1. Introduction
Infertility, defined as a disease by the WHO [
1], is an increasing problem worldwide. Infertility is estimated to affect between 8% and 12% of reproductive-aged couples; the 12-month prevalence of infertility globally is around 9% and more than 7 million children have been born by assisted reproductive technology (ART) procedures [
2,
3,
4]. It is worth noting that in some areas infertility rates are much higher, reaching about 30% [
5]. Despite many known causes of infertility, including ovulation failure, tubal factor infertility, male factors, and ovarian or uterine factors, in about 20–25% of couples looking for fertility treatment, the cause, or the causes, remain unexplained [
6]. The high prevalence of infertility worldwide makes the identification of modifiable predictors of a successful fertility treatment pertinent. Recently, thanks to some studies concerning an association between unexplained recurrent pregnancy loss (RPL) and the structure of the vaginal microbiota, it has been suggested that the presence of certain bacteria (i.e.,
Cutibacterium and
Anaerobacillus) could be a predictor of RPL in the absence of an aneuploid karyotype and that the cervicovaginal microbiota may be a useful area of investigation into possible causes of RPL [
7]. Vaginal bacterial communities are inter-ethnically classified in five different community state types (CST IV) according to bacterial richness and
Lactobacillus spp. dominance [
8]. Communities expressing low richness and
L. crispatus dominance (CST I) correlate with a low obstetric-gynaecological risk. Those characterized by high richness and poor
Lactobacillus dominance (CST IV) correlate mostly with vaginal discomfort and/or obstetric-gynaecological diseases [
9].
Regarding fertility, systematic review and meta-analysis have identified a negative correlation between vaginal microbiota with high
Lactobacillus content and female infertility [
10]. A recent study has also correlated the
L. crispatus pre-pregnancy dominance with a better chance of falling pregnant within 12 months [
11]. Two well-known negative predictors for pregnancy are polycystic ovary syndrome (PCOS) and obesity and in both cases, severalobservational studies describe a higher prevalence of non-
Lactobacillus-dominated vaginal microbiota; among the
Lactobacillus-dominated consortia,
L. crispatus was reported to be the least common [
12,
13,
14,
15,
16]. Reviews and meta-analysis describe a strong correlation between abnormal vaginal microbiota (CST IV) and failure of in vitro fertilization (IVF) with an odds ratio of 0.70 (95% CI = 0.49–0.99) [
17]. Similarly, the vaginal microbiota profile observed at the time of embryo transfer in women undergoing IVF or intracytoplasmic sperm injection (ICSI) with donated oocytes showed a higher proportion of samples dominated by
L. crispatus in women achieving a positive pregnancy test, clinical pregnancy, and live birth compared with those who did not [
18]. Moreover, recurrent implantation failure (RIF) is significantly more common in women with a non-
Lactobacillus-dominated vaginal microbiota [
19]. Again, the clinical pregnancy rate after intrauterine insemination positively correlates with a dominance of vaginal
L. crispatus [
20]. Despite this, the idea of a womb stably colonized by microbial communities in a healthy pregnancy remains a subject of debate [
21]. The correlation observed between fertility and vaginal microbiota could be based on the possible existence of an endometrial microbiota, whose eubiosis, dominated by the genus
Lactobacillus and particularly by the species
L. crispatus in a similar way to what is observed in cervicovaginal samples, would reduce the endometrial inflammatory phenomena, favouring the onset of pregnancy [
22,
23,
24,
25]. Although the debate regarding the presence of a physiologically expressed intrauterine microbiota capable of influencing fertility is still ongoing, the idea that elevated vaginal lactobacilli could have a beneficial effect on pregnancy outcome is generally accepted [
26,
27,
28,
29].
To our knowledge, the only attempt to positively affect the vaginal microbiota to restore a
Lactobacillus-dominated composition by means of a probiotic prior to fertility treatment failed [
30]. As a possible explanation, the authors suggested that perhaps the use of
L. crispatus strains would have a better chance ofsuccess. In fact, the trial was performed using a probiotic product containing strains of
L. gasseri and
L. rhamnosus. A double-blind, placebo-controlled, multicentre trial to evaluate the reproductive outcomes of IVF patients with abnormal vaginal microbiota treated with the likely most investigated strain of
L. crispatus (strain CTV-05) is currently ongoing [
31].
In January 2020, our department started to use the well-documented M247 strain of
L. crispatus in women undergoing IVF [
32]. This study is therefore concerned with the retrospective analysis of the results gathered from January 2020 to December 2021. As the aim of our work was to highlight a possible significant role of
L. crispatus in favoring clinical pregnancy and live birth rates, we have retrospectively compared the results obtained with the probiotic treatment with those obtained before its introduction (January 2018–December 2019) at the U.O.S.D. PMA of Conegliano Hospital (Treviso, Italy).
4. Discussion
Female causes of infertility include sexually transmitted infections, tuboperitoneal abnormalities, endometriosis, uterine anatomical abnormalities, as well as autoimmune, genetic, and endocrine disorders [
41,
42]. As in some cases the cause of female infertility still remains unknown, a dysbiotic vaginal microbiota—that is, one that is not
Lactobacillus-dominated or, more precisely, not
L. crispatus-dominated—has been proposed as a possible additional factor [
43]. ART is the most advanced approach to infertility treatment. Despite progress, the implantation rate of transferred embryos remains low. Success or failure in ART has been attributed to a woman’s age, weight, endometrial receptivity, embryo quality, and to the transfer technique used [
44,
45]. However, in many cases, the reasons for failure still remain unclear and an imbalanced vaginal microbiota has been proposed as a possible contributing factor. Indeed, a recent study observed that women with CST IV (that is, not-
Lactobacillus dominated), or with CST III (that is
L. iners dominated) or with CST II (
L. gasseri dominated), had a lower ART success rate than women with the
L. crispatus-predominant vaginal microbiota, that is, CST I [
46].
To analyze whether the treatment with a probiotic containing the species
L. crispatus could affect the success of ART, we retrospectively analyzed results routinely obtained in our hospital department over two years in which we treated 80 unfertile women with M247 orally, using a well-documented and safe strain of
L. crispatus described to increase, after oral administration, the vaginal content of
L. crispatus and also clinically capable of exerting an anti-HPV role [
47,
48,
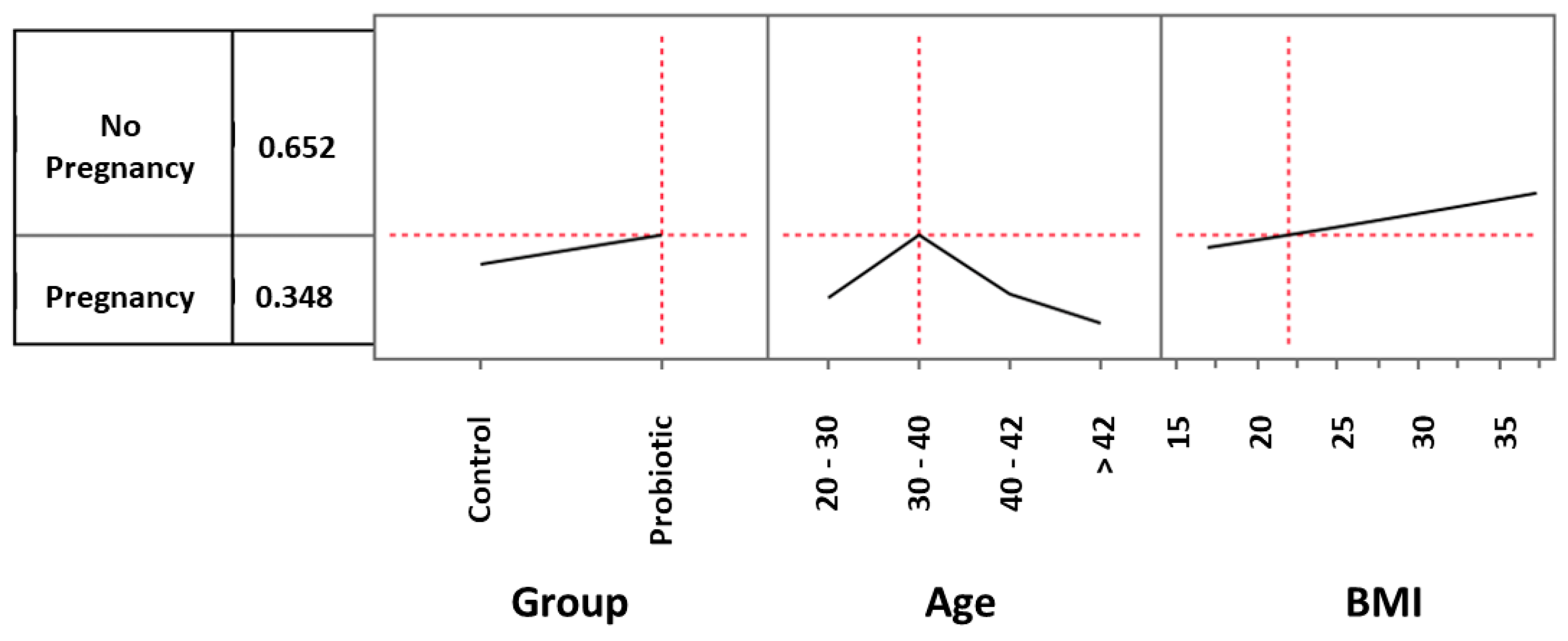
49]. Our analysis, performed by comparing two extremely similar groups of women, showed that, independent of the ART procedure adopted, treatment with the strain M247 increased the chance of a clinical pregnancy by 56%. The age and BMI ranges particularly favored by treatment with the probiotic were 30–40 (years) and 22–35 (kg/cm
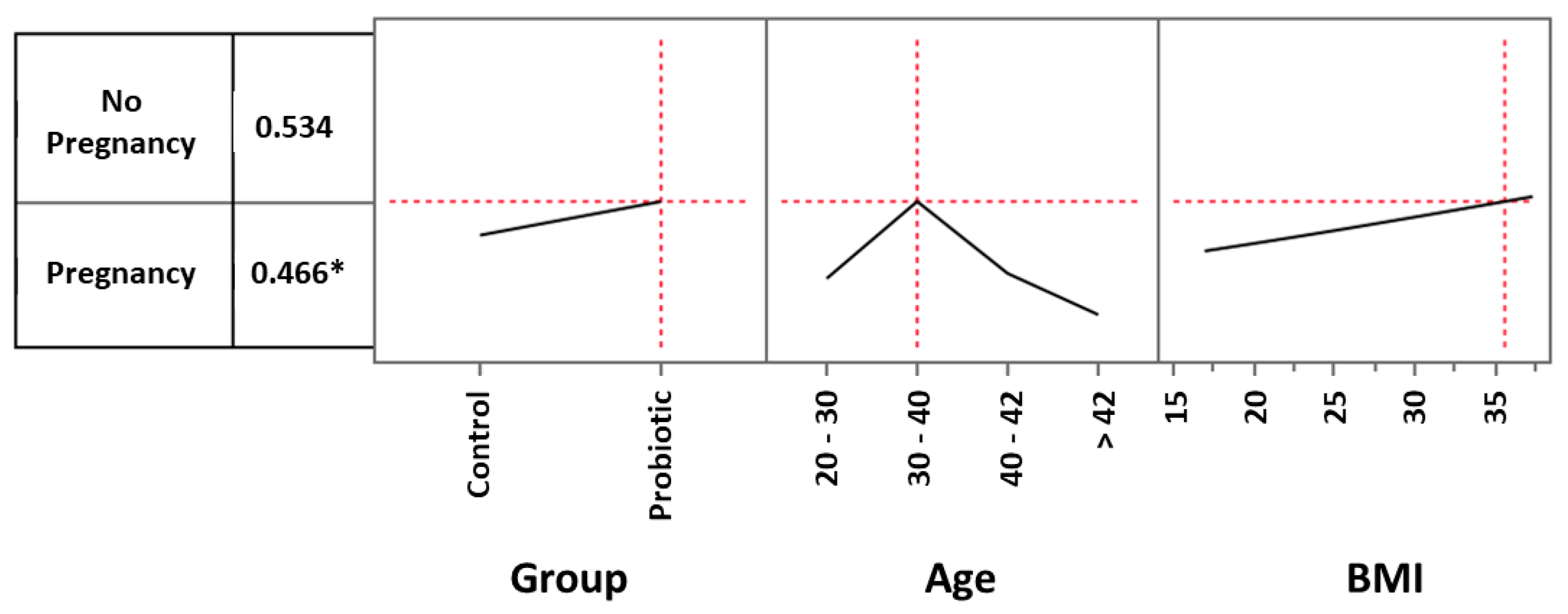
2), respectively. Within this range of age and with a BMI of 35, treatment with the probiotic increased the chance of a positive pregnancy test by 34%, versus an identical control independent of the ART procedure adopted. Besides age and BMI, the ART procedure adopted also demonstrated a favorable outcome. In fact, a woman subjected to embryo transfer with a D5- blastocysts, below 43 years, with a BMI over 18.6, and treated with the strain M247, had a significantly higher chance of a clinical pregnancy, with an increase of 66.3% versus an identical control.
While these results seem to demonstrate that the use of
L. crispatus M247 may significantly increase the chance of pregnancy, they do not help us to understand exactly why. Of course, our assumption is that the probiotic could improve the woman’s vaginal environment, enriching and/or restoring an eubiotic (CST I;
L. crispatus dominated) vaginal bacterial community. A trial on HPV-infected women and a very recent clinical case report hasin fact demonstrated the capability of the strain M247 to effectively restore a CST I [
47,
48]. Moreover, a study performed using a probe to specifically detect the strain M247 has shown that following oral treatment, the strain M247 was indeed found first in the gut and then the vaginal environment of a treated volunteer [
50].
Being a retrospective analysis of data obtained in our clinical routine and since the sampling and investigation of the vaginal microbiota are not routinely carried out either before or after treatment with the probiotic, it is impossible for us to demonstrate both the possibility of an effective colonization of the strain and/or the possible restoration of a vaginal microbiota classifiable as CST I or at least
Lactobacillus-dominated. Undeniably, having available data from which to deduce that the administered strain was able to improve vaginal eubiosis in women treated with the probiotic, with particular reference to those in whom a clinical pregnancy was subsequently demonstrated, could have allowed us to confirm some recent results which should seem to have demonstrated, in a very preliminary manner, a causative and anti-pathological role of the
L. crispatus species. Indeed, in the few cases of vaginal microbiota transplantation performed so far, in which CST IV women were transplanted with vaginal secretions from CST I women, the authors clearly demonstrated a shift of CST, from CST IV to CST I, together with the resolution of the “problem,” be it an intractable bacterial vaginosis condition or an infertility condition [
51,
52]. Similarly, the possibility that fecal dysbiosis could be a possible contributing cause of female infertility cannot be ruled out. In fact, numerous studies discuss the potential influence of gut microbiota on female fertility [
53,
54,
55]. Some studies have indeed highlighted the role of the M247 strain in counteracting dysbiosis and intestinal inflammation [
56,
57,
58]. It is therefore possible that the strain used in our study also played a role in re-establishing a certain intestinal eubiosis. However, since the gut microbiota of the enrolled women were not analyzed, we do not have the data to demonstrate this hypothesis.
The analysis of the data obtained clearly indicates that maternal age is decisive in favoring, or not, a clinical pregnancy. It is well recognized that increasing age contributes to difficulties in becoming pregnant. Fertility rates begin to decline gradually at the age of 30, more so at 35, and markedly at 40 [
59]. At this age, even with fertility treatments, women have more difficulty falling pregnant or may deliver an abnormal fetus [
60]. That said, the range in which the intake of the probiotic strain seems to play a favorable role compared to the control also includes rather ‘elevated’ ages close to 40, in which the success of ART normally tends to fall due to the decline of ovarian reserves, the reduction of oocyte competence and the high increase of embryo aneuploidies [
60,
61]. Our results could therefore indicate that the clinical effect of the probiotic is more evident in conditions in which age begins to become a discriminating element of failure. Noteworthy is the fact that as age increases, the percentage of women with non-
Lactobacillus-dominated vaginal microbiota also increases [
62]. A similar pattern is seen with BMI. Higher BMI values are certainly not considered to favor pregnancy and higher BMI values have long been considered to be a negative element in ART and in cases of euploid embryo transfer [
63,
64,
65]. Our data seem to show a more pronounced effect from the probiotic in BMI ranges considered unfavorable for pregnancy, such as those above 30. As previously mentioned for age, for BMI there is a certain correlation between weight gain and reduced vaginal eubiosis [
16]. It may therefore be that the probiotic influences those categories of women for whom the existence of a dysbiotic vaginal microbiota is described as more probable.
Regarding the ART method adopted, our analysis indicates blastocysts transfer as the method in which the probiotic seems to determine the greatest clinical success. One might wonder whether, as in the case of age and BMI, this procedure is the one favoring the least positive outcome and therefore the one in which the probiotic could show its greatest effects in restoring a correct vaginal eubiosis. However, we can also assume that the effect clearly identified in this subgroup is linked to a numerical issue, to the extent that any other method is so weakly represented in our study as to likely fail to demonstrate any possible therapeutic effect.
The number of women enrolled in our analysis is the first among the many limitations of our study. Indeed, in addition to the known limitations of non-prospective, non-randomized and non-blind studies, the results of which have maybe a lower predictive value in general terms, 160 women is perhaps too few in number to distinguish the effect of a probiotic in relation to the different procedures adopted. Having said that, our approach has been focused on obtaining the most controlled data possible, to the best of what can be done in a retrospective study. All the analyses performed indeed showed us that the two groups were extremely superimposable and therefore the data obtained with our analysis could be considered of sufficient quality.
In the attempt to understand how comparable the two groups were, we discovered a single difference between the two groups: the method of administration of the progesterone. Progesterone was mainly administered orally in the control group and mainly by injection in the probiotic-treated group. Statistical analysis, however, did not show any influence of this difference on the final result. Similarly, our study demonstrated no influence of other parameters such as the vaginal-rectal swab results or the antibiotic and/or antifungal therapy adopted.
A further limitation intrinsic to our retrospective analysis is the lack of information regarding the ploidy of the implanted embryos. This aspect would have allowed a better interpretation of the results obtained.
Within the framework of the obvious caution necessary when considering the results of non-blind, open-label, and retrospective studies, our analysis would seem to show that the administration of L. crispatus during the adoption of ART methods should in any case be considered safe and potentially advantageous to the extent that it would seem to increase the possibility of a clinical pregnancy by about 50%, regardless of age, BMI, and procedure adopted. This chance is further increased in women between 30 and 40 years of age and with a BMI greater than 22 and would further increase as the BMI increases, at least up to a value of 35. It is also possible that of all methods, the ART method using a 5-day blastocyst may highlight a greater success for the probiotic. In our study, in women under 43 years of age and with a BMI of at least around 20, this success was found to be significant (p < 0.05) with a net doubling of the chances of a clinical pregnancy. Larger, randomized, controlled, prospective, and double-blind studies are urgently needed to confirm the validity of what we have observed.
Of the women in our study who had a clinical pregnancy, we can report 10 and 6 live births from a total of 19 and 14 women in the probiotic group and control group, respectively. Despite the fact that these results are non-significant, the calculation of the odds ratio demonstrated an increase (by about 50% and 80% according to the number of women considered, see
Table 7) in the possibility of giving birth to a healthy child for women treated with the probiotic compared to women in the control group.
When evaluating exclusively the number of live births in relation to the ART method adopted, it appeared evident that the transfer of blastocysts was the one factor in which the effect of the probiotic was most evident, with the number of live births three times higher than that observed in controls. Blastocyst transfer is considered the method most capable of replicating the physiology of the natural intrauterine implant. It is therefore possible that in these conditions, the recovery of a vaginal eubiosis, an element that we hypothesize could have occurred as a consequence of the treatment with the probiotic, could have a particularly relevant positive impact for procreative purposes.
Finally, using specific statistical indices capable of extrapolating the risk-benefit ratio deriving from treating, or not, a woman with the L. crispatus M247 strain, we observed (i) a NNT value indicating that few patients need to be treated to achieve positive results; (ii) a NNH value suggesting that the treatment is less likely to cause harm compared to control; and (iii) a LHH value showing a higher likelihood of benefits compared to harms associated with the treatment. Taken together, these results indicate that there is a good overall probability that women undergoing ART may benefit from oral treatment with L. crispatus M247.


 ,
, 









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}