
Unexpected Vertical Transmission of SARS-CoV-2: Discordant Clinical Course and Transmission from Mother to Newborn

 , , ,
, , ,  , , and
, , and
Abstract
:1. Introduction
2. Case Description
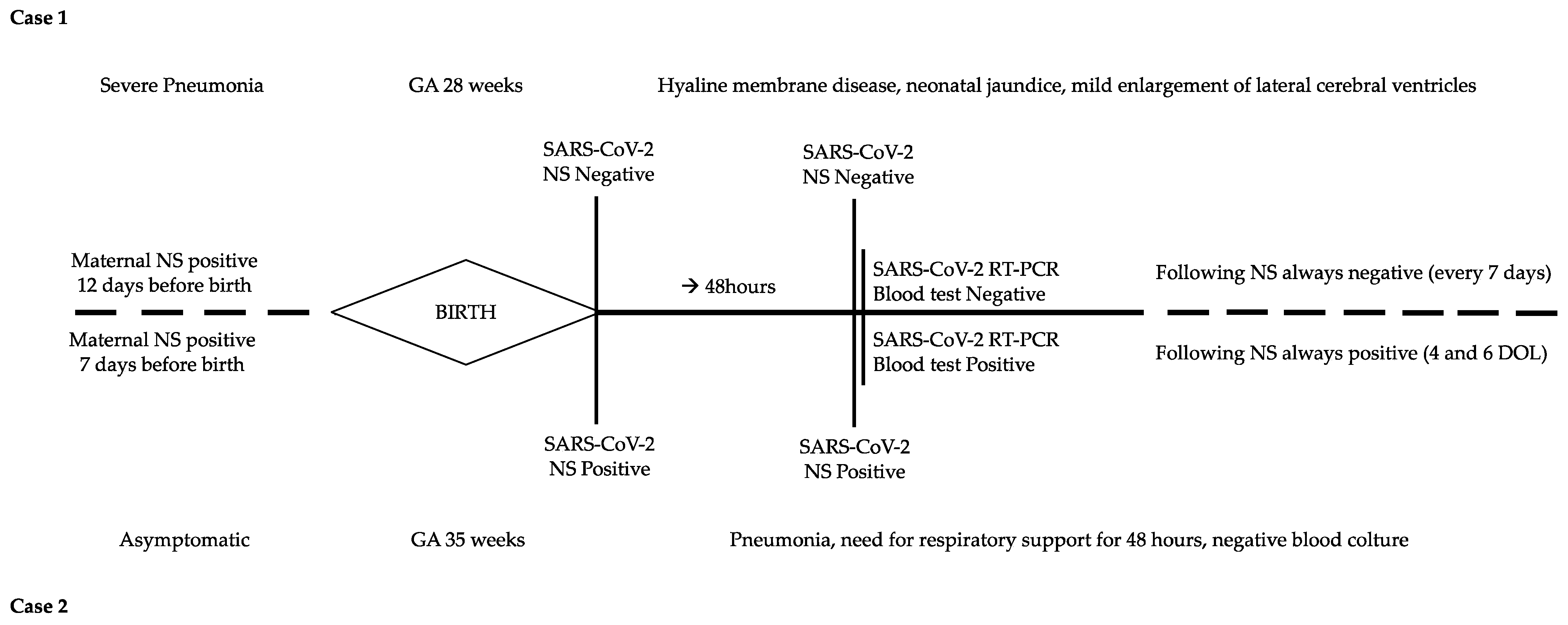
2.1. Case 1
2.2. Case 2
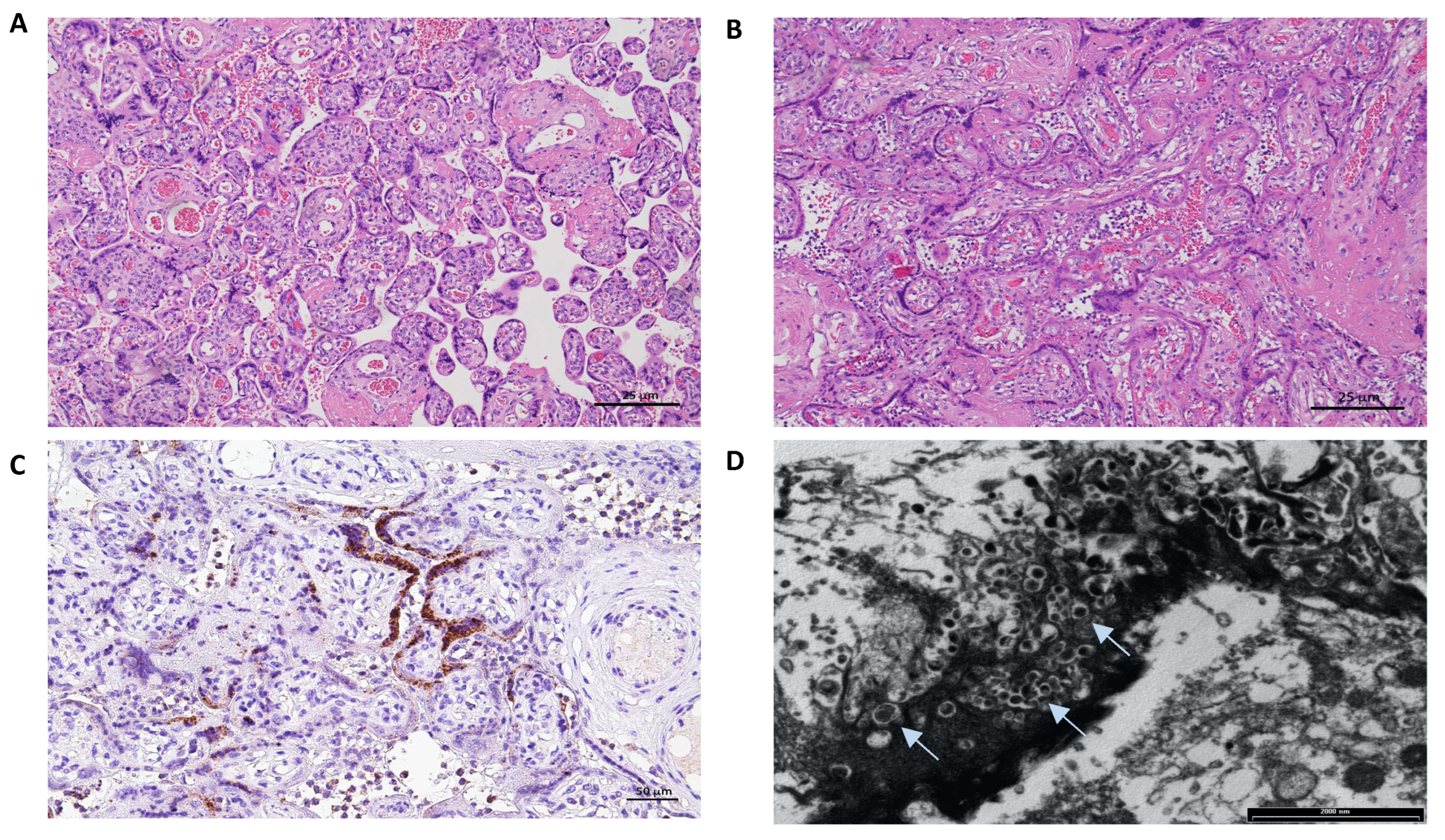
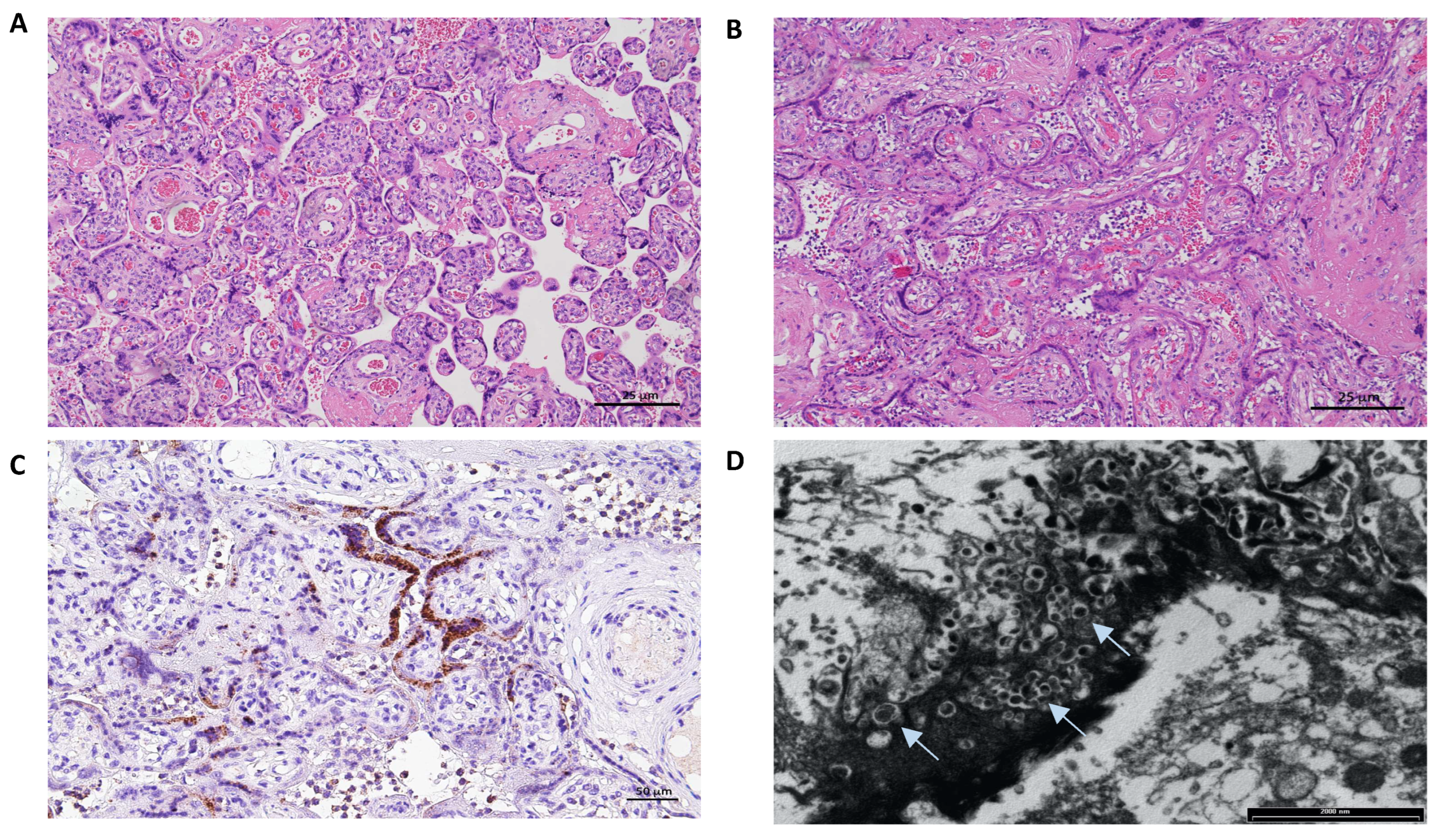
3. Placental Pathology
4. Discussion
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Gale, C.; Quigley, M.A.; Placzek, A.; Knight, M.; Ladhani, S.; Draper, E.S.; Sharkey, D.; Doherty, C.; Mactier, H.; Kurinczuk, J.J. Characteristics and Outcomes of Neonatal SARS-CoV-2 Infection in the UK: A Prospective National Cohort Study Using Active Surveillance. Lancet Child. Adolesc. Health 2021, 5, 113–121. [Google Scholar] [CrossRef]
- Forchette, L.; Sebastian, W.; Liu, T. A Comprehensive Review of COVID-19 Virology, Vaccines, Variants, and Therapeutics. Curr. Med. Sci. 2021, 41, 1037–1051. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.-L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Biasucci, G.; Cannalire, G.; Raymond, A.; Capra, M.E.; Benenati, B.; Vadacca, G.; Schiavo, R.; Pavesi, C.; Bonini, R. Safe Perinatal Management of Neonates Born to SARS-CoV-2 Positive Mothers at the Epicenter of the Italian Epidemic. Front. Pediatr. 2020, 8, 565522. [Google Scholar] [CrossRef]
- Joma, M.; Fovet, C.-M.; Seddiki, N.; Gressens, P.; Laforge, M. COVID-19 and Pregnancy: Vertical Transmission and Inflammation Impact on Newborns. Vaccines 2021, 9, 391. [Google Scholar] [CrossRef]
- Jafari, M.; Pormohammad, A.; Sheikh Neshin, S.A.; Ghorbani, S.; Bose, D.; Alimohammadi, S.; Basirjafari, S.; Mohammadi, M.; Rasmussen-Ivey, C.; Razizadeh, M.H.; et al. Clinical Characteristics and Outcomes of Pregnant Women with COVID-19 and Comparison with Control Patients: A Systematic Review and Meta-analysis. Rev. Med. Virol. 2021, 31, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Ryan, L.; Plötz, F.B.; van den Hoogen, A.; Latour, J.M.; Degtyareva, M.; Keuning, M.; Klingenberg, C.; Reiss, I.K.M.; Giannoni, E.; Roehr, C.; et al. Neonates and COVID-19: State of the Art: Neonatal Sepsis Series. Pediatr. Res. 2022, 91, 432–439. [Google Scholar] [CrossRef]
- Di Toro, F.; Gjoka, M.; Di Lorenzo, G.; De Santo, D.; De Seta, F.; Maso, G.; Risso, F.M.; Romano, F.; Wiesenfeld, U.; Levi-D’Ancona, R.; et al. Impact of COVID-19 on Maternal and Neonatal Outcomes: A Systematic Review and Meta-Analysis. Clin. Microbiol. Infect. 2021, 27, 36–46. [Google Scholar] [CrossRef]
- Mullins, E.; Evans, D.; Viner, R.M.; O’Brien, P.; Morris, E. Coronavirus in Pregnancy and Delivery: Rapid Review. Ultrasound Obs. Gynecol. 2020, 55, 586–592. [Google Scholar] [CrossRef]
- Pietrasanta, C.; Artieri, G.; Ronchi, A.; Crippa, B.; Ballerini, C.; Crimi, R.; Mosca, F.; Pugni, L. SARS-CoV-2 Infection and Neonates: Evidence-based Data after 18 Months of the Pandemic. Pediatric Allergy Immunol. 2022, 33, 96–98. [Google Scholar] [CrossRef]
- Trevisanuto, D.; Cavallin, F.; Cavicchiolo, M.E.; Borellini, M.; Calgaro, S.; Baraldi, E. Coronavirus Infection in Neonates: A Systematic Review. Arch. Dis. Child. Fetal Neonatal Ed. 2021, 106, 330–335. [Google Scholar] [CrossRef]
- Musa, S.S.; Bello, U.M.; Zhao, S.; Abdullahi, Z.U.; Lawan, M.A.; He, D. Vertical Transmission of SARS-CoV-2: A Systematic Review of Systematic Reviews. Viruses 2021, 13, 1877. [Google Scholar] [CrossRef]
- Perlman, J.M.; Salvatore, C. Coronavirus Disease 2019 Infection in Newborns. Clin. Perinatol. 2022, 49, 73–92. [Google Scholar] [CrossRef]
- WHO Scientific Brief, Definition and Categorization of the Timing of Mother-to-Child Transmission of SARS-CoV-2. 2021. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-mother-to-child-transmission-2021.1 (accessed on 4 November 2021).
- Vivanti, A.J.; Vauloup-Fellous, C.; Prevot, S.; Zupan, V.; Suffee, C.; Do Cao, J.; Benachi, A.; De Luca, D. Transplacental Transmission of SARS-CoV-2 Infection. Nat. Commun. 2020, 11, 3572. [Google Scholar] [CrossRef]
- Kotlyar, A.M.; Grechukhina, O.; Chen, A.; Popkhadze, S.; Grimshaw, A.; Tal, O.; Taylor, H.S.; Tal, R. Vertical Transmission of Coronavirus Disease 2019: A Systematic Review and Meta-Analysis. Am. J. Obstet. Gynecol. 2021, 224, 35–53.e3. [Google Scholar] [CrossRef]
- Goh, X.L.; Low, Y.F.; Ng, C.H.; Amin, Z.; Ng, Y.P.M. Incidence of SARS-CoV-2 Vertical Transmission: A Meta-Analysis. Arch. Dis. Child. Fetal Neonatal Ed. 2021, 106, 112–113. [Google Scholar] [CrossRef]
- Raschetti, R.; Vivanti, A.J.; Vauloup-Fellous, C.; Loi, B.; Benachi, A.; De Luca, D. Synthesis and Systematic Review of Reported Neonatal SARS-CoV-2 Infections. Nat. Commun. 2020, 11, 5164. [Google Scholar] [CrossRef]
- Schwartz, D.A. An Analysis of 38 Pregnant Women With COVID-19, Their Newborn Infants, and Maternal-Fetal Transmission of SARS-CoV-2: Maternal Coronavirus Infections and Pregnancy Outcomes. Arch. Pathol. Lab. Med. 2020, 144, 799–805. [Google Scholar] [CrossRef]
- Rad, H.S.; Röhl, J.; Stylianou, N.; Allenby, M.C.; Bazaz, S.R.; Warkiani, M.E.; Guimaraes, F.S.F.; Clifton, V.L.; Kulasinghe, A. The Effects of COVID-19 on the Placenta During Pregnancy. Front. Immunol. 2021, 12, 743022. [Google Scholar] [CrossRef]
- Algarroba, G.N.; Rekawek, P.; Vahanian, S.A.; Khullar, P.; Palaia, T.; Peltier, M.R.; Chavez, M.R.; Vintzileos, A.M. Visualization of Severe Acute Respiratory Syndrome Coronavirus 2 Invading the Human Placenta Using Electron Microscopy. Am. J. Obstet. Gynecol. 2020, 223, 275–278. [Google Scholar] [CrossRef]
- Patberg, E.T.; Adams, T.; Rekawek, P.; Vahanian, S.A.; Akerman, M.; Hernandez, A.; Rapkiewicz, A.V.; Ragolia, L.; Sicuranza, G.; Chavez, M.R.; et al. Coronavirus Disease 2019 Infection and Placental Histopathology in Women Delivering at Term. Am. J. Obstet. Gynecol. 2021, 224, 382.e1–382.e18. [Google Scholar] [CrossRef]
- Schwartz, D.A.; Morotti, D. Placental Pathology of COVID-19 with and without Fetal and Neonatal Infection: Trophoblast Necrosis and Chronic Histiocytic Intervillositis as Risk Factors for Transplacental Transmission of SARS-CoV-2. Viruses 2020, 12, 1308. [Google Scholar] [CrossRef]
- Lugli, L.; Bedetti, L.; Guidotti, I.; Pugliese, M.; Picciolini, O.; Roversi, M.F.; DellaCasa Muttini, E.; Lucaccioni, L.; Bertoncelli, N.; Ancora, G.; et al. Neuroprem 2: An Italian Study of Neurodevelopmental Outcomes of Very Low Birth Weight Infants. Front. Pediatr. 2021, 9, 697100. [Google Scholar] [CrossRef] [PubMed]
- Allotey, J.; Chatterjee, S.; Kew, T.; Gaetano, A.; Stallings, E.; Fernández-García, S.; Yap, M.; Sheikh, J.; Lawson, H.; Coomar, D.; et al. SARS-CoV-2 Positivity in Offspring and Timing of Mother-to-Child Transmission: Living Systematic Review and Meta-Analysis. BMJ 2022, 376, e067696. [Google Scholar] [CrossRef] [PubMed]
- Salvatore, M.A.; Corsi Decenti, E.; Bonasoni, M.P.; Botta, G.; Castiglione, F.; D’Armiento, M.; Fulcheri, E.; Nebuloni, M.; Donati, S.; the ItOSS COVID-19 Working Group. Placental Characteristics of a Large Italian Cohort of SARS-CoV-2-Positive Pregnant Women. Microorganisms 2022, 10, 1435. [Google Scholar] [CrossRef] [PubMed]
- Suhren, J.-T.; Meinardus, A.; Hussein, K.; Schaumann, N. Meta-Analysis on COVID-19-Pregnancy-Related Placental Pathologies Shows No Specific Pattern. Placenta 2022, 117, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Chaubey, I.; Vignesh, R.; Babu, H.; Wagoner, I.; Govindaraj, S.; Velu, V. SARS-CoV-2 in Pregnant Women: Consequences of Vertical Transmission. Front. Cell. Infect. Microbiol. 2021, 11, 717104. [Google Scholar] [CrossRef]
- Watkins, J.C.; Torous, V.F.; Roberts, D.J. Defining Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Placentitis. Arch. Pathol. Lab. Med. 2021, 145, 1341–1349. [Google Scholar] [CrossRef]
- Argueta, L.B.; Lacko, L.A.; Bram, Y.; Tada, T.; Carrau, L.; Zhang, T.; Uhl, S.; Lubor, B.C.; Chandar, V.; Gil, C.; et al. SARS-CoV-2 Infects Syncytiotrophoblast and Activates Inflammatory Responses in the Placenta. bioRxiv 2021. [Google Scholar] [CrossRef]
- Stenton, S.; McPartland, J.; Shukla, R.; Turner, K.; Marton, T.; Hargitai, B.; Bamber, A.; Pryce, J.; Peres, C.L.; Burguess, N.; et al. SARS-COV2 Placentitis and Pregnancy Outcome: A Multicentre Experience during the Alpha and Early Delta Waves of Coronavirus Pandemic in England. eClinicalMedicine 2022, 47, 101389. [Google Scholar] [CrossRef]
- Weber, M.A.; Nikkels, P.G.J.; Hamoen, K.; Duvekot, J.J.; de Krijger, R. Co-Occurrence of Massive Perivillous Fibrin Deposition and Chronic Intervillositis: Case Report. Pediatr. Dev. Pathol. 2006, 9, 234–238. [Google Scholar] [CrossRef]
- Chen, A.; Roberts, D.J. Placental Pathologic Lesions with a Significant Recurrence Risk—What Not to Miss! APMIS 2018, 126, 589–601. [Google Scholar] [CrossRef]
- Lugli, L.; Bedetti, L.; Lucaccioni, L.; Gennari, W.; Leone, C.; Ancora, G.; Berardi, A. An Uninfected Preterm Newborn Inadvertently Fed SARS-CoV-2–Positive Breast Milk. Pediatrics 2020, 146, e2020004960. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Data | Case 1 | Case 2 |
|---|---|---|
| Maternal characteristics | ||
| Ethnic Group | North African | Caucasian |
| Pre-existing medical conditions | Nephrotic syndrome in remission | None |
| BMI | <25 | <25 |
| Sociodemographic risk factors | NA | NA |
| Smoking | No | No |
| Pregnancy course | Regular | Regular |
| Antenatal exams | Normal | Normal |
| Maternal symptoms | Severe pneumonia | Asymptomatic |
| Maternal laboratory findings | ||
| Platelets (109/L) | 303 | 130 |
| Hemoglobin (g/dL) | 9.8 | 12.2 |
| LDH (U/L) | 1045 | 1313 |
| D-dimer (ng/dL) | 1440 | >40,000 |
| CRP (mg/dL) | 13.3 | 3.4 |
| IL-6 (pg/mL) | 326.1 | NA |
| Blood SARS-CoV-2 (copies/mL) | 1066 | NA |
| Neonatal characteristics | ||
| Signs/symptoms | Hyaline membrane disease | Pneumonia |
| Neonatal SARS-CoV-2 investigations (Real-time polymerase chain reaction, RT-PCR) | ||
| Nasopharyngeal swab at birth | Negative | Positive |
| Nasopharyngeal swab at 48 h of life | Negative | Positive |
| Nasopharyngeal swab until discharge | Every 7 days, always negative | Positive at DOL 4 and 6 |
| Blood (copies/mL) | Negative | 1108 |
| Placental examinations | ||
| RT-PCR SARS-CoV-2 (copies/µg) | Negative | 1,068,963 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boncompagni, A.; De Agostini, M.; Lugli, L.; Ternelli, G.; Colonna, V.; Biagioni, E.; Bonasoni, M.P.; Salviato, T.; Gabrielli, L.; Falconi, M.; et al. Unexpected Vertical Transmission of SARS-CoV-2: Discordant Clinical Course and Transmission from Mother to Newborn. Microorganisms 2022, 10, 1718. https://doi.org/10.3390/microorganisms10091718
Boncompagni A, De Agostini M, Lugli L, Ternelli G, Colonna V, Biagioni E, Bonasoni MP, Salviato T, Gabrielli L, Falconi M, et al. Unexpected Vertical Transmission of SARS-CoV-2: Discordant Clinical Course and Transmission from Mother to Newborn. Microorganisms. 2022; 10(9):1718. https://doi.org/10.3390/microorganisms10091718
Chicago/Turabian StyleBoncompagni, Alessandra, Mattia De Agostini, Licia Lugli, Giliana Ternelli, Valeria Colonna, Emanuela Biagioni, Maria Paola Bonasoni, Tiziana Salviato, Liliana Gabrielli, Mirella Falconi, and et al. 2022. "Unexpected Vertical Transmission of SARS-CoV-2: Discordant Clinical Course and Transmission from Mother to Newborn" Microorganisms 10, no. 9: 1718. https://doi.org/10.3390/microorganisms10091718
APA StyleBoncompagni, A., De Agostini, M., Lugli, L., Ternelli, G., Colonna, V., Biagioni, E., Bonasoni, M. P., Salviato, T., Gabrielli, L., Falconi, M., Facchinetti, F., & Berardi, A. (2022). Unexpected Vertical Transmission of SARS-CoV-2: Discordant Clinical Course and Transmission from Mother to Newborn. Microorganisms, 10(9), 1718. https://doi.org/10.3390/microorganisms10091718