


Co-Circulation of SARS-CoV-2 and Other Respiratory Pathogens in Upper and Lower Respiratory Tracts during Influenza Season 2022–2023 in Lazio Region

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
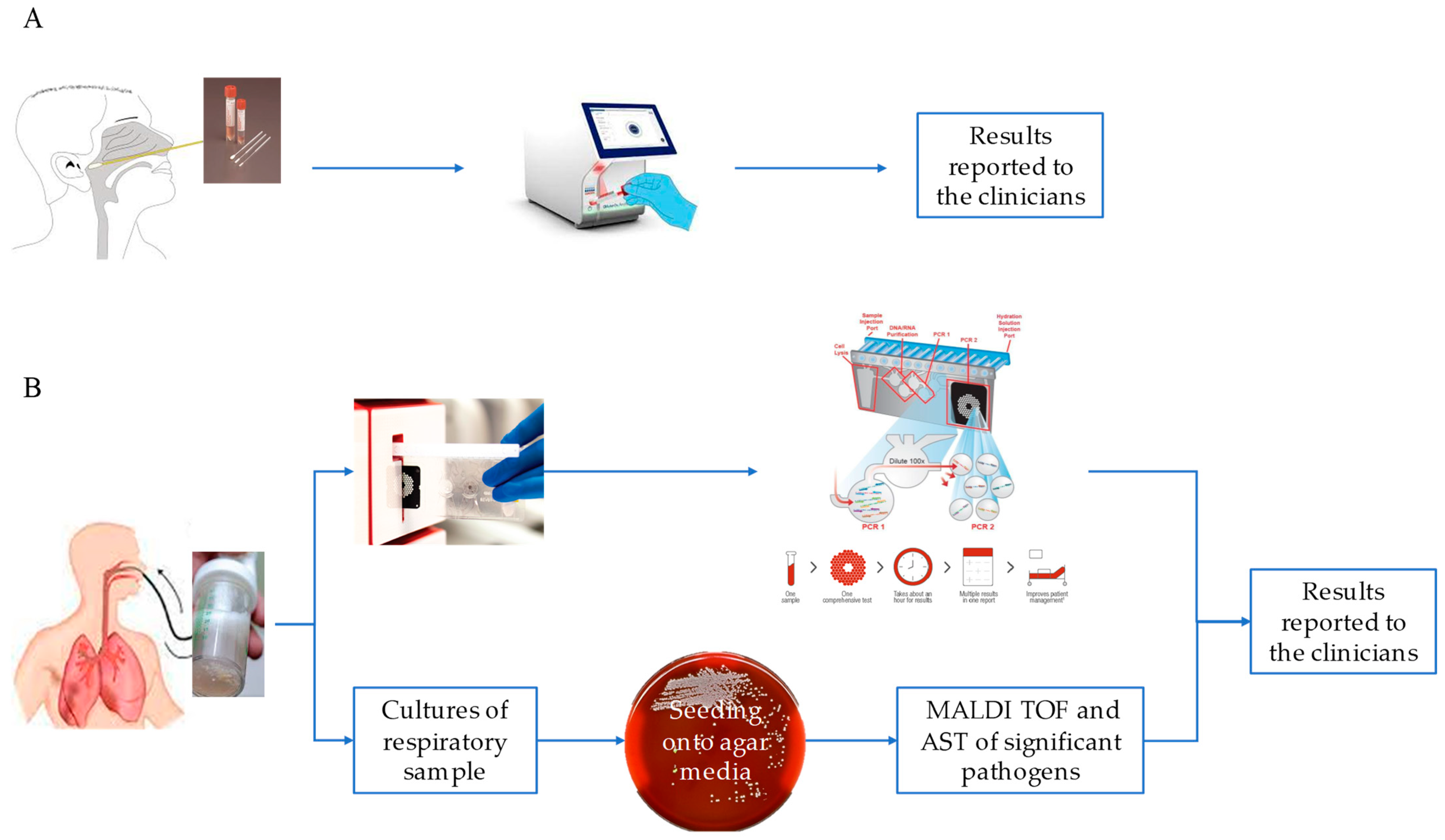
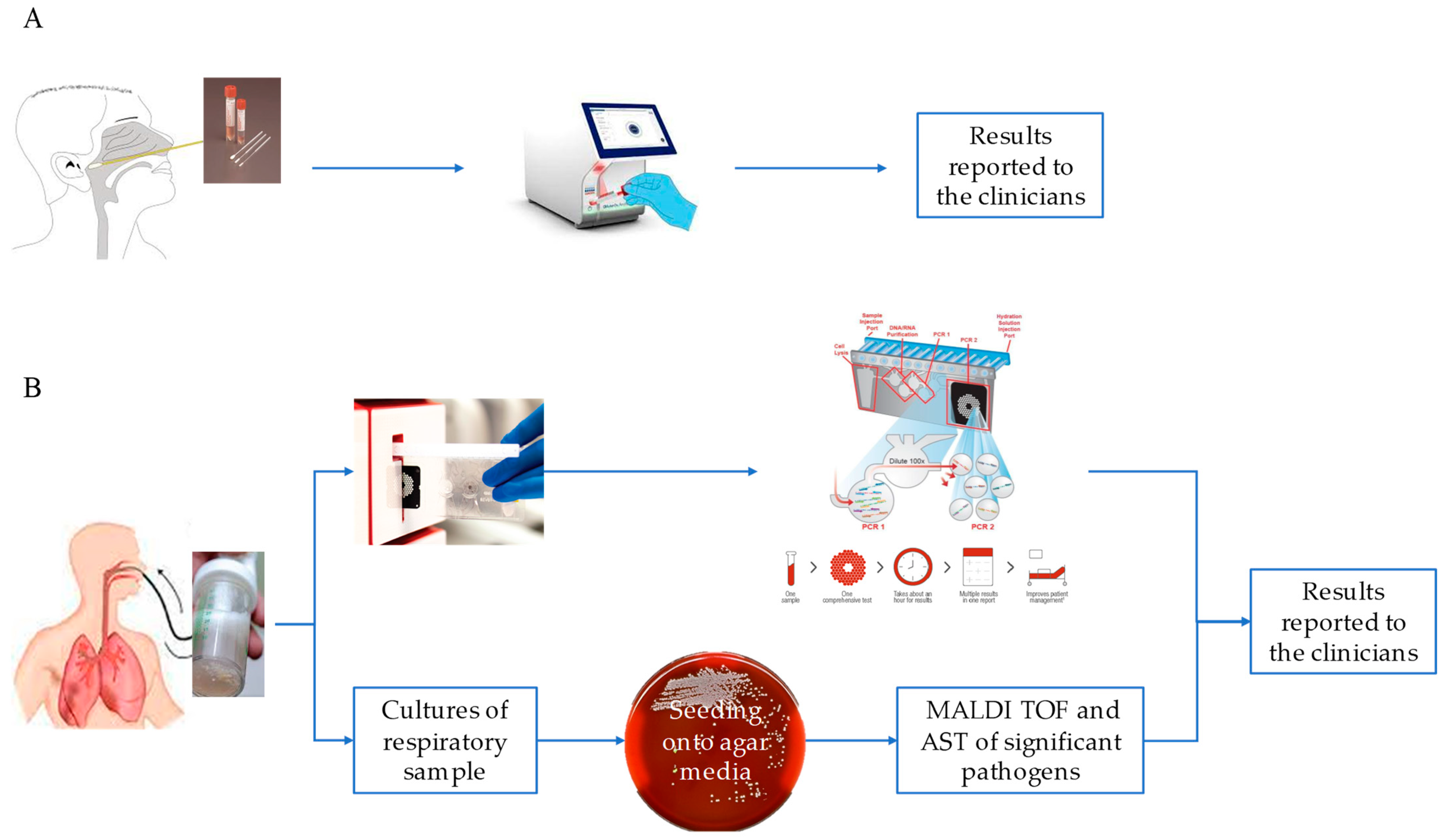
2.1. Study Population and Sample Collection
2.2. Molecular Assays
2.3. Statistical Evaluation
2.4. Culture
3. Results and Discussion
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Safiri, S.; Mahmoodpoor, A.; Kolahi, A.A.; Nejadghaderi, S.A.; Sullman, M.J.M.; Mansournia, M.A.; Ansarin, K.; Collins, G.S.; Kaufman, J.S.; Abdollahi, M. Global burden of lower respiratory infections during the last three decades. Front. Public. Health 2023, 10, 1028525. [Google Scholar] [CrossRef] [PubMed]
- Calderaro, A.; Buttrini, M.; Farina, B.; Montecchini, S.; De Conto, F.; Chezzi, C. Respiratory Tract Infections and Laboratory Diagnostic Methods: A Review with A Focus on Syndromic Panel-Based Assays. Microorganisms 2022, 10, 1856. [Google Scholar] [CrossRef] [PubMed]
- Hedberg, P.; Ternhag, A.; Giske, C.G.; Strålin, K.; Özenci, V.; Johansson, N.; Spindler, C.; Hedlund, J.; Mårtensson, J.; Nauclér, P. Ventilator-Associated Lower Respiratory Tract Bacterial Infections in COVID-19 Compared with Non-COVID-19 Patients. Crit. Care Med. 2022, 50, 825–836. [Google Scholar] [CrossRef] [PubMed]
- Pandey, M.; May, A.; Tan, L.; Hughes, H.; Jones, J.P.; Harrison, W.; Bradburn, S.; Tyrrel, S.; Muthuswamy, B.; Berry, N.; et al. Comparative incidence of early and late bloodstream and respiratory tract co-infection in patients admitted to ICU with COVID-19 pneumonia versus Influenza A or B pneumonia versus no viral pneumonia: Wales multicentre ICU cohort study. Crit. Care 2022, 26, 158. [Google Scholar] [CrossRef] [PubMed]
- Maltezou, H.C.; Papanikolopoulou, A.; Vassiliu, S.; Theodoridou, K.; Nikolopoulou, G.; Sipsas, N.V. COVID-19 and Respiratory Virus Co-Infections: A Systematic Review of the Literature. Viruses 2023, 15, 865. [Google Scholar] [CrossRef] [PubMed]
- Fan, H.; Zhou, L.; Lv, J.; Yang, S.; Chen, G.; Liu, X.; Han, C.; Tan, X.; Qian, S.; Wu, Z.; et al. Bacterial coinfections contribute to severe COVID-19 in winter. Cell Res. 2023, 33, 562–564. [Google Scholar] [CrossRef] [PubMed]
- Bantun, F. Fungal-Bacterial Co-Infections and Super-Infections among Hospitalized COVID-19 Patients: A Systematic Review. J. Fungi 2023, 9, 598. [Google Scholar] [CrossRef] [PubMed]
- EUCAST. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 10.0. 2020. Available online: https://www.eucast.org/ (accessed on 1 January 2020).
- EUCAST. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 11.0. 2021. Available online: https://www.eucast.org/ (accessed on 1 January 2021).
- EUCAST. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 10.0. 2022. Available online: https://www.eucast.org/ (accessed on 1 January 2022).
- Alqahtani, A.; Alamer, E.; Mir, M.; Alasmari, A.; Alshahrani, M.M.; Asiri, M.; Ahmad, I.; Alhazmi, A.; Algaissi, A. Bacterial Coinfections Increase Mortality of Severely Ill COVID-19 Patients in Saudi Arabia. Int. J. Environ. Res. Public. Health 2022, 19, 2424. [Google Scholar] [CrossRef] [PubMed]
- Soltani, S.; Faramarzi, S.; Zandi, M.; Shahbahrami, R.; Jafarpour, A.; Akhavan Rezayat, S.; Pakzad, I.; Abdi, F.; Malekifar, P.; Pakzad, R. Bacterial coinfection among coronavirus disease 2019 patient groups: An updated systematic review and meta-analysis. New Microbes New Infect. 2021, 43, 100910. [Google Scholar] [CrossRef] [PubMed]
- Mirzaei, R.; Goodarzi, P.; Asadi, M.; Soltani, A.; Aljanabi, H.A.A.; Jeda, A.S.; Dashtbin, S.; Jalalifar, S.; Mohammadzadeh, R.; Teimoori, A.; et al. Bacterial co-infections with SARS-CoV-2. IUBMB Life 2020, 72, 2097–2111. [Google Scholar] [CrossRef] [PubMed]
- Bengoechea, J.A.; Bamford, C.G. SARS-CoV-2, bacterial co-infections, and AMR: The deadly trio in COVID-19? EMBO Mol. Med. 2020, 12, e12560. [Google Scholar] [CrossRef] [PubMed]
- Zheng, B.; Xiao, Y.; Tong, B.; Mao, Y.; Ge, R.; Tian, F.; Dong, X.; Zheng, P. S373P Mutation Stabilizes the Receptor-Binding Domain of the Spike Protein in Omicron and Promotes Binding. JACS Au 2023, 3, 1902–1910. [Google Scholar] [CrossRef] [PubMed]
- Harvey, W.T.; Carabelli, A.M.; Jackson, B.; Gupta, R.K.; Thomson, E.C.; Harrison, E.M.; Ludden, C.; Reeve, R.; Rambaut, A.; COVID-19 Genomics UK (COG-UK) Consortium; et al. SARS-CoV-2 variants, spike mutations and immune escape. Nat. Rev. Microbiol. 2021, 19, 409–424. [Google Scholar] [CrossRef] [PubMed]
- Lansbury, L.; Lim, B.; Baskaran, V.; Lim, W.S. Co-infections in people with COVID-19: A systematic review and meta-analysis. J. Infect. 2020, 81, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Massey, B.W.; Jayathilake, K.; Meltzer, H.Y. Respiratory microbial co-infection with SARS-CoV-2. Front. Microbiol. 2020, 11, 2079. [Google Scholar] [CrossRef] [PubMed]
- Piltcher, O.B.; Kosugi, E.M.; Sakano, E.; Mion, O.; Testa, J.R.G.; Romano, F.R.; Santos, M.C.J.; Di Francesco, R.C.; Mitre, E.I.; Bezerra, T.F.P.; et al. How to avoid the inappropriate use of antibiotics in upper respiratory tract infections? A position statement from an expert panel. Braz. J. Otorhinolaryngol. 2018, 84, 265–279. [Google Scholar] [CrossRef] [PubMed]
- Majumder, M.A.A.; Rahman, S.; Cohall, D.; Bharatha, A.; Singh, K.; Haque, M.; Gittens-St Hilaire, M. Antimicrobial Stewardship: Fighting Antimicrobial Resistance and Protecting Global Public Health. Infect. Drug Resist. 2020, 13, 4713–4738. [Google Scholar] [CrossRef] [PubMed]
- Van Der Westhuyzen, M.; Samodien, N.; Brink, A.J.; Moodley, C. Utility of the BioFire® FilmArray® Pneumonia Panel plus assay for syndromic testing of lower respiratory tract infections in a low/middle-income setting. JAC Antimicrob. Resist. 2023, 5, dlac139. [Google Scholar] [CrossRef] [PubMed]
- Fontana, C.; Favaro, M.; Minelli, S.; Bossa, M.C.; Altieri, A. Co-infections observed in SARS-CoV-2 positive patients using a rapid diagnostic test. Sci. Rep. 2021, 11, 16355. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Total | SARS-CoV-2 Positive Other Respiratory Pathogens Positive | SARS-CoV-2 Negative Other Respiratory Pathogens Positive | SARS-CoV-2 Positive Other Respiratory Pathogens Negative | |||||
|---|---|---|---|---|---|---|---|---|
| NPS | BAL | NPS | BAL | NPS | BAL | NPS | BAL | |
| Number of patients (%) | 306 (80.31) | 75 (19.67) | 9 (2.36) | 14 (3.67) | 193 (50.66) | 57 (14.96) | 104 (27.30) | 4 (1.05) |
| Male (%) | 173 (56.54) | 44 (58.67) | 4 (44.44) | 10 (71.43) | 103 (53.37) | 33 (57.89) | 66 (63.46) | 1 (25.00) |
| Female (%) | 133 (43.46) | 31 (41.33) | 5 (55.56) | 4 (28.57) | 90 (46.63) | 24 (42.11) | 38 (36.54) | 3 (75.00) |
| Median age (years) (±SD) | 71 (±19.7) | 66 (±17.8) | 71 (±20.7) | 76.5 (±15.1) | 67 (±21.9) | 63 (±18.2) | 74.5 (±13.9) | 70.5 (±10.6) |
| NPS | BAL | |
|---|---|---|
| Renal failure | 0.8 | - |
| Respiratory failure | 0.8 | - |
| Cerebral ischemia | 0.8 | - |
| Cytomegalic disease | 0.8 | - |
| Alveolar and parietoalveolar pneumopathies | 0.8 | - |
| Severe sepsis | 0.8 | - |
| Pleural effusion | 0.8 | - |
| Complications of liver transplantation | 1.7 | - |
| Influenza | 1.7 | - |
| Meningitis | 2.5 | - |
| HIV-1 complications | 5.0 | - |
| Bacterial pneumonia | 5.0 | 6.7 |
| Viral pneumonia | 5.9 | - |
| Suspected tuberculosis | 5.9 | 6.7 |
| COVID-19 pneumonia | 24.2 | - |
| COVID-19 respiratory distress syndrome | 42.5 | 86.6 |
| Pathogens | Percentage | |||
|---|---|---|---|---|
| NPS (SARS-CoV-2 Negative) | NPS (SARS-CoV-2 Positive) | BAL (SARS-CoV-2 Negative) | BAL (SARS-CoV-2 Positive) | |
| Influenza A/B | 29.53% | 11.11% | 10.67% | - |
| Parainfluenza Virus | 5.18% | - | 4.00% | - |
| RSV | 26.42% | 11.11% | 5.33% | - |
| Rhino/Entero | 23.32% | 44.44% | 6.67% | - |
| Metapneumo Virus | 13.99% | 22.22% | 4.00% | - |
| Adenovirus | 2.59% | - | 4.00% | - |
| Coronavirus (non-SARS-CoV-2) | 4.66% | 33.33% | 2.67% | - |
| B. pertussis | 1.55% | - | - | - |
| A. baumannii complex | - | - | 1.33% | - |
| P. aeruginosa | - | - | 22.67% | 35.71% |
| Proteus spp. | - | - | 5.33% | 14.28% |
| K. oxytoca | - | - | 5.33% | 7.14% |
| K. pneumoniae group | - | - | 9.33% | 14.28% |
| E. cloacae complex | - | - | 4.00% | - |
| E. coli | - | - | 6.67% | 7.14% |
| S. aureus | - | - | 21.33% | 21.43% |
| H. influenzae | - | - | 9.33% | 14.28% |
| S. pneumoniae | - | - | 2.67% | 7.14% |
| L. pneumophila | - | - | 1.33% | - |
| K. aerogenes | - | - | 1.33% | - |
| S. marcescens | - | - | 2.67% | - |
| S. pyogenes | - | - | 1.33% | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bordi, L.; Vulcano, A.; Sberna, G.; Nonis, M.; Giacomini, P.; Maggi, F.; Fontana, C.; Lalle, E. Co-Circulation of SARS-CoV-2 and Other Respiratory Pathogens in Upper and Lower Respiratory Tracts during Influenza Season 2022–2023 in Lazio Region. Microorganisms 2023, 11, 2239. https://doi.org/10.3390/microorganisms11092239
Bordi L, Vulcano A, Sberna G, Nonis M, Giacomini P, Maggi F, Fontana C, Lalle E. Co-Circulation of SARS-CoV-2 and Other Respiratory Pathogens in Upper and Lower Respiratory Tracts during Influenza Season 2022–2023 in Lazio Region. Microorganisms. 2023; 11(9):2239. https://doi.org/10.3390/microorganisms11092239
Chicago/Turabian StyleBordi, Licia, Antonella Vulcano, Giuseppe Sberna, Marino Nonis, Paolo Giacomini, Fabrizio Maggi, Carla Fontana, and Eleonora Lalle. 2023. "Co-Circulation of SARS-CoV-2 and Other Respiratory Pathogens in Upper and Lower Respiratory Tracts during Influenza Season 2022–2023 in Lazio Region" Microorganisms 11, no. 9: 2239. https://doi.org/10.3390/microorganisms11092239
APA StyleBordi, L., Vulcano, A., Sberna, G., Nonis, M., Giacomini, P., Maggi, F., Fontana, C., & Lalle, E. (2023). Co-Circulation of SARS-CoV-2 and Other Respiratory Pathogens in Upper and Lower Respiratory Tracts during Influenza Season 2022–2023 in Lazio Region. Microorganisms, 11(9), 2239. https://doi.org/10.3390/microorganisms11092239