
The Angiopoietin Signaling Pathway Is Involved in Inflammatory Processes in Hospitalized COVID-19 Patients

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Samples
2.2. Characteristics of Patients
2.3. Assays: Ang1, Ang2, and IL-6
2.4. ELISA IgG Titer
2.5. Statistical Analysis
2.6. Study Approval
3. Results
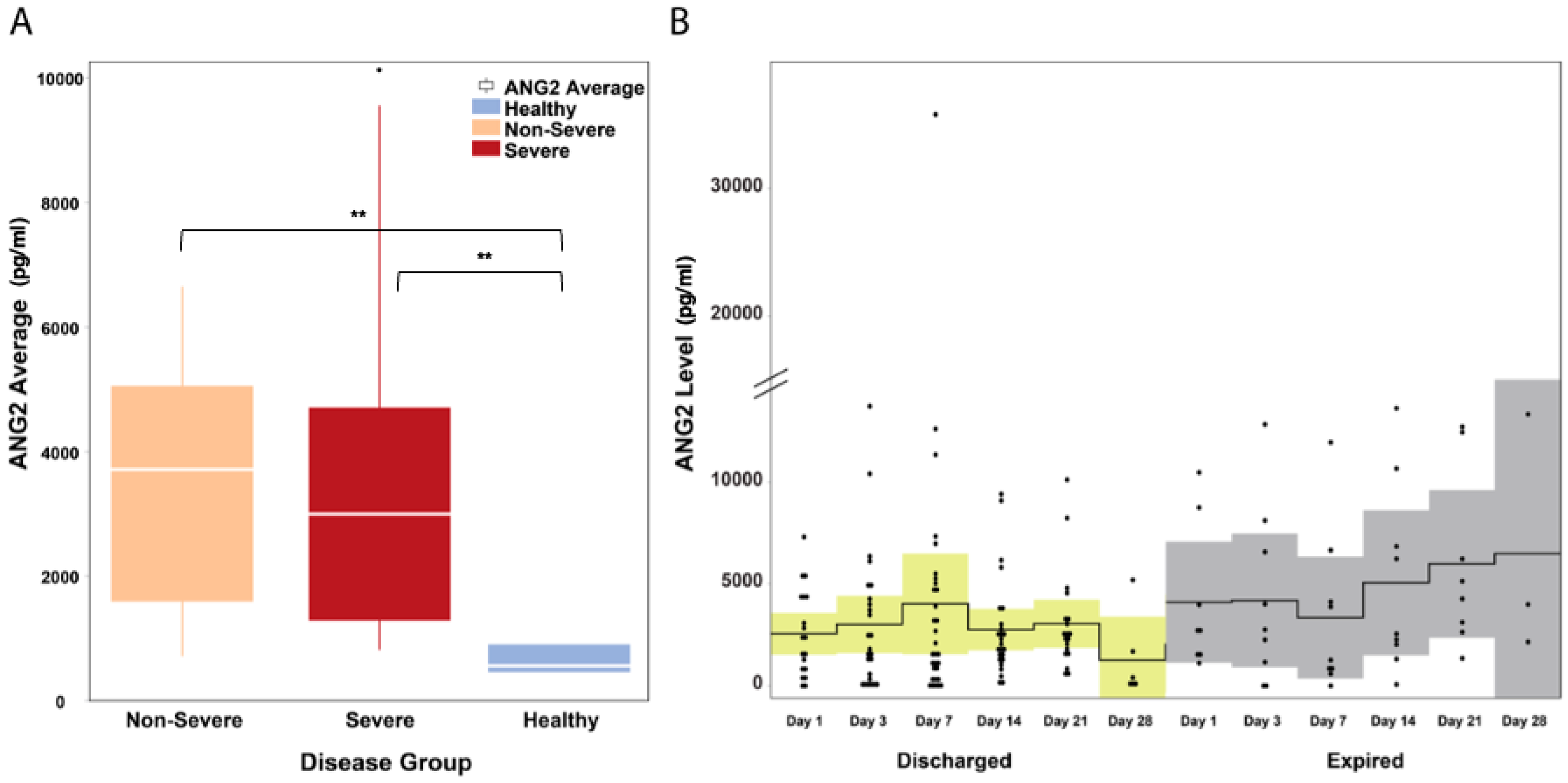
3.1. Ang2 Serum Levels Are Significantly Elevated in COVID-19 Patients
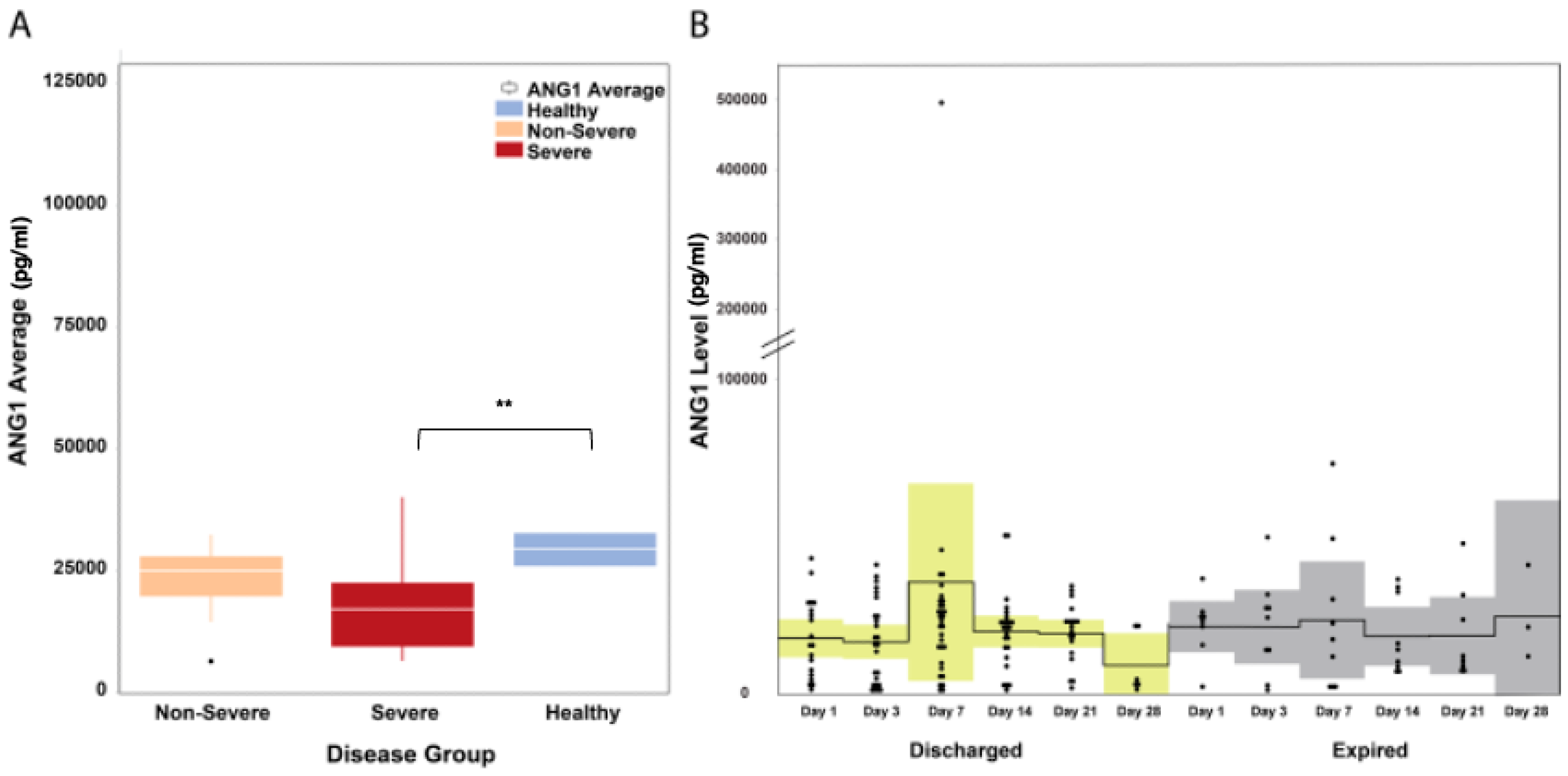
3.2. Ang1 Serum Levels Are Decreased in COVID-19 Patients
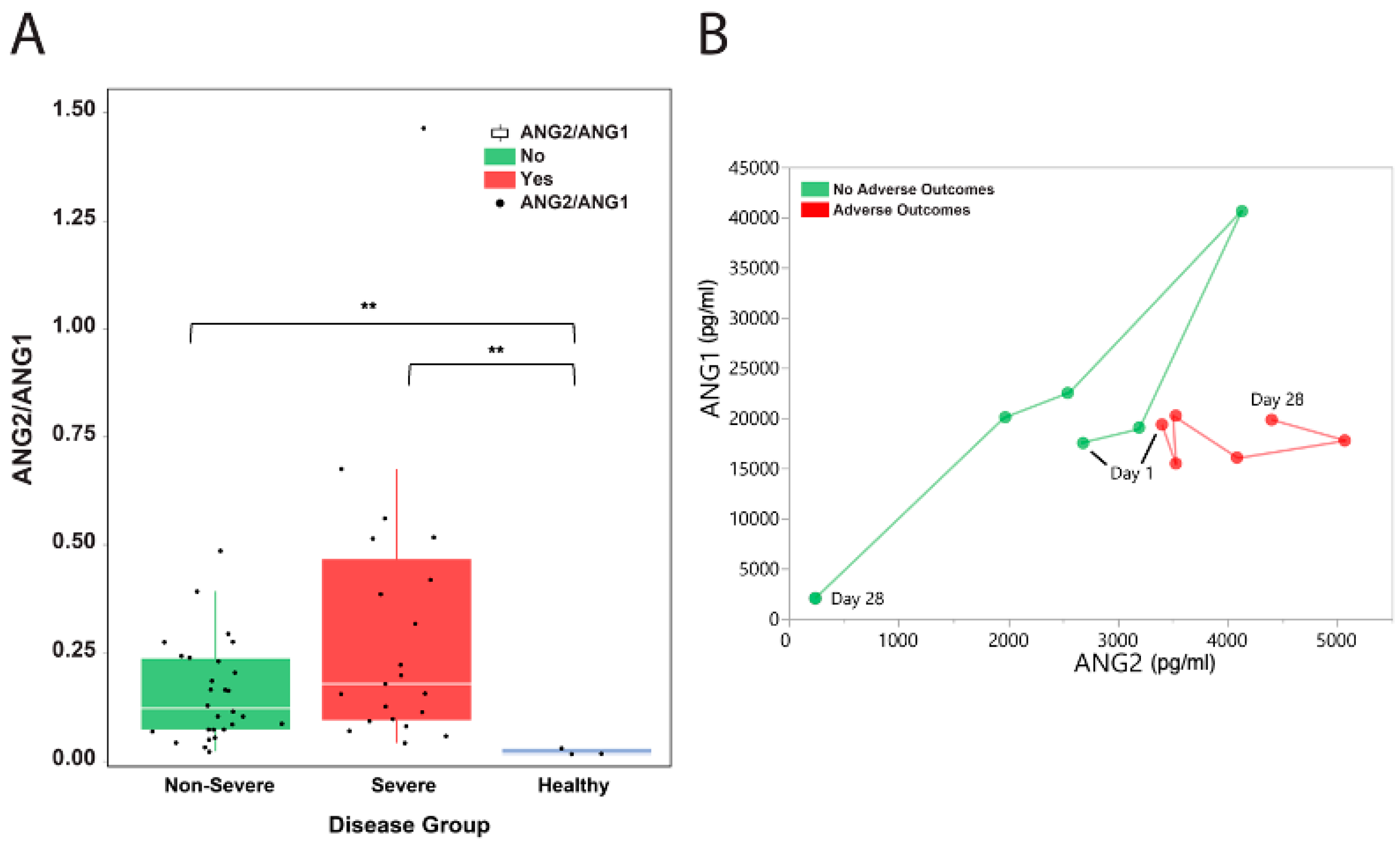
3.3. The Dynamic Levels of Ang1 and Ang2 during the Clinical Course May Predict Adverse Outcomes in COVID-19 Patients
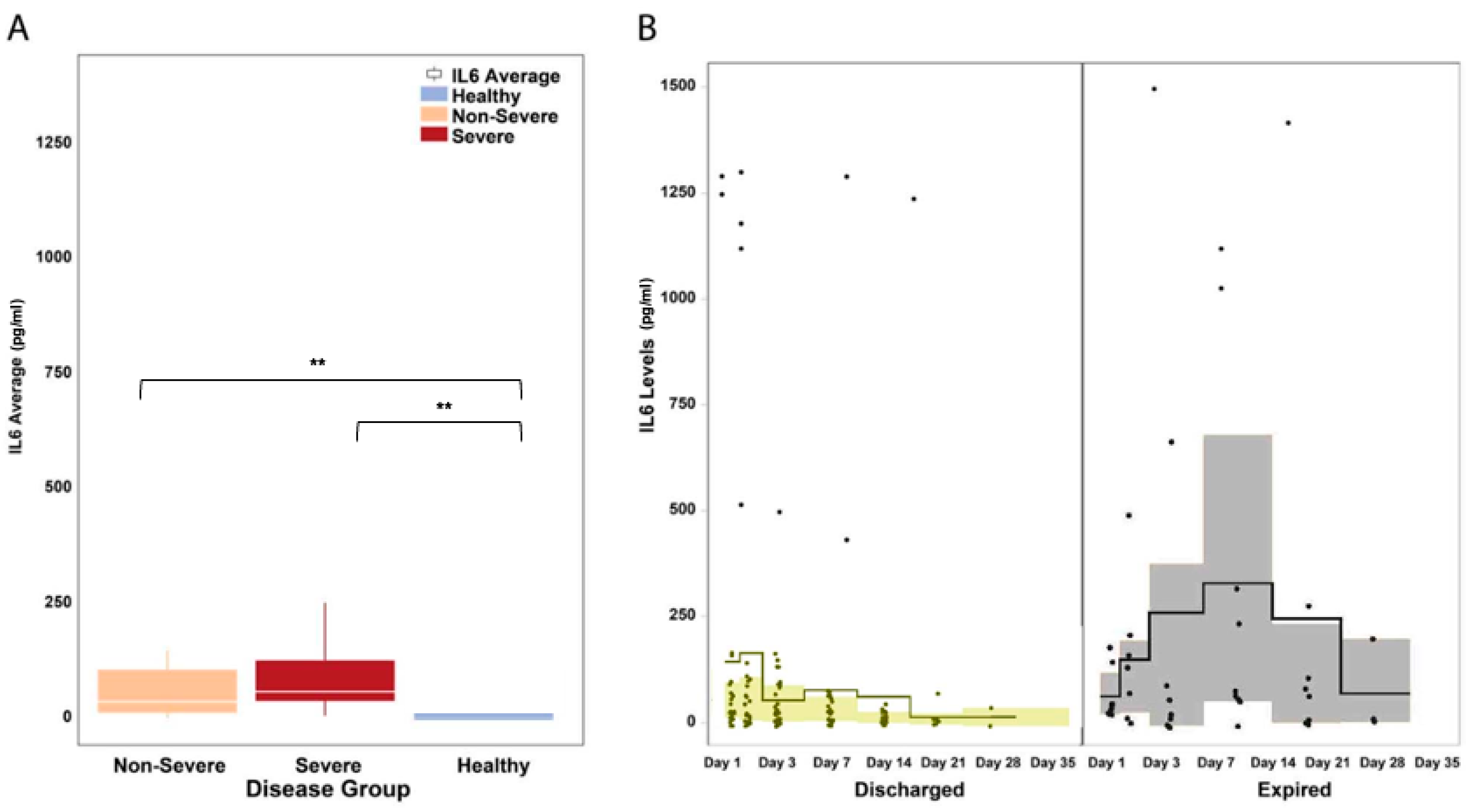
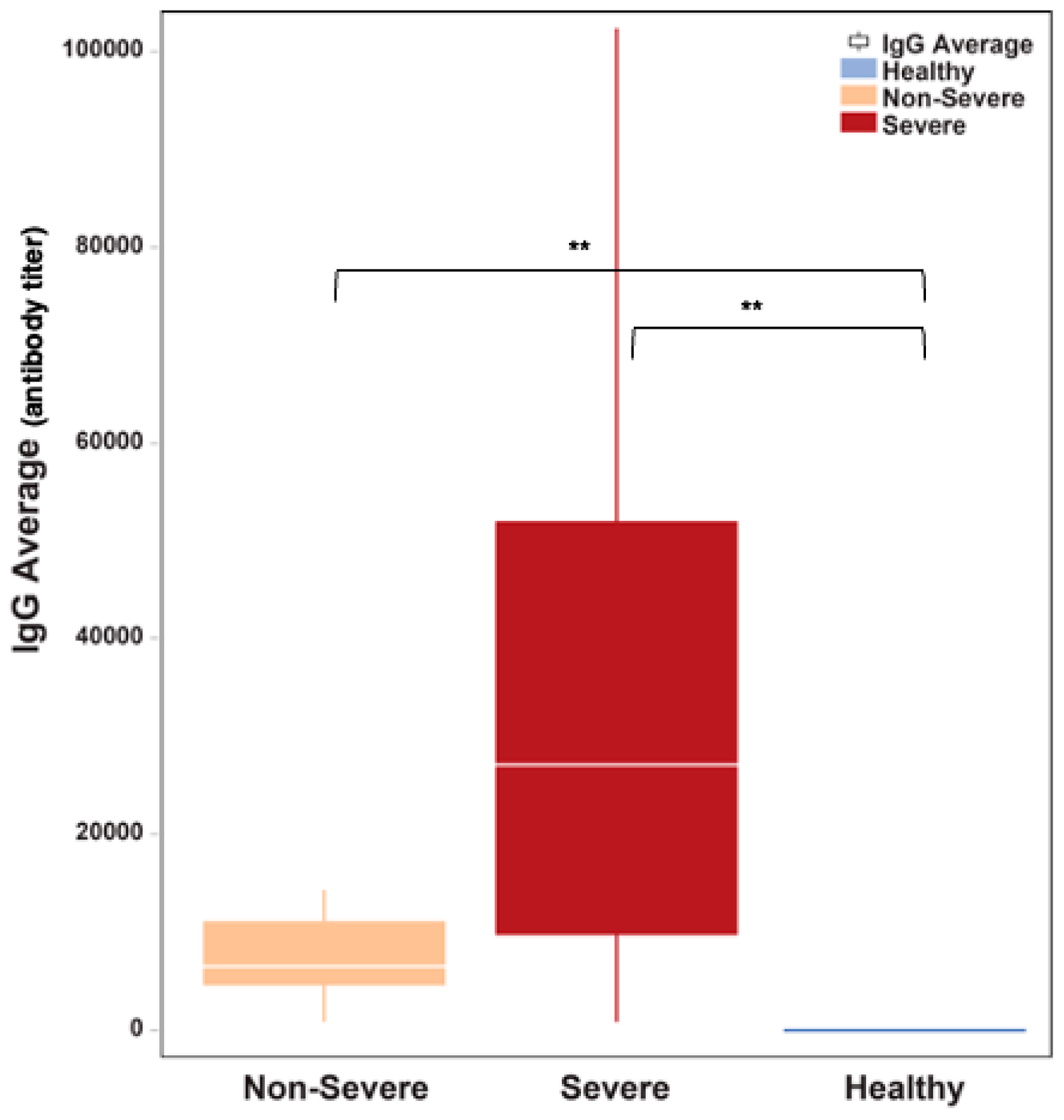
3.4. IL-6 Serum Levels and Anti-SARS-CoV2 IgG Titers Are Significantly Elevated in COVID-19 Patients
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thomas, M.; Augustin, H.G. The role of the Angiopoietins in vascular morphogenesis. Angiogenesis 2009, 12, 125–137. [Google Scholar] [CrossRef]
- Gopinathan, G.; Milagre, C.; Pearce, O.M.; Reynolds, L.E.; Hodivala-Dilke, K.; Leinster, D.A.; Zhong, H.; Hollingsworth, R.E.; Thompson, R.; Whiteford, J.R.; et al. Interleukin-6 Stimulates Defective Angiogenesis. Cancer Res. 2015, 75, 3098–3107. [Google Scholar] [CrossRef]
- Barton, W.A.; Dalton, A.C.; Seegar, T.C.M.; Himanen, J.P.; Nikolov, D.B. Tie2 and Eph receptor tyrosine kinase activation and signaling. Cold Spring Harb. Perspect. Biol. 2014, 6, a009142. [Google Scholar] [CrossRef]
- Yu, X.; Ye, F. Role of Angiopoietins in Development of Cancer and Neoplasia Associated with Viral Infection. Cells 2020, 9, 457. [Google Scholar] [CrossRef] [PubMed]
- Jeansson, M.; Gawlik, A.; Anderson, G.; Li, C.; Kerjaschki, D.; Henkelman, M.; Quaggin, S.E. Angiopoietin-1 is essential in mouse vasculature during development and in response to injury. J. Clin. Investig. 2011, 121, 2278–2289. [Google Scholar] [CrossRef]
- Thurston, G.; Rudge, J.S.; Ioffe, E.; Papadopoulos, N.; Daly, C.; Vuthoori, S.; Daly, T.; Wiegand, S.J.; Yancopoulos, G.D. The anti-inflammatory actions of angiopoietin-1. In Mechanisms of Angiogenesis; Springer: Berlin/Heidelberg, Germany, 2005; pp. 233–245. [Google Scholar]
- Thurston, G.; Wang, Q.; Baffert, F.; Rudge, J.; Papadopoulos, N.; Jean-Guillaume, D.; Wiegand, S.; Yancopoulos, G.D.; McDonald, D.M. Angiopoietin 1 causes vessel enlargement, without angiogenic sprouting, during a critical developmental period. Development 2005, 132, 3317–3326. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Xu, W.D.; Huang, A.F. Role of angiopoietin-2 in inflammatory autoimmune diseases: A comprehensive review. Int. Immunopharmacol. 2020, 80, 106223. [Google Scholar] [CrossRef]
- Scholz, A.; Plate, K.H.; Reiss, Y. Angiopoietin-2: A multifaceted cytokine that functions in both angiogenesis and inflammation. Ann. N. Y. Acad. Sci. 2015, 1347, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Mandriota, S.J.; Pepper, M.S. Regulation of angiopoietin-2 mRNA levels in bovine microvascular endothelial cells by cytokines and hypoxia. Circ. Res. 1998, 83, 852–859. [Google Scholar] [CrossRef]
- Akwii, R.G.; Sajib, M.S.; Zahra, F.T.; Mikelis, C.M. Role of Angiopoietin-2 in Vascular Physiology and Pathophysiology. Cells 2019, 8, 471. [Google Scholar] [CrossRef]
- Trent, B.; Liang, Y.; Xing, Y.; Esqueda, M.; Wei, Y.; Cho, N.H.; Kim, H.I.; Kim, Y.S.; Shelite, T.R.; Cai, J.; et al. Polarized lung inflammation and Tie2/angiopoietin-mediated endothelial dysfunction during severe Orientia tsutsugamushi infection. PLoS Negl. Trop. Dis. 2020, 14, e0007675. [Google Scholar] [CrossRef] [PubMed]
- Becker, R.C. COVID-19-associated vasculitis and vasculopathy. J. Thromb. Thrombolysis 2020, 50, 499–511. [Google Scholar] [CrossRef] [PubMed]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wu, H.; Khardori, R.; Song, Y.H.; Lu, Y.W.; Geng, Y.J. Insulin-like growth factor-1 receptor activation prevents high glucose-induced mitochondrial dysfunction, cytochrome-c release and apoptosis. Biochem. Biophys. Res. Commun. 2009, 384, 259–264. [Google Scholar] [CrossRef]
- Smadja, D.M.; Guerin, C.L.; Chocron, R.; Yatim, N.; Boussier, J.; Gendron, N.; Khider, L.; Hadjadj, J.; Goudot, G.; Debuc, B.; et al. Angiopoietin-2 as a marker of endothelial activation is a good predictor factor for intensive care unit admission of COVID-19 patients. Angiogenesis 2020, 23, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Mendoza, R.; Saha, N.; Momeni, A.; Gabutan, E.; Alawad, M.; Dehghani, A.; Diks, J.; Lin, B.; Wang, D.; Alshal, M.; et al. Ephrin-A1 and the sheddase ADAM12 are upregulated in COVID-19. Heliyon 2021, 7, e07200. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.S.; Yeo, T.W.; Piera, K.A.; Woodberry, T.; Celermajer, D.S.; Stephens, D.P.; Anstey, N.M. Angiopoietin-2 is increased in sepsis and inversely associated with nitric oxide-dependent microvascular reactivity. Crit. Care 2010, 14, R89. [Google Scholar] [CrossRef]
- Kim, I.; Oh, J.-L.; Ryu, Y.S.; So, J.-N.; Sessa, W.C.; Walsh, K.; Koh, G.Y. Angiopoietin-1 negatively regulates expression and activity of tissue factor in endothelial cells. FASEB J. 2002, 16, 126–128. [Google Scholar] [CrossRef]
- Kim, I.; Moon, S.-O.; Park, S.K.; Chae, S.W.; Koh, G.Y. Angiopoietin-1 reduces VEGF-stimulated leukocyte adhesion to endothelial cells by reducing ICAM-1, VCAM-1, and E-selectin expression. Circ. Res. 2001, 89, 477–479. [Google Scholar] [CrossRef]
- Liu, F.; Han, K.; Blair, R.; Kenst, K.; Qin, Z.; Upcin, B.; Wörsdörfer, P.; Midkiff, C.C.; Mudd, J.; Belyaeva, E.; et al. SARS-CoV-2 Infects Endothelial Cells In Vivo and In Vitro. Front. Cell. Infect. Microbiol. 2021, 11, 701278. [Google Scholar] [CrossRef] [PubMed]
- Iba, T.; Levy, J.H.; Levi, M.; Connors, J.M.; Thachil, J. Coagulopathy of Coronavirus Disease 2019. Crit. Care Med. 2020, 48, 1358–1364. [Google Scholar] [CrossRef] [PubMed]
- Ong, T.; McClintock, D.E.; Kallet, R.H.M.; Ware, L.B.; Matthay, M.A.; Liu, K.D.M. Ratio of angiopoietin-2 to angiopoietin-1 as a predictor of mortality in acute lung injury patients. Crit. Care Med. 2010, 38, 1845–1851. [Google Scholar] [CrossRef] [PubMed]
- Hachim, A.K.; Ali, A.S.; Arif, K.B. Effect of IL-6 and CRP titer with antibody level on severity of COVID-19 infection. Hum. Antibodies 2023, 31, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Gomes, S.M.R.; Brito, A.C.D.S.; Manfro, W.F.P.; Ribeiro-Alves, M.; Ribeiro, R.S.D.A.; da Cal, M.S.; Lisboa, V.D.C.; Abreu, D.P.B.D.; Castilho, L.D.R.; Porto, L.C.D.M.S.; et al. High levels of pro-inflammatory SARS-CoV-2-specific biomarkers revealed by in vitro whole blood cytokine release assay (CRA) in recovered and long-COVID-19 patients. PLoS ONE 2023, 18, e0283983. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.T.; Sudhir, U.; Punith, K.; Kumar, V.N.R.; Rao, M.Y.; Kumar, R. Cytokine profile in elderly patients with sepsis. Indian J. Crit. Care Med. 2009, 13, 74–78. [Google Scholar] [CrossRef]
- Madureira, G.; Soares, R. The misunderstood link between SARS-CoV-2 and angiogenesis. A narrative review. Pulmonology 2023, 29, 323–331. [Google Scholar] [CrossRef]
- Li, F.; Yin, R.; Guo, Q. Circulating angiopoietin-2 and the risk of mortality in patients with acute respiratory distress syndrome: A systematic review and meta-analysis of 10 prospective cohort studies. Ther. Adv. Respir. Dis. 2020, 14, 1753466620905274. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Category | All (n = 49) | Non-Severe (n = 29) | Severe (n = 20) |
|---|---|---|---|---|
| Age | Median (IQR), years | 63 (57–70) | 63 (55–71) | 63.5 (58.8–68.5) |
| Sex | Male | 25 (51.0) | 15 (51.7) | 10 (50.0) |
| Female | 24 (49.0) | 14 (48.3) | 10 (50.0) | |
| Race | Black | 36 (73.5) | 23 (79.3) | 13 (65.0) |
| Caucasian | 8 (16.3) | 5 (17.2) | 3 (15.0) | |
| Asian | 1 (2.0) | 0 (0.0) | 1 (5.0) | |
| Undisclosed | 4 (8.2) | 1 (3.4) | 3 (15.0) | |
| Co-morbid condition/s | Any condition | 48 (98.0) | 29 (100) | 19 (95.0) |
| HTN | 38 (77.6) | 25 (86.2) | 13 (65.0) | |
| DM | 32 (65.3) | 21 (72.4) | 11 (55.0) | |
| ESRD | 14 (28.6) | 12 (41.4) | 2 (10.0) | |
| Cardiac disease (i.e., heart failure, arrhythmia) | 14 (28.6) | 8 (27.6) | 6 (30.0) | |
| CNS disease (i.e., dementia, stroke) | 10 (20.4) | 6 (20.7) | 4 (20.0) | |
| Lung disease (i.e., COPD, ILD) | 6 (12.2) | 1 (3.4) | 5 (25.0) | |
| Cancer | 2 (4.1) | 2 (6.9) | 0 (0.0) | |
| Others | 19 (38.8) | 12 (41.4) | 7 (35.0) | |
| Clinical Outcome | Discharged | 37 (75.5) | 28 (96.6) | 9 (45.0) |
| Expired | 12 (24.5) | 1 (3.4) | 11 (55.0) | |
| Length of hospitalization | Median (IQR), days | 20 (9–28) | 11 (8–22) | 26 (19.3–31.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mendoza, R.P.; Momeni, A.; Saha, N.; Arshi, J.; Gabutan, E.C.; Alejandro, N.; Zuretti, A.; Premsrirut, P.K.; Nikolov, D.B. The Angiopoietin Signaling Pathway Is Involved in Inflammatory Processes in Hospitalized COVID-19 Patients. Microorganisms 2023, 11, 2940. https://doi.org/10.3390/microorganisms11122940
Mendoza RP, Momeni A, Saha N, Arshi J, Gabutan EC, Alejandro N, Zuretti A, Premsrirut PK, Nikolov DB. The Angiopoietin Signaling Pathway Is Involved in Inflammatory Processes in Hospitalized COVID-19 Patients. Microorganisms. 2023; 11(12):2940. https://doi.org/10.3390/microorganisms11122940
Chicago/Turabian StyleMendoza, Rachelle P., Amir Momeni, Nayanendu Saha, Juwairiya Arshi, Elmer C. Gabutan, Nichole Alejandro, Alejandro Zuretti, Prem K. Premsrirut, and Dimitar B. Nikolov. 2023. "The Angiopoietin Signaling Pathway Is Involved in Inflammatory Processes in Hospitalized COVID-19 Patients" Microorganisms 11, no. 12: 2940. https://doi.org/10.3390/microorganisms11122940
APA StyleMendoza, R. P., Momeni, A., Saha, N., Arshi, J., Gabutan, E. C., Alejandro, N., Zuretti, A., Premsrirut, P. K., & Nikolov, D. B. (2023). The Angiopoietin Signaling Pathway Is Involved in Inflammatory Processes in Hospitalized COVID-19 Patients. Microorganisms, 11(12), 2940. https://doi.org/10.3390/microorganisms11122940