1. Introduction
Constipation, as a common disease, affects 12–19% of the global population [
1,
2,
3], significantly impacting the quality of life of patients. One of the causes of constipation is disordered intestinal peristalsis [
4]. One of the clinical treatment methods is abdominal massage [
5], which promotes intestinal peristalsis by applying massage force externally and has the advantages of non-invasiveness, safety, and comfort [
1,
6,
7]. However, abdominal massage is highly dependent on the experience of professional therapists, and there are problems such as high labor costs, insufficient treatment standardization, and large individual differences in efficacy. The high-frequency treatment requirement of 15 min per day exacerbates the shortage of medical resources, and the subjectivity of the manipulation force and the position of the massage effect make it difficult to quantitatively evaluate the efficacy. Against this background, intelligent abdominal massage devices integrating robot technology have become a key direction to breaking through the bottleneck of traditional therapies.
Globally, related research has been continuously exploring the mechanical structure, control strategies, and clinical applicability of the devices. Early commercial products, such as the Israeli Free-Lax [
8], achieved vertical mechanical stimulation through double-disk vibration, and the Spanish MOWOOT [
9,
10] used an air pressure belt for rhythmic extra-colonic peristalsis treatment. Although basic automation was achieved, these products could only provide a single vibration or pressing function. Moreover, limited by the wearable structure, it was difficult to adapt to the complex anatomical contours of the abdomen. The South Korean Bamk001 [
11] integrated an air-bag hot-compress module and simulated the intestinal tract direction through clockwise air-pressure massage. However, due to the complex pneumatic system, it had high maintenance costs and insufficient action accuracy. Regarding the intestinal management training massage devices developed in China, except for one that has been applied in clinical practice [
12,
13], the rest are still in the patent research and development stage [
14,
15,
16]. They rely on manual adjustment, have a low level of intelligence, and cannot achieve autonomous control of force control and path planning. In terms of non-wearable devices, the medical transformation of industrial collaborative robots provides a new direction. The variable-stiffness drive technology of the German DLR seven-degree-of-freedom robotic arm [
17] and the compliant control algorithm of the Danish UR robot [
18] have laid a technical foundation for precise force control. The Singaporean EMMA robot [
19] combines 3D vision to achieve human body shape analysis, and the French IYU robotic arm [
20] completes compound actions such as pushing and pinching through a massage glove, demonstrating the possibility of realizing multi-modal manipulation by robots. Chinese research focuses on the bionic realization of traditional Chinese medicine manipulation methods. For example, the four-degree-of-freedom massage head-switching technology of Southeast University [
21] and the six-manipulation integrated system of the LLR-1 robot of Shandong Jianzhu University [
22,
23,
24,
25,
26] have made progress in action diversity. However, there is still a gap in the adaptive control of abdominal soft tissues.
The bottlenecks of existing technologies are concentrated in three aspects: First, the standardized modeling of abdominal massage techniques is insufficient. The core techniques of traditional Chinese medicine, such as pressing, kneading, pushing, and vibrating, involve multi-axis movement coordination. Most existing devices are limited to single-dimension actions and lack in-depth integration of the theory of Chinese medicine meridians and anatomical positioning. Second, the precision of intelligent control needs to be improved. The nonlinear mechanical properties of abdominal soft tissues (such as contour fluctuations caused by breathing and differences in individual fat layer thickness) pose higher requirements for the force control system. However, most devices rely on fixed impedance models and are difficult to dynamically adapt to complex physiological environments. Third, there are defects in the clinical adaptability of the device structure. Although large robotic arms have high degrees of freedom, their large size can easily cause psychological stress to patients. Wearable devices are limited in their range of motion and cannot cover key areas such as the ascending colon and descending colon.
In response to the above challenges, this study proposes a six-degree-of-freedom multi-functional abdominal massage robot system based on the integration of traditional Chinese and Western medicine. By analyzing traditional Chinese medicine meridian theory and modern anatomy, an abdominal key point model including core acupoints such as Zhongwan and Tianshu is established to solve the problem of non-visual positioning. An innovative series-parallel hybrid mechanical structure is designed. The upper track module conforms to the inverted U-shaped trend of the colon. The middle parallel mechanism realizes the adjustment of the angle and depth of the massage head, and the lower series module completes fine movements such as kneading and pinching, forming a multi-dimensional treatment space covering the entire abdomen. In terms of control strategy, admittance control, and adaptive fuzzy algorithm are integrated to build a force–position closed-loop system, which can respond to the impedance changes in soft tissues in real-time and ensure that the massage force error is stable within the safe threshold. This research not only breaks through the single function of traditional equipment but also provides a technical solution to solve the uneven distribution of resources and curative effect differences in constipation treatment through standardized manipulation modeling and intelligent control technology. Through simulation and human experiments, the robot can accurately reproduce four basic manipulation techniques and demonstrates stable force control performance in tests on silicone phantoms and human abdomens, providing an innovative path for promoting the intelligentization and standardization of clinical abdominal massage. In the previous work, our team proposed the first-generation abdominal massage robot [
27], introduced the structural design and motion analysis of the first-generation robot, and simultaneously carried out research on the biomechanical characteristics of the abdomen [
28]. This system can realize four different massage techniques (pressing, pushing, kneading, and vibrating). In order to further enrich the massage techniques and apply appropriate massage forces, this paper improves the system from three aspects: mechanical structure integration, control strategy optimization, and experimental system verification.
Section 1 of this paper elaborates on the research status of abdominal massage robots; mechanically (
Section 2), this paper enhances the manipulation actuator to integrate five core techniques (pressing, vibrating, pushing, kneading, and pinching). Crucially, we introduce dual assembly modes: a tandem structure for immediate access to all vibrating, kneading, and pinching techniques without reassembly, and an on-demand parallel structure enabling quick disassembly and assembly of these three techniques. This parallel design reduces motor count, lowers hardware costs, and facilitates future expansion and maintenance. For the control strategy (
Section 3), beyond basic admittance control, we incorporate a variable-stiffness physical model representing abdominal environmental damping. This provides a predictive basis for both massage force and depth, significantly stabilizing force interaction and confining errors within 0.8 N. Experimentally (
Section 4), validation is enhanced with dynamic force tracking tests on both static phantoms and a novel dynamic phantom simulating respiratory motion, rigorously challenging force stability under physiological disturbances.
2. Structural Modeling of Abdominal Massage Robot
The human abdomen and the abdominal massage robot can form a human–machine coupling system. The abdominal massage robot needs to consider more about the effectiveness of output operations, system safety, and the psychological cognition of the audience’s experience. The structural design of the abdominal massage robot designed in this paper mainly follows the following conditions: (1) The robot should be able to enter the massage operation state through convenient and simple operations. (2) The robot can output a variety of different massage techniques that can be combined as required. (3) The working space of the robot should cover the range of all abdominal action points, or even the entire abdomen. (4) The massage end-effector should be able to adapt to the non-homogeneous distribution specificity of the surface morphology of the human abdomen. (5) It must be safe and reliable.
Based on the above conditions, the requirements are as follows: (1) In the case where the human body is in a supine position during clinical massage, the robot should be able to quickly approach the human body and reach the ready-to-operate posture. Therefore, the robot needs to have the ability to move and a configuration suitable for the supine position. (2) There are many types of clinical massage techniques at home and abroad, mainly focusing on five types: pressing, vibrating, pushing, kneading, and pinching. (3) The working space of the robot should be determined based on the “Abdominal Key-point Identification Model” [
27]. (4) The massage end-effector needs to add a degree of freedom for angle adjustment. (5) The system needs to be equipped with complete safety protection measures.
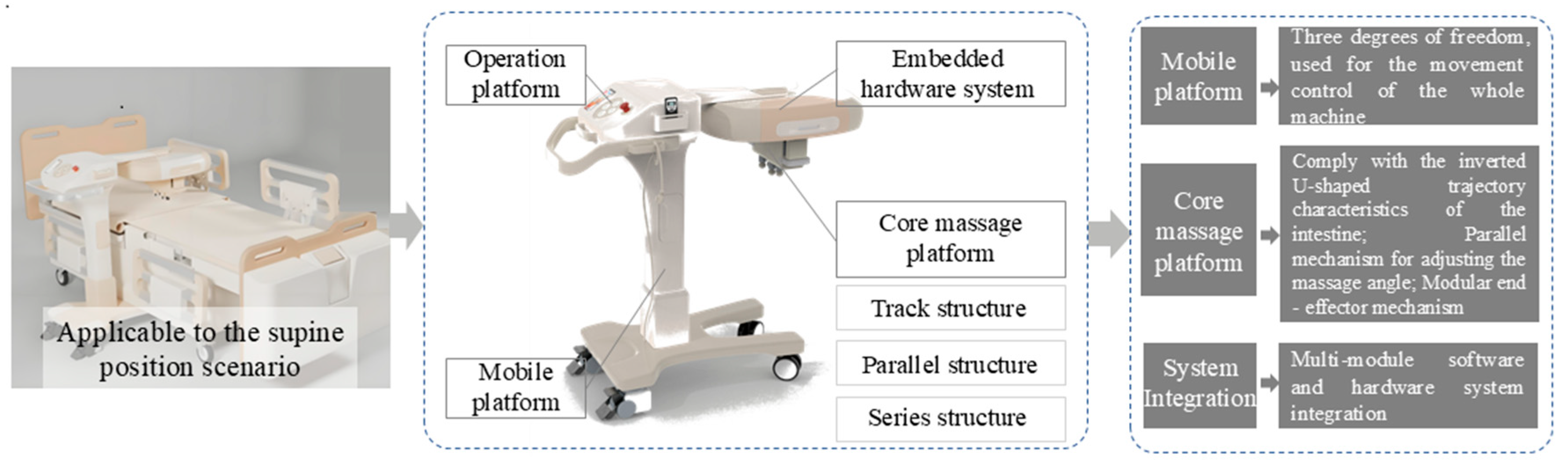
Figure 1 shows the overall design scheme of the series-parallel abdominal massage robot mechanical system. This conceptual device consists of four main parts: (1) The three-degree-of-freedom (up-down, left-right, front-back) mobile platform of the robot, which is used for the movement of the whole machine. (2) The core massage platform, which includes the following: (a) a track structure, used to achieve the movement characteristics of the massage trajectory along the inverted U-shaped trajectory of the intestine; (b) a parallel structure, used to achieve stable operation of pressing and pushing techniques, adjustment of the massage angle, and fine-tuning of the massage trajectory; and (c) a series structure, with a universal design, to which different forms of end massage execution mechanisms can be added to adapt to different usage scenarios. (3) The control hardware system, composed of multiple motors, sensors, and their supporting drive boards and circuit boards, etc., is used for the interaction between the human abdomen and the robot. (4) The whole machine operation platform, including the basic button control of the three-degree-of-freedom mobile platform and the placement platform for the upper computer (such as a mobile phone or a tablet).
The design of the abdominal massage robot system for supine human ergonomics needs to meet the following core functional requirements: First, based on the biomechanical characteristics of the human body in the supine position, the system must have a rapid postural adaptation mechanism and positioning ability. Specifically, a rapid-positioning system with the navel as the reference point needs to be established to achieve precise alignment with the target anatomical area, which poses strict requirements for the dynamic response characteristics of the mobile platform. Second, to meet the adaptability of the intestinal anatomical direction, the non-homogeneous distribution specificity of the abdominal body surface morphology, and the multi-modal task requirements in clinical treatment, the system needs to integrate a modular actuator to achieve the following key technologies: a multi-mode manipulation generation system (including five traditional Chinese medicine manipulation methods such as pressing, pushing, vibrating, pinching, and kneading) and a three-dimensional space attitude adjustment system.
Based on the above functional requirements, this study proposes a design scheme of a dual-platform collaborative architecture: a three-degree-of-freedom (3-DOF) mobile platform is used to achieve rapid positioning of the navel, and a six-degree-of-freedom (6-DOF) core massage platform is used to complete fine-scale massage operations through a series-parallel massage actuator. Among them, the mobile platform realizes planar movement through a universal wheel system and combines a three-motor module combination to achieve a three-degree-of-freedom alignment function; the core massage platform is based on a series-parallel configuration, combines fixed-track limiting and the integration of a multi-modal end-effector for massage, and can complete spatial pose adjustment and multi-manipulation switching.
2.1. Structural Generation of Three-Degree-of-Freedom Mobile Platform
Based on the requirements of the rapid postural adaptation mechanism and positioning ability, this study designed a three-degree-of-freedom mobile platform (shown in
Figure 2), which includes a reversing structure, three-degree-of-freedom adjustment, and a braking chassis. Based on the requirements of the supine clinical scenario, this mobile platform adopts a C-shaped topological structure, that is, a cantilever beam is designed at the top of the vertical main structure, and the base extends in the same direction at the bottom to form a stable torque balance system. The top reversing structure consists of a cantilever beam and a damping limit mechanism to achieve reversing. The damping limit mechanism uses a disk damper in combination with a spring-preloaded indexing pin to achieve 180° reversing positioning. The vertical main body is composed of a Z-axis vertical lifting unit (lifting column) and X/Y axial translation units (two linear stepping motors) to form a three-degree-of-freedom adjustment module, which can achieve the adjustment function of aligning with the navel and a maximum three-degree-of-freedom adjustment space of 100 mm × 100 mm × 100 mm. The base is a braking system with double universal double Fuma wheels. When in use, it needs to be extended under the bed body and is consistent with the trend of the top reversing mechanism to form a stable torque balance system. The movement adopts an omnidirectional movement scheme. The front wheel set is designed without a locking mechanism, and the rear wheel set integrates a foot-operated braking Fuma wheel. The traditional tangential locking method is replaced by friction braking on the contact surface, effectively overcoming the stability defects of the traditional universal wheel combination when not all wheels can be braked.
2.2. Structural Generation of Six-Degree-of-Freedom Core Massage Platform
Based on the kinematic characteristic analysis of five traditional Chinese medicine massage techniques, namely pressing, vibrating, pushing, kneading, and pinching, this study innovatively proposes the core massage structure design of a series-parallel hybrid abdominal massage robot. By combining the track motion platform with a three-degree-of-freedom massage head, five different massage techniques and the attitude adjustment of the end massage execution mechanism can be achieved.
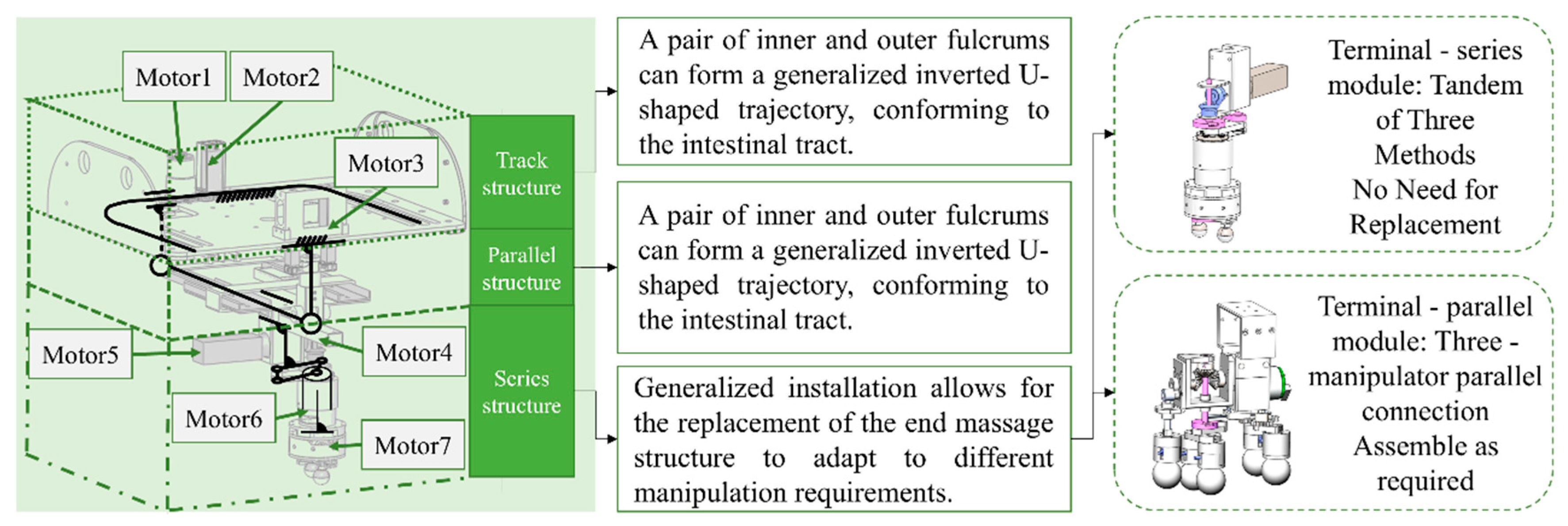
Figure 3 shows the overall design concept of the core massage structure of the abdominal massage robot. The robot has three layers of functional modules. The upper structure is the track module, the middle layer is the parallel module, and the lower layer is the series module.
Multi-scheme design of the series-connected massage end-module: The lower-layer series-connected massage end-module is designed with a universal interface, which is used to combine massage ends as needed according to different application requirements, to achieve three required manipulation techniques: vibration, kneading, and pinching. In order to distinguish different application requirements, two schemes are designed: the three-manipulation series-connected structure (
Figure 4a) and the three-manipulation parallel-on-demand structure (
Figure 4b). The published research [
27] introduced the three-manipulation series-connected structure, which is characterized by functional continuity. It does not require combined installation and is suitable for scenarios where all three manipulation techniques need to be applied, and long-term stable operation is required. The overall height is relatively large, making it suitable for people who do not mind a long massage end. The three-manipulation parallel-on-demand structure, on the other hand, has the core advantages of dynamic collaboration and flexible reconfiguration, with a higher degree of integration. It is suitable for people who need parallel kneading and pinching techniques and those who mind the excessive length of the massage end. However, the parallel-connected massage execution ends require manual quick-disassembly and quick-assembly intervention. The differences between the two in topological configuration, functional expandability, and space efficiency provide complementary solutions for different clinical application scenarios.
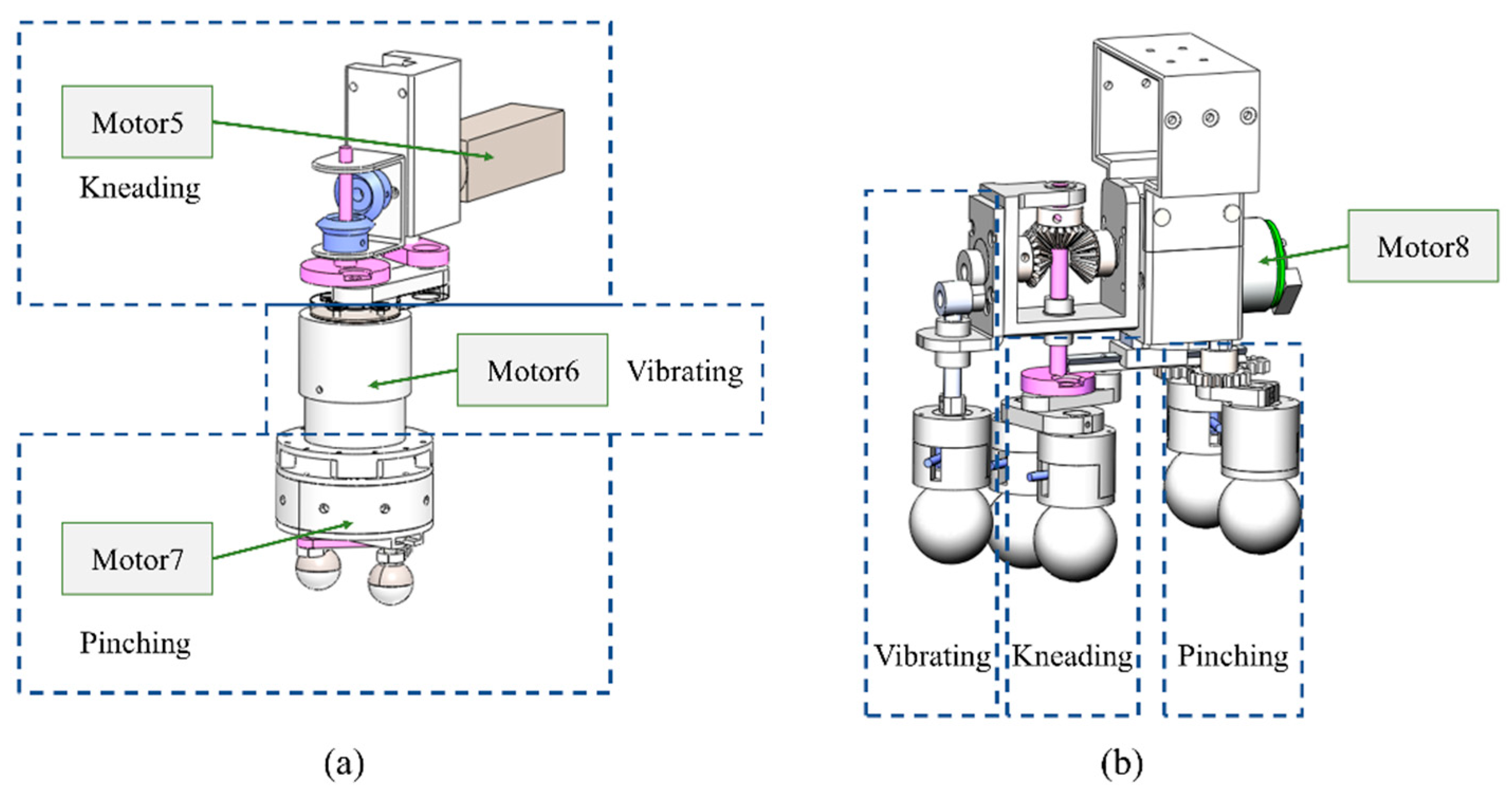
This article focuses on introducing the on-demand parallel structure scheme of three manipulation methods: based on the universal interface, a bevel gear reversing structure with one input and two outputs is used to achieve the parallel connection of three execution structures. The one input is a rotary motor (Motor8), and the two outputs are two types of output structures, respectively. One is a vibration manipulation mechanism that uses a crank slider combined with a linear bearing to form an up-and-down reciprocating motion. The second is a kneading-manipulation mechanism formed by using the crank motion characteristics in the crank-slider structure and a pinching-manipulation mechanism with a reciprocating opening and closing formed by combining the reciprocating motion characteristics of the slider with a gear-rack meshing structure. This greatly improves the utilization efficiency of the rotary motor (Motor8). In the actual application process, there are four implementation modes: vibration, kneading, pinching, and kneading-vibration simultaneously. The massage end uses the coarse-thread characteristics to achieve the function of quick disassembly and quick assembly, making the on-demand combination more convenient, and also facilitating scenarios such as expansion and maintenance in subsequent engineering applications.
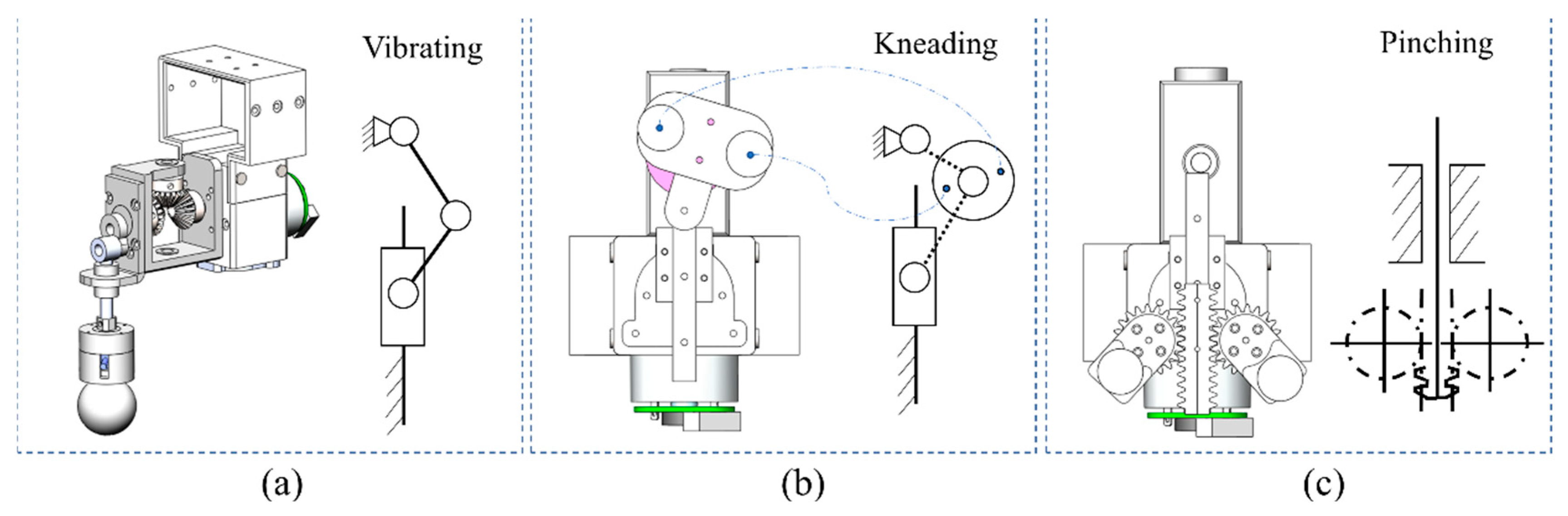
The schematic diagrams and kinematic diagrams of the three techniques in the on-demand parallel structure scheme of the three-technique method are shown in
Figure 5. Analyze the motion characteristics of the vibrating technique from the side view (
Figure 5a), and analyze the motion characteristics of the kneading technique and the pinching technique from the bottom view (
Figure 5b,c).
The overall machine integration is shown in
Figure 6.
3. Research on Safety Massage Control Strategies
The target of massage—the anterior abdomen, as a part that encloses important organs—has no rigid bone support or protection. If subjected to inappropriate external forces, it may pose a life-threatening risk to the human body and cause irreparable harm. Achieving safe force application control that aligns with the biomechanical characteristics of the abdomen has become the core challenge in abdominal massage. The second study on the biomechanical characteristics of the abdomen carried out by our team during the same period [
28] developed variable-stiffness physical models and massage force prediction methods for different populations. A personalized abdominal biomechanical model was established, contributing to the exploration of quantifying the force–displacement relationship of abdominal interaction. This is combined with an innovative series-parallel abdominal massage robot solution proposed in this paper. By exploring the robot massage force interaction strategy based on these two types of research, the mechanical adaptability of the robot to abdominal soft tissues can be effectively improved.
3.1. Analysis of Safety Massage Requirements
According to the safety requirements for abdominal massage robots, the control of massage force is the control target of core risks. Clinical massage experts point out that the basic requirements of massage techniques are durability, forcefulness, uniformity, softness, and penetration [
29]. As can be seen from
Table 1, researchers [
30] have conducted kinematic and dynamic analyses of various techniques, clarifying parameters such as the number of degrees of freedom and the action frequency of each technique. The degree-of-freedom matrices of different techniques are inconsistent. However, current research on the magnitude of the applied force and the intelligent force control strategy of the robot still rely on individual test data, and there is no systematic answer to how to apply an appropriate massage force. Moreover, in the actual massage process, the lightness or heaviness of the applied massage force has a strong subjective color. Applying the “light, medium, and heavy” massage forces according to subjective feelings also requires a scientific basis for differentiation.
This study is based on the pressing method with a relatively low operating frequency and uses the manipulation of a single degree of freedom to study the interactive control strategy of massage force. In the second study on the biomechanical properties of the abdomen [
28] conducted by our team during the same period, the collection of force–displacement coupling data of the massage interaction force of the pressing method was completed. This study will establish a safety control algorithm based on safety thresholds. In the actual interaction process, the subjective feelings of the subjects range from no feeling to discomfort and inability to continue, as shown in
Figure 7. The turning point from no feeling to a slight feeling is recorded as sensory point 1; the turning point from a slight feeling to a strong feeling without discomfort is recorded as sensory point 2; and the turning point from a strong feeling without discomfort to a strong feeling with discomfort is recorded as sensory point 3. Analyzing these three points provides a basis for dividing the light, medium, and heavy massage forces.
3.1.1. Basis for Setting the Speed of Abdominal Massage
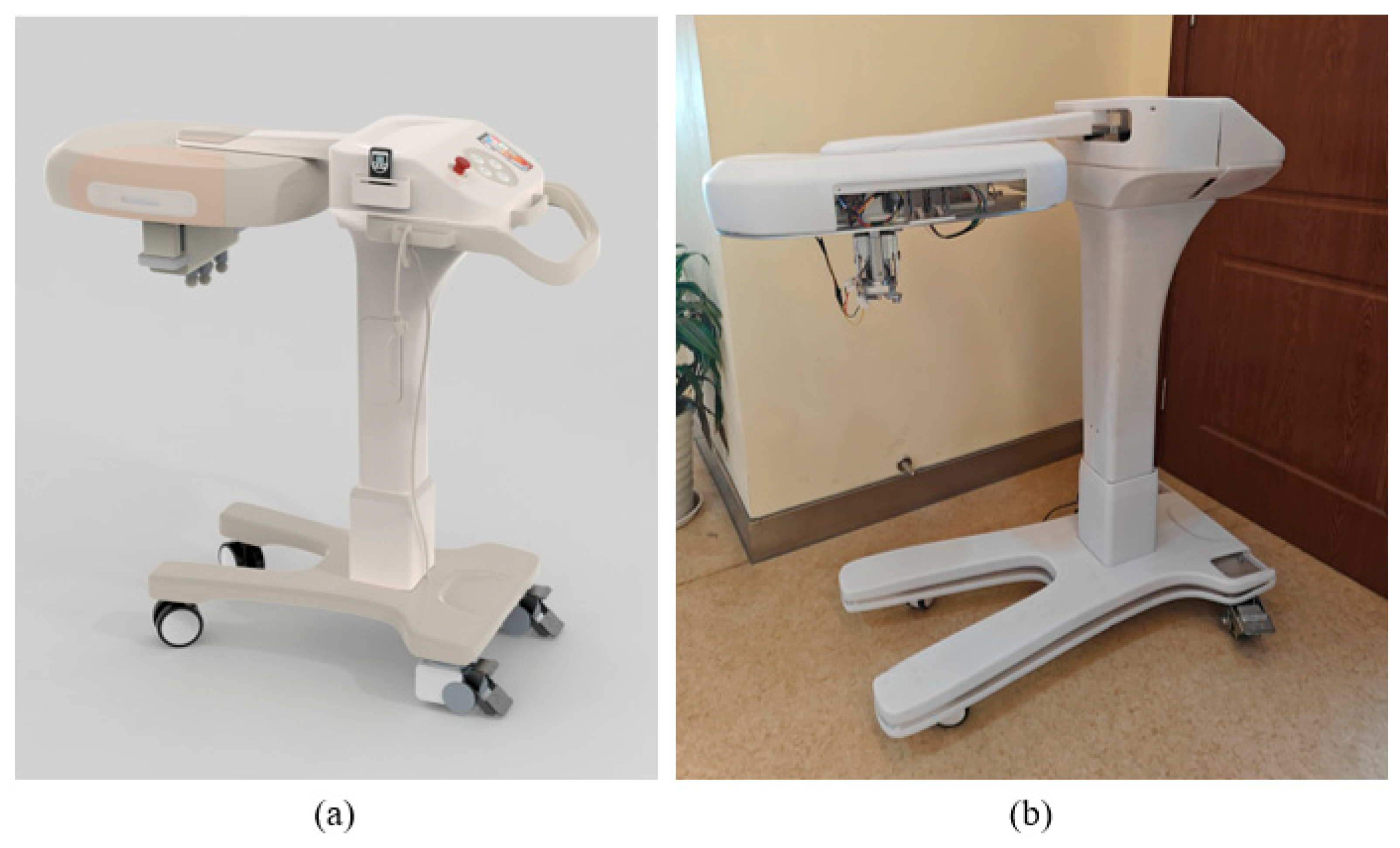
It can be seen from
Table 1 that the application frequency/speed of different massage techniques can be within a certain range. Then, the following questions arise: What frequency/speed should the robot apply? Will different frequencies/speeds lead to differences in the abdominal mechanical response? To address these questions, this paper selected three subjects and chose any three points from the key point identification model of the abdominal action for experiments. Data collection of three different pressing speeds (3 mm/s, 6 mm/s, 8 mm/s) was carried out on the subjects using the independently developed mechanical experimental platform (
Figure 8).
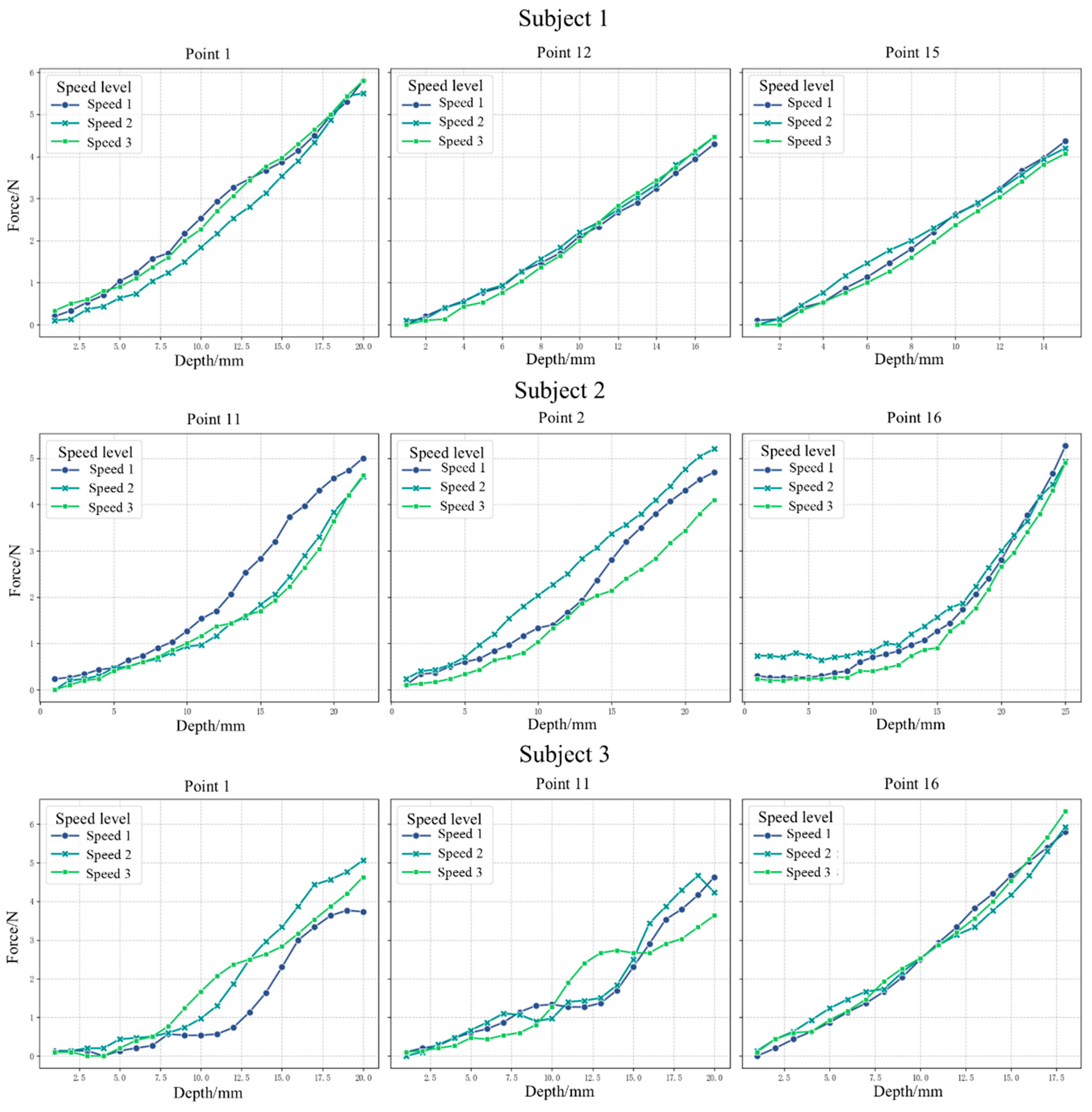
Use Levene’s Test for homogeneity of variance to test the homogeneity of variance of the three velocity groups at each point. Select the test method based on the results of the homogeneity of variance. When
p is greater than or equal to 0.05, use ANOVA; when
p is less than 0.05, use the Kruskal–Wallis non-parametric test. The output results are shown in
Table 2 and
Figure 9. The
p-value of the Levene test result represents the significance level of the homogeneity of variance test; the capital F-value in the ANOVA result represents the ratio of between-group variation to within-group variation, reflecting the significance of the mean difference, and the
p-value represents the significance level of the mean difference test. The threshold significance level for both is alpha equal to 0.05. As can be seen from the table, the
p-values of all the above Levene tests are greater than 0.05, indicating that the homogeneity of variance of the three velocity groups holds and meets the preconditions for ANOVA. The
p-values of the ANOVA tests are all greater than 0.05, indicating that there is no significant difference in the mean pressing force of different velocity levels (the closer the F-value is to 0, the smaller the between-group difference). Therefore, it can be concluded that under slow-speed conditions, the interaction force–displacement data is not sensitive to the pressing speed.
3.1.2. Basis for Setting the Intensity of Abdominal Massage
Clinical massage involves therapists differentiating light, medium, and heavy intensities based on their own experience combined with the subjective feedback of the subjects. This section aims to quantify the ranges of light, medium, and heavy intensities. Therefore, a study on the basis for classifying abdominal massage intensities was carried out. According to the data collected in the experiments during the research on the biomechanical properties of the abdomen [
28], subjective perception data of seven subjects were obtained. The information about the subjects is shown in
Table 3. If the number of valid points is less than 18, some points may fall outside the subject’s abdomen or on its edge, resulting in invalid data. In the experiment, the pressing depth values corresponding to three types of sensory points were collected. It is also necessary to determine the pressing force values corresponding to the force–displacement experimental data of that time according to the pressing depth. The processed pressing depth values and force values of each type of sensory point were summarized and analyzed to explore whether the subjective perception is related to the pressing depth or the pressing force.
Parameter Space Distribution Trend Model
where
represents the measured value of parameter
at point
for subject
, and
is the spatial residual term.
Calculate the distribution characteristic quantities of parameters at each point:
Establish a two-factor analysis of the variance model:
Among them,
is the subject effect,
is the point effect,
. Construct the F-test statistic:
Report the significance levels of each factor through the ANOVA table (
Table 4). According to the results in the table, individual differences are significant at sensory points 1 and 3, but not significant at sensory point 2, which may be caused by the physiological or perceptual differences in the subjects. Therefore, in clinical massage applications, it is necessary to prioritize personalized adjustment of the intensity rather than relying on a unified standard. Therefore, the distinction of light, medium, and heavy intensities in abdominal massage should vary from person to person. Trend diagram of pressing depth and force corresponding to sensory point 1 is shown in
Figure 10.
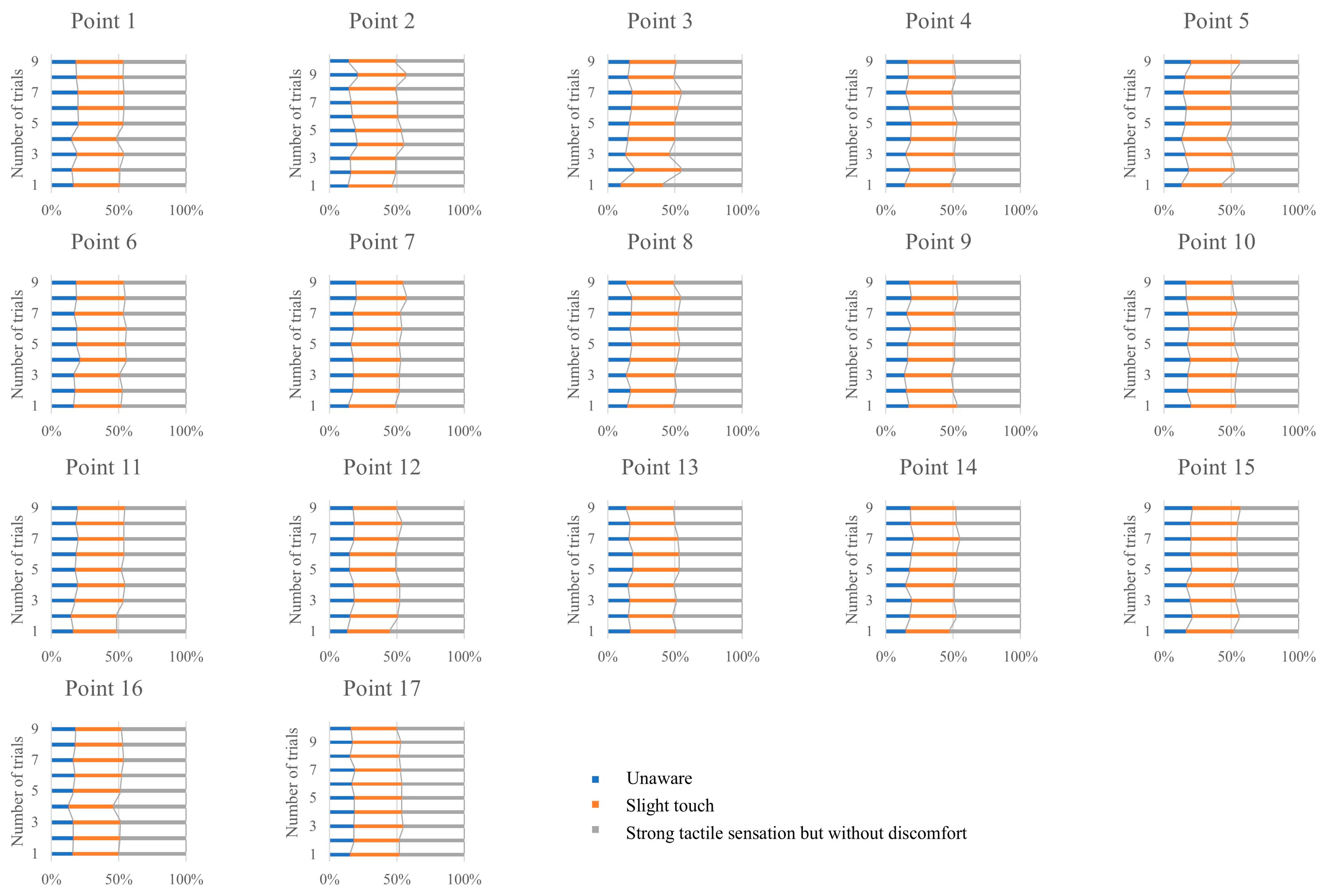
This paper shifts the research focus to the distribution patterns of the subjects’ three sensory points throughout the entire experimental process and aggregates the results from seven subjects. This enables us to study the proportional relationship of the three sensory points throughout the interaction process. In this study, sensory point 3 is set as the end point of the interaction, that is, it is located at the 100% position in the entire interaction process. The proportional relationship of the remaining sensory points 1 and 2, after data processing, is shown in
Figure 11.
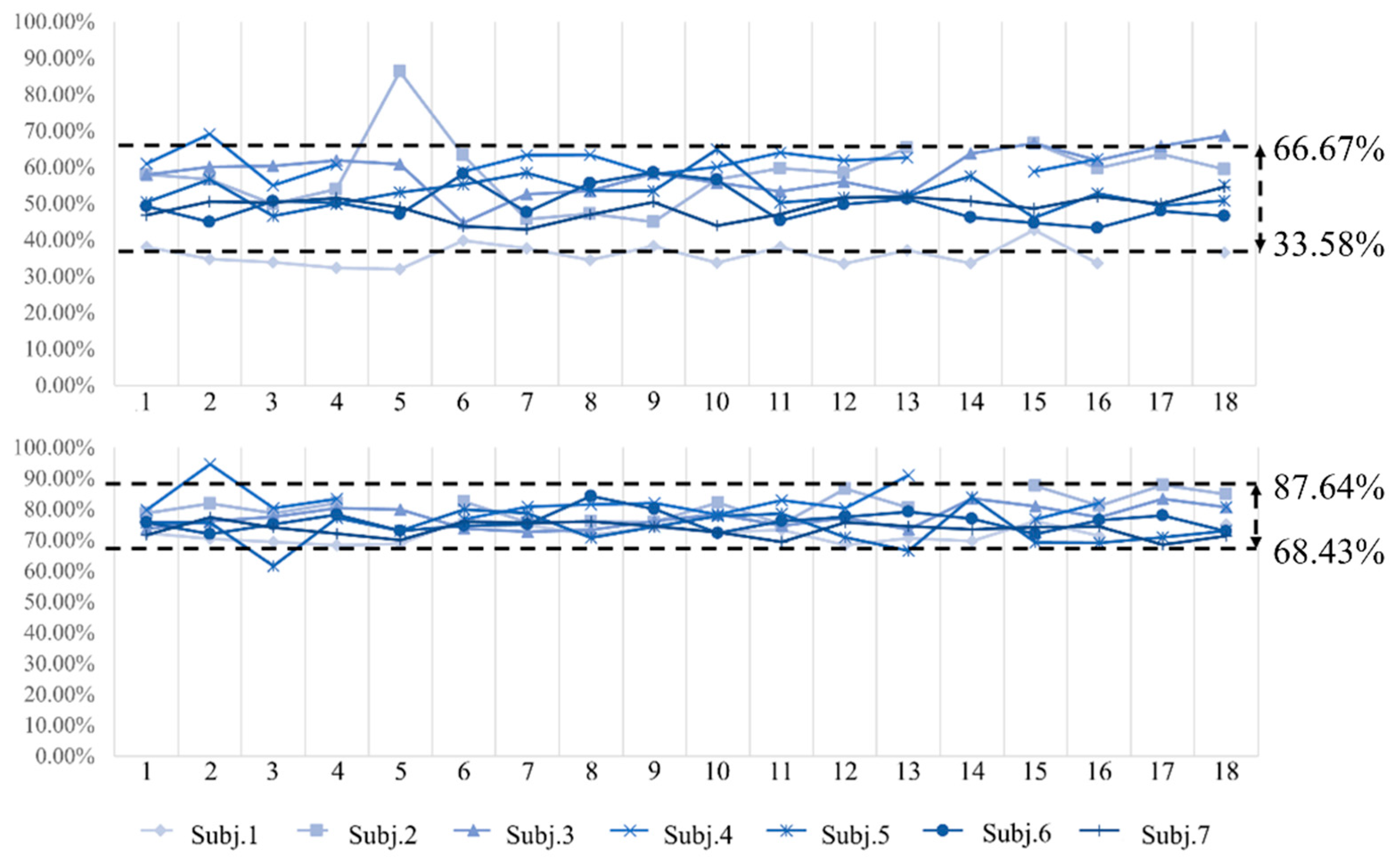
Summarize the three-sense distribution of all valid points of seven subjects (as shown in
Figure 12), and calculate the range within the 95% confidence interval. It can be seen that the distribution range of sensory point 1 is 33.58–66.67%, and the distribution range of sensory point 2 is 68.44–87.64%. Based on the above data, this study sets the light, medium, and heavy ranges of the pressing force within the distribution ranges of the two sensory points. The insensitive interval and the discomfort interval during the interaction process are removed, and the remaining two sensory intervals are divided into three equal parts. The front section, middle section, and end section are defined as light, medium, and heavy pressing forces, respectively, as shown in
Figure 13.
3.2. Biomechanical Adaptation Control Strategy Integrating Variable-Stiffness Physical Model
3.2.1. Force Interaction Control Based on the Variable-Stiffness Physical Model of the Abdomen
This abdominal massage robot uses pressure sensors and push rod motors for force control in the pressing technique. The miniature tension–compression sensor SBT674 (Sibatuo, Guangzhou, China) is selected to measure the interaction force between the end-effector massage structure and the human abdomen. It has a measurement range of 0–20 N, a signal voltage accuracy of 0.06 mv, and an error ≤ ±0.3%, enabling real-time and accurate monitoring of changes in the massage force. Signal processing involves acquiring force data from the SBT674 sensor as a voltage signal via an ADC channel, followed by applying a median filter to remove high-frequency noise (such as electrical interference or transient physiological tremors), thus ensuring stable force readings by eliminating outliers while preserving true force trends. In the prototype of the abdominal massage robot, the motor used to implement abdominal pressing is the push-rod motor MNTL (Luilec, Changzhou, China, 50 mm stroke, 60 N load, 0–8 mm/s speed).
Based on the massage interaction force–displacement coupling data from the second study on the research of abdominal biomechanical properties [
28], a variable-stiffness physical model applicable to abdominal massage was derived:
Among them, represents the contact force, and represents the deformation at the pressed location. This simplified physical model can reflect the typical mechanical behavior of soft tissues: an initial approximately linear response, dominated by the parameter , which describes the stiffness of the soft tissue in the initial stage (the proportionality coefficient between force and deformation). Subsequently, it exhibits nonlinear hardening, regulated by the parameter , which describes the phenomenon that the soft tissue becomes significantly stiffer under large deformations, representing the rate of material nonlinear hardening. The variable-stiffness physical model can reflect the biomechanical properties of the abdomen and describe the interaction force–displacement mapping relationship of the abdomen.
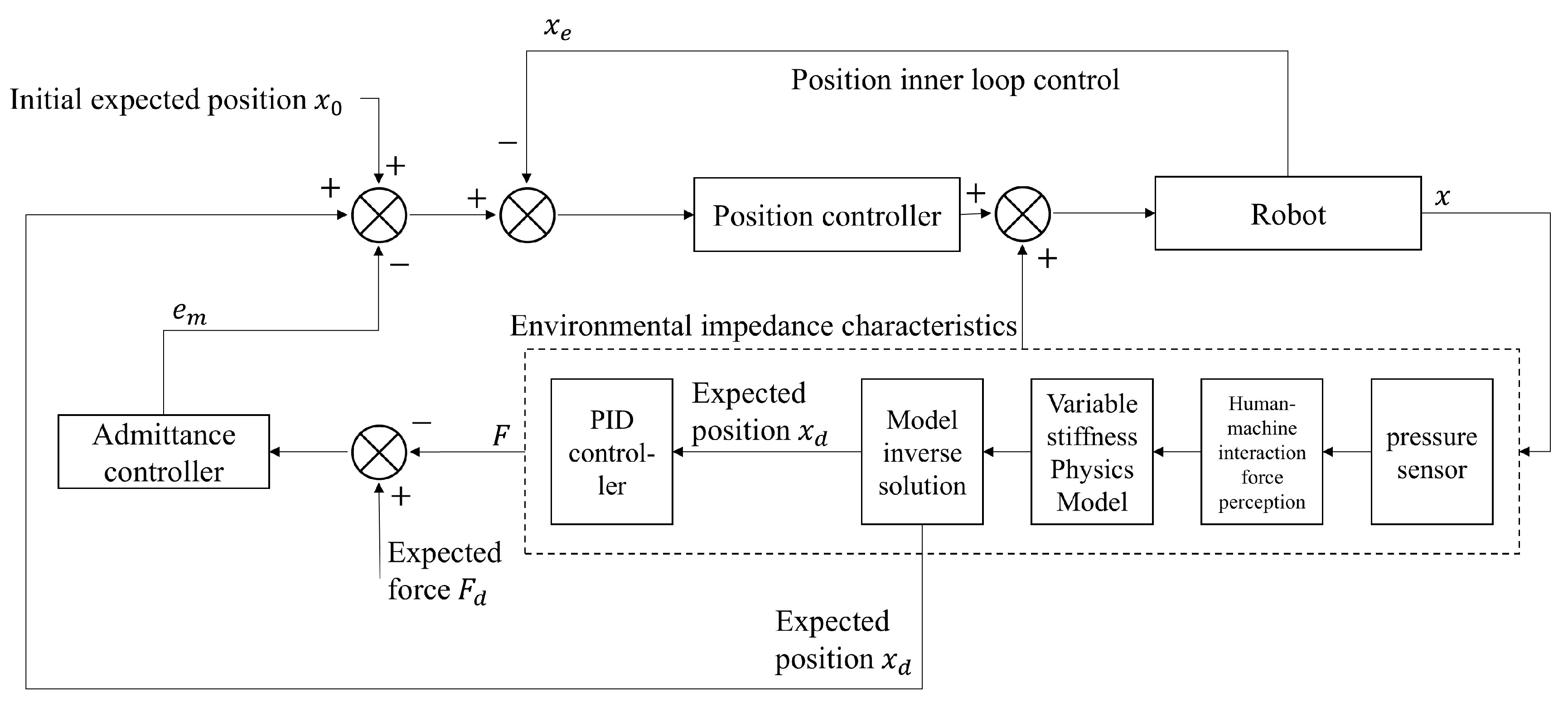
Select this variable-stiffness physical model to represent the force–displacement mapping relationship. During the actual massage process, the prediction results of the variable-stiffness physical model are added as feedforward input to improve the high-precision tracking control of the push rod motor, thus achieving stable control of the massage force. An inner–outer loop, admittance-PID hybrid control model is designed. The outer loop employs admittance control to retain compliant interaction characteristics, while the inner loop uses PID control to achieve high-precision tracking, enhancing both tracking accuracy and dynamic response. This combination effectively balances both “safety” and “precision”. Biomechanical adaptation interactive force control strategy incorporating a variable-stiffness physical model is shown in
Figure 14.
Inner loop PID control strategy: First, set the target force at a certain point of the massaged person as
. During the massage process of the pressing method, the change process of
is from
to the pause, and then
. Then, it is necessary to control the pressing displacement
. During the massage process, first, use the conventional force control strategy to obtain the initial control target
, and obtain the force–displacement data in the change process of
:
. Introduce the variable-stiffness physical model (Formula (5)). Use the least-squares method to derive the parameters
and
. Substitute the parameter derivation results into the model and inversely solve the theoretical target displacement
corresponding to
. According to the variable-stiffness physical model (Equation (5)),
is the exact displacement that satisfies
. Therefore, by setting
as the PID reference input, adjust the actual displacement
through the PID controller to make it converge to
. When
, the contact force
will converge to
due to the fundamental mapping
. After completing one control, reset
and obtain new force–displacement data. Use PID control to approximate the target: Take
as the set value, and adjust the actual displacement
through the PID controller to make it converge to the target value.
Among them, represents the control signal, driving the actuator to adjust the displacement. After completing one control, reset , and obtain the force–displacement data during the new-round change of : , continuously adapting to the changes in biomechanical characteristics and self-adaptively adjusting the parameters of the variable-stiffness physical model.
3.2.2. Simulation Experiments and Verification
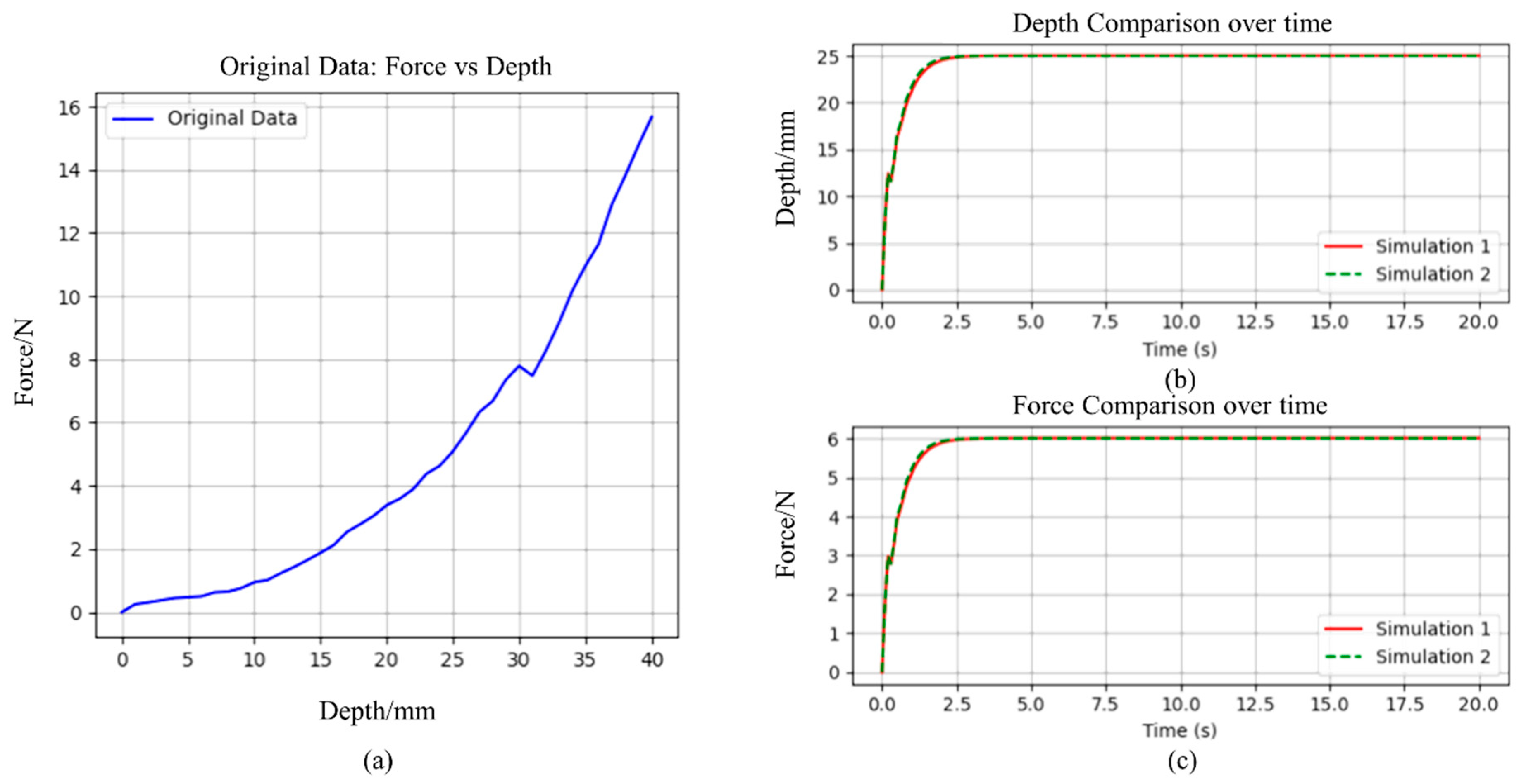
In this section, the proposed massage force interaction control strategy based on the variable-stiffness physical model is verified through simulation experiments. The simulation object is an abdominal massage robot. First, a certain desired force
and initial desired position
are set. Based on the position controller, the actual force–displacement data during the change of
is obtained
, as shown in
Figure 15a. The parameters
and
of the variable-stiffness physical model are derived using the multi-array
, and then inverse calculation is carried out to generate the variable-stiffness physical model; the desired position
based on the actual force–displacement data is output. Stable force–position control is carried out based on the desired force
and the desired position
. Based on the force–displacement coupling relationship, three advanced simulations are carried out. However, the result from the third iteration is the same as that from the second. This is because, in the second simulation, the parameters
and
of the variable-stiffness physical model had already converged to their optimal values. As a result, there were no changes in the third simulation data. Therefore, only the simulation results of the first and second simulations are analyzed here. These two sets of simulation results are evaluated and presented in
Figure 15b,c. A detailed analysis of the data from both simulations is shown in
Table 5. From the results, it can be seen that the simulation consistency is good—both MSE and MAE are extremely low, the overall results of the two simulations are highly consistent, and the model parameter setting is reasonable. The target position and target force are reached and remain stable at around 2.5 s. The simulation reliability of the pressure value is high, the stability is better than the displacement performance, and the robustness is stronger. The Max error of the displacement is 0.5281, which is within the allowable error range and is still a reliable result.
4. Experimental Research
The test platform for the abdominal massage robot mainly consists of a prototype of the abdominal massage robot for testing, a static simulation prosthesis for testing, a dynamic simulation prosthesis for testing (airbag + integrated portable air pump for inflation and deflation), a bed body, and distributed pressure sensors, as shown in
Figure 16.
Among them, the test prostheses are divided into two types: one is a static simulation prosthesis, which uses a sponge material model imitating the human abdomen, and the other is a dynamic test prosthesis. The inflatable airbag (180 mm × 260 mm) is equipped with a special air nozzle connected to an air pump, which can simulate the abdominal undulation characteristics of human breathing. The integrated inflatable and exhaust portable air pump has a model GR-688C and an airflow rate of 400 L/min. The miniature tension–compression sensor SBT674 (Sibatuo, Guangzhou, China) and the push-rod motor MNTL (Luilec, Changzhou, China, 50 mm stroke, 60 N load, 0–8 mm/s speed). During the experiment, the distributed pressure sensor is covered on the surface of the static/dynamic simulation prosthesis. The end massage head of the abdominal massage robot is spherical, and the direct contact area with the prosthesis during the experiment does not exceed the size of a single sensing point.
4.1. Research on the Functional Simulation Experiment of the Abdominal Massage Robot Prosthesis
4.1.1. Massage Performance Test Experiment
For the performance evaluation of the abdominal massage robot system, this study focuses on systematically verifying three performance indicators: the diversity of massage modes, the target positioning range, and the steady-state characteristics of force output. The specific research content and results are as follows:
- (1)
Multimodal verification experiment of massage modes
The diversity of abdominal massage modes depends on the number of massage techniques applied by the robot. Different massage needs require different massage techniques. Based on the six-degree-of-freedom abdominal massage robot core platform developed in this study, this study carried out kinematic verification experiments of basic massage techniques. Through the coordinated control strategy of the serial end-effector and the track motion platform, this platform realizes the precise decoupling control of five basic massage actions: pressing, vibrating, pushing, kneading, and pinching. The experiment mainly verified the motion trajectory generation ability and the action parameter adjustment range under each massage mode.
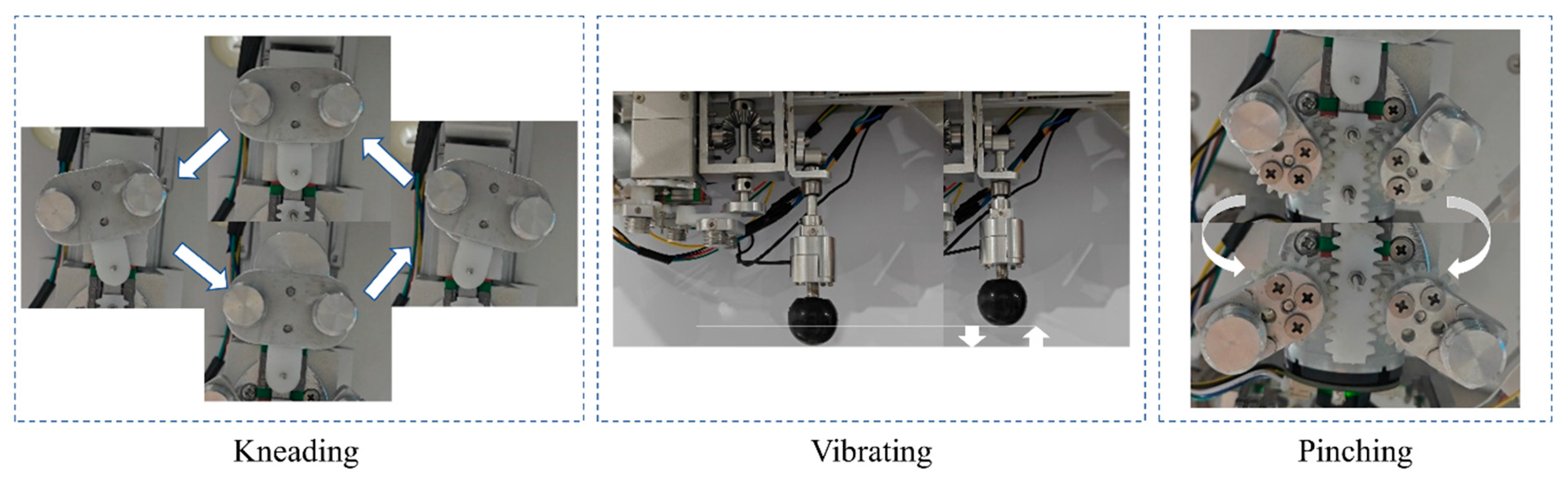
Figure 17 shows the motion characteristics of the kneading, pinching, and vibrating techniques of two schemes in the series module of the six-degree-of-freedom core massage platform: the three-technique series structure and the three-technique on-demand parallel structure.
Based on the parallel structure of the three-manipulation on-demand system, multi-modal motion tests of five manipulations are carried out. The results in
Figure 18 show that the robot system can accurately reproduce the preset massage action patterns: (1) According to the force–displacement coupling data of the second study, the vast majority of the pressing forces around 20 N reach intolerable intensity for the subjects. Therefore, it is required that the pressing manipulation provides an output force of 0–20 N. As shown in
Figure 18a, the vertical pressure regulation of 0–20 N can be achieved in the pressing manipulation mode. (2) The vibrating manipulation mode generates a mechanical wave output of 0–20 Hz. (3) The pushing manipulation can perform a planar reciprocating motion on the track. (4) The kneading mechanism can complete a rotational kneading motion of ±31.89°. (5) The pinching mechanism can achieve a symmetrical opening-closing motion to simulate the double-finger pinching manipulation. The experimental data confirm that this platform meets the kinematic requirements of diversified manipulations for abdominal massage through motion-coupling modeling. The smooth switching between various modes verifies the real-time response characteristics of the control system, laying a technical foundation for subsequent clinical efficacy research.
- (2)
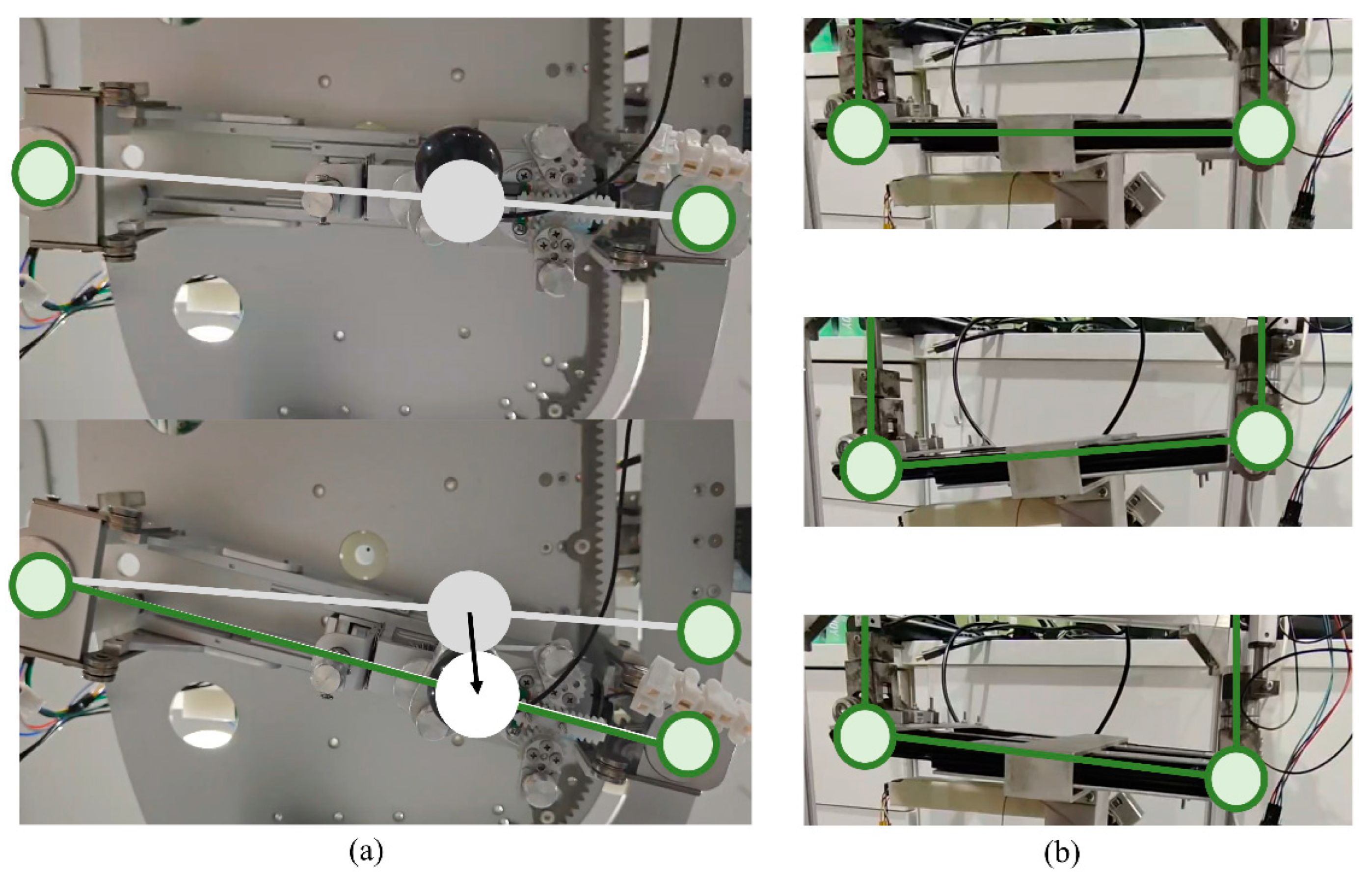
Verification Experiment of Massage Angle Adjustment
By using the push-rod motor in the middle-layer parallel structure and the massage angle control algorithm, the projection position and tilt angle of the massage actuator can be flexibly adjusted. This enables the massage force to act on the abdominal target points at different angles according to actual needs, thus adapting to the complex physiological structure of the human abdomen and diverse massage requirements, and improving the massage effect. In order to adapt to the non-planar surface-specific characteristics of the abdomen, this study conducts a special test on the spatial attitude regulation ability of the massage actuator (as shown in
Figure 19b).
Based on the configuration design of the parallel mechanism, the middle-layer adjustment module realizes the dynamic pose adjustment of the end-effector through the integrated control of multi-motor collaborative driving and the inverse kinematics algorithm. According to the characteristics of the track layer of this massage robot, the distance between the inner and outer fulcrums and the stroke range of the vertical push rod motor determines the adjustment range of the end angle. This depends on the setting of the structural parameter dimensions. The actual angle shown here is in the proportion of this design scheme and is only for reference to the verification results of the angle adjustment function. According to the design parameters of this abdominal robot, the angle adjustment results in
Table 6 can be obtained. By using the position control effect of the robot, it is verified that the maximum angle adjustment accuracy under no-load conditions can be ±17°.
- (3)
Verification Experiment of Force Output Steady-state Characteristics
To verify the output force stability of the robot, this experiment adopts an admittance control-based force–position hybrid control strategy to conduct mechanical tests on a static simulated prosthesis. The test scenario is shown in
Figure 20a. The actual collected mechanical curve is highly consistent with the expected curve in trend (as shown in
Figure 20b), and the error can be stably controlled within 0.2 N. This result indicates that the force–position hybrid control strategy based on admittance control is effective. The robot can accurately track the expected force curve during the massage process, achieving precise control of the magnitude and change the trend of the massage force, ensuring the stability and accuracy of the massage intensity and laying a solid foundation for providing stable and effective massage services to patients in practical applications.
4.1.2. Dynamic Force Tracking Test Experiment
In response to the performance verification requirements of the abdominal massage robot system, this study constructed an experimental platform containing static/dynamic simulated tissues and carried out force-tracking performance tests on targets with different biomechanical properties. The experimental platform uses a sponge composite material that mimics the human abdomen as a static prosthesis model, and at the same time constructs a dynamic prosthesis system that can simulate the characteristics of respiratory rhythm based on inflatable airbags.
- (1)
Static prosthesis dynamic target force tracking experiment
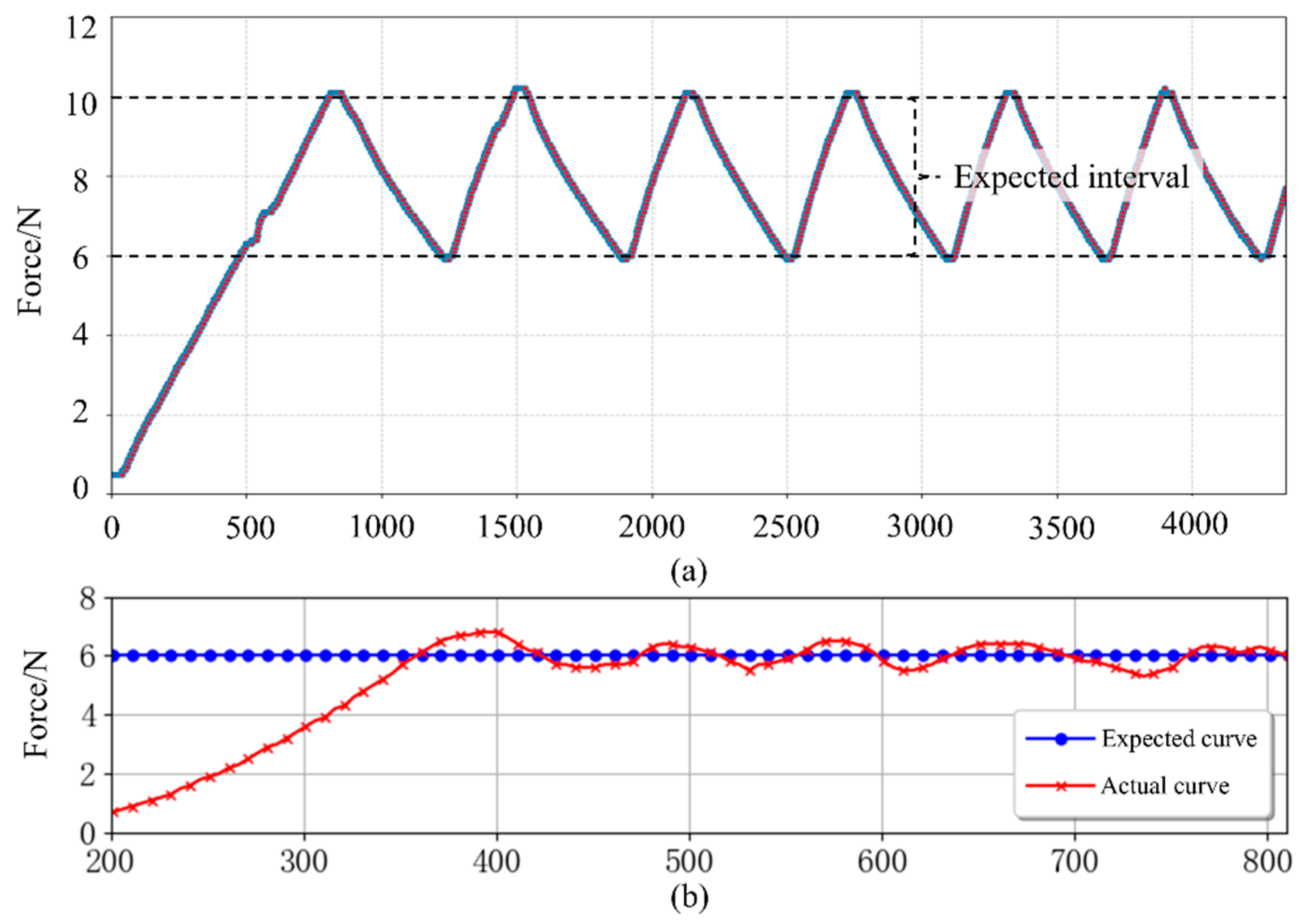
Based on the differences in biomechanical characteristics between the pressing method and the vibrating method in massage mechanics, this study specifically conducts a quantitative analysis of the periodic force application characteristics in the sagittal plane. The vibrating method is mainly manifested as reciprocating motion with a fixed displacement amplitude, while the pressing method has periodic dynamic force output as its core characteristic. To verify the system’s tracking performance for dynamic force commands, the experiment sets the boundary of periodic force parameters (
,
) to construct a dynamic force-tracking task. The experimental data show (
Figure 21a) that the system can achieve a steady-state accuracy of the 0.2 N level within the set dynamic force range of 6.0–10.0 N, verifying the superior performance of the actuator in time-varying force control.
- (2)
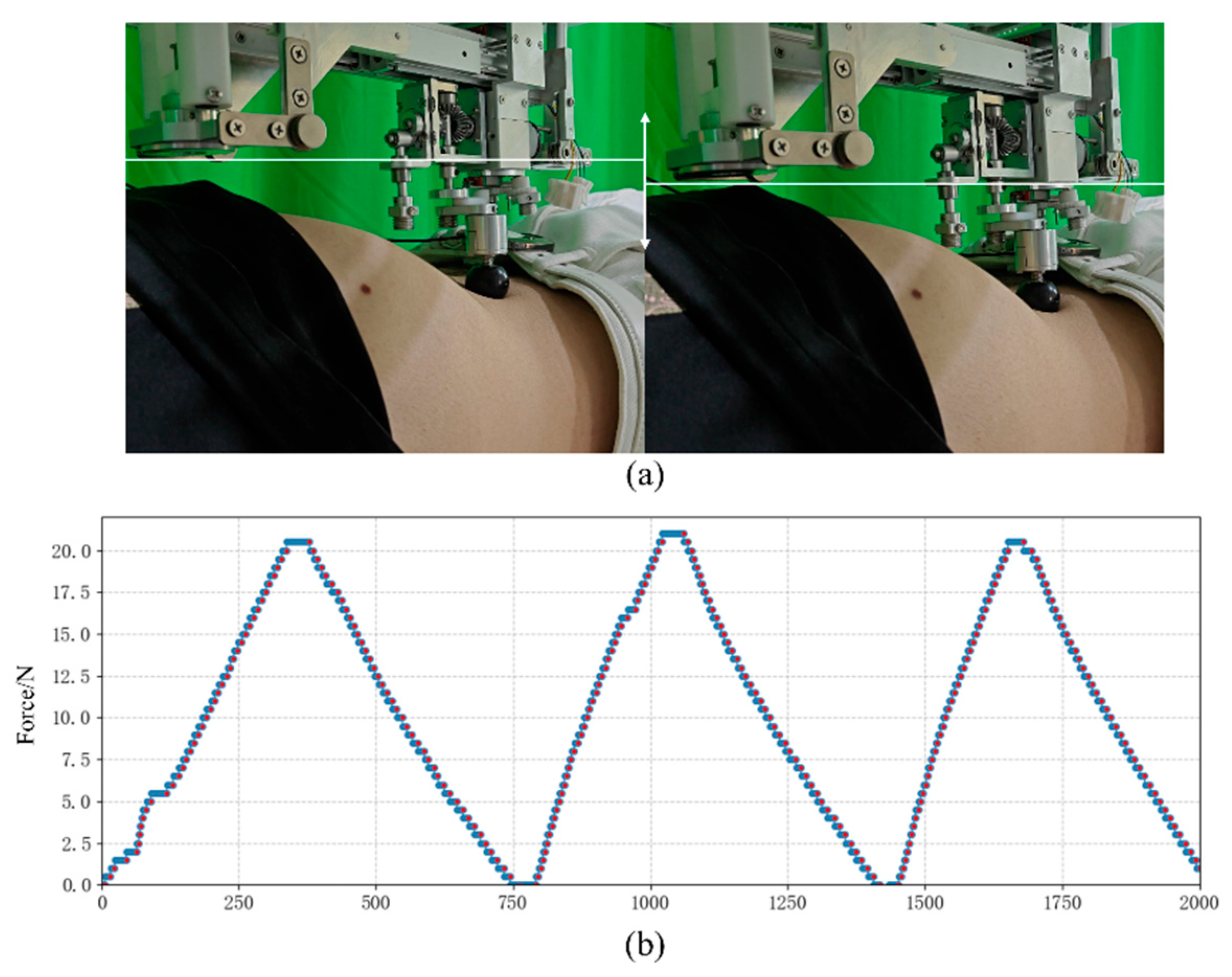
Dynamic Prosthesis Constant Force Tracking Experiment
To simulate the tissue deformation characteristics caused by human respiratory motion, this study innovatively constructed a pneumatic coupling experimental system. The airbag prosthesis is driven by an integrated two-way air pump (with adjustable inflation/extraction rate) to accurately reproduce the respiratory rhythm with a 4 s cycle in the resting state (2 s for the inspiratory phase and 2 s for the expiratory phase). Under this dynamic deformation condition, a constant force-tracking experiment was carried out. The results show (
Figure 21b) that the system can effectively compensate for tissue displacement disturbances and maintain a dynamic force control accuracy of the 0.8 N level. The periodic force fluctuations presented by the experimental data are highly consistent with the preset respiratory rhythm, confirming the robustness of the control system against external disturbances.
This study systematically verified three core performance indicators of the abdominal massage robot through a dual-modal experimental framework: ① diversity of massage modes; ② spatial coverage of target point positioning; ③ force steady-state characteristics in dynamic interaction scenarios. The experimental data show that the system has clinical-level control accuracy within the force range of 0–20 N, and its maximum positioning error does not exceed ±2.0 mm. These research results not only provide a quantitative basis for the biomechanical adaptability of the abdominal massage robot but also lay a key technical foundation for subsequent preclinical research.
4.2. Experimental Research on Abdominal Massage Robot Massage for Healthy People
To verify the effectiveness of the control strategy, a healthy subject was recruited to conduct an interaction experiment with the massage robot. The specific experimental process is as follows:
- (1)
Experimental design and implementation
Before the start of the experiment, the personal biometric data was first calibrated, and the basic information of the volunteer was collected and combined with the positioning method proposed in the “Identification Model of Key Points of Abdominal Action” [
27]. The massage target points were then accurately marked with an erasable liquid pen.
Implementation process of force interaction control: Control the robot to apply pressing force on the target action point of the volunteer until the volunteer feels discomfort. The experimental process is shown in
Figure 22. Fit the variable-stiffness physical model (Formula 10) based on the human body force–displacement coupling data collected by the robot. Select any value within the range from slight to intense feeling as the desired curve. Select one of the multiple key action points on the volunteer’s abdomen to perform constant force control of three control strategies and dynamic force tracking control within three different ranges. Then, select four adjacent action points of the volunteer to perform continuous constant force pressing control. Control the end effector of the robot to perform dynamic pressing on the four action points along the preset trajectory. The system synchronously collects the data of the distributed pressure sensors to establish the force-displacement coupling database of the subject. After completing the pressing task at the current point, the rotary motor Motor1 and the push rod motor Motor4 will work together to drive the end massage head to move to the next point. During the movement, the push rod motor Motor2 and the push rod motor Motor3 will continuously control the pressing force and maintain the current force magnitude, while tracking the desired force at all points. After the massage is completed, output the pressure sensor information of all points and fit the curve. Each change in the figure represents the change in force at each massage point, with a total of four points.
- (2)
Verification of Dynamic Control Performance
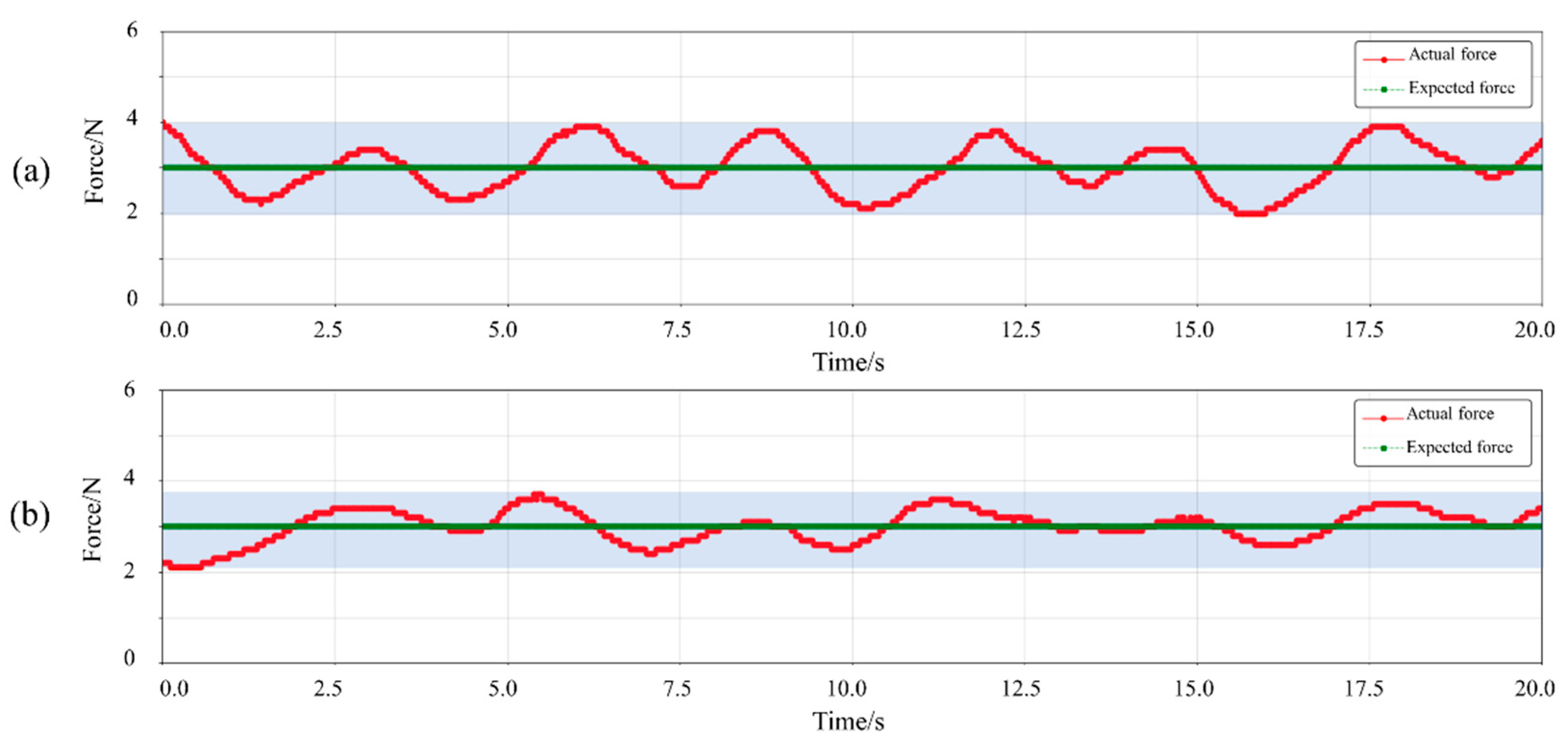
The experimental results in
Figure 23 demonstrate the constant force tracking performance during the volunteer’s massage process, showing the time-domain characteristics of displacement (pressing depth) and interaction force. In the fuzzy adaptive admittance control strategy [
27] mentioned in the original paper, the mean absolute error between the actual output force and the desired curve is 0.43 N, and the maximum instantaneous error is 1.0 N (half of the blue-shaded range in
Figure 23a). In the biomechanical adaptation control strategy integrating the variable-stiffness physical model, the mean absolute error between the actual output force and the desired curve is 0.29 N, and the maximum instantaneous error is 0.9 N (half of the blue-shaded range in
Figure 23b).
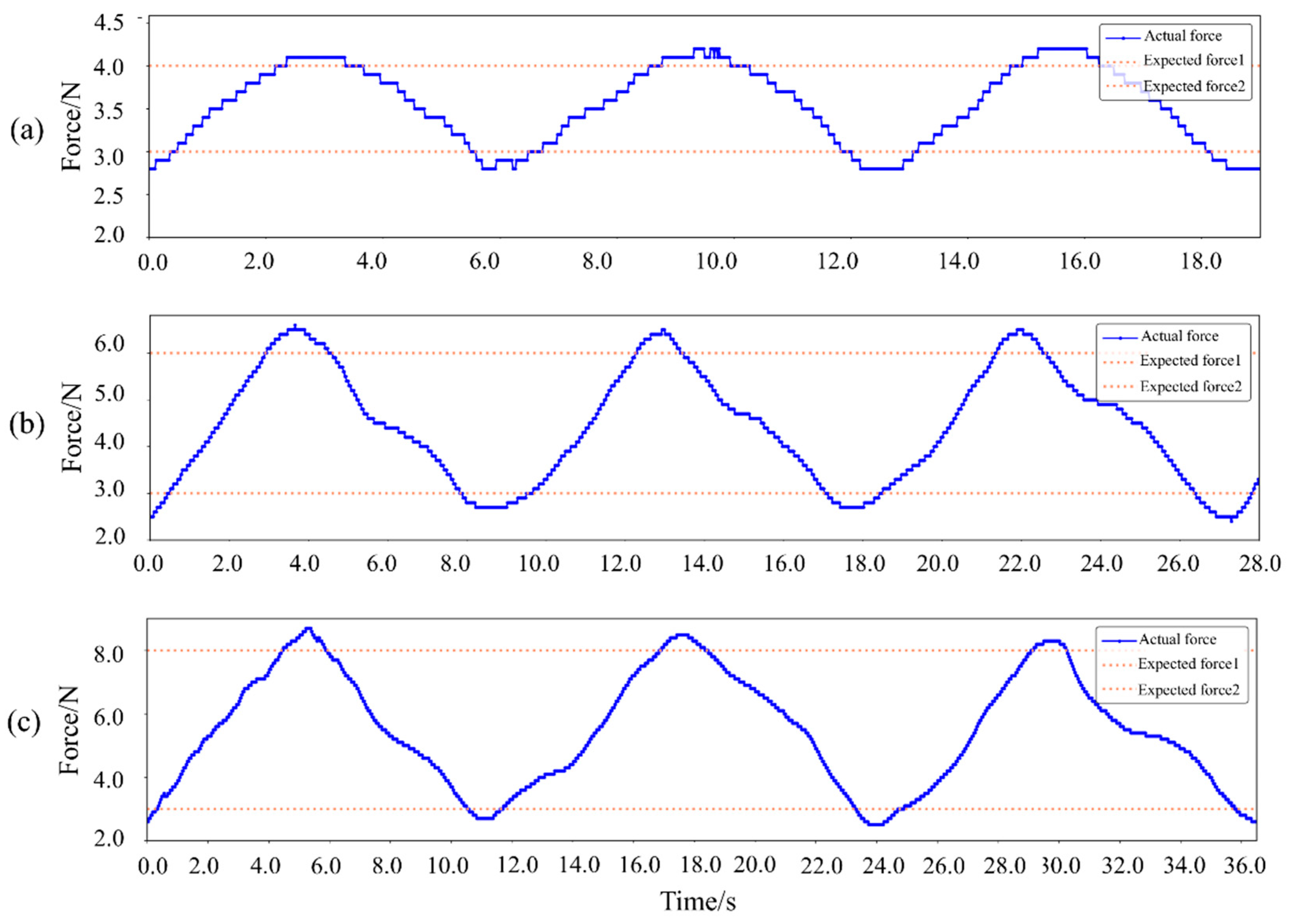
It can be seen from
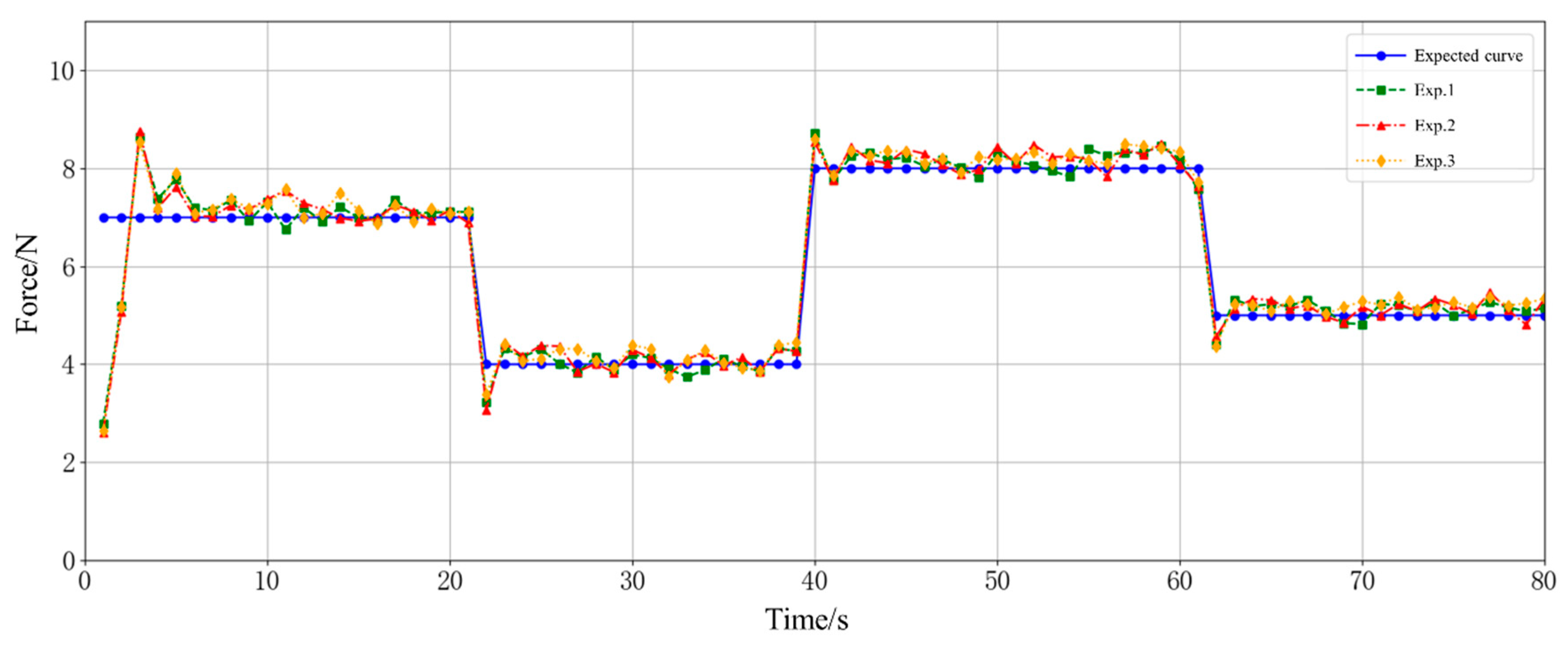
Figure 24 that within the range of 3.0–4.0 N, the overshoot of dynamic force tracking is 0.2 N; within the range of 3.0–6.0 N, the overshoot of dynamic force tracking is 0.5 N; within the range of 3.0–8.0 N, the overshoot of dynamic force tracking is 0.7 N.
From the experimental results in
Figure 25, the continuous constant force tracking performance of the four points during the massage process for the volunteers can be obtained. The average absolute error between the actual output force and the expected curve is 0.38 N, the maximum instantaneous error is 0.8 N, and the regulation time is ≤0.3 s. The subjects’ subjective feedback indicated that the applied force was stable and perceived as between a slight and a strong sensation. No skin erythema or mechanical damage occurred.
The above experimental results verify that the end massage actuator of the massage robot can closely track the preset massage force curve, demonstrating excellent tracking accuracy and response speed and ensuring the efficient execution of the rehabilitation massage task.
5. Discussion
This study aims to address the deficiencies of existing abdominal massage robots and conducts systematic improvements from three aspects—mechanical structure, control strategy, and experimental verification—forming a set of safe and efficient abdominal massage robot systems. In terms of mechanical structure design, a dual-platform collaborative architecture is proposed. Through the integration of a three-degree-of-freedom mobile platform and a six-degree-of-freedom core massage platform, rapid positioning of the supine human abdomen and multi-modal manipulation can be achieved. The three-degree-of-freedom mobile platform adopts a C-type topological framework and an omnidirectional mobile solution, which solves the stability defect of traditional universal wheels, with a positioning accuracy of ±2 mm. The core message platform integrates five manipulation methods, namely pressing, pushing, vibrating, kneading, and pinching, through a serial-parallel hybrid structure. Among them, the three-manipulation-on-demand parallel structure improves the flexibility and space efficiency of the end-effector through bevel gear commutation and quick-release design, meeting the needs of different clinical scenarios. In the research of control strategy, based on the biomechanical characteristics of the abdomen, an admittance-PID—PID hybrid control strategy integrating a variable-stiffness physical model is constructed. Through human experiments, the basis for dividing the pressing force into light, medium, and heavy levels is determined. It is found that individual differences have a significant impact on the distribution of sensory points, and the force needs to be adjusted individually. The simulation and experimental results show that this strategy can effectively control the massage force error within 0.2 N, and the dynamic tracking accuracy reaches the 0.8 N level, significantly improving the mechanical adaptability of the robot and safety of abdominal soft tissues. The prototype test verifies the reliability and practicality of the system. The static prosthesis experiment shows that the robot can achieve a vertical pressure adjustment of 0–20 N, a kneading rotation of ±31.89°, and a symmetrical pinching opening and closing, with the steady-state error of force output controlled within 0.2 N. In the dynamic prosthesis experiment, the system can compensate for the tissue deformation caused by the respiratory rhythm and maintain a dynamic force control accuracy of the 0.8 N level. The human experiment further shows that the optimized control strategy of the integrated variable-stiffness model has an average absolute error of 0.29 N in constant-force tracking, and no discomfort or injury to the subjects is observed, verifying the clinical feasibility of the system. In summary, this study provides key technical support for the engineering application of abdominal massage robots. Its multi-modal manipulation generation, precise positioning, and safe force-control capabilities are expected to promote the intelligent development of the rehabilitation and physiotherapy field.
This study establishes an adaptive force control framework for abdominal massage robots, integrating a variable-stiffness model () to achieve precise force tracking (0.2–0.8 N error); several limitations require resolution for clinical translation:
Synergizing Adaptive Control with Clinical Scalability: The stiffness-based force adaptation (parameterized by and ) validation relies on a single-subject experiment, insufficient to address anatomical heterogeneity (e.g., fat layer thickness, muscle tone). Future work must expand to multi-center trials across diverse populations, integrating multimodal sensing (EMG, pressure distribution) to refine the variable-stiffness model to better characterize the relationship between the massage interaction force and the massage pressing depth. This refined variable-stiffness model provides a crucial biomechanically grounded foundation for force prediction and control. This will enhance the model’s capacity to initialize parameters for impedance learning algorithms, accelerating safe adaptation in dynamic abdominal environments. The stiffness-based force adaptation values offer physically meaningful priors for initializing variable impedance controllers when interacting with unknown or varying abdominal tissues, helping to address challenges highlighted in research on ‘Impedance learning for human-guided robots in contact with unknown environments.
Toward Multi-DOF Collaborative Manipulation: Current control focuses on single-DOF pressing, neglecting composite techniques (e.g., pressing-to-kneading transitions). Here, Dynamic Movement Primitives (DMPs) can provide a critical solution: by encoding and reproducing therapist-demonstrated multi-dimensional trajectories (position, orientation, force profile transitions), they enable reproducible multi-technique sequences while preserving force customization. Crucially, our proposed biomechanical adaptation control strategy (variable-stiffness model + admittance-PID) can be embedded within the DMP framework. Coupling DMPs with our force control strategy ensures precise and compliant force tracking (<20 N safety threshold) during the execution of complex trajectories, even under respiratory undulations. This integrated approach aligns with the goals of ‘Dynamic motion primitives-based trajectory learning for physical human–robot interaction force control’, aiming to achieve both trajectory fidelity and safe, adaptive force interaction. To operationalize this, tactile-EMG-pressure sensor fusion is essential to quantify “comfort” and optimize force-delivery kinematics.
Closed-Loop Personalization via Physics-Guided Learning: The machine learning-based force personalization synergizes with physics-guided impedance tuning. Initializing impedance parameters using tissue-specific and values derived from our model reduces exploration risk and enhances convergence speed for online impedance learning in unknown abdominal environments, as explored in impedance learning research. Concurrently, large-scale clinical data will train user-specific biomechanical signatures, enabling the following: (a) real-time impedance adaptation during physiological changes (e.g., breathing) leveraging the predictive capability of the variable-stiffness model and (b) long-term optimization of personalized DMP trajectories and impedance/admittance control parameters via reinforcement learning based on user feedback and physiological responses.
Cross-Domain Applicability: The robustness and adaptability of our core framework—combining a biomechanically informed variable-stiffness model with stable admittance-PID force control—for dynamic force control extends beyond massage applications. Rehabilitation Robotics: DMP-guided limb therapy with stiffness-modeled force constraints for stroke rehab. Surgical Palpation: Tumor detection probes using and parameterized stiffness mapping and impedance learning for safe interaction. Human–Robot Collaboration: Manufacturing tasks (e.g., curved surface polishing) via DMP-admittance force coupling.
6. Conclusions
This research focuses on three aspects of optimization for the abdominal massage robot system: mechanical structure integration, control strategy optimization, and experimental system verification. Based on a six-degree-of-freedom platform, the system enables programmable combinations of five massage techniques, namely, pressing, pushing, kneading, vibrating, and pinching. Innovatively, a variable-stiffness physical model based on abdominal biomechanical characteristics is embedded in the massage force interaction control loop. The experimental verification results show that the interaction force error of the system is controlled within 0.8N, achieving high-precision and stable force control interaction performance. Follow-up research will comprehensively improve the performance and clinical application reliability of the abdominal massage robot system from three dimensions: constructing a personalized massage force model based on machine learning, integrating multi-modal sensors to optimize the comfort control strategy, and conducting multi-center clinical experiments to expand the sample size for validating effectiveness.


 ,
, 









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}