
Safety and Tolerability of Six Months of Isoniazid Plus Pyridoxine or Three Months of Rifampicin for Tuberculosis among Subjects with Diabetes Mellitus: A Randomized Trial

 , ,
, ,  , , , and
, , , and
Abstract
1. Introduction
2. Methods
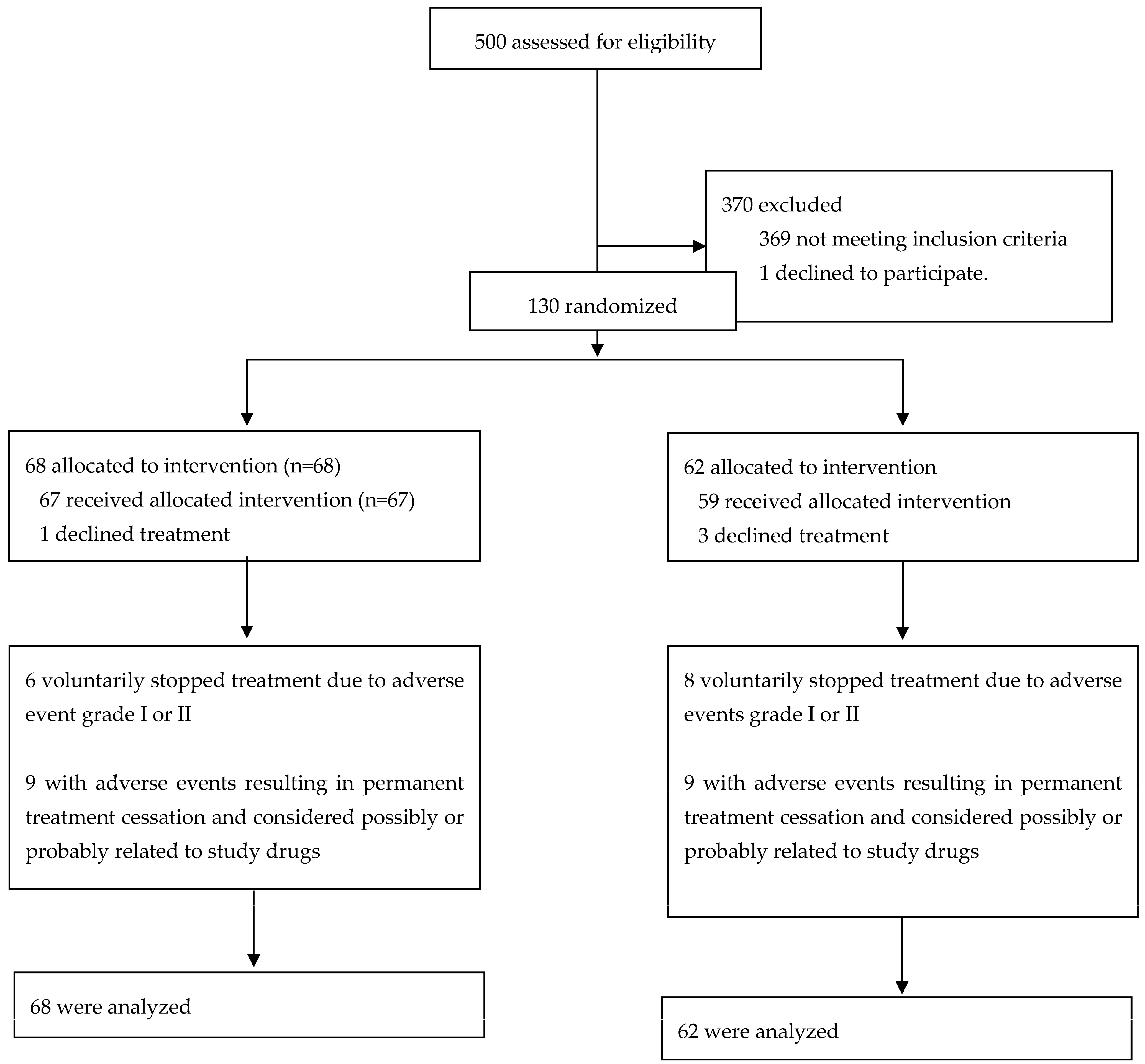
2.1. Study Design, Participants, and Randomization
2.2. Procedures
2.3. Outcomes
2.4. Statistical Analysis
2.5. Ethical Considerations
2.6. Role of the Funding Source
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Control: WHO Report 2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/336069/9789240013131 (accessed on 2 March 2021).
- Lin, Y.; Harries, A.; Kumar, A.; Critchley, J.; van Crevel, R.; Owiti, P.; Dlodlo, R.A.; Dejgaard, A. Management of Diabetes Mellitus-Tuberculosis: A Guide to the Essential Practice; International Union against Tuberculosis and Lung Disease (The Union): Paris, France, 2019. [Google Scholar]
- Jeon, C.Y.; Murray, M.B. Diabetes mellitus increases the risk of active tuberculosis: A systematic review of 13 observational studies. PLoS Med. 2008, 5, e152. [Google Scholar]
- Baker, M.A.; Harries, A.D.; Jeon, C.Y.; Hart, J.E.; Kapur, A.; Lonnroth, K.; Ottmani, S.-E.; Goonesekera, S.D.; Murray, M.B. The impact of diabetes on tuberculosis treatment outcomes: A systematic review. BMC Med. 2011, 9, 81. [Google Scholar] [CrossRef] [PubMed]
- Jimenez-Corona, M.E.; Cruz-Hervert, L.P.; Garcia-Garcia, L.; Ferreyra-Reyes, L.; Delgado-Sanchez, G.; Bobadilla-Del-Valle, M.; Canizales-Quintero, S.; Ferreira-Guerrero, E.; Báez-Saldaña, R.; Téllez-Vázquez, N.; et al. Association of diabetes and tuberculosis: Impact on treatment and post-treatment outcomes. Thorax 2013, 68, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Restrepo, B.I. Diabetes and Tuberculosis. Microbiol. Spectr. 2016, 4, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.H.; Yu, C.T.; Lin, H.C.; Liu, C.Y.; Kuo, H.P. Hypodense alveolar macrophages in patients with diabetes mellitus and active pulmonary tuberculosis. Tuber. Lung Dis. 1999, 79, 235–242. [Google Scholar] [CrossRef] [PubMed]
- van Exel, E.; Gussekloo, J.; de Craen, A.J.; Frolich, M.; Bootsma-Van Der Wiel, A.; Westendorp, R.G. Low production capacity of interleukin-10 associates with the metabolic syndrome and type 2 diabetes: The Leiden 85-Plus Study. Diabetes 2002, 51, 1088–1092. [Google Scholar] [CrossRef]
- Tsukaguchi, K.; Okamura, H.; Matsuzawa, K.; Tamura, M.; Miyazaki, R.; Tamaki, S.; Kimura, H. Longitudinal assessment of IFN-gamma production in patients with pulmonary tuberculosis complicated with diabetes mellitus. Kekkaku 2002, 77, 409–413. [Google Scholar]
- Tsukaguchi, K.; Yoneda, T.; Yoshikawa, M.; Tokuyama, T.; Fu, A.; Tomoda, K.; Narita, N.; Enoki, Y.; Tsukaguchi, M.; Shirai, F. Case study of interleukin-1 beta, tumor necrosis factor alpha and interleukin-6 production peripheral blood monocytes in patients with diabetes mellitus complicated by pulmonary tuberculosis. Kekkaku 1992, 67, 755–760. [Google Scholar]
- Restrepo, B.I.; Fisher-Hoch, S.P.; Pino, P.A.; Salinas, A.; Rahbar, M.H.; Mora, F.; Cortes-Penfield, N.; McCormick, J.B. Tuberculosis in poorly controlled type 2 diabetes: Altered cytokine expression in peripheral white blood cells. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2008, 47, 634–641. [Google Scholar] [CrossRef]
- Ronacher, K.; van Crevel, R.; Critchley, J.A.; Bremer, A.A.; Schlesinger, L.S.; Kapur, A.; Basaraba, R.; Kornfeld, H.; Restrepo, B.I. Defining a Research Agenda to Address the Converging Epidemics of Tuberculosis and Diabetes: Part 2: Underlying Biologic Mechanisms. Chest 2017, 152, 174–180. [Google Scholar] [CrossRef]
- World Health Organization. Global Tuberculosis Report 2022. Available online: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2022 (accessed on 29 May 2023).
- Meza, R.; Barrientos-Gutierrez, T.; Rojas-Martinez, R.; Reynoso-Noverón, N.; Palacio-Mejia, L.S.; Lazcano-Ponce, E.; Hernández-Ávila, M. Burden of type 2 diabetes in Mexico: Past, current and future prevalence and incidence rates. Prev. Med. 2015, 81, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Shamah-Levy, T.; Vielma-Orozco, E.; Heredia-Hernández, O.; Romero-Martínez, M.; Mojica-Cuevas, J.; Cuevas-Nasu, L.; Santaella-Castell, J.A.; Rivera-Dommarco, J. Encuesta Nacional de Salud y Nutrición 2018–19: Resultados Nacionales; Instituto Nacional de Salud Pública: Cuernavaca, México, 2020; Available online: https://ensanut.insp.mx/encuestas/ensanut2018/informes.php (accessed on 29 May 2023).
- Delgado-Sánchez, G.; García-García, L.; Castellanos-Joya, M.; Cruz-Hervert, P.; Ferreyra-Reyes, L.; Ferreira-Guerrero, E.; Hernández, A.; Ortega-Baeza, V.M.; Montero-Campos, R.; Sulca, J.A.; et al. Association of Pulmonary Tuberculosis and Diabetes in Mexico: Analysis of the National Tuberculosis Registry 2000–2012. PLoS ONE 2015, 10, e0129312. [Google Scholar] [CrossRef]
- Sterling, T.R.; Njie, G.; Zenner, D.; Cohn, D.L.; Reves, R.; Ahmed, A.; Menzies, D.; Horsburgh, C.R.; Crane, C.M.; Burgos, M.; et al. Guidelines for the Treatment of Latent Tuberculosis Infection: Recommendations from the National Tuberculosis Controllers Association and CDC, 2020. MMWR Recomm. Rep. 2020, 69, 1–11. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guidelines on the Management of Latent Tuberculosis Infection. WHO/HTM/TB. 2015. Available online: http://apps.who.int/iris/bitstream/10665/136471/1/9789241548908_eng.pdf?ua=1&ua=1 (accessed on 2 March 2021).
- World Health Organization. Collaborative Framework for Care and Control of Tuberculosis and Diabetes. 2011. Available online: http://www.ncbi.nlm.nih.gov/pubmed/17158327 (accessed on 2 March 2021).
- World Health Organization. The END TB Strategy. In Global Strategy and Targets for Tuberculosis Prevention, Care and Control after 2015; WHO: Geneva, Switzerland, 2016; Available online: https://www.who.int/tb/strategy/End_TB_Strategy.pdf?ua=1 (accessed on 2 March 2021).
- Dye, C.; Glaziou, P.; Floyd, K.; Raviglione, M. Prospects for tuberculosis elimination. Annu. Rev. Public Health 2013, 34, 271–286. [Google Scholar] [CrossRef] [PubMed]
- Feldman, E.L.; Stevens, M.J.; Thomas, P.K.; Brown, M.B.; Canal, N.; Greene, D.A. A practical two-step quantitative clinical and electrophysiological assessment for the diagnosis and staging of diabetic neuropathy. Diabetes Care 1994, 17, 1281–1289. [Google Scholar] [CrossRef]
- National Commission of Sanitary Risks. [Comisión Federal de Riesgos Sanitarios]. Guidelines for Pharmacovigilance in Clinical Research. Available online: https://www.gob.mx/cofepris/documentos/guias-lineamientos-y-requerimientos-de-farmacovigilancia (accessed on 15 February 2021).
- National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE), v4.0. 2009. Available online: https://www.eortc.be/services/doc/ctc/CTCAE_4.03_2010-06-14_QuickReference_5x7.pdf (accessed on 15 February 2020).
- Saukkonen, J.J.; Cohn, D.L.; Jasmer, R.M.; Schenker, S.; Jereb, J.A.; Nolan, C.M.; Peloquin, C.A.; Gordin, F.M.; Nunes, D.; Strader, D.B.; et al. An official ATS statement: Hepatotoxicity of antituberculosis therapy. Am. J. Respir. Crit. Care Med. 2006, 174, 935–952. [Google Scholar] [CrossRef]
- Glasheen, W.P.; Renda, A.; Dong, Y. Diabetes Complications Severity Index (DCSI)-Update and ICD-10 translation. J. Diabetes Complicat. 2017, 31, 1007–1013. [Google Scholar] [CrossRef]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.-C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef]
- Deyo, R.; Cherkin, D.; Ciol, M. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J. Clin. Epidemiol. 1992, 45, 613–619. [Google Scholar] [CrossRef]
- Gordin, F.; Chaisson, R.E.; Matts, J.P.; Miller, C.; Garcia, M.d.L.; Hafner, R.; Valdespino, J.L.; Coberly, J.; Schechter, M.; Klukowicz, A.J.; et al. Rifampin and pyrazinamide vs isoniazid for prevention of tuberculosis in HIV-infected persons: An international randomized trial. JAMA 2000, 283, 1445–1450. [Google Scholar] [CrossRef]
- Lesnichii, A.V.; Karpina, L.Z. Tuberculosis chemoprophylaxis for diabetics: Are the benefits of isoniazid worth the risk. Probl. Tuberk 1969, 47, 1–3. [Google Scholar]
- Smith, B.M.; Schwartzman, K.; Bartlett, G.; Menzies, D. Adverse events associated with treatment of latent tuberculosis in the general population. CMAJ 2011, 183, E173–E179. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.-L.; Huang, W.-C.; Lin, K.-D.; Liu, S.-S.; Lee, M.-R.; Cheng, M.-H.; Chin, C.-S.; Lu, P.-L.; Sheu, C.-C.; Wang, J.-Y.; et al. Completion Rate and Safety of Programmatic Screening and Treatment for Latent Tuberculosis Infection in Elderly Patients with Poorly Controlled Diabetic Mellitus: A Prospective Multicenter Study. Clin. Infect. Dis. 2021, 73, e1252–e1260. [Google Scholar] [CrossRef]
- Pease, C.; Hutton, B.; Yazdi, F.; Wolfe, D.; Hamel, C.; Barbeau, P.; Skidmore, B.; Alvarez, G.G. A systematic review of adverse events of rifapentine and isoniazid compared to other treatments for latent tuberculosis infection. Pharmacoepidemiol. Drug Saf. 2018, 27, 557–566. [Google Scholar] [CrossRef]
- Ostrosky-Zeichner, L.; Rangel-Frausto, M.S.; García-Romero, E.; Vázquez, A.; Ibarra, M.J.; Ponce de León-Rosales, S. Tuberculosis in health personnel: Importance of surveillance and control programs. Salud Publica Mex. 2000, 42, 48–52. [Google Scholar] [PubMed]
- Bourlon, C.; Camacho-Hernández, R.; Fierro-Angulo, O.M.; Acosta-Medina, A.A.; Bourlon, M.T.; Niembro-Ortega, M.D.; Gonzalez-Lara, M.F.; Sifuentes-Osornio, J.; Ponce-De-León, A. Latent Tuberculosis in Hematopoietic Stem Cell Transplantation: Diagnostic and Therapeutic Strategies to Prevent Disease Activation in an Endemic Population. Biol. Blood Marrow Transplant. 2020, 26, 1350–1354. [Google Scholar] [CrossRef] [PubMed]
- Daintith, H.; Stevenson, I.H.; O’Malley, K. Influence of diabetes mellitus on drug metabolism in man. Int. J. Clin. Pharmacol. Biopharm. 1976, 13, 55–58. [Google Scholar]
- Ruslami, R.; Nijland, H.M.J.; Adhiarta, I.G.N.; Kariadi, S.H.K.S.; Alisjahbana, B.; Aarnoutse, R.E.; van Crevel, R. Pharmacokinetics of antituberculosis drugs in pulmonary tuberculosis patients with type 2 diabetes. Antimicrob. Agents Chemother. 2010, 54, 1068–1074. [Google Scholar] [CrossRef]
- Yang, Y.; Liu, X. Imbalance of Drug Transporter-CYP450s Interplay by Diabetes and Its Clinical Significance. Pharmaceutics 2020, 12, 348. [Google Scholar] [CrossRef]
- Niazi, A.K.; Kalra, S. Diabetes and tuberculosis: A review of the role of optimal glycemic control. J. Diabetes Metab. Disord. 2012, 11, 28. [Google Scholar] [CrossRef]
- Ena, J.; Valls, V. Short-course therapy with rifampin plus isoniazid, compared with standard therapy with isoniazid, for latent tuberculosis infection: A meta-analysis. Clin. Infect. Dis. 2005, 40, 670–676. [Google Scholar] [CrossRef] [PubMed]
- LoBue, P.A.; Moser, K.S. Use of isoniazid for latent tuberculosis infection in a public health clinic. Am. J. Respir. Crit. Care Med. 2003, 168, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Menzies, D.; Long, R.; Trajman, A.; Dion, M.J.; Yang, J.; Al Jahdali, H.; Memish, Z.; Khan, K.; Gardam, M.; Hoeppner, V.; et al. Adverse events with 4 months of rifampin therapy or 9 months of isoniazid therapy for latent tuberculosis infection: A randomized trial. Ann. Intern. Med. 2008, 149, 689–697. [Google Scholar] [CrossRef] [PubMed]
- Menzies, D.; Adjobimey, M.; Ruslami, R.; Trajman, A.; Sow, O.; Kim, H.; Baah, J.O.; Marks, G.B.; Long, R.; Hoeppner, V.; et al. Four Months of Rifampin or Nine Months of Isoniazid for Latent Tuberculosis in Adults. N. Engl. J. Med. 2018, 379, 440–453. [Google Scholar] [CrossRef] [PubMed]
- Shamah, T.; Cuevas, L.; Rivera, J.; Hernández, M. Encuesta Nacional de Salud y Nutrición 2016; Instituto Nacional de Salud Pública: Cuernavaca, Mexico, 2016. [Google Scholar]
- Rojas-Martinez, R.; Basto-Abreu, A.; Aguilar-Salinas, C.A.; Zarate-Rojas, E.; Villalpando, S.; Barrientos-Gutierrez, T. Prevalence of Previously Diagnosed Diabetes Mellitus in Mexico. Salud Publica Mex. 2018, 60, 224–232. [Google Scholar] [PubMed]
- Fitzgerald, D.; Sterling, T.; Haas, D. Mycobacterium tuberculosis. In Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, 9th ed.; Mandell, J., Dolin, R., Blaser, M., Eds.; Elsevier, Inc: Philadelphia, PA, USA, 2020; pp. 2985–3021. [Google Scholar]
- Magro, L.; Moretti, U.; Leone, R. Epidemiology and characteristics of adverse drug reactions caused by drug-drug interactions. Expert Opin. Drug Saf. 2012, 11, 83–94. [Google Scholar] [CrossRef]
- Grosset, J.; Leventis, S. Adverse effects of rifampin. Rev. Infect. Dis. 1983, 5 (Suppl. S3), S440–S450. [Google Scholar] [CrossRef]
- Abulfathi, A.A.; Decloedt, E.H.; Svensson, E.M.; Diacon, A.H.; Donald, P.; Reuter, H. Clinical Pharmacokinetics and Pharmacodynamics of Rifampicin in Human Tuberculosis. Clin. Pharmacokinet. 2019, 58, 1103–1129. [Google Scholar] [CrossRef]
- Zawada, A.E.; Moszak, M.; Skrzypczak, D.; Grzymisławski, M. Gastrointestinal complications in patients with diabetes mellitus. Adv. Clin. Exp. Med. 2018, 27, 567–572. [Google Scholar] [CrossRef]
- Soldevila-Boixader, L.; Murillo, O.; Waibel, F.W.A.; Huber, T.; Schöni, M.; Lalji, R.; Uçkay, I. The Epidemiology of Antibiotic-Related Adverse Events in the Treatment of Diabetic Foot Infections: A Narrative Review of the Literature. Antibiotics 2023, 12, 774. [Google Scholar] [CrossRef]
- Basto-Abreu, A.; Barrientos-Gutierrez, T.; Rojas-Martinez, R.; Aguilar-Salinas, C.A.; Lopez-Olmedo, N.; De la Cruz-Gongora, V.; Rivera-Dommarco, J.; Shamah-Levy, T.; Romero-Martínez, M.; Barquera, S.; et al. Prevalence of diabetes and poor glycemic control in Mexico: Results from Ensanut 2016. Salud Publica Mex. 2020, 62, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Borgharkar, S.S.; Das, S.S. Real-world evidence of glycemic control among patients with type 2 diabetes mellitus in India: The TIGHT study. BMJ Open Diabetes Res. Care 2019, 7, e000654. [Google Scholar] [CrossRef] [PubMed]
- Ayele, B.H.; Roba, H.S.; Beyene, A.S.; Mengesha, M.M. Prevalent, uncontrolled, and undiagnosed diabetes mellitus among urban adults in Dire Dawa, Eastern Ethiopia: A population-based cross-sectional study. SAGE Open Med. 2020, 8, 2050312120975235. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Total N = 130 (%) | Isoniazid n = 68 (%) | Rifampicin n = 62 (%) | p Value * |
|---|---|---|---|---|
| Age (Median, IQR) | 57 (50–62) | 57 (52–62) | 57 (48–62) | 0.464 |
| Men | 54 (41.2) | 24 (35.2) | 30 (47.0) | 0.152 ** |
| BMI (kg/m2) | 28.1 (25.6–31.6) | 27.7 (25.6–31.2) | 28.7 (25.6–31.7) | 0.622 |
| Time since DM diagnosis (years) | 11 (4–19) | 13 (5–23) | 10 (3.5–15.5) | 0.045 |
| Alcohol drinking | 58 (44.2) | 29 (42.6) | 29 (45.2) | 0.697 ** |
| Cigarette smoking | 60 (46.5) | 29 (42.6) | 31 (50.0) | 0.350 ** |
| Oral glucose-lowering drugs | 128 (98.4) | 68 (100) | 60 (96.8) | 0.139 ** |
| Insulin | 73 (55.7) | 42 (61.8) | 31 (49.2) | 0.148 ** |
| Years of insulin use | 7 (4–12) | 8 (4–14) | 6.5 (4–11) | 0.673 |
| Number of drugs taken | 6 (4–7) | 6 (5–8) | 5 (4–7) | 0.171 |
| Chronic kidney disease | 28 (22.1) | 15 (22) | 13 (21.0) | 0.982 |
| Time since diagnosis (years) | 7 (6–7) | 7 (7–8.5) | 4 (2–6) | 0.049 |
| Retinopathy | 24 (19) | 19 (27.9) | 5 (8.0) | 0.007 |
| Time since diagnosis of retinopathy (years) | 3 (2–9) | 3.5 (2–9) | 2.5 (1–6) | 0.349 |
| Foot ulcer or amputation | 5 (4.5) | 4 (5.8) | 1 (1.6) | 0.459 |
| Ischemic heart disease | 4 (3.8) | 3 (4.4) | 1 (1.6) | 0.712 |
| Neuropathy | 25 (19.8) | 14 (20.5) | 11 (17.7) | 0.825 |
| Diabetes Complications Severity Index | 1 (1–2) | 1 (1–3) | 1 (0–2) | 0.064 |
| Comorbidities | ||||
| Hypertension | 66 (51.9) | 39 (57.3) | 27 (45.9) | 0.194 |
| Time since diagnosis of hypertension | 10.5 (4.5–18) | 11 (6–18) | 10 (4–18) | 0.557 |
| Obesity | 39 (29.7) | 18 (26.4) | 21 (33.3) | 0.391 |
| Time since diagnosis of obesity | 15 (10–28) | 18 (12–28) | 13 (7–28.5) | 0.464 |
| Dyslipidemia | 85 (64.8) | 42 (61.7) | 43 (68.2) | 0.437 |
| Depressive symptoms | 34 (25.9) | 17 (25) | 17 (26.9) | 0.796 |
| Gastrointestinal symptoms | 6 (4.5) | 3 (4.4) | 3 (4.7) | 0.924 |
| Osteoarthritis | 13 (9.9) | 8 (11.7) | 5 (7.9) | 0.464 |
| Cataratacts | 20 (15.2) | 14 (20.5) | 6 (9.5) | 0.079 |
| Glaucoma | 6 (4.5) | 5 (7.3) | 1 (1.5) | 0.115 |
| Charlson Index score | 3 (2–4) | 3 (2–4) | 3 (2–4) | 0.545 |
| Baseline Laboratory parameters | ||||
| Alanine aminotransferase (U/L) median (IQR) | 18.9 (14.2–23.6) | 19 (14–26.9) | 18.6 (14.7–21.9) | 0.778 |
| Aspartate aminotransferase (U/L) median (IQR) | 18 (15–22) | 19 (15.5–23.5) | 18 (15–21) | 0.538 |
| Total bilirubin (mg/dL) median (IQR) | 0.53 (0.43–0.63) | 0.53 (0.43–0.62) | 0.53 (0.43–0.64) | 0.661 |
| Glycated hemoglobin (median, IQR) | 8.2 (6.6–10) | 8.2 (6.8–9.7) | 8 (6.4–10.2) | 0.933 |
| Concomitant Drug | Total N = 130 (%) | Isoniazid n = 68 (%) | Rifampicin n = 62 (%) | p Value ** |
|---|---|---|---|---|
| Metformin | 123 (93.9) | 64 (94.1) | 59 (93.6) | 0.911 |
| Sulfonylureas | 17 (13) | 7 (10.3) | 10 (15.9) | 0.342 |
| Sitagliptin | 13 (9.9) | 8 (11.7) | 5 (7.9) | 0.464 |
| SLGT2 inhibitors * | 15 (11.5) | 9 (13.2) | 6 (9.5) | 0.505 |
| Statins | 98 (74.8) | 53 (77.9) | 45 (71.4) | 0.391 |
| Fibrates | 48 (36.6) | 21 (30.9) | 27 (42.9) | 0.155 |
| Antidepressants | 20 (15.3) | 10 (14.7) | 10 (15.9) | 0.853 |
| Antihypertensive agents | 81 (61.8) | 44 (64.7) | 37 (58.7) | 0.482 |
| Aspirin | 70 (53.4) | 36 (52.9) | 34 (54) | 0.906 |
| Other | 76 (58) | 40 (58.8) | 36 (57.1) | 0.846 |
| Outcome | Total N = 130 | Isoniazid n = 68 | Rifampicin n = 62 | Relative Risk (95% CI) * |
|---|---|---|---|---|
| Primary outcome | ||||
| Recurrent grade 2 hepatotoxicity or grade 3–4 adverse events | 18 (13.84) | 9 (13.23) | 9 (14.51) | 1.09 (0.47 to 2.59) |
| Secondary Outcomes | ||||
| Recurrent grade 2 hepatotoxicity | 1 (0.76) | 1 (1.47) | 0 | ----- |
| Grade 3–4 hepatotoxicity | 6 (4.61) | 6 (8.82) | 0 | ----- |
| Grade 3–4 gastrointestinal intolerance | 11 (8.46) | 2 (2.94) | 9 (14.51) | 4.93 (1.11 to 21.96) |
| Characteristics | Adverse Events III-IV Related to Therapy Hazard Ratio | 95% Confidence Interval | p Value |
|---|---|---|---|
| Chronic kidney disease | 6.44 | 1.56–26.58 | 0.010 |
| Female | 4.53 | 1.25–16.39 | 0.021 |
| Alcohol usage | 2.02 | 0.70–5.84 | 0.196 |
| Age | 1.03 | 0.97–1.09 | 0.359 |
| Isoniazid arm | 0.62 | 0.24–1.57 | 0.311 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tamez-Torres, K.M.; Mongua-Rodríguez, N.; Ferreyra-Reyes, L.; Torres-Gonzalez, P.; Delgado-Sánchez, G.; Martínez-Hernández, M.; Bobadilla-del-Valle, M.; Jasso-Sosa, V.Y.; López-Castillo, P.d.S.; Ferreira-Guerrero, E.; et al. Safety and Tolerability of Six Months of Isoniazid Plus Pyridoxine or Three Months of Rifampicin for Tuberculosis among Subjects with Diabetes Mellitus: A Randomized Trial. Microorganisms 2023, 11, 1917. https://doi.org/10.3390/microorganisms11081917
Tamez-Torres KM, Mongua-Rodríguez N, Ferreyra-Reyes L, Torres-Gonzalez P, Delgado-Sánchez G, Martínez-Hernández M, Bobadilla-del-Valle M, Jasso-Sosa VY, López-Castillo PdS, Ferreira-Guerrero E, et al. Safety and Tolerability of Six Months of Isoniazid Plus Pyridoxine or Three Months of Rifampicin for Tuberculosis among Subjects with Diabetes Mellitus: A Randomized Trial. Microorganisms. 2023; 11(8):1917. https://doi.org/10.3390/microorganisms11081917
Chicago/Turabian StyleTamez-Torres, Karla M., Norma Mongua-Rodríguez, Leticia Ferreyra-Reyes, Pedro Torres-Gonzalez, Guadalupe Delgado-Sánchez, Maribel Martínez-Hernández, Miriam Bobadilla-del-Valle, Velma Y. Jasso-Sosa, Priscila del S. López-Castillo, Elizabeth Ferreira-Guerrero, and et al. 2023. "Safety and Tolerability of Six Months of Isoniazid Plus Pyridoxine or Three Months of Rifampicin for Tuberculosis among Subjects with Diabetes Mellitus: A Randomized Trial" Microorganisms 11, no. 8: 1917. https://doi.org/10.3390/microorganisms11081917
APA StyleTamez-Torres, K. M., Mongua-Rodríguez, N., Ferreyra-Reyes, L., Torres-Gonzalez, P., Delgado-Sánchez, G., Martínez-Hernández, M., Bobadilla-del-Valle, M., Jasso-Sosa, V. Y., López-Castillo, P. d. S., Ferreira-Guerrero, E., Cruz-Hervert, L. P., Sifuentes-Osornio, J., Aguilar-Salinas, C. A., García-García, L., & Ponce-de-Leon, A. (2023). Safety and Tolerability of Six Months of Isoniazid Plus Pyridoxine or Three Months of Rifampicin for Tuberculosis among Subjects with Diabetes Mellitus: A Randomized Trial. Microorganisms, 11(8), 1917. https://doi.org/10.3390/microorganisms11081917