
Cutaneous Complications of mRNA and AZD1222 COVID-19 Vaccines: A Worldwide Review

 ,
,  ,
, 

Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Extraction of Data
2.4. Quality of Evidence Assessment
3. Results
3.1. Quality of Evidence Assessment
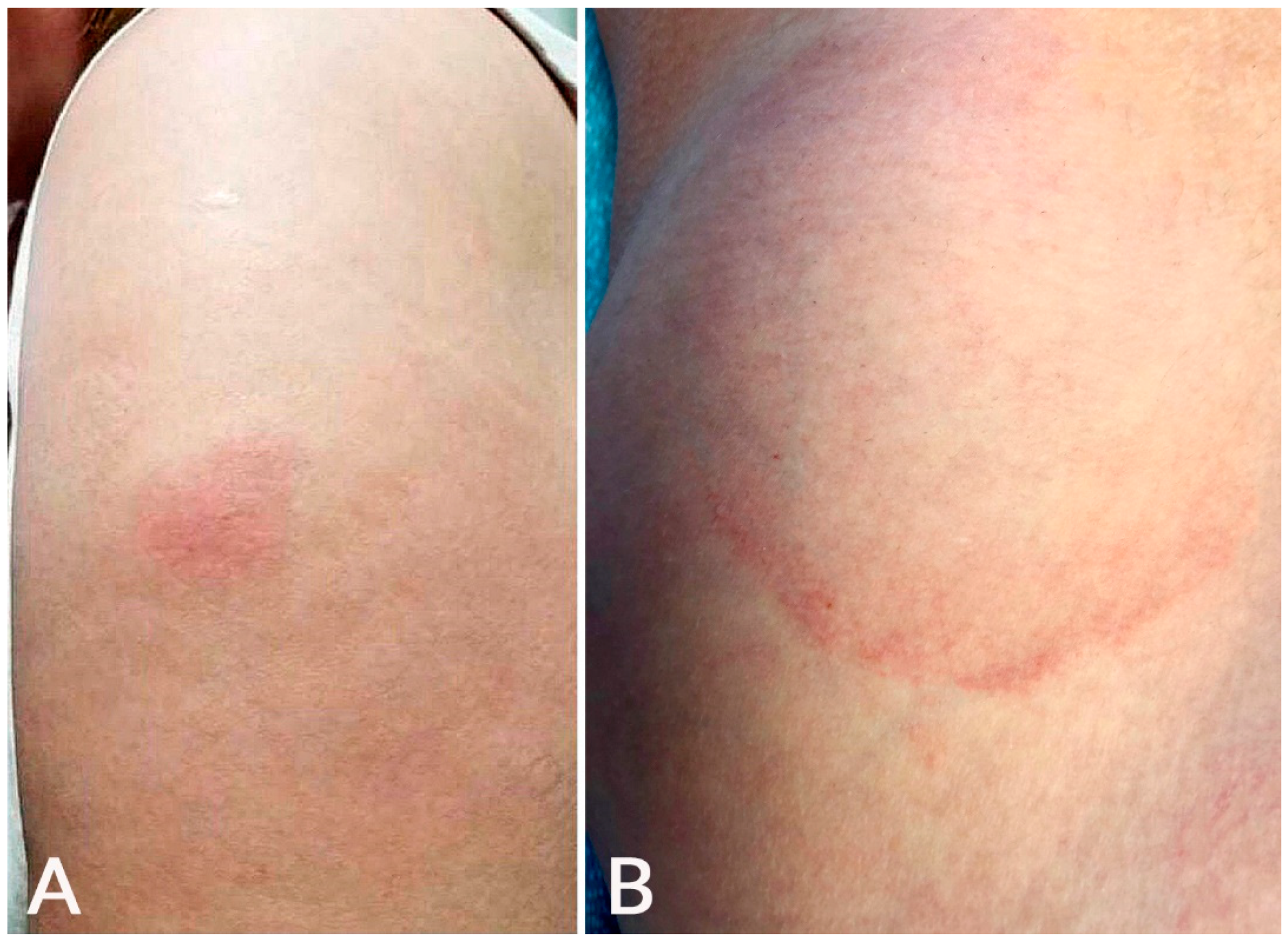
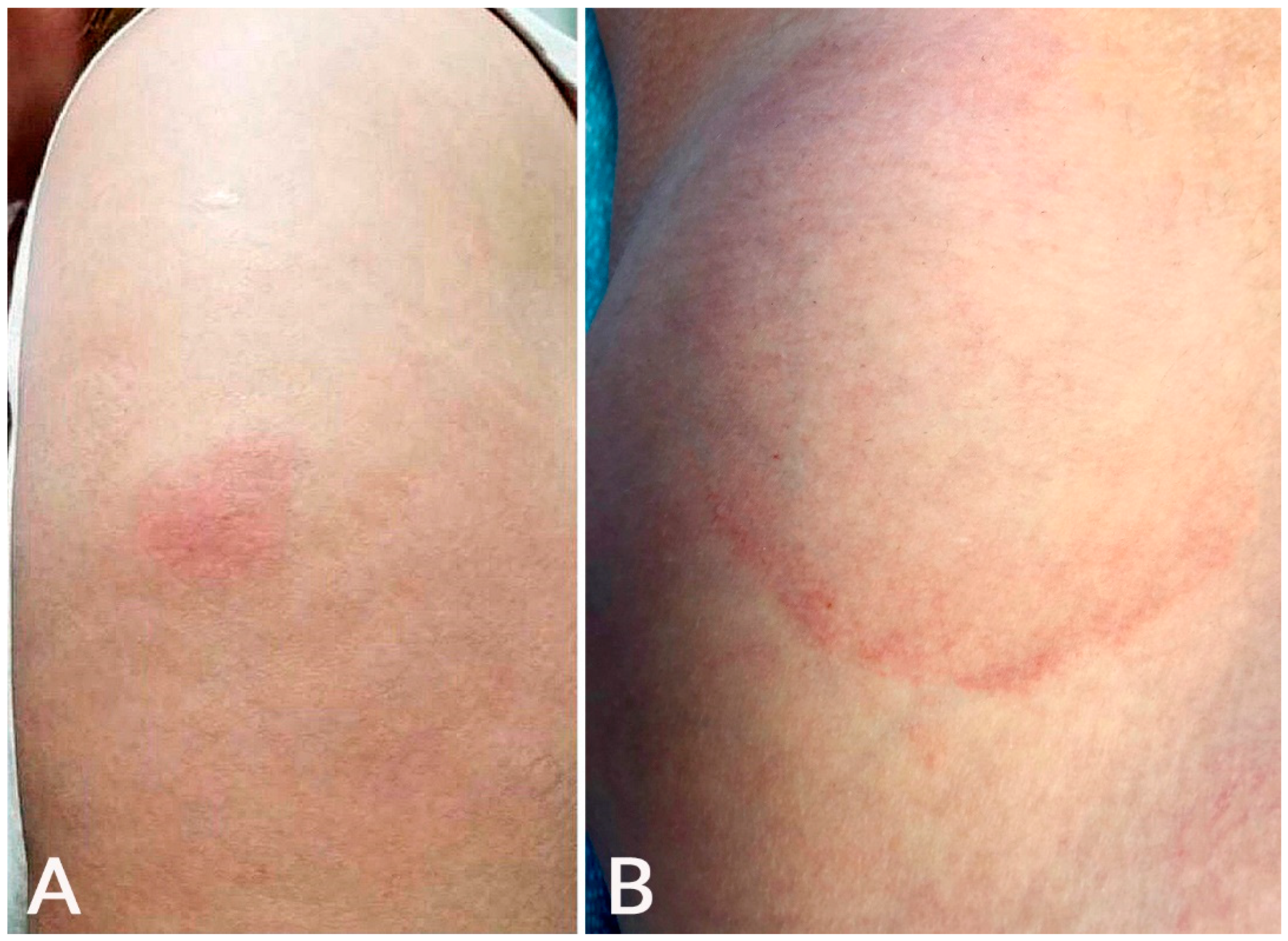
3.2. Local Site Injection Reaction
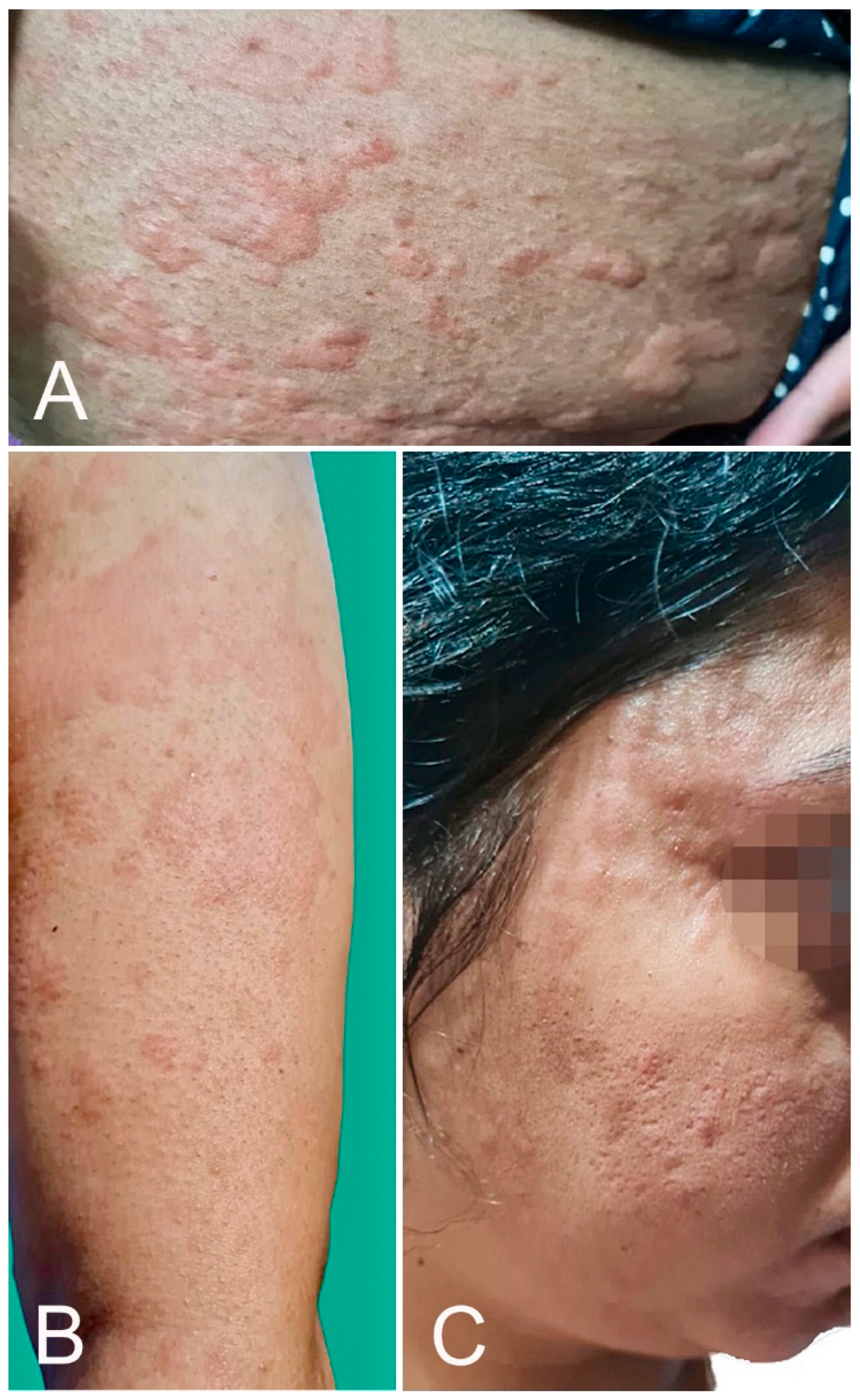
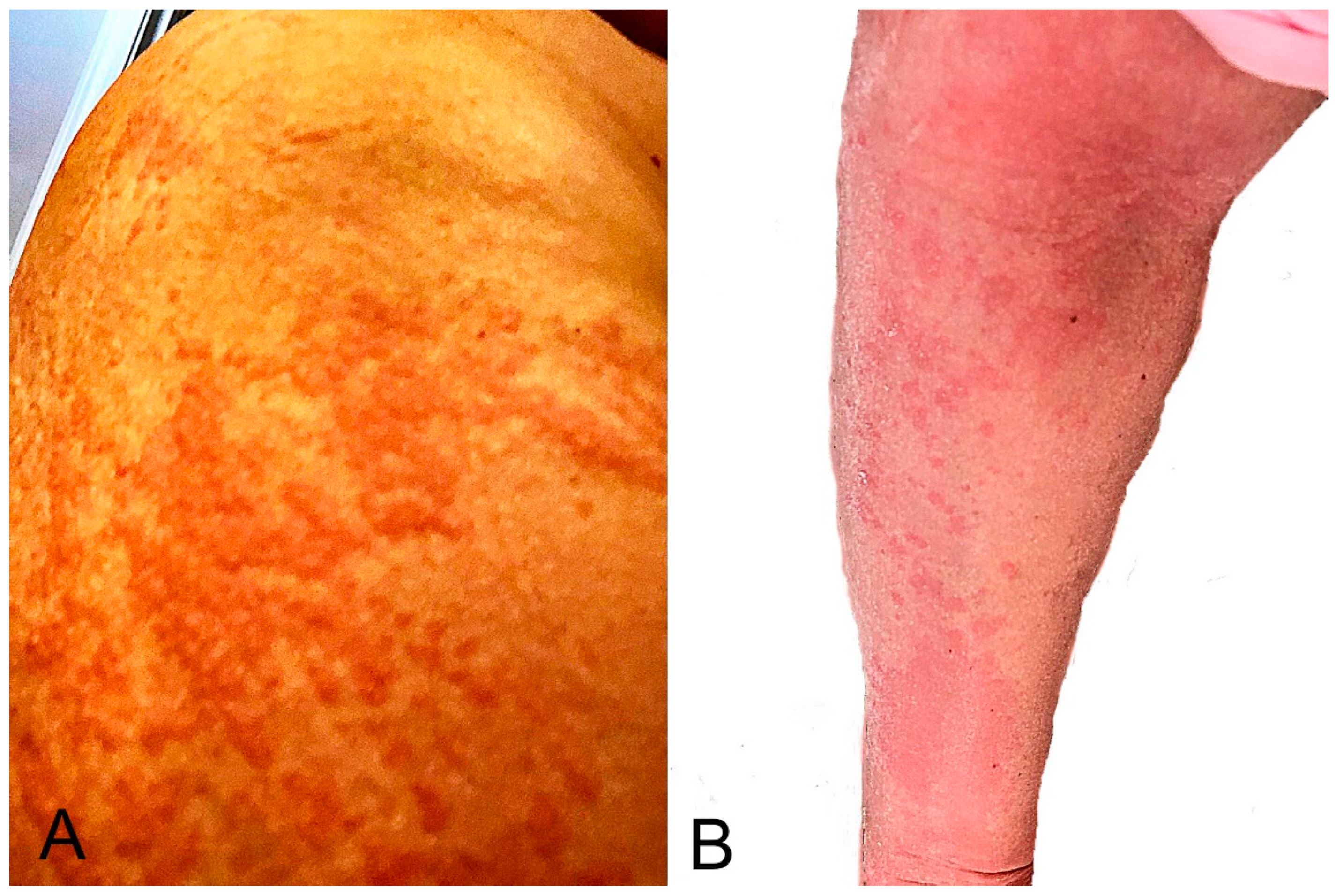
3.3. Urticaria
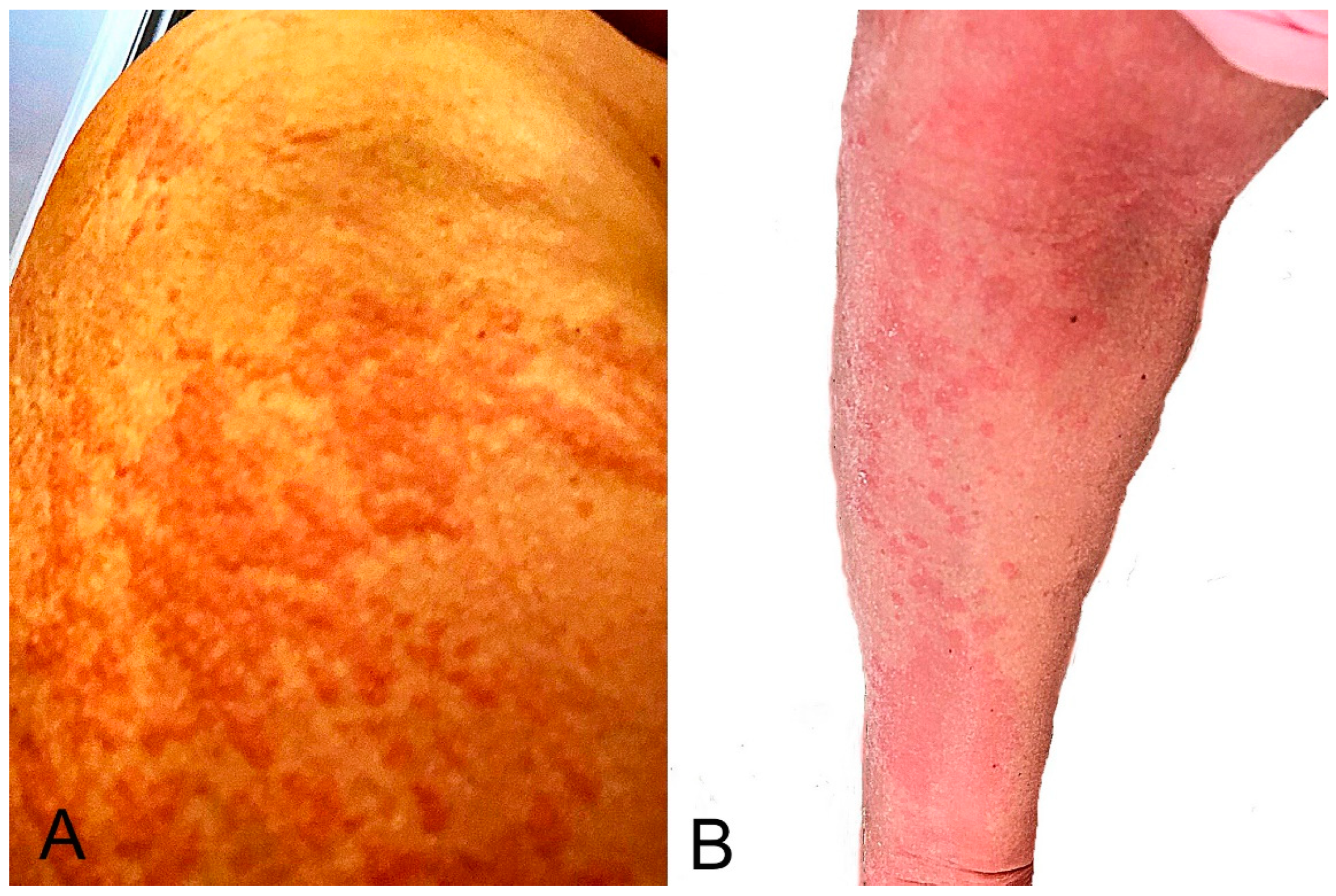
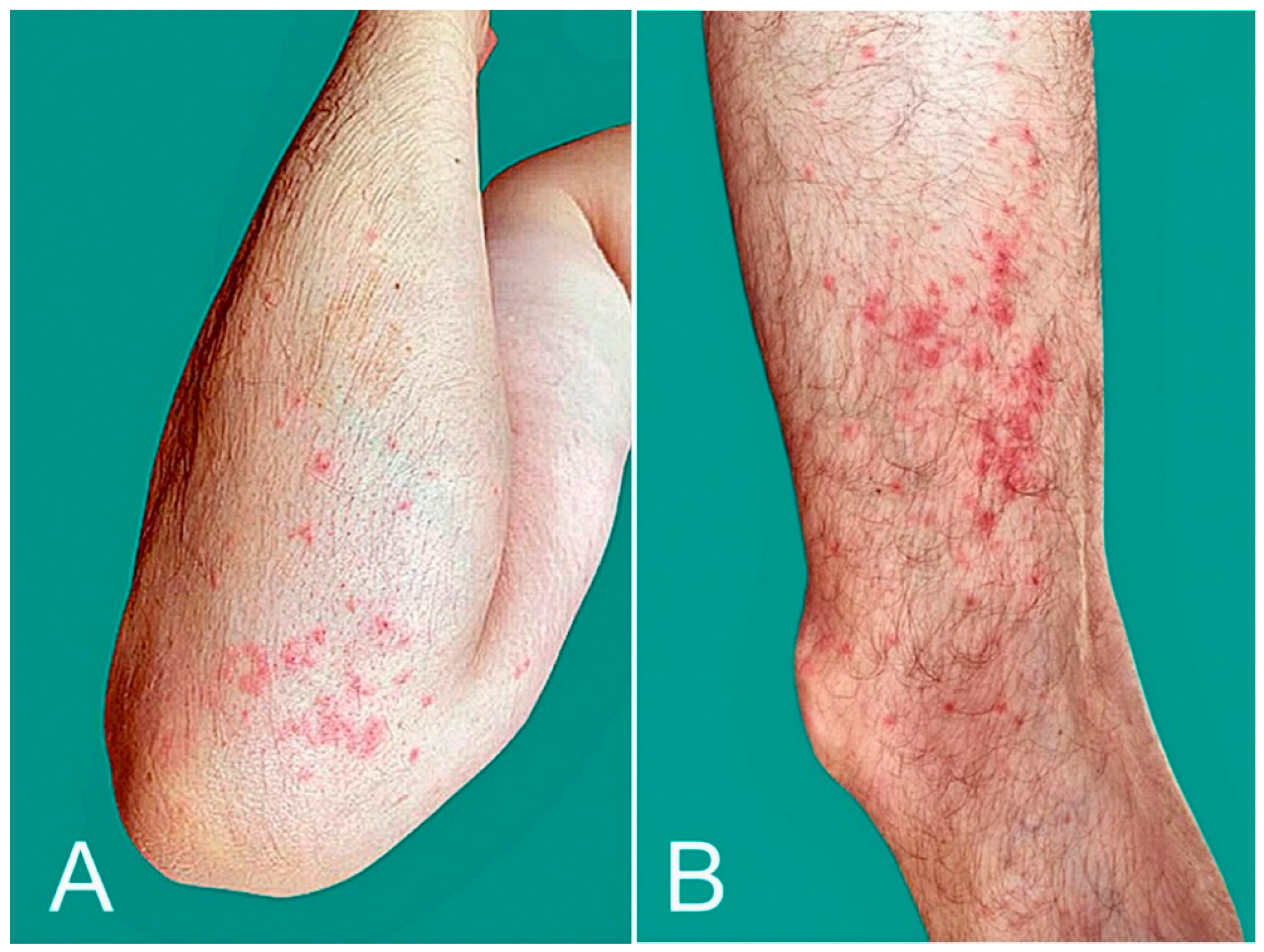
3.4. Mobilliform Eruption
3.5. Varicella Zoster Virus (VZV) and Herpes Simplex Virus (HSV) Reactivation
3.6. Pityriasis Rosea-like Eruption
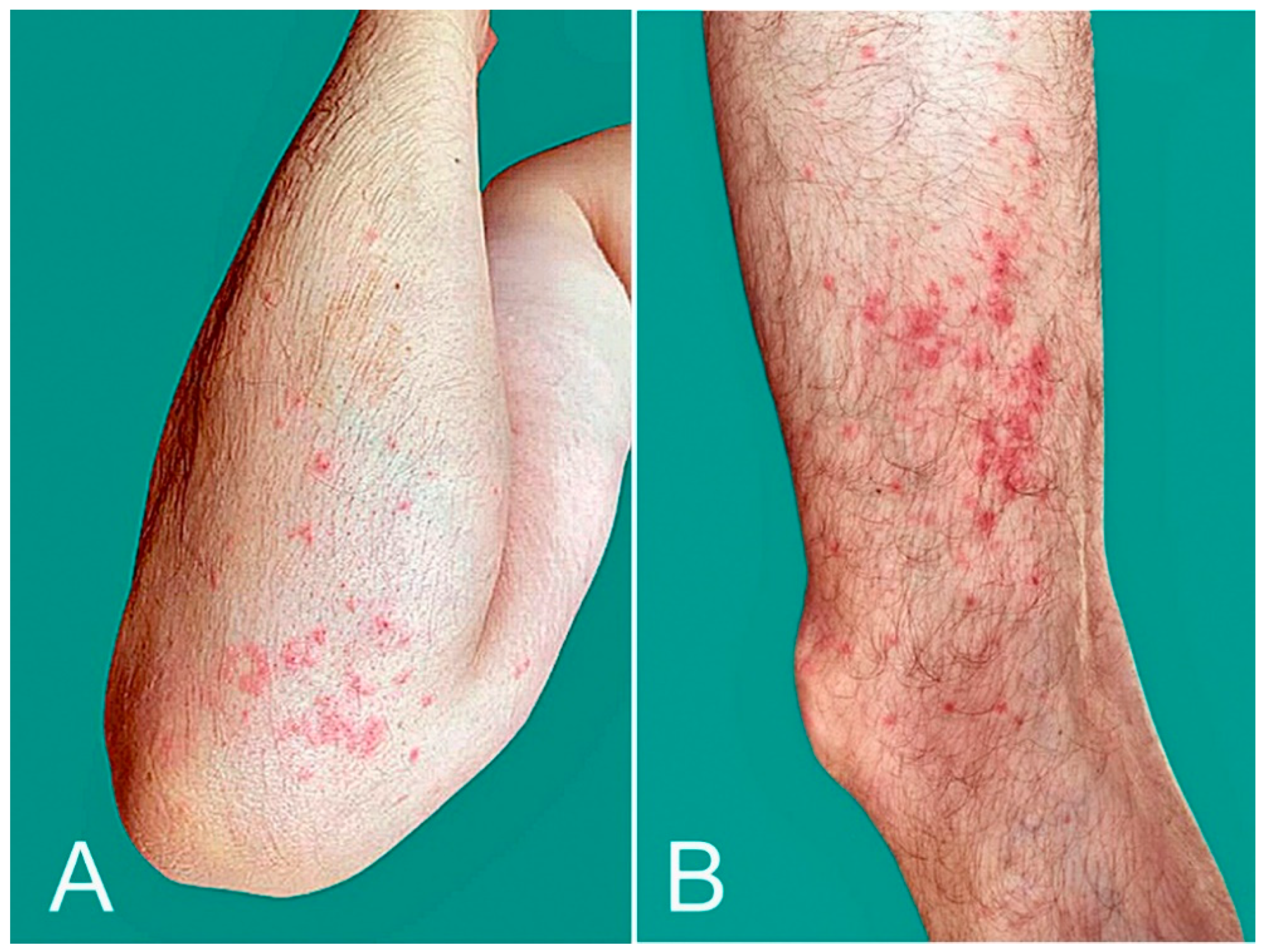
3.7. Pernio, Chilblains, and Purpura
3.8. Delayed Inflammatory Reaction (DIR) to Dermal Hyaluronic Acid Filler
3.9. Unusual Reactions
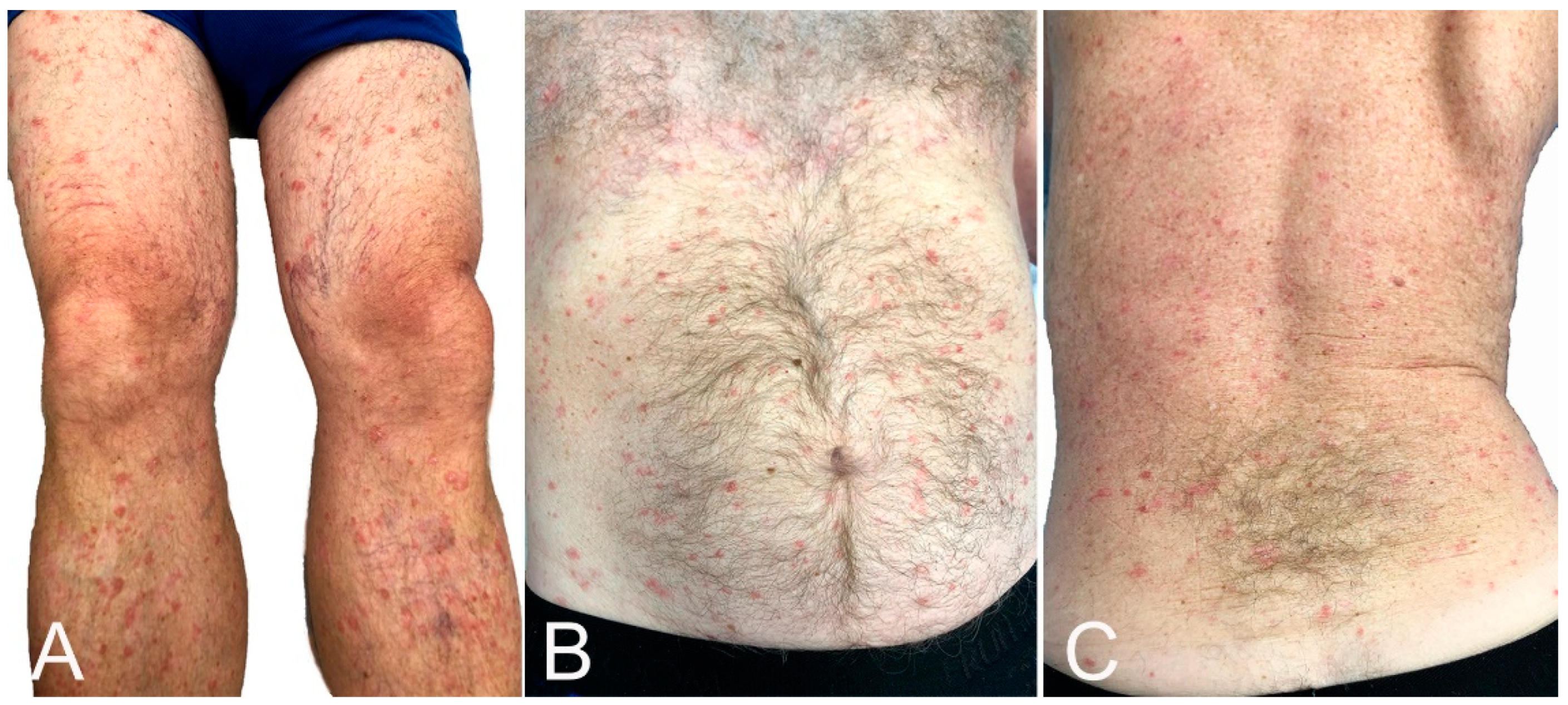
3.9.1. Papulovesicular Lesions
3.9.2. Vesiculobullous Lesions
3.9.3. Erythromelalgia
3.9.4. Eczematous Eruption
3.9.5. Other Eruptions
3.9.6. Exacerbation of Pre-Existing Skin Condition
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McMahon, D.E.; Amerson, E.; Rosenbach, M.; Lipoff, J.B.; Moustafa, D.; Tyagi, A.; Desai, S.R.; French, L.E.; Lim, H.W.; Thiers, B.H.; et al. Cutaneous reactions reported after Moderna and Pfizer COVID-19 vaccination: A registry-based study of 414 cases. J. Am. Acad. Dermatol. 2021, 85, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Català, A.; Munoz-Santos, C.; Galvan-Casas, C.; Roncero Riesco, M.; Revilla Nebreda, D.; Solá-Truyols, A.; Giavedoni, P.; Llamas-Velasco, M.; González-Cruz, C.; Cubiró, X.; et al. Cutaneous reactions after SARS-CoV-2 vaccination: A cross-sectional Spanish nationwide study of 405 cases. Br. J. Dermatol. 2021. epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Robinson, L.B.; Fu, X.; Hashimoto, D.; Wickner, P.; Shenoy, E.S.; Landman, A.B.; Blumenthal, K.G. Incidence of cutaneous reactions after messenger RNA COVID-19 vaccines. JAMA Dermatol. 2021, 157, 1000–1002. [Google Scholar] [CrossRef]
- Menni, C.; Klaser, K.; May, A.; Polidori, L.; Capdevila, J.; Louca, P.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Merino, J.; et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: A prospective observational study. Lancet Infect. Dis. 2021, 21, 939–949. [Google Scholar] [CrossRef]
- JAMA Network Open—Instructions for Authors: Ratings of the Quality of the Evidence. Available online: https://jamanetwork.com/journals/jamanetworkopen/pages/instructions-for-authors#SecRatingsofQuality (accessed on 17 January 2022).
- The Centre for Evidence-Based Medicine. Available online: https://www.cebm.net (accessed on 17 January 2022).
- Fernandez-Nieto, D.; Hammerle, J.; Fernandez-Escribano, M.; Moreno-Del Real, C.M.; Garcia-Abellas, P.; Carretero-Barrio, I.; Solano-Solares, E.; de la Hoz-Caballer, B.; Jimenez-Cauhe, J.; Ortega-Quijano, D.; et al. Skin manifestations of the BNT162b2 mRNA COVID-19 vaccine in healthcare workers. ‘COVID-arm’: A clinical and histological characterization. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e425–e427. [Google Scholar] [CrossRef] [PubMed]
- Juárez Guerrero, A.; Domínguez Estirado, A.; Crespo Quirós, J.; Rojas-Pérez-Ezquerra, P. Delayed cutaneous reactions after the administration of mRNA vaccines against COVID-19. J. Allergy Clin. Immunol. Pract. 2021, 9, 3811–3813. [Google Scholar] [CrossRef]
- Blumenthal, K.G.; Freeman, E.E.; Saff, R.R.; Robinson, L.B.; Wolfson, A.R.; Foreman, R.K.; Hashimoto, D.; Banerji, A.; Li, L.; Anvari, S.; et al. Delayed large local reactions to mRNA-1273 vaccine against SARS-CoV-2. N. Engl. J. Med. 2021, 384, 1273–1277. [Google Scholar] [CrossRef]
- Johnston, M.S.; Galan, A.; Watsky, K.L.; Little, A.J. Delayed localized hypersensitivity reactions to the Moderna COVID-19 vaccine: A case series. JAMA Dermatol. 2021, 157, 716–720. [Google Scholar] [CrossRef]
- Jacobson, M.A.; Zakaria, A.; Maung, Z.; Hart, C.; McCalmont, T.; Fassett, M.; Amerson, E. Incidence and characteristics of delayed injection site reaction to the mRNA-1273 SARS-CoV2 vaccine (Moderna) in a cohort of hospital employees. Clin. Infect. Dis. 2021, 74, 591–596. [Google Scholar] [CrossRef]
- Ramos, C.L.; Kelso, J.M. “COVID Arm”: Very delayed large injection site reactions to mRNA COVID-19 vaccines. J. Allergy Clin. Immunol. Pract. 2021, 9, 2480–2481. [Google Scholar] [CrossRef]
- Hoff, N.P.; Freise, N.F.; Schmidt, A.G.; Firouzi-Memarpuri, P.; Reifenberger, J.; Luedde, T.; Bölke, E.; Meller, S.; Homey, B.; Feldt, T.; et al. Delayed skin reaction after mRNA-1273 vaccine against SARS-CoV-2: A rare clinical reaction. Eur. J. Med. Res. 2021, 26, 98. [Google Scholar] [CrossRef] [PubMed]
- Wei, N.; Fishman, M.; Wattenberg, D.; Gordon, M.; Lebwohl, M. “COVID arm”: A reaction to the Moderna vaccine. JAAD Case Rep. 2021, 10, 92–95. [Google Scholar] [CrossRef] [PubMed]
- Shin, E.; Bae, S.; Jung, J.; Song, W.J.; Kwon, H.S.; Kim, H.S.; Kim, S.H.; Kim, T.B.; Cho, Y.S.; Lee, J.H. Delayed local reactions after the first administration of the ChAdOx1 nCoV-19 vaccine. Allergy 2021, 76, 3520–3522. [Google Scholar] [CrossRef] [PubMed]
- Choi, E.; Liew, C.F.; Oon, H.H. Cutaneous adverse effects and contraindications to COVID-19 vaccination; four cases and an illustrative review from an Asian country. Dermatol. Ther. 2021, 34, e15123. [Google Scholar] [CrossRef]
- Tihy, M.; Menzinger, S.; André, R.; Laffitte, E.; Toutous-Trellu, L.; Kaya, G. Clinicopathological features of cutaneous reactions after mRNA-based COVID-19 vaccines. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 2456–2461. [Google Scholar] [CrossRef]
- CDC COVID-19 Response Team; Food and Drug Administration. Allergic reactions including anaphylaxis after receipt of the first dose of Pfizer-BioNTech COVID-19 vaccine—United States, December 14–23, 2020. Morb. Mortal. Wkly. Rep. 2021, 70, 46–51. [Google Scholar] [CrossRef]
- Sidlow, J.S.; Reichel, M.; Lowenstein, E.J. Localized and generalized urticarial allergic dermatitis secondary to SARS-CoV-2 vaccination in a series of 6 patients. JAAD Case Rep. 2021, 14, 13–16. [Google Scholar] [CrossRef]
- Kelso, J.M. Misdiagnosis of systemic allergic reactions to mRNA COVID-19 vaccines. Ann. Allergy Asthma Immunol. 2021, 127, 133–134. [Google Scholar] [CrossRef]
- Yu, J.N.; Angeles, C.B.; Lim, H.G.; Chavez, C.; Roxas-Rosete, C. Cutaneous reactions to inactivated SARS-CoV-2 vaccine and ChAdOx1-S (recombinant) vaccine against SARS-CoV-2: A case series from the Philippines. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e841–e845. [Google Scholar] [CrossRef]
- Corbeddu, M.; Diociaiuti, A.; Vinci, M.R.; Santoro, A.; Camisa, V.; Zaffina, S.; El Hachem, M. Transient cutaneous manifestations after administration of Pfizer-BioNTech COVID-19 Vaccine: An Italian single-centre case series. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e483–e485. [Google Scholar] [CrossRef]
- Niebel, D.; Wenzel, J.; Wilsmann-Theis, D.; Ziob, J.; Wilhelmi, J.; Braegelmann, C. Single-center clinico-pathological case study of 19 patients with cutaneous adverse reactions following COVID-19 vaccines. Dermatopathology 2021, 8, 463–476. [Google Scholar] [CrossRef] [PubMed]
- Holmes, G.A.; Desai, M.; Limone, B.; Love, J.; Tawfik, M.; Wong, L.; Furukawa, B. A case series of cutaneous COVID-19 vaccine reactions at Loma Linda University Department of Dermatology. JAAD Case Rep. 2021, 16, 53–57. [Google Scholar] [CrossRef]
- CDC COVID-19 Response Team; Food and Drug Administration. Allergic reactions including anaphylaxis after receipt of the first dose of Moderna COVID-19 vaccine—United States, December 21, 2020–January 10, 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Peigottu, M.F.; Ferreli, C.; Atzori, M.G.; Atzori, L. Skin adverse reactions to novel messenger RNA Coronavirus vaccination: A case series. Diseases 2021, 9, 58. [Google Scholar] [CrossRef] [PubMed]
- Annabi, E.; Dupin, N.; Sohier, P.; Garel, B.; Franck, N.; Aractingi, S.; Guégan, S.; Oulès, B. Rare cutaneous adverse effects of COVID-19 vaccines: A case series and review of the literature. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e847–e850. [Google Scholar] [CrossRef] [PubMed]
- Ackerman, M.; Henry, D.; Finon, A.; Binois, R.; Esteve, E. Persistent maculopapular rash after the first dose of Pfizer-BioNTech COVID-19 vaccine. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e423–e425. [Google Scholar] [CrossRef] [PubMed]
- Jedlowski, P.M.; Jedlowski, M.F. Morbilliform rash after administration of Pfizer-BioNTech COVID-19 mRNA vaccine. Dermatol. Online J. 2021, 27, 20. [Google Scholar] [CrossRef]
- Fathy, R.A.; McMahon, D.E.; Lee, C.; Chamberlin, G.C.; Rosenbach, M.; Lipoff, J.B.; Tyagi, A.; Desai, S.R.; French, L.E.; Lim, H.W.; et al. Varicella zoster and herpes simplex virus reactivation post-COVID-19 vaccination: A review of 40 cases in an international dermatology registry. J. Eur. Acad. Dermatol. Venereol. 2021. epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Cotter, D.; Basa, J.; Greenberg, H.L. 20 post-COVID-19 vaccine-related shingles cases seen at the Las Vegas Dermatology clinic and sent to us via social media. J. Cosmet. Dermatol. 2021, 20, 1960–1964. [Google Scholar] [CrossRef]
- Psichogiou, M.; Samarkos, M.; Mikos, N.; Hatzakis, A. Reactivation of varicella zoster virus after vaccination for SARS-CoV-2. Vaccines 2021, 9, 572. [Google Scholar] [CrossRef]
- Rodríguez-Jiménez, P.; Chicharro, P.; Cabrera, L.M.; Seguí, M.; Morales-Caballero, Á.; Llamas-Velasco, M.; Sánchez-Pérez, J. Varicella-zoster virus reactivation after SARS-CoV-2 BNT162b2 mRNA vaccination: Report of 5 cases. JAAD Case Rep. 2021, 12, 58–59. [Google Scholar] [CrossRef] [PubMed]
- Furer, V.; Zisman, D.; Kibari, A.; Rimar, D.; Paran, Y.; Elkayam, O. Herpes zoster following BNT162b2 mRNA COVID-19 vaccination in patients with autoimmune inflammatory rheumatic diseases: A case series. Rheumatology 2021, 60, SI90–SI95. [Google Scholar] [CrossRef] [PubMed]
- Chiu, H.H.; Wei, K.C.; Chen, A.; Wang, W.H. Herpes zoster following COVID-19 vaccine: A report of three cases. QJM Int. J. Med. 2021, 114, 531–532. [Google Scholar] [CrossRef] [PubMed]
- Alpalhão, M.; Filipe, P. Herpes zoster following SARS-CoV-2 vaccination—A series of four cases. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e750–e752. [Google Scholar] [CrossRef] [PubMed]
- van Dam, C.S.; Lede, I.; Schaar, J.; Al-Dulaimy, M.; Rösken, R.; Smits, M. Herpes zoster after COVID vaccination. Int. J. Infect. Dis. 2021, 111, 169–171. [Google Scholar] [CrossRef] [PubMed]
- Santovito, L.S.; Pinna, G. A case of reactivation of varicella-zoster virus after BNT162b2 vaccine second dose? Inflamm. Res. 2021, 70, 935–937. [Google Scholar] [CrossRef]
- David, E.; Landriscina, A. Herpes zoster following COVID-19 vaccination. J. Drugs Dermatol. 2021, 20, 898–900. [Google Scholar] [CrossRef]
- Temiz, S.A.; Abdelmaksoud, A.; Dursun, R.; Durmaz, K.; Sadoughifar, R.; Hasan, A. Pityriasis rosea following SARS-CoV-2 vaccination: A case series. J. Cosmet. Dermatol. 2021, 20, 3080–3084. [Google Scholar] [CrossRef]
- Cyrenne, B.M.; Al-Mohammedi, F.; DeKoven, J.G.; Alhusayen, R. Pityriasis rosea-like eruptions following vaccination with BNT162b2 mRNA COVID-19 Vaccine. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e546–e548. [Google Scholar] [CrossRef] [PubMed]
- Cohen, O.G.; Clark, A.K.; Milbar, H.; Tarlow, M. Pityriasis rosea after administration of Pfizer-BioNTech COVID-19 vaccine. Hum. Vaccines Immunother. 2021, 17, 4097–4098. [Google Scholar] [CrossRef] [PubMed]
- Adya, K.A.; Inamadar, A.C.; Albadri, W. Post COVID-19 vaccination papulovesicular pityriasis rosea-like eruption in a young male. Dermatol. Ther. 2021, 34, e15040. [Google Scholar] [CrossRef]
- Dormann, H.; Grummt, S.; Karg, M. Pityriasis rosea as a possible complication of vaccination against COVID-19. Dtsch. Arztebl. Int. 2021, 118, 431. [Google Scholar] [CrossRef] [PubMed]
- Busto-Leis, J.; Servera-Negre, G.; Mayor-Ibarguren, A.; Sendagorta-Cudós, E.; Feito-Rodríguez, M.; Nuño-González, A.; Montero-Vega, M.D.; Herranz-Pinto, P. Pityriasis rosea, COVID-19 and vaccination: New keys to understand an old acquaintance. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e489–e491. [Google Scholar] [CrossRef] [PubMed]
- Carballido Vázquez, A.M.; Morgado, B. Pityriasis rosea-like eruption after Pfizer-BioNTech COVID-19 vaccination. Br. J. Dermatol. 2021, 185, e34. [Google Scholar] [CrossRef] [PubMed]
- Leerunyakul, K.; Pakornphadungsit, K.; Suchonwanit, P. Case report: Pityriasis rosea-like eruption following COVID-19 vaccination. Front. Med. 2021, 8, 752443. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, L.; Hasbani, D.; Kurban, M.; Abbas, O. Pityriasis rosea after mRNA COVID-19 vaccination. Int. J. Dermatol. 2021, 60, 1150–1151. [Google Scholar] [CrossRef]
- Bostan, E.; Jarbou, A. Atypical pityriasis rosea associated with mRNA COVID-19 vaccine. J. Med. Virol. 2021. epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Larson, V.; Seidenberg, R.; Caplan, A.; Brinster, N.K.; Meehan, S.A.; Kim, R.H. Clinical and histopathological spectrum of delayed adverse cutaneous reactions following COVID-19 vaccination. J. Cutan. Pathol. 2021. epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Mazzatenta, C.; Piccolo, V.; Pace, G.; Romano, I.; Argenziano, G.; Bassi, A. Purpuric lesions on the eyelids developed after BNT162b2 mRNA COVID-19 vaccine: Another piece of SARS-CoV-2 skin puzzle? J. Eur. Acad. Dermatol. Venereol. 2021, 35, e543–e545. [Google Scholar] [CrossRef] [PubMed]
- Lopez, S.; Vakharia, P.; Vandergriff, T.; Freeman, E.E.; Vasquez, R. Pernio after COVID-19 vaccination. Br. J. Dermatol. 2021, 185, 445–447. [Google Scholar] [CrossRef] [PubMed]
- Kha, C.; Itkin, A. New-onset chilblains in close temporal association to mRNA-1273 (Moderna) vaccination. JAAD Case Rep. 2021, 12, 12–14. [Google Scholar] [CrossRef] [PubMed]
- Qiao, J.W.; Dan, Y.; Wolf, M.E.; Zoccoli, C.M.; Demetriou, T.J.; Lennon, R.P. Post-vaccination COVID toes (chilblains) exacerbated by rituximab infusion suggests interferon activation as mechanism. Mil. Med. 2021. epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Cazzato, G.; Romita, P.; Foti, C.; Cimmino, A.; Colagrande, A.; Arezzo, F.; Sablone, S.; Barile, A.; Lettini, T.; Resta, L.; et al. Purpuric skin rash in a patient undergoing Pfizer-BioNTech COVID-19 vaccination: Histological evaluation and perspectives. Vaccines 2021, 9, 760. [Google Scholar] [CrossRef]
- Irvine, N.J.; Wiles, B.L. Petechiae and desquamation of fingers following immunization with BTN162b2 messenger RNA (mRNA) COVID-19 vaccine. Cureus 2021, 13, e16858. [Google Scholar] [CrossRef] [PubMed]
- Munavalli, G.G.; Guthridge, R.; Knutsen-Larson, S.; Brodsky, A.; Matthew, E.; Landau, M. COVID-19/SARS-CoV-2 virus spike protein-related delayed inflammatory reaction to hyaluronic acid dermal fillers: A challenging clinical conundrum in diagnosis and treatment. Arch. Dermatol. Res. 2021, 314, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Munavalli, G.G.; Knutsen-Larson, S.; Lupo, M.P.; Geronemus, R.G. Oral angiotensin-converting enzyme inhibitors for treatment of delayed inflammatory reaction to dermal hyaluronic acid fillers following COVID-19 vaccination-a model for inhibition of angiotensin II-induced cutaneous inflammation. JAAD Case Rep. 2021, 10, 63–68. [Google Scholar] [CrossRef]
- Michon, A. Hyaluronic acid soft tissue filler delayed inflammatory reaction following COVID-19 vaccination—A case report. J. Cosmet. Dermatol. 2021, 20, 2684–2690. [Google Scholar] [CrossRef]
- Coto-Segura, P.; Fernández-Prada, M.; Mir-Bonafé, M.; García-García, B.; González-Iglesias, I.; Alonso-Penanes, P.; González-Guerrero, M.; Gutiérrez-Palacios, A.; Miranda-Martínez, E.; Martinón-Torres, F. Vesiculobullous skin reactions induced by COVID-19 mRNA vaccine: Report of four cases and review of the literature. Clin. Exp. Dermatol. 2021. epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Leasure, A.C.; Cowper, S.E.; McNiff, J.; Cohen, J.M. Generalized eczematous reactions to the Pfizer-BioNTech COVID-19 vaccine. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e716–e717. [Google Scholar] [CrossRef]
- Gambichler, T.; Scholl, L.; Dickel, H.; Ocker, L.; Stranzenbach, R. Prompt onset of Rowell’s syndrome following the first BNT162b2 SARS-CoV-2 vaccination. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e415–e416. [Google Scholar] [CrossRef] [PubMed]
- Lavery, M.J.; Nawimana, S.; Parslew, R.; Stewart, L. A flare of pre-existing erythema multiforme following BNT162b2 (Pfizer-BioNTech) COVID-19 vaccine. Clin. Exp. Dermatol. 2021, 46, 1325–1327. [Google Scholar] [CrossRef]
- Soyfer, V.; Gutfeld, O.; Shamai, S.; Schlocker, A.; Merimsky, O. COVID-19 Vaccine-induced radiation recall phenomenon. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 957–961. [Google Scholar] [CrossRef] [PubMed]
- Lim, P.N.; Wylie, G. Symmetrical drug-related intertriginous and flexural exanthema like eruption associated with COVID-19 vaccination. Clin. Exp. Dermatol. 2021. epub ahead of print. [Google Scholar] [CrossRef]
- Dash, S.; Sirka, C.S.; Mishra, S.; Viswan, P. COVID-19 vaccine induced Steven-Johnson syndrome: A case report. Clin. Exp. Dermatol. 2021. epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Elboraey, M.O.; Essa, E. Stevens-Johnson syndrome post second dose of Pfizer COVID-19 vaccine: A case report. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 132, e139–e142. [Google Scholar] [CrossRef]
- Bakir, M.; Almeshal, H.; Alturki, R.; Obaid, S.; Almazroo, A. Toxic epidermal necrolysis post COVID-19 vaccination—First reported case. Cureus 2021, 13, e17215. [Google Scholar] [CrossRef] [PubMed]
- Majid, I.; Mearaj, S. Sweet syndrome after Oxford-AstraZeneca COVID-19 vaccine (AZD1222) in an elderly female. Dermatol. Ther. 2021. epub ahead of print. [Google Scholar] [CrossRef]
- Torrealba-Acosta, G.; Martin, J.C.; Huttenbach, Y.; Garcia, C.R.; Sohail, M.R.; Agarwal, S.K.; Wasko, C.; Bershad, E.M.; Hirzallah, M.I. Acute encephalitis, myoclonus and Sweet syndrome after mRNA-1273 vaccine. BMJ Case Rep. 2021, 14, e243173. [Google Scholar] [CrossRef]
- Kaminetsky, J.; Rudikoff, D. New-onset vitiligo following mRNA-1273 (Moderna) COVID-19 vaccination. Clin. Case Rep. 2021, 9, e04865. [Google Scholar] [CrossRef] [PubMed]
- Sandhu, S.; Bhatnagar, A.; Kumar, H.; Dixit, P.K.; Paliwal, G.; Suhag, D.K.; Patil, C.; Mitra, D. Leukocytoclastic vasculitis as a cutaneous manifestation of ChAdOx1 nCoV-19 corona virus vaccine (recombinant). Dermatol. Ther. 2021, 34, e15141. [Google Scholar] [CrossRef]
- Mücke, V.T.; Knop, V.; Mücke, M.M.; Ochsendorf, F.; Zeuzem, S. First description of immune complex vasculitis after COVID-19 vaccination with BNT162b2: A case report. BMC Infect. Dis. 2021, 21, 958. [Google Scholar] [CrossRef]
- Hunjan, M.K.; Roberts, C.; Karim, S.; Hague, J. Pityriasis rubra pilaris-like eruption following administration of the BNT163b2 (Pfizer-BioNTech) mRNA COVID-19 vaccine. Clin. Exp. Dermatol. 2021. epub ahead of print. [Google Scholar] [CrossRef]
- Merrill, E.D.; Kashem, S.W.; Amerson, E.H.; Pincus, L.B.; Lang, U.E.; Shinkai, K.; Chang, A.Y. Association of facial pustular neutrophilic eruption with messenger RNA-1273 SARS-CoV-2 vaccine. JAMA Dermatol. 2021, 157, 1128–1130. [Google Scholar] [CrossRef]
- Lopatynsky-Reyes, E.Z.; Acosta-Lazo, H.; Ulloa-Gutierrez, R.; Ávila-Aguero, M.L.; Chacon-Cruz, E. BCG scar local skin inflammation as a novel reaction following mRNA COVID-19 vaccines in two international healthcare workers. Cureus 2021, 13, e14453. [Google Scholar] [CrossRef]
- Bostan, E.; Elmas, L.; Yel, B.; Yalici-Armagan, B. Exacerbation of plaque psoriasis after inactivated and BNT162b2 mRNA COVID-19 vaccines: A report of two cases. Dermatol. Ther. 2021. epub ahead of print. [Google Scholar] [CrossRef]
- Krajewski, P.K.; Matusiak, L.; Szepietowski, J.C. Psoriasis flare-up associated with second dose of Pfizer-BioNTech BNT16B2b2 COVID-19 mRNA vaccine. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e632–e634. [Google Scholar] [CrossRef]
- Perna, D.; Jones, J.; Schadt, C.R. Acute generalized pustular psoriasis exacerbated by the COVID-19 vaccine. JAAD Case Rep. 2021, 17, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, M.; Schorno, P.; Hunger, R.E.; Heidemeyer, K.; Feldmeyer, L.; Yawalkar, N. New onset of mainly guttate psoriasis after COVID-19 vaccination: A case report. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e752–e755. [Google Scholar] [CrossRef] [PubMed]
- Quattrini, L.; Verardi, L.; Caldarola, G.; Peluso, G.; De Simone, C.; D’Agostino, M. New onset of remitting seronegative symmetrical synovitis with. pitting oedema and palmoplantar psoriasis flare-up after SARS-CoV-2 vaccination. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e727–e729. [Google Scholar] [CrossRef] [PubMed]
- Joseph, A.K.; Chong, B.F. Subacute cutaneous lupus erythematosus flare triggered by COVID-19 vaccine. Dermatol. Ther. 2021, 34, e15114. [Google Scholar] [CrossRef]
- Elbaek, M.V.; Vinding, G.R.; Jemec, G.B.E. Darier’s disease flare following COVID-19 vaccine. Case Rep. Dermatol. 2021, 13, 432–436. [Google Scholar] [CrossRef] [PubMed]
- Hiltun, I.; Sarriugarte, J.; Martínez-de-Espronceda, I.; Garcés, A.; Llanos, C.; Vives, R.; Yanguas, J.I. Lichen planus arising after COVID-19 vaccination. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e414–e415. [Google Scholar] [CrossRef] [PubMed]
- Risma, K.A.; Edwards, K.M.; Hummell, D.S.; Little, F.F.; Norton, A.E.; Stallings, A.; Wood, R.A.; Milner, J.D. Potential mechanisms of anaphylaxis to COVID-19 mRNA vaccines. J. Allergy Clin. Immunol. 2021, 147, 2075–2082.e2. [Google Scholar] [CrossRef] [PubMed]
- Ohsawa, R.; Sano, H.; Ikeda, M.; Sano, S. Clinical and histopathological views of morbilliform rash after COVID-19 mRNA vaccination mimic those in SARS-CoV-2 virus infection-associated cutaneous manifestations. J. Dermatol. Sci. 2021, 103, 124–127. [Google Scholar] [CrossRef] [PubMed]
- Afacan, E.; Ogut, B.; Ustun, P.; Şentürk, E.; Yazıcı, O.; Adışen, E. Radiation recall dermatitis triggered by inactivated COVID-19 vaccine. Clin. Exp. Dermatol. 2021. epub ahead of print. [Google Scholar] [CrossRef]
- Mungmunpuntipantip, R.; Wiwanitkit, V. COVID-19 vaccination and exanthema like eruption. Clin. Exp. Dermatol. 2021. epub ahead of print. [Google Scholar] [CrossRef]
- McMahon, D.E.; Kovarik, C.L.; Damsky, W.; Rosenbach, M.; Lipoff, J.B.; Tyagi, A.; Chamberlin, G.; Fathy, R.; Nazarian, R.M.; Desai, S.R.; et al. Clinical and pathologic correlation of cutaneous COVID-19 vaccine reactions including V-REPP: A registry-based study. J. Am. Acad. Dermatol. 2021. epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- ASDS Provides Guidance Regarding SARS-CoV-2 mRNA Vaccine Side Effects. 28 December 2020. Available online: https://www.prweb.com/releases/asds_provides_guidance_regarding_sars_cov_2_mrna_vaccine_side_effects_in_dermal_filler_patients/prweb17636524.htm (accessed on 7 November 2021).
- United States Census Bureau. Your Health Care Is in Women’s Hands. Available online: https://www.census.gov/library/stories/2019/08/your-health-care-in-womens-hands.html (accessed on 15 November 2021).
- Rasmussen, T.H.; Mortz, C.G.; Georgsen, T.K.; Rasmussen, H.M.; Kjaer, H.F.; Bindslev-Jensen, C. Patients with suspected allergic reactions to COVID-19 vaccines can be safely revaccinated after diagnostic work-up. Clin. Transl. Allergy 2021, 11, e12044. [Google Scholar] [CrossRef]
- Blumenthal, K.G.; Robinson, L.B.; Camargo, C.A., Jr.; Shenoy, E.S.; Banerji, A.; Landman, A.B.; Wickner, P. Acute allergic reactions to mRNA COVID-19 vaccines. JAMA 2021, 325, 1562–1565. [Google Scholar] [CrossRef]
- Worm, M.; Bauer, A.; Wedi, B.; Treudler, R.; Pfuetzner, W.; Brockow, K.; Buhl, T.; Zuberbier, T.; Fluhr, J.; Wurpts, G.; et al. Practical recommendations for the allergological risk assessment of the COVID-19 vaccination—A harmonized statement of allergy centers in Germany. Allergol. Sel. 2021, 5, 72–76. [Google Scholar] [CrossRef]
- Liu, X.; Shaw, R.H.; Stuart, A.S.V.; Greenland, M.; Aley, P.K.; Andrews, N.J.; Cameron, J.C.; Charlton, S.; Clutterbuck, E.A.; Collins, A.M.; et al. Safety and immunogenicity of heterologous versus homologous prime-boost schedules with an adenoviral vectored and mRNA COVID-19 vaccine (Com-COV): A single-blind, randomised, non-inferiority trial. Lancet 2021, 398, 856–869. [Google Scholar] [CrossRef]
- Lim, R.K.; Kalagara, S.; Chen, K.K.; Mylonakis, E.; Kroumpouzos, G. Dermatology in a multidisciplinary approach with infectious disease and obstetric medicine against COVID-19. Int. J. Womens Dermatol. 2021. epub ahead of print. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Article Reference; Patient Region | Study Design | Rating Score * | Vaccine (Number of Persons); Sex | Cutaneous Reaction | Total Reactions | Reactions to Dose 1 | Reactions to Dose 2 | Time to Onset after Vaccination (Median) | Time to Resolution (Median) | Intervention |
|---|---|---|---|---|---|---|---|---|---|---|
| Local site injection reaction | ||||||||||
| McMahon; USA [1] | Registry-based study | 3 3 | mRNA-1273 (343), BNT16b2 (71); 40 M: 374 F | DLLR local injection site reaction | 218 (206 mRNA-1273) 232 (186 mRNA-1273) | 180 (175 mRNA-1273) 151 (143 mRNA-1273) | 38 (30 mRNA-1273); 11 recurrent (mRNA-1273) 81 (71 mRNA-1273); 21 recurrent (20 mRNA-1273) | Dose 1: 7 d Dose 2: 2 d Dose 1: 1 d Dose 2: 1 d | Dose 1: 4 d Dose 2: 3 d Dose 1: 4 d Dose 2: 3 d | TCS, OAH, analgesics, ice, antibiotics |
| Català; Spain [2] | Cross-sectional national study | 3 | BNT16b2 (163), mRNA-1273 (147), AZD1222 (95); 80 M: 325 F | DLLR | 130 (91 mRNA-1273, 23 BNT16b2, 16 AZD1222) | 85 | 45 | 4.9 d (mean) | 7.4 d (mean) | 93 rashes: topical/ systemic CS, OAH, paracetamol, NSAIDS, oral antibiotics |
| Fernandez-Nieto; Spain [7] | Retrospective study | 3 | BNT16b2 (103); 12 M: 91 F | DLLR | 103 | 49 | 54; 16 recurrent | NR | <8 h: 23; 8–24 h: 27; 48–72 h: 38; >72 h: 14 | NR |
| Guerrero; Spain [8] | Case series | 4 | mRNA-1273 (13), BNT16b2 (1); 14 F | DLLR | 22 | 13 (12 mRNA-1273) | 9 (mRNA-1273); 8 recurrent | Dose 1: 6 d Dose 2: 1 d | Dose 1: 5 d Dose 2: 3 d | TCS (3 patients), OAH (1 patient) |
| Blumenthal; USA [9] | Case series | 4 | mRNA-1273 (12); 2 M: 10 F | DLLR | 20 | 12 | 8; recurrent | Dose 1: 8 d Dose 2: 2 d | Dose 1: 6 d Dose 2: 2.5 d | Ice packs, TCS/OCS, OAH, antibiotics |
| Johnston; USA [10] | Case series | 4 | mRNA-1273 (16); 3 M: 13 F | Delayed localized hypersensitivity reaction | 27 | 15 | 12; 11 recurrent | Dose 1: 7 d Dose 2: 2 d | Dose 1: 5 d Dose 2: 3 d | TCS, OAH, cool compress, cephalexin |
| Jacobson; USA [11] | Case series | 4 | mRNA-1273 (14); 14 F | Delayed injection site reaction | 19 | 13 | 6; 5 recurrent | Dose 1: 7 d Dose 2: 2 d | Dose 1: 4 d Dose 2: 4 d | OAH, low-potency TCS |
| Ramos; USA [12] | Case series | 4 | mRNA-1273 (11), BNT16b2 (1); NR | DLLR | 12 | 11 (mRNA-1273) | 1 (BNT16b2) | 5–11 d (mean, 7 d) | 3–8 d (mean, 5 d) | TCS, OAH, ice, analgesics |
| Hoff; Germany [13] | Case series | 4 | mRNA-1273 (11); 2 M: 9 F | Delayed skin reaction | 11 | 8 | 3 | Dose 1: 7 d Dose 2: 3 d | With Rx: 1–2 d Without Rx: 2–4 d | 4 patients: TCS, OAH |
| Wei; USA [14] | Case series | 4 | mRNA-1273 (4); 4 F | DLLR | 4 | 4 | NR | 7–10 d | 2–4 d | TCS, OAH |
| Shin; Korea [15] | Case series | 4 | AZD1222 (4); 4 F | DLLR | 4 | 4 | NR | 10 d | 4 d | NSAIDS, ice packs, SCS |
| Choi; Singapore [16] | Case series | 5 | BNT16b2 (1); 1 F | Local injection site reaction | 2 | 1 | 1 | Dose 1: 1 d Dose 2: NR | NR | NR |
| Tihy; Switzerland [17] | Case series | 5 | mRNA-1273 (1); 1 F | DLLR | 1 | 0 | 1 | 5 d | <2 wks | NR |
| Urticaria | ||||||||||
| Català; Spain [2] | Cross-sectional national study | 3 | BNT16b2 (163) mRNA-1273 (147) AZD1222 (95); 80 M: 325 | Urticaria and/or angioedema | 59 (15 mRNA-1273, 24 BNT16b2, 20 AZD1222) | 35 | 24 | 4.9 d (mean) | 7.5 d (mean) | OAH, TCS, SCS, antibiotics, paracetamol, NSAIDS, epinephrine injection (1 case) |
| McMahon; USA [1] | Registry-based study | 3 | mRNA-1273 (343), BNT16b2 (71); 40 M: 374 F | Urticaria | 40 (23 mRNA-1273) | 25 | 15; 4 recurrent (3 mRNA-1273) | Dose 1: 3 d Dose 2: 2 d | Dose 1: 5 d Dose 2: 3 d | TCS, OAH, analgesics, antibiotics |
| Team CC-R, FDA; USA [18] | Registry-based study | 3 | BNT16b2 (10); 1 M: 9 F | Generalized urticaria, anaphylaxis | 10 | 10 | NR | 5–54 min | NR | Epinephrine injection |
| Sidlow; USA [19] | Case series | 4 | mRNA-1273 (6); 1 M: 5 F | Urticarial dermatitis | 6 | 5 | 1; recurrent | ≤3 d | ≤17 d | OAH |
| Kelso; USA [20] | Case series | 5 | mRNA-1273 (1); 1 F | Urticaria | 1 | 1 | No dose 2 | 6 min | NR | OCS, OAH, epinephrine injection |
| Yu; Philippines [21] | Case series | 4 | AZD1222 (3); 3 F | Angioedema (2), urticaria (1) | 3 | 3 | NR | Angioedema: 3 h, 3 d Urticaria: 15 min | Angioedema: 3 d, 4 d Urticaria: 14 d | OAH, OCS, epinephrine (angioedema case), TCS, i.m. diphenhydramine, |
| Corbeddu; Italy [22] | Case series | 4 | BNT16b2 (2); 2 M | Urticaria | 2 | 2 | 0 | 1 h, 2 d | 2–3 d | None |
| Choi; Singapore [16] | Case series | 4 | BNT16b2 (2); 2 F | Urticaria | 2 | 2 | 0 | Dose 1: 17 d, a few d | Dose 1: 2 wks, 6 wks | OAH |
| Niebel; Germany [23] | Case series | 4 | BNT16b2 (1), AZD1222 (1); 2 F | Urticaria, generalized hives | 2 | 2 | 0 | 1 d, 2 d | NR | OAH |
| Holmes; USA [24] | Case series | 5 | mRNA-1273 (1); 1 F | Urticaria, angioedema | 1 | 1 | No dose 2 | ≤2 d | 3 d | OAH, baking soda baths |
| Tihy; Switzerland [17] | Case report | 5 | BNT16b2 (1); 1 M | Urticarial plaques and papules | 1 | 0 | 1 | 21 d | >24 h | NR |
| Team CC-R, FDA; USA [25] | Registry-based study | 5 | mRNA-1273 (1); 1 F | Generalized urticarial rash, anaphylaxis | 1 | 1 | NR | 11 min | NR | Epinephrine injection |
| Morbiliform/diffuse erythematous eruption | ||||||||||
| Català; Spain [2] | Cross-sectional national study | 3 | BNT16b2 (163), mRNA-1273 (147), AZD1222 (95); 80 M: 325 F | Morbilliform rash | 36 (6 mRNA-1273, 19 BNT16b2, 11 AZD1222) | 25 | 11 | 4 d (mean) | 10.3 d (mean) | OAH, TCS, OCS |
| McMahon; USA [1] | Registry-based study | 3 | mRNA-1273 (343), BNT16b2 (71); 40 M: 374 F | Morbilliform rash | 27 (18 mRNA-1273) | 6 BNT16b2 11 mRNA-1273 | 3 BNT16b2 7 mRNA-1273 | Dose 1: 3 d Dose 2: 2 d | Dose 1: 4.5 d Dose 2: 2.5 d | TCS, OAH, analgesics, antibiotics |
| Team CC-R, FDA; USA [18] | Registry-based study | 4 | BNT16b2 (7); 1 M: 6 F | Diffuse erythematous rash, anaphylaxis | 7 | 7 | NR | 2–25 min | NR | Epinephrine injection |
| Tihy; Switzerland [17] | Case series | 4 | BNT16b2 (4), mRNA-1273 (2); 3 M: 3 F | Morbilliform rash (1); erythematous rash (5) | 6 (4 BNT16b2) | 1 (BNT16b2) | 5 (3 BNT16b2) | Dose 1: 8 d Dose 2: 13 d (range, 2–16 d) | ≤2 wks | |
| Team CC-R, FDA; USA [25] | Registry-based study | 4 | mRNA-1273 (4); 4 F | Diffuse erythematous rash, anaphylaxis | 4 | 4 | NR | 5–45 min | NR | Epinephrine injection |
| Peigottu; Italy [26] | Case series | 4 | BNT16b2 (5); 1 M: 4 F | Maculopapular rash | 5 | 1 | 4 | Dose 1: 24 h Dose 2: 28 h | NR | OAH ± short course OCS |
| Corbeddu; Italy [22] | Case series | 4 | BNT16b2 (3); 1 M: 2 F | Morbilliform rash | 3 | 0 | 3 | 5 h, 48 h, 3 d | 2–3 d | None |
| Annabi; France [27] | Case series | 4 | BNT16b2 (2); 2 F | Morbilliform rash | 2 | 2 | 0 | 7 d, 8 d | 8 d, 15 d | Case 1: none Case 2: TCS |
| Holmes; USA [24] | Case report | 5 | mRNA-1273 (1); 1 F | Morbilliform rash | 1 | 0 | 1 | 1 d | ≤23 d | OCS, OAH, TCS |
| Ackerman; France [28] | Case report | 5 | BNT16b2 (1); 1 M | Maculopapular rash | 1 | 1 | No dose 2 | 3 h | 1 mo | TCS |
| Jedlowski; USA [29] | Case report | 5 | BNT16b2 (1); 1 M | Morbilliform rash | 2 | 1 | 1; recurrent | 48 h | 24 h | None |
| Niebel; Germany [23] | Case series | 5 | BNT16b2 (1); 1 F | Generalized erythematous plaques | 1 | 1 | No dose 2 | 10 d | NR | Prednisolone |
| VZV/HSV reactivation | ||||||||||
| Fathy; USA [30] | Registry-based study | 3 | mRNA-1273 (17), BNT16b2 (23); 12 M: 28 F | Zoster, HSV reactivation | 35 zoster (19 BNT16b2), 5 HSV (4 BNT16b2) | 27 zoster, 4 HSV | 8 zoster, 1 HSV | VZV: 7 d HSV: 13 d | VZV: 7 d HSV: 7 d | Systemic antiviral; VZV cases also gabapentin, acetaminophen, TCS |
| Català; Spain [2] | Cross-sectional national study | 3 | BNT16b2 (163) mRNA-1273 (147) AZD1222 (95); 80 M: 325 F | Zoster, HSV reactivation | 41 zoster (28 BNT16b2, 6 mRNA-1273, 7 AZD1222); 15 HSV (5 BNT16b2, 4 mRNA-1273, 6 AZD1222) | 35 (VZV 26) | 21 (VZV 15) | VZV: 6.9 d (mean) HSV: 4.6 d (mean) | VZV: 12.1 d (mean) HSV: 9.3 d (mean) | Systemic antiviral; some VZV patients also NSAIDS, topical antibiotics, paracetamol, OAH |
| McMahon; USA [1] | Registry-based study | 4 | mRNA-1273 (343), BNT16b2 (71); 40 M: 374 F | Zoster | 10 (5 BNT16b2) | 6 (5 mRNA-1273) | 4 (BNT16b2) | Dose 1: 15 d Dose 2: 10 d | Dose 1: 6 d Dose 2: 8 d | NR |
| Lee; USA [31] | Case series | 4 | mRNA-1273 (14), BNT16b2 (6); 10 M: 10 F | Zoster | 20 (14 mRNA-1273, 6 BNT16b2) | 15 (12 mRNA-1273) | 5 (3 BNT16b2) | Dose 1: 5 d (range, 3–21 d) Dose 2: 5 d (range, 3–38 d) | NR | Valacyclovir, gabapentin (8 patients), topical lidocaine 4% (5 cases), OCS, tramadol, TCS, Terrasil shingles cream |
| Psichogiou; Greece [32] | Case series | 4 | BNT16b2 (7); 4 M: 3 F | Zoster, zoster opthalmicus (1 case) | 7 | 5 | 2 | 8 d (range, 7–20 d) | 10 d post-oral Rx (6 cases) | Valacyclovir (6 patients); hospitalization and iv valacyclovir followed by oral (1 case) |
| Furer; Israel [33] | Case series | 4 | BNT16b2 (6); 6 F | Zoster; zoster opthalmicus (1 case) | 6 | 5 | 1 | 2.5 d (range, 2–10 d) | 4.5 wks (range, 1.5–6 wks) | Acyclovir (2 patients), valacyclovir (2 patients) |
| Rodríguez-Jiménez; Spain [34] | Case series | 4 | BNT16b2 (5); 2 M: 3 F | Zoster | 5 | 3 | 2 | 3 d (range, 1–16 d) | NR | NR |
| Chiu; Taiwan [35] | Case series | 4 | mRNA-1273 (1) AZD1222 (2); 3 M | Zoster | 3 | 3 | 0 | 2 d (mRNA-1273); 2 d, 7 d (AZD1222) | 1 wk post-oral Rx | Acyclovir |
| Alpalhão; Portugal [36] | Case series | 4 | BNT16b2 (2) AZD1222 (2); 1 M: 3 F | Zoster | 4 | 4 | 0 (dose 2 in 2 patients) | 3.5 d (range, 3–6 d) | NR | Valacyclovir |
| Van Dam; Netherlands [37] | Case series | 4 | BNT16b2 (2); 1 M: 1 F | Zoster | 2 | 2 | 0 | Case 1: 15 d Case 2: 13 d | Case 1: 2 wks Case 2: 10 d | Case 1: no Rx Case 2: valacyclovir |
| Santovito; Switzerland [38] | Case report | 5 | BNT16b2 (1); 1 M | Zoster | 1 | 0 | 1 | 3 d | 30 d (Rx started at 72 h) | Prednisone, hydroxyzine, and 2% mupirocin ineffective |
| David; USA [39] | Case report | 5 | mRNA-1273 (1); 1 F | Zoster | 1 | 1 | NR | 2–3 d | NR | None |
| Pityriasis rosea-like eruption | ||||||||||
| Temiz; Turkey [40] | Case series | 4 | BNT16b2 (14); 4 M: 10 F | Pityriasis rosea-like rash | 14 | 10 BNT16b2 | 4 BNT16b2 | Dose 1: 14 d (range, 5–21 d) Dose 2: 9 d (range, 4–13 d) | Dose 1: 8.5 wks (range, 6–12 wks) Dose 2: 4 wks (range, 3–6 wks) | Topical CS, OAH |
| Català; Spain [2] | Cross-sectional national study | 3 | BNT16b2 (163), mRNA-1273 (147), AZD1222 (95); 80 M: 325 F | Pityriasis rosea-like rash | 20 (5 mRNA-1273, 11 BNT16b2, 4 AZD1222) | 12 | 8 | 6.3 d (mean) | 25.2 (mean) | 13 patients treated with TCS, OCS, OAH, analgesics |
| McMahon; USA [1] | Registry-based study | 4 | mRNA-1273 (343), BNT16b2 (71); 40 M: 374 F | Pityriasis rosea-like rash | 4 (3 BNT16b2) | 3 (2 BNT16b2) | 1; recurrent (BNT16b2) | Dose 1: 14 d Dose 2: 4 d | Dose 1: 10 d Dose 2: 5 d | NR |
| Niebel; Germany [23] | Case series | 4 | BNT16b2 (1), AZD1222 (1); 1 M: 1 F | Pityriasis rosea-like rash | 2 | 1 (AZD1222) | 1 (BNT16b2) | Dose 1: 8 d Dose 2: 22 d | NR | TCS, emollients |
| Cyrenne; Canada [41] | Case series | 4 | BNT16b2 (2), 1 M: 1 F | Pityriasis rosea-like rash | 3 | 1 | 2 (1 recurrent) | Dose 1: 2 d Dose 2: 3 wks | Dose 1: 2 wks Dose 2: 3 wks | TCS, doxycycline, OAH |
| Choi, Singapore [16]; Tihy, Switzerland [17]; Yu; Philippines [21]; Cohen; USA [42]; Adya; India [43]; Dormann; Germany [44]; Busto-Leis; Spain [45]; Carbadillo Vazquez; Portugal [46]; Leerunyakal; Thailand [47]; Abdullah; Lebanon [48]; Bostan; Turkey [49]; Larson, USA [50] | Case reports/series | 4 [45], 5 | BNT16b2 (8), mRNA-1273 (1), AZD1222 (4); 5 M: 8 F | Pityriasis rosea-like rash | 14 (9 BNT16b2, 4 AZD1222, 1 mRNA-1273) | 8 (3 BNT16b2, 4 AZD1222, 1 mRNA-1273) | 6 (BNT16b2); 1 recurrent | Dose 1: 4 d (range, 4–14 d) Dose 2: 7 d (range, 1–15 d) | 1–4 wks | TCS, OAH, symptomatic Rx |
| Pernio, chilblains and purpuric reactions | ||||||||||
| Català; Spain [2] | Cross-sectional national study | 3 | BNT16b2 (163), mRNA-1273 (147), AZD1222 (95); 80 M: 325 F | Purpuric rash | 16 (9 AZD1222, 7 BNT16b2) | 11 | 5 | 7.6 d | 15.7 d | 8 patients treated: TCS, OCS, OAH, paracetamol |
| McMahon; USA [1] | Registry-based study | 4 | mRNA-1273 (343), BNT16b2 (71); 40 M: 374 F | Pernio/chilblains, petechiae | 8 pernio/chilblains (5 BNT16b2), 4 petechiae (3 mRNA-1273) | 6 pernio/chilblains (3 BNT16b2), 2 petechiae (1 mRNA-1273) | 2 pernio/chilblains (BNT16b2), 2 petechiae (1 mRNA-1273) | Dose 1: 10 d (pernio/chilblains), 2 d (patechaie) Dose 2: 11 d (pernio/chilblains), 1 d (petechiae) | Dose 1: 10.5 d (pernio/chilblains), 4.5 d (petechiae) Dose 2: 4.5 d (pernio/chilblains), 3 d (petechiae) | NR |
| Mazzatenta; Italy [51] | Case series | 4 | BNT16b2 (3); 1 M: 2 F | Purpuric lesions | 3 | 1 | 2 | Dose 1: 10 d Dose 2: mean of 22 d | Dose 1: 12 d Dose 2: mean of 13 d | Self-resolved |
| Holmes; USA [24] | Case series | 4 | BNT16b2 (1), mRNA-1273 (1); 2 F | Purpuric, reticulated patches (BNT16b2); chilblain-like papules | 2 | 1 (mRNA-1273) | 1 (BNT16b2) | Dose 1: 10 d Dose 2: 5 d | Dose 1: ≤13 d Dose 2: ≤2 wks | Case 1: OCS, TCS, OAH Case 2: OAH, TCS |
| Lopez; USA [52] | Case report | 5 | BNT16b2; 1 M | Pernio | 1 | 0 | 1 | 3 d | 28 d | Clobetasol, avoidance of cold |
| Kha; USA [53] | Case report | 5 | mRNA-1273; 1 F | Chilblains | 1 | 1 | 0 | 2 d | 7 d | Clobetasol |
| Qiao; USA [54] | Case report | 5 | BNT16b2; 1 F | Chilblains | 2 | 1 | 1; worsening | Dose 1: 2 wks Dose 2: h | 21 d | Improved with TCS x 2 wks; then worse with rituximab |
| Annabi; France [27] | Case series | 5 | BNT16b2; 1 M | Chilblains | 1 | 0 | 1 | 5 d | ≤7 d | None |
| Cazzato; Italy [55] | Case report | 5 | BNT16b2; 1 M | Purpuric rash | 1 | 0 | 1 | 15 d | NR | i.v. methylprednisolone |
| Irvine; USA [56] | Case report | 5 | BNT16b2; 1 F | Petechiae, desquamation | 1 | 0 | 1 | 5 d | 3 wks | Monitoring complete blood cell count |
| Niebel; Germany [23] | Case series | 5 | BNT16b2; 1 M | Petechial annular plaques | 1 | 0 | 1 | 2 d | NR | Dapsone, prednisolone |
| DIR to dermal HA filler | ||||||||||
| McMahon; USA [1] | Registry-based study | 4 | mRNA-1273 (343), BNT16b2 (71); 40 M: 374 F | DIR to dermal HA filler | 9 (1 BNT16b2, 8 mRNA-1273) | 3 (mRNA-1273) | 6 (5 mRNA-1273) | NR | NR | NR |
| Munavalli; USA [57] | Case series | 4 | BNT16b2 (1), mRNA-1273 (1); 2 F | DIR to dermal HA filler | 2 | 1 (mRNA-1273) | 1 (BNT16b2) | Dose 1: 12 h Dose 2: 24 h | Dose 1 (mRNA-1273): 48 h (lisinopril at 48 h) Dose 2 (BNT16b2): 24 h | BNT16b2: OCS mRNA-1273: OAH, acetaminophen, lisinopril |
| Munavalli; USA [58] | Case series | 4 | mRNA-1273 (2), BNT16b2 (2); 4 F | DIR to dermal HA filler | 5 (3 mRNA-1273) | 2 (1 BNT16b2) | 3 (2 mRNA-1273); 1 recurrent (mRNA-1273) | Dose 1: 10 d (BNT16b2), 18 h (mRNA-1273) Dose 2: 2 d (BNT16b2), 24h (mRNA-1273) | Dose 1 (BNT16b2): 7 d Dose 2 ((BNT16b2): 4 d (lisinopril started at 72 h) Dose 1 (mRNA-1273): 48 h (lisinopril started at 24 h) Dose 2 (mRNA-1273): 5 d (lisinopril started at 48 h) | Low-dose lisinopril |
| Michon; Canada [59] | Case series | 4 | BNT16b2 (2); 2 F | DIR to dermal HA filler | 2 | 2 | NR | Case 1: 2 d Case 2: a few d | Case 1: 5 d Case 2: hyaluronidase injected at 3 wks | Case 1: no R× Case 2: resolved within 48 h after hyaluronidase injection |
| Unusual reactions | ||||||||||
| Català; Spain [2] | Cross-sectional national study | 3 | BNT16b2 (163), mRNA-1273 (147), AZD1222 (95); 80 M: 325 F | Papulovesicular | 26 (7 mRNA-1273, 11 BNT16b2, 8 AZD1222) | 18 | 8 | 6.4 d (mean) | 19.3 d (mean) | OAH, TCS, SCS, topical antibiotics, paracetamol |
| McMahon; USA [1] | Registry-based study | 4 | mRNA-1273 (343), BNT16b2 (71); 40 M: 374 F | Vesicular | 10 (5 mRNA-1273) | 7 (4 mRNA-1273) | 3 (2 BNT16b2) | Dose 1: 7 d Dose 2: 3 d | Dose 1: 7 d Dose 2: 7 d | NR |
| Niebel; Germany [23] | Case series | 4 | BNT16b2 (2); 2 F | Vesicular | 2 | 0 | 2 | 3 d, 7 d | NR | TCS, topical fusidine |
| Coto-Segura; Spain [60] | Case series | 4 | BNT16b2 (4); 4 M | Bullous pemphigoid (3); linear IgA dermatosis (1) | 4 | 4 | NR | 3–17 d | NR | NR |
| Larson; USA [50] | Case series | 4 | BNT16b2 (1), mRNA-1273 (1); 2 M | New-onset bullous pemphigoid | 2 | 1 (BNT16b2) | 1 | Dose 1: 3 wks Dose 2: 2 wks | NR | Improvement with OCS, TCS, doxycycline, niacinamide, OAH |
| McMahon; USA [1] | Registry-based study | 3 | mRNA-1273 (343), BNT16b2 (71); 40 M: 374 F | Erythromelalgia | 14 (11 mRNA-1273, 3 BNT16b2) | 6 (5 mRNA-1273) | 8 (6 mRNA-1273) | Dose 1: 7 d Dose 2: 1 d | Dose 1: 5.5 d Dose 2: 3 d | NR |
| Leasure; USA [61] | Case series | 4 | BNT16b2 (2); 1 M: 1 F | Generalized eczematous eruption | 4 | 2 | 2; recurrent | Dose 1: 5 d (mean) Dose 2: 9 d (mean) | Several wks | TCS, OAH, OCS |
| Corbeddu; Italy [22] | Case series | 5 | BNT16b2; 1 M | Generalized eczematous eruption | 1 | 1 | NR | 2 d | 2–3 d | OCS |
| Holmes; USA [24] | Case series | 5 | BNT16b2; 1 M | Eczematous dermatitis | 2 | 1 | 1; recurrent | Dose 1: ≤7 d Dose 2: NR | 2–3 wks | TCS, tacrolimus ointment |
| Niebel; Germany [23] | Case series | 4 5 | BNT16b2 (3); 2 M: 1 F BNT16b2; 1 M | Hematogenous contact dermatitis Psoriasiform flare of atopic dermatitis | 3 1 | 2 1 | 1 0 | Dose1: 2 d, 3 d Dose 2: 12 d 21 d | NR NR | TCS; prednisolone and cyclosporine (1 case) Prednisolone, TCS, narrowband UVB |
| McMahon; USA [1] | Registry-based study | 4 | mRNA-1273 (343), BNT16b2 (71); 40 M: 374 F | Erythema multiforme | 3 (mRNA-1273) | 3 | 0 | N/A | N/A | NR |
| Gambichler; Germany [62] Lavery; UK [63] | Case report Case report | 5 5 | BNT16b2; 1 F BNT16b2; 1 F | Erythema multiforme, Rowell syndrome Erythema multiforme flare | 1 2 | 1 1 | NR 1; recurrent | 1 d Dose 1: 12 h Dose 2: 24 h | NR NR | OCS TCS |
| Tihy; Switzerland [17] | Case series | 5 | BNT16b2; 1 F | Prurigo nodularis | 1 | 0 | 1 | 15 d | 2 wks | NR |
| Soyfer; Israel [64] | Case series | 4 | BNT16b2 (2); 2 M | Radiation recall dermatitis | 2 | 0 | 2 | 6 d | ≤7 d | TCS, analgesics |
| Lim; UK [65] | Case report | 5 | AZD1222; 1 M | SDRIFE-like eruption | 1 | NR | 1 | 1 d | 1 mo | OCS, potassium permanganate soaks betamethasone/clotrimazole, |
| Dash; India [66] | Case report | 5 | AZD1222; 1 M | SJS | 1 | 1 | No dose 2 | 3 d | 14 d | Cyclosporine |
| Elboraey; Saudi Arabia [67] Bakir; Saudi Arabia [68] | Case report Case report | 5 5 | BNT16b2; 1 F BNT16b2; 1 F | SJS TEN | 1 1 | 0 1 | 1 NR | 5 d 7 d | NS 22 d post-etanercept | OCS admission, multidisciplinary care, etanercept |
| Majid; India [69] | Case report | 5 | AZD1222; 1 F | Sweet’s syndrome | 1 | 1 | NR | 7 d | 4 wks (betamethasone started at 3 wks) | Injectable betamethasone |
| Torrealba-Acosta; USA [70] | Case report | 5 | mRNA-1273; 1 M | Sweet’s syndrome | 1 | 1 | NR | 1 d | ≥13 d | Oral antibiotics, systemic antivirals, SCS |
| Kaminetsky; USA [71] | Case report | 5 | mRNA-1273; 1 F | Vitiligo | 2 | 1 | 1; worsening | Several days | NR | NR |
| Sandu; India [72] Mücke; Germany [73] Larson; USA [50] | Case series Case report Case series | 4 5 4 | AZD1222; 1 M: 1 F BNT16b2; 1 M BNT16b2 (1), mRNA-1273 (1); 2 F | Vasculitis Vasculitis Vasculitis | 3 1 2 | 2 0 1 (mRNA-1273) | 1; recurrent 1 1 (BNT16b2) | Dose 1: 5 d, 7 d Dose 2: 2 d 12 d Dose 1: day of Dose 2: 7 d | Dose 1: 2 wks, 7 d Dose 2: NR 5 d post-Rx initiation NR | OCS, TCS OCS OAH, SCS, oral antibiotics, dapsone, TCS |
| Annabi; France [27] | Case series | 5 5 | BNT16b2; 1 F mRNA-1273; 1 F | Livedo racemose Fixed drug eruption | 1 1 | 1 0 | 0 1 | 12 d 2 d | PIH at 2 mos 5 d | None TCS |
| Hunjun; UK [74] | Case report | 5 | BNT16b2; 1 M | Pityriasis rubra pilaris-like | 2 | 1 | 1; worsening | Dose 1: 3 d Dose 2: a few d | NR | Acitretin, TCS |
| Merrill; USA [75] | Case series | 4 | mRNA-1273; 2 M | Facial pustular neutrophilic eruption | 2 | 1 | 1 | ≤24 h | ≤7 d, >15 d | Case 1: Cephalexin, TCS Case 2: vancomycin, piperacillin/tazobactam, tacrolimus 0.1%, doxycycline |
| Lopatynsky-Reyes; Costa Rica, Mexico [76] | Case series | 4 | BNT16b2 (1), mRNA-1273 (1); 2 F | BCG scar local skin inflammation | 2 | 0 | 2 | 2 d, 36 h | 4 d, 2 d | None |
| Bostan; Turkey [77] Niebel; Germany [23] Krajewski; Poland [78] | Case report Case series Case report | 5 5 5 | BNT16b2; 1 M BNT16b2; 1 M BNT16b2; 1 M | Psoriasis vulgaris flare Psoriasis vulgaris flare Psoriasis vulgaris flare | 2 1 1 | 1 0 0 | 1; recurrent 1 1 | Dose 1: NS Dose 2: 2 wks 20 d 1 d | NR NR NR | NR Cignoline, TCS, narrowband UVB, tildrakizumab NR |
| Perna; USA [79] | Case report | 5 | BNT16b2; 1 M | Generalized pustular psoriasis | 1 | 1 | NR | 5 d | 12 d (cyclosporine started at 7 d) | Cyclosporine |
| Lehmann; Switzerland [80] | Case report | 5 | BNT16b2; 1 F | New onset guttate psoriasis | 2 | 1 | 1 (recurrent) | Dose 1: 10 d | NS | Clobetasol, ultraviolet light B, betamethasone/calcipotriene |
| Quattrini; Italy [81] | Case report | 5 | BNT16b2; 1 F | Palmoplantar psoriasis flare | 1 | NR | 1 | 48 h | Rapid improvement | OCS, methotrexate |
| Niebel; Germany [23] | Case series | 4 | BNT16b2 (2), mRNA-1273 (2); 1 M: 3 F | CLE (3 cases; 2 with mRNA-1273), CLE flare (BNT16b2; 1 case) | 4 | 3 | 1 (mRNA-1273) | 7 d (range, 5–10 d) | 3 wks post-OCS Rx | Prednisolone; single cases with OAH, hydroxychloroquine, methotrexate, etoricoxib, TCS |
| Joseph; USA [82] | Case report | 5 | mRNA-1273; 1 F | Subacute CLE flare | 2 | 1 | 1; worsening | Dose 1: 4 d | NR | OCS continuation, Mycophenolate mofetil dose increase, TCS |
| Elbaek; Denmark [83] | Case report | 5 | AZD1222; 1 F | Darier’s disease flare | 1 | 1 | No dose 2 | 2 d | >6 wks | TCS, salicylic acid, oral isotretinoin |
| Hiltun; Spain [84] | Case report | 5 | BNT16b2; 1 F | Lichen planus flare | 1 | 0 | 1 | 48 h | NR | TCS |
| Reaction | mRNA-1273 No. (%) a | BNT162b2 No. (%) | ADZ1222 No. (%) | Row Total b |
|---|---|---|---|---|
| Delayed large local reaction (‘COVID arm’) | 411 (72) | 140 (24.5) | 20 (3.5) | 571 (40.4) |
| Local injection site reaction | 186 (79.5) | 48 (20.5) | 0 | 234 (16.5) |
| Urticaria | 47 (36.7) | 57 (44.5) | 24 (18.8) | 128 (9.0) |
| Morbilliform/diffuse erythematous eruption | 31 (33.0) | 53 (55.3) | 11 (11.7) | 95 (6.7) |
| VZV/HSV reactivation | 48 (29.8) | 90 (59.6) | 17 (10.6) | 155 (11.0) c |
| Pityriasis rosea-like eruption | 7 (12.3) | 41 (71.9) | 9 (15.8) | 57 (4.0) |
| Pernio, chilblains, and purpuric eruptions | 7 (17.1) | 25 (61.0) | 9 (22.0) | 41 (2.9) |
| DIR to dermal HA filler | 12 (66.7) | 6 (33.3) | 0 | 18 (1.3) |
| Unusual reactions | 39 (33.6) | 62 (53.4) | 15 (12.9) | 116 (8.2) |
| Column total | 788 (55.7) | 522 (36.9) | 105 (7.4) | 1415 |
| Skin Reaction | Potential Mechanisms |
|---|---|
| Delayed large local reaction | T-cell mediated responses to a vaccine excipient, lipid nanoparticle, or mRNA component [10,11] |
| Urticaria | IgE-mediated reactions are more typically associated with the inactive components of the vaccine (i.e., egg proteins, gelatin, and latex) [85] |
| Anaphylaxis | Pre-existing antibody recognition of the vaccine excipient polyethylene glycol (PEG); contact system activation by nucleic acid; complement recognition of the vaccine-activating allergic effector cells; direct mast cell activation [85] |
| Morbilliform eruption | Immune activation-mediated skin response; prior coronavirus infection may generate a cross-reaction with antigen that mRNA vaccine encodes [86] |
| VZV/HSV reactivation | Innate or cell-mediated immune defense failures initiated by the host in response to mRNA COVID-19 vaccines; [22] strong immune response against the S protein from vaccine may distract the cell-mediated control of another, latent virus [2] |
| Pityriasis rosea-like eruption | Vaccination leads to a state of altered immunity and may lead to endogenous reactivation of HHV-6 or HHV-7 [40]; T-cell mediated response triggered by molecular mimicry from a viral epitope [41] |
| Pernio, chilblains, and purpuric lesions | Vaccine-induced microangiopathy [51]; viral proteins in the endothelial cells of the dermal vessels and accumulation of immune complexes that activate the complement cascade, causing small vessel wall damage [52] |
| DIR to dermal hyaluronic acid fillers | COVID-19 spike protein interacts with ACE2 receptors which trigger pro-inflammatory loco-regional TH1 cascade and promote a CD8 and T cell mediated reaction to incipient granulomas [57,58] |
| Vesiculobullous lesions | Cross-reactions between SARS-CoV-2 spike protein antibody and tissue proteins such as transglutaminase 2 and 3, collagen, and S100B antigen may play a role in developing these immune-mediated skin lesions [60] |
| Generalized eczematous eruptions | Vaccine may act as an environmental trigger in a genetically susceptible individual (i.e., personal/family history of atopy) [61] |
| Radiation recall dermatitis | Offending agent upregulates inflammatory cytokines that are already increased in area of irradiation, leading to a local hypersensitivity reaction [87] |
| SDRIFE-like eruption | Co-infection by other viruses or uncommon clinical presentation of post-vaccination hyperviscosity [88] |
| Stevens-Johnson syndrome | Expression of vaccine antigens on keratinocytes leads to a CD8+ T-cell response against epidermal cells, thus causing apoptosis of keratinocytes and detachment of dermo-epidermal junction in a genetically susceptible individual [66] |
| Psoriasis exacerbation | Vaccine increases IL-6 production and recruitment of Th17 cells which are involved in psoriasis; [78] vaccine may activate the plasmacytoid and dermal myeloid dendritic cells, which upregulate type I IFNs that initiate the inflammatory cascade; [81] mRNA vaccines bind to Toll-like receptors that result in increased production of type I IFNs [45] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kroumpouzos, G.; Paroikaki, M.E.; Yumeen, S.; Bhargava, S.; Mylonakis, E. Cutaneous Complications of mRNA and AZD1222 COVID-19 Vaccines: A Worldwide Review. Microorganisms 2022, 10, 624. https://doi.org/10.3390/microorganisms10030624
Kroumpouzos G, Paroikaki ME, Yumeen S, Bhargava S, Mylonakis E. Cutaneous Complications of mRNA and AZD1222 COVID-19 Vaccines: A Worldwide Review. Microorganisms. 2022; 10(3):624. https://doi.org/10.3390/microorganisms10030624
Chicago/Turabian StyleKroumpouzos, George, Maria Eleni Paroikaki, Sara Yumeen, Shashank Bhargava, and Eleftherios Mylonakis. 2022. "Cutaneous Complications of mRNA and AZD1222 COVID-19 Vaccines: A Worldwide Review" Microorganisms 10, no. 3: 624. https://doi.org/10.3390/microorganisms10030624
APA StyleKroumpouzos, G., Paroikaki, M. E., Yumeen, S., Bhargava, S., & Mylonakis, E. (2022). Cutaneous Complications of mRNA and AZD1222 COVID-19 Vaccines: A Worldwide Review. Microorganisms, 10(3), 624. https://doi.org/10.3390/microorganisms10030624