.13 ± 0.30 | 0.651 | |
| Lactobacillus | 0.52 ± 2.80 | 0.19 ± 0.83 | 0.653 | |
| Romboutsia | 0.29 ± 0.57 | 0.29 ± 0.63 | 0.666 | |
| Anaerostipes | 5.51 ± 5.91 | 5.04 ± 5.12 | 0.671 | |
| Roseburia | 3.97 ± 3.86 | 3.94 ± 3.74 | 0.897 | |
| Gut Microbiota | Men (n = 442) | Women (n = 588) | ||
|---|---|---|---|---|
| β (95%CI) | p-Value | β (95%CI) | p-Value | |
| Acidaminococcus | −0.12 (−0.17, −0.07) | <0.001 | −0.01 (−0.06, 0.03) | 0.549 |
| Allisonella | −0.83 (−1.36, −0.29) | 0.003 | −0.35 (−0.89, 0.19) | 0.201 |
| Blautia | 0.01 (0.00, 0.02) | 0.021 | 0.00 (−0.00, 0.01) | 0.666 |
| Clostridium XVIII | 0.03 (0.00, 0.05) | 0.038 | −0.01 (−0.03, 0.01) | 0.236 |
| Collinsella | −0.01 (−0.02, −0.00) | 0.005 | 0.00 (−0.00, 0.00) | 0.926 |
| Dialister | −0.07 (−0.13, −0.01) | 0.023 | −0.02 (−0.05, 0.01) | 0.189 |
| Eggerthella | 0.18 (0.04, 0.31) | 0.009 | 0.07 (0.00, 0.12) | 0.028 |
| Erysipelotrichaceae_incertae_sedis | 0.03 (0.00, 0.05) | 0.027 | −0.01 (−0.00, 0.01) | 0.611 |
| Escherichia Shigella | 0.02 (0.00, 0.04) | 0.041 | −0.00 (−0.02, 0.00) | 0.129 |
| Faecalibacterium | 0.00 (−0.00, 0.01) | 0.459 | −0.01 (−0.01, −0.00) | 0.003 |
| Parasutterella | −0.04 (−0.07, −0.00) | 0.036 | −0.03 (−0.06, 0.01) | 0.168 |
| Ruminococcus | −0.01 (−0.02, 0.00) | 0.157 | 0.00 (0.00, 0.01) | 0.047 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sugimura, Y.; Yang, Y.; Kanda, A.; Mawatari, A.; Tamada, Y.; Mikami, T.; Nakaji, S.; Ihara, K. Association between Gut Microbiota and Muscle Strength in Japanese General Population of the Iwaki Health Promotion Project. Microorganisms 2024, 12, 622. https://doi.org/10.3390/microorganisms12030622
Sugimura Y, Yang Y, Kanda A, Mawatari A, Tamada Y, Mikami T, Nakaji S, Ihara K. Association between Gut Microbiota and Muscle Strength in Japanese General Population of the Iwaki Health Promotion Project. Microorganisms. 2024; 12(3):622. https://doi.org/10.3390/microorganisms12030622
Chicago/Turabian StyleSugimura, Yoshikuni, Yichi Yang, Akira Kanda, Akihiro Mawatari, Yoshinori Tamada, Tatsuya Mikami, Shigeyuki Nakaji, and Kazushige Ihara. 2024. "Association between Gut Microbiota and Muscle Strength in Japanese General Population of the Iwaki Health Promotion Project" Microorganisms 12, no. 3: 622. https://doi.org/10.3390/microorganisms12030622
APA StyleSugimura, Y., Yang, Y., Kanda, A., Mawatari, A., Tamada, Y., Mikami, T., Nakaji, S., & Ihara, K. (2024). Association between Gut Microbiota and Muscle Strength in Japanese General Population of the Iwaki Health Promotion Project. Microorganisms, 12(3), 622. https://doi.org/10.3390/microorganisms12030622