

Ten-Year Analysis of Bacterial Colonisation and Outcomes of Major Burn Patients with a Focus on Pseudomonas aeruginosa

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Patient Eligibility
2.2. Defining Common Factors
2.3. Statistical Analysis
3. Results
3.1. Factors Tested
3.2. Species of Microorganisms
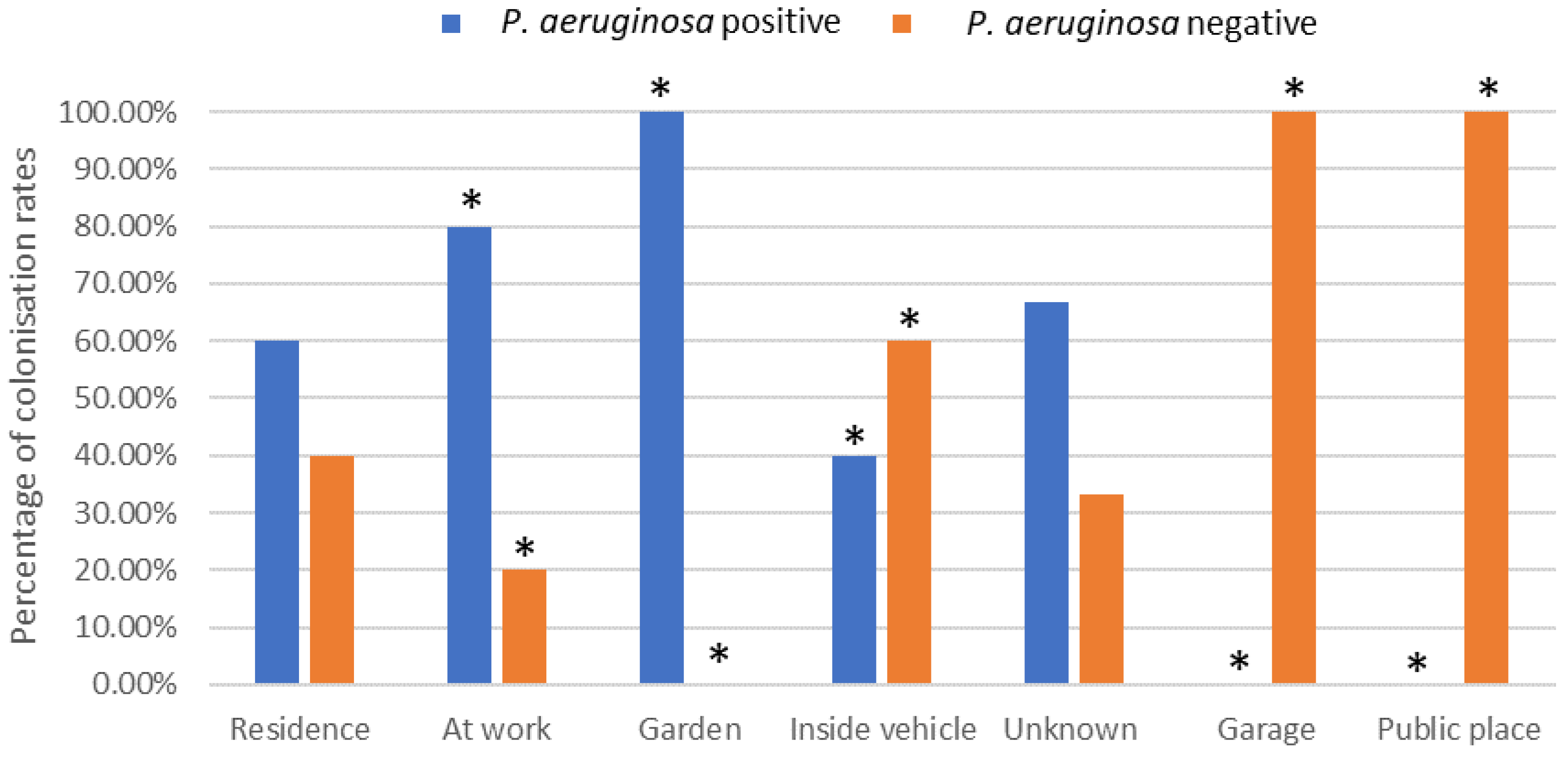
3.3. Environment
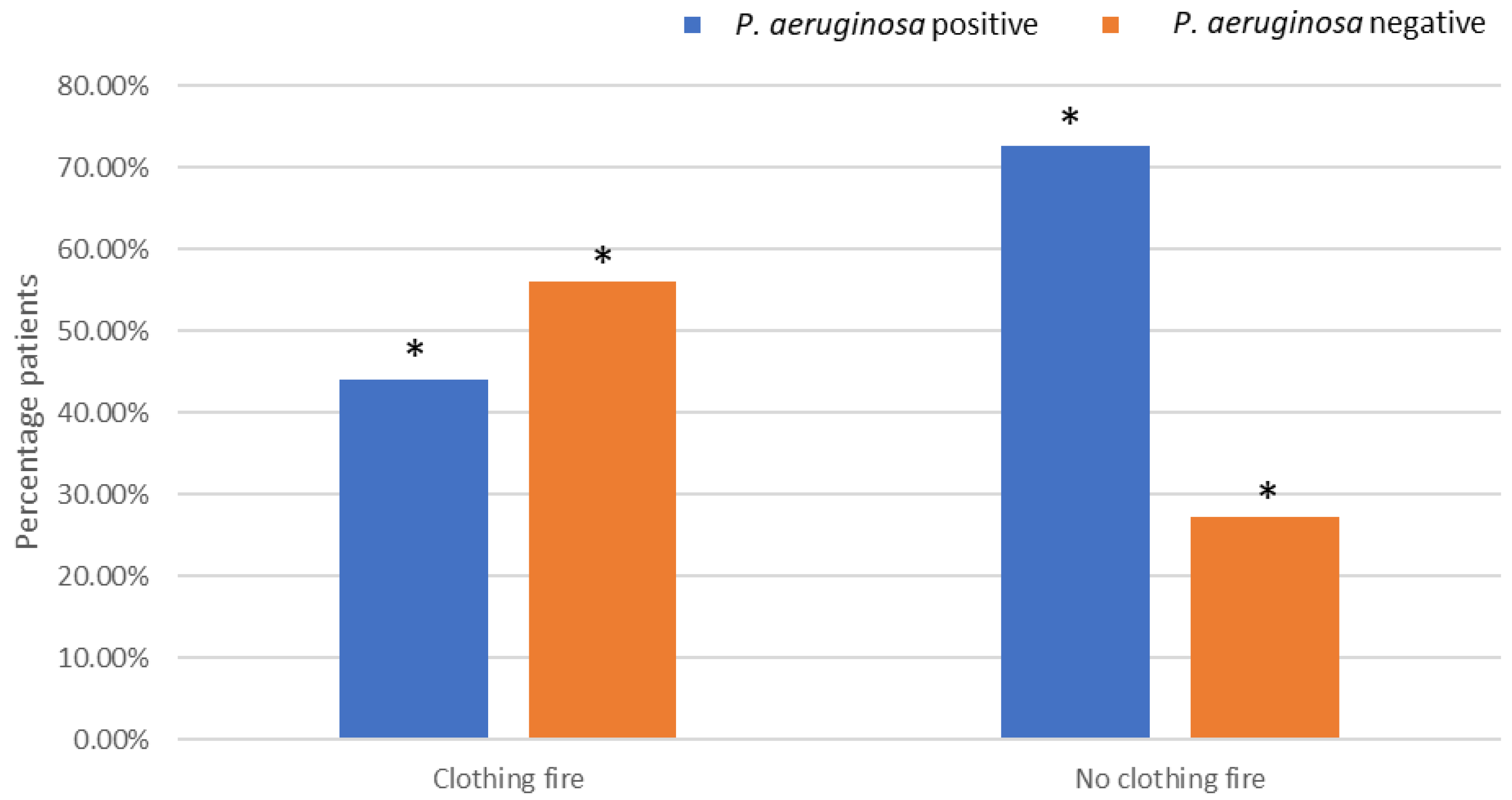
3.4. Clothing Fire
3.5. Number of Surgeries
3.6. Mental Health Illness and Substance Abuse
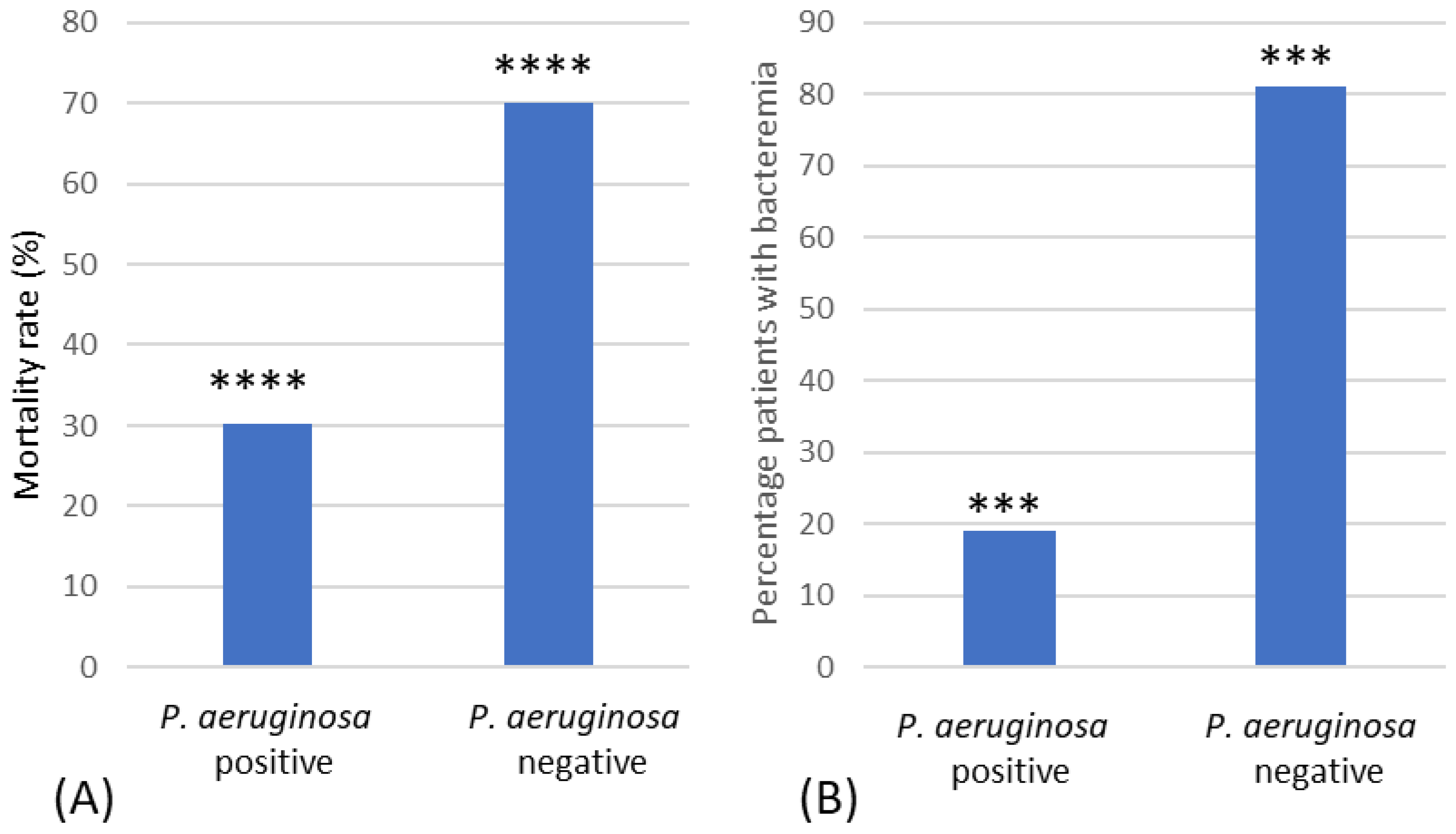
3.7. Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Whitaker, I.S.; Shokrollahi, K.; Dickson, W.A. Burns (Oxford Specialist Handbooks in Surgery); Oxford University Press: Oxford, UK, 2019; Chapter 2: Incidence and Epidemiology. [Google Scholar]
- Sevgi, M.; Toklu, A.; Vecchio, D.; Hamblin, M.R. Topical antimicrobials for burn infections—An update. Recent Pat. Anti-Infect. Drug Discov. 2013, 8, 161–197. [Google Scholar] [CrossRef]
- Krishnan, P.; Frew, Q.; Green, A.; Martin, R.; Dziewulski, P. Cause of death and correlation with autopsy findings in burns patients. Burns 2013, 39, 583–588. [Google Scholar] [CrossRef]
- Azzopardi, E.; Azzopardi, E.; Camilleri, L.; Villapalos, J.; Boyce, D.E.; Dziewulski, P.; Dickson, W.A.; Whitaker, I.S. Gram negative wound infection in hospitalised adult burn patients—Systematic review and metanalysis. PLoS ONE 2014, 9, e95042. [Google Scholar] [CrossRef]
- Strateva, T.; Yordanov, D. Pseudomonas aeruginosa—A phenomenon of bacterial resistance. J. Med. Microbiol. 2009, 58, 1133–1148. [Google Scholar] [CrossRef]
- Yoon, S.S.; Hennigan, R.F.; Hilliard, G.M.; Ochsner, U.A.; Parvatiyar, K.; Kamani, M.C.; Allen, H.L.; DeKievit, T.R.; Gardner, P.R.; Schwab, U.; et al. Pseudomonas aeruginosa anaerobic respiration in biofilms: Relationships to cystic fibrosis pathogenesis. Dev. Cell 2002, 3, 593–603. [Google Scholar] [CrossRef]
- Mah, T.-F.; Pitts, B.; Pellock, B.; Walker, G.C.; Stewart, P.S.; O’Toole, G.A. A genetic basis for Pseudomonas aeruginosa biofilm antibiotic resistance. Nature 2003, 426, 306–310. [Google Scholar] [CrossRef]
- DeLeon, S.; Clinton, A.; Fowler, H.; Everett, J.; Horswill, A.R.; Rumbaugh, K.P. Synergistic interactions of Pseudomonas aeruginosa and Staphylococcus aureus in an in vitro wound model. Infect. Immun. 2014, 82, 4718–4728. [Google Scholar] [CrossRef]
- Maslova, E.; Eisaiankhongi, L.; Sjöberg, F.; McCarthy, R. Burns and biofilms: Priority pathogens and in vivo models. NPJ Biofilms Microbiomes 2021, 7, 73–82. [Google Scholar] [CrossRef]
- Wanis, M.; Walker, S.A.N.; Daneman, N.; Elligsen, M.; Palmay, L.; Simor, A.; Cartotto, R. Impact of hospital length of stay on the distribution of Gram negative bacteria and likelihood of isolating a resistant organism in a Canadian burn center. Burns 2016, 42, 104–111. [Google Scholar] [CrossRef]
- Altoparlak, U.; Erol, S.; Akcan, M.N.; Celebi, F.; Kadanali, A. The time-related changes of antimicrobial resistance patterns and predominant bacterial profiles of burn wounds and body flora of burned patients. Burns 2004, 30, 660–664. [Google Scholar] [CrossRef]
- Church, N.A.; McKillip, J.L. Antibiotic resistance crisis: Challenges and imperatives. Biologia 2021, 76, 1535–1550. [Google Scholar] [CrossRef]
- Shareen George, K.G.; Basavarajappa, A.R.; Hanumanthappa, A.R. Bacteriological study of burns infection. J. Evol. Med. Dent. Sci. 2015, 4, 14216–14224. [Google Scholar] [CrossRef]
- Hassen, A.F.; Khalifa, S.B.; Daiki, M. Epidemiological and bacteriological profiles in children with burns. Burns 2014, 40, 1040–1045. [Google Scholar] [CrossRef] [PubMed]
- Tredget, E.E.; Shankowsky, H.A.; Joffe, A.M.; Inkson, T.I.; Volpel, K.; Paranchych, W.; Kibsey, P.C.; Alton, J.D.M.; Burke, J.F. Epidemiology of infections with Pseudomonas aeruginosa in burn patients: The role of hydrotherapy. Clin. Inf. Dis. 1992, 15, 941–949. [Google Scholar] [CrossRef] [PubMed]
- Barret, J.; Herndon, D. Effects of burn wound excision on bacterial colonization and invasion. Plast. Reconstr. Surg. 2003, 111, 744–750. [Google Scholar] [CrossRef] [PubMed]
- Bang, R.L.; Gang, R.K.; Sanyal, S.C.; Mokaddas, E.M.; Lari, A.R.A. Beta- haemolytic Streptococcus infection in burns. Burns 1999, 25, 242–246. [Google Scholar] [CrossRef] [PubMed]
- Ramzy, P.; Wolf, S.; Irtun, O.; Hart, D.W.; Thompson, J.C.; Herdon, D.N. Gut epithelial apoptosis after severe burn: Effects of gut hypoperfusion. J. Am. Coll. Surg. 2000, 190, 281–287. [Google Scholar] [CrossRef]
- Weber, J.; Sheridan, R.; Pasternack, M.; Tompkins, R.G. Nosocomial infections in pediatric patients with burns. Am. J. Inf. Con. 1997, 25, 195–201. [Google Scholar] [CrossRef]
- Smith, K.; Rajendran, R.; Kerr, S.; Lappin, D.F.; Mackay, W.G.; Williams, C.; Ramage, G. Aspergillus fumigatus enhances elastase production in Pseudomonas aeruginosa co-cultures. Med. Mycol. 2015, 53, 645–655. [Google Scholar] [CrossRef]
- Reece, E.; Doyle, S.; Greally, P.; Renwick, J.; McClean, S. Aspergillus fumigatus Inhibits Pseudomonas aeruginosa in Co-culture: Implications of a Mutually Antagonistic Relationship on Virulence and Inflammation in the CF Airway. Front. Microbiol. 2018, 9, 1205–1219. [Google Scholar] [CrossRef]
- Mousa, H.A.-L.; Al-Bader, S.M. Yeast infection of burns. Mycoses 2001, 44, 147–149. [Google Scholar] [CrossRef] [PubMed]
- Capoor, M.R.; Gupta, S.; Sarabahi, S.; Mishra, A.; Tiwari, V.K.; Aggarwal, P. Epidemiological and clinico-mycological profile of fungal wound infection from largest burn centre in Asia. Mycoses 2012, 55, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Akhavan, A.A.; Shamoun, F.; Lagziel, T.; Rostami, S.; Cox, C.A.; Cooney, C.M.; Sood, G.; Hultman, C.S.; Caffrey, J.A. Invasive Non-Candida Fungal Infections in Acute Burns—A 13-Year Review of a Single Institution and Review of the Literature. J. Burn Care Res. 2023, 44, 1005–1012. [Google Scholar] [CrossRef] [PubMed]
- Muguregowda, H. An observational study on clothing characteristics involved as major contributors in sustaining domestic burns injuries. World J. Plas. Surg. 2019, 8, 293–297. [Google Scholar]
- Mahendraraj, K.; Durgan, D.M.; Chamberlain, R.S. Acute mental disorders and short and long term morbidity in patients with third degree flame burn: A population-based outcome study of 96,451 patients from the Nationwide Inpatient Sample (NIS) database (2001–2011). Burns 2016, 42, 1766–1773. [Google Scholar] [CrossRef]
- Nam, J.; Sljivic, S.; Matthews, R.; Pak, J.; Agala, C.; Salamah, H.; Hatch, E.; Nizamani, R.; King, B.; Laughon, S.L.; et al. The cost of mental health comorbid conditions in burn patients: A single-site experience. J. Burn Care Res. 2023, 44, 751–757. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factor | Subgroup | Significance |
|---|---|---|
| Species of microorganisms | Gram-negative bacteria | N/A |
| Gram-positive bacteria | N/A | |
| Yeast and fungi | N/A | |
| Environment | Inside a place of residence | No |
| Inside a vehicle | Yes | |
| In a public place | Yes | |
| At work | Yes | |
| In a garden | Yes | |
| In a garage | Yes | |
| Unknown location | No | |
| Location of burn | Scalp | No |
| Face and head | No | |
| Neck | No | |
| Chest | No | |
| Abdomen | No | |
| Upper limb | No | |
| Hands | No | |
| Back | No | |
| Buttocks | No | |
| Perineum and genitalia | No | |
| Lower limb | No | |
| Feet | No | |
| Type of burn | Flame burns | Numbers too small |
| Scalds | Numbers too small | |
| Flash burns | Numbers too small | |
| Contact burns | Numbers too small | |
| Radiation burns | Numbers too small | |
| Explosions | Numbers too small | |
| Clothing fire | Yes | |
| Hospitals | Admission from other hospitals | Numbers too small |
| Intubation | The number of intubated patients | No |
| Location of intubation | No | |
| Surgeries and length of stay | Number of surgeries | Yes |
| Length of stay | Yes | |
| First aid | Unknown | Numbers too small |
| Water | Numbers too small | |
| Cling film | Numbers too small | |
| Co-morbidities | Mental health issues | Yes |
| Substance abuse | Yes | |
| Mental health issues and substance abuse | Yes | |
| Mortality | Mortality rate | Yes |
| Mortality with P. aeruginosa bacteraemia | Yes | |
| Age | No | |
| Total body surface area (%) | No | |
| Type of antibiotic | Tazocin | No |
| Meropenem | No | |
| Vancomycin | No | |
| Clindamycin | No | |
| Amphotericin | No | |
| Colomycin | No | |
| Clarithromycin | No | |
| Co-trimoxazole | No | |
| Gentamicin | No | |
| Flucloxacillin | No | |
| Benzylpenicillin | No | |
| Co-amoxiclav | No | |
| Cefuroxime | No | |
| Erythromycin | No | |
| Tobramycin | No | |
| Amoxicillin | No | |
| Ciprofloxacin | No |
| P. aeruginosa-Positive Culture (%) | P. aeruginosa-Negative Culture (%) | P. aeruginosa-Positive Culture (%) | P. aeruginosa-Negative Culture (%) | ||
|---|---|---|---|---|---|
| Acinetobacter baumannii | 14.8 | 5 | Bacillus cereus | 0 | 5 |
| Acinetobacter lwoffii | 3.7 | 0 | Clostridium difficile | 3.7 | 0 |
| Aeromonas hydrophila | 3.7 | 5 | Enterococcus faecalis | 40.7 | 30 |
| Citrobacter freundii | 14.8 | 5 | Enterococcus faecium | 11.1 | 10 |
| Cronobacter sakazakii | 0 | 5 | Staphylococcus aureus | 40.7 | 55 |
| Enterobacter cloacae | 29.6 | 20 | Staphylococcus epidermidis | 3.7 | 5 |
| Escherichia coli | 33.3 | 30 | Methicillin-resistant Staphylococcus aureus (MRSA) | 18.5 | 10 |
| Escherichia vulneris | 3.7 | 0 | Streptococcus milleri | 3.7 | 0 |
| Haemophilus influenzae | 14.8 | 5 | Streptococcus pneumoniae | 11.1 | 10 |
| Klebsiella pneumoniae | 0 | 15 | Streptococcus oralis | 0 | 5 |
| Klebsiella oxytoca | 0 | 10 | Viridans group streptococci (VGS) | 0 | 5 |
| Leclercia adecarboxylata | 7.4 | 0 | Group A Streptococcus | 0 | 5 |
| Moraxella catarrhalis | 3.7 | 5 | Group B Streptococcus | 11.1 | 10 |
| Morganella morganii | 0 | 5 | Group C Streptococcus | 3.7 | 10 |
| Neisseria meningitidis | 0 | 5 | Group G Streptococcus | 3.7 | 5 |
| Proteus mirabilis | 3.7 | 0 | Group F Streptococcus | 0 | 5 |
| Proteus vulgaris | 0 | 5 | |||
| Pseudomonas aeruginosa | 57.45 | 43 | Fungi and yeast | ||
| Pseudomonas putida | 3.7 | 0 | Aspergillus fumigatus | 0 | 5 |
| Raoultella planticola | 3.7 | 0 | Candida albicans | 29.7 | 25 |
| Serratia marcescens | 0 | 5 | Candida dubliniensis | 3.7 | 0 |
| Serratia liquefaciens | 0 | 5 | Candida glabrata | 3.7 | 0 |
| Stenotrophomonas maltophilia | 18.5 | 10 | Candida parapsilosis | 11.1 | 5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gomersall, J.; Mortimer, K.; Hassan, D.; Whitehead, K.A.; Slate, A.J.; Ryder, S.F.; Chambers, L.E.; El Mohtadi, M.; Shokrollahi, K. Ten-Year Analysis of Bacterial Colonisation and Outcomes of Major Burn Patients with a Focus on Pseudomonas aeruginosa. Microorganisms 2024, 12, 42. https://doi.org/10.3390/microorganisms12010042
Gomersall J, Mortimer K, Hassan D, Whitehead KA, Slate AJ, Ryder SF, Chambers LE, El Mohtadi M, Shokrollahi K. Ten-Year Analysis of Bacterial Colonisation and Outcomes of Major Burn Patients with a Focus on Pseudomonas aeruginosa. Microorganisms. 2024; 12(1):42. https://doi.org/10.3390/microorganisms12010042
Chicago/Turabian StyleGomersall, Jenny, Kalani Mortimer, Deniz Hassan, Kathryn A. Whitehead, Anthony J. Slate, Steven F. Ryder, Lucy E. Chambers, Mohamed El Mohtadi, and Kayvan Shokrollahi. 2024. "Ten-Year Analysis of Bacterial Colonisation and Outcomes of Major Burn Patients with a Focus on Pseudomonas aeruginosa" Microorganisms 12, no. 1: 42. https://doi.org/10.3390/microorganisms12010042
APA StyleGomersall, J., Mortimer, K., Hassan, D., Whitehead, K. A., Slate, A. J., Ryder, S. F., Chambers, L. E., El Mohtadi, M., & Shokrollahi, K. (2024). Ten-Year Analysis of Bacterial Colonisation and Outcomes of Major Burn Patients with a Focus on Pseudomonas aeruginosa. Microorganisms, 12(1), 42. https://doi.org/10.3390/microorganisms12010042