Abstract
With the aging society in Japan, the number of elderly people residing in elderly facilities is increasing. In previous study, we developed a transfer assistive device designed to aid the elderly in transferring from the bedroom to the bathroom. Additionally, the device assists the elderly with standing and sitting to facilitate independent toileting activities. We verified that, throughout the entire transfer movement, the lumbar burden on caregivers remained below 3400 N. In this study, based on quantitative evaluation indices of transfer movements, the relationship between the lumbar burden on caregivers and factors such as psychological anxiety or cognitive impairment in the elderly during the use of a transfer assistive device was elucidated through motion analysis. We developed a control algorithm for the human–machine collaborative transfer system with the aim of alleviating the strain on the caregiver’s lower back while ensuring the elderly can use the device with peace of mind. The practicality of the control algorithm was verified.
1. Introduction
Recently, due to the rapid aging of Japanese society, the proportion of people aged 65 and older (aging rate) has reached 29.0% [1]. This trend has been accompanied by a continuous increase in the number of residents in elderly care facilities, significantly impacting the working environment of caregivers and the quality of life (QOL) for elderly residents in these facilities [2]. Reports indicate that approximately 70% of back pain among caregivers is caused by movements associated with transferring elderly individuals. Therefore, alleviating the burden on caregivers’ lower backs caused by transfer movements is crucial to reduce the risk of back pain [3]. At the same time, the QOL for the elderly should not be overlooked. Facilitating communication, movement, and toileting for the elderly is necessary to enhance their overall well-being. Assisting the elderly in transferring from their living spaces to the bathroom is crucial. When the elderly refrain from using diapers and instead use the toilet for excretion, it can activate the autonomic nervous system through the defecation reflex. Additionally, adopting a seated position can improve constipation.
However, assisting in transfers is the caregiving action associated with the highest risk of lower back pain for caregivers. According to a report by the Ministry of Health, Labour and Welfare, guidelines for preventing lower back pain in the workplace recommend avoiding manual lifting during transfers that require full assistance. Instead, the use of transfer assistive devices is advocated for assistance [3].
Considering the autonomous defecation behavior in the elderly, facilitating smooth execution is essential. In the Japanese market, various transfer assistive devices have been developed to aid elderly people in transitioning from a seated to a standing position, thereby enhancing their quality of life. For instance, the Hybrid Assistive Limb (HAL) [4] is a device designed to assist with bodily movements. Although effective, its usage may impose additional pressure on the upper limbs and trunk of the elderly, particularly challenging for those with impaired arm or trunk function. Another device, Ai ijo-kun [5], allows elderly individuals to sit down autonomously without external assistance by automatically adjusting the seat height, meeting the needs for independent usage. However, for elderly people with conditions such as Parkinson’s disease or cognitive impairments, the absence of caregiver physical support might limit their ability to use such devices [6]. Therefore, the presence and assistance of caregivers in stabilizing the elderly while operating these transfer assistive devices are crucial.
Moreover, literature reviews on personnel transfer assistive systems predominantly focus on ceiling- and floor-mounted hoists [7], highlighting the risk of caregiver injury during use but seldom exploring the impact on the elderly themselves. Blaauw compared a novel robotic assistive transfer device with the traditional clinical care standard (Hoyer advance) [8] and measured muscle activity among caregivers during use, introducing an ergonomic method to reduce injuries for both caregivers and wheelchair users during transfers. However, the research did not fully account for the fact that wheelchair users are often elderly, necessitating not only physical support during device use but also consideration of upper limb impairments and other complex factors. Krishnan developed a self-transfer system and successfully moved participants from wheelchair to chair in less than a minute with less effort [9], demonstrating technical feasibility. Nonetheless, for elderly users, the presence and physical support of caregivers remain critically important when using automated devices. Ulrey’s study on the Bending Non-Demand Return (BNDR) weight transfer device (WTD) [10] showed a significant reduction in lumbar erector spinae muscle activity during bending motions, providing an effective intervention for caregivers who frequently engage in such postures. Yet, for caregivers tasked with assisting the elderly in transfers, avoiding lumbar bending is nearly impossible.
In this context, the method of assisting the elderly in stabilizing their bodies becomes crucial. Touching their bodies to provide support not only helps the elderly maintain balance but also facilitates emotional communication and psychological well-being. An increasing body of research suggests the positive impact of physical touch on health, including lowering blood pressure, increasing oxytocin levels, and improving sleep [11]. Furthermore, touch has been found to alleviate stress, which is particularly important during the global COVID-19 pandemic [12,13]. Meanwhile, despite the development and market availability of a large number of transfer assistive devices, the adoption rate of these devices in existing elderly facilities remains relatively low, as indicated by the findings in report [14] on the hindering factors of introducing transfer assistive devices. The majority of transfer tasks still heavily rely on manual assistance. The report explicitly identifies reasons for the non-adoption of transfer devices, including concerns about space occupancy and inconvenience in usage. Therefore, developing a human–machine collaborative transfer system that addresses practical needs, aims to minimize equipment footprint, and allows manual touch for caregiving actions during device usage is worth considering.
In this study, we propose a human–machine collaborative transfer system suitable for elderly residents with upper limb and torso functional impairments. The system is designed to meet practical needs and alleviate the lumbar burden of caregivers during the transfer process from the living space to the bathroom. This study primarily discusses two key points as follows:
- Emphasis is placed on the evolution of equipment specifications proposed in previous studies [15,16]. Through an investigation of elderly care facilities, we ascertained that transfer actions by caregivers predominantly involve a frontal embrace, addressing scenarios where a single caregiver assists a person in using the toilet. Design requirements for the equipment include “assistance for the user to sit up” and “wheelchair usability in accessible toilets”, considering aspects such as “applicable size”, “elimination of rotational movements”, “manual movements”, and “pressure-free transfer on the upper limbs and torso”.
- Detailed discussion revolves around the comprehensive consideration of the caregiver’s lumbar burden factors and corresponding control methods for reducing lumbar stress in the human–machine collaborative transfer system. Particularly noteworthy is the full consideration in system design of physical contact with the cared-for elderly person, aiming to alleviate their psychological burden and enhance acceptance of transfer assistive devices. Simultaneously, emphasis is placed on ensuring that the lumbar burden on caregivers during transfer movements does not exceed the benchmark of 3400 N.
Specifically, Section 2 provides a detailed exposition of the specifications and identified issues of the transfer assistive device developed in previous studies. In Section 3, the control algorithm of the collaborative transfer system is discussed, with a particular focus on setting control objectives, designing control systems, and establishing a rigid link model. Section 4 introduces quantitative evaluation metrics based on the analysis of caregiver transfer movements, encompassing experimental design, results, discussions, and validation of the system’s effectiveness. Finally, Section 5 presents the conclusions drawn from this study.
2. Positioning of Existing Research and This Research
We conducted on-site surveys of nine elderly care facilities, extracting constraints related to facility environments and equipment requirements for facility use. Subsequently, by utilizing a three-dimensional motion measurement device, we quantitatively assessed the transfer movements of caregivers, extracting equipment requirements to alleviate the lower back burden of caregivers. The equipment specifications, as illustrated in Figure 1, are reported in [16].
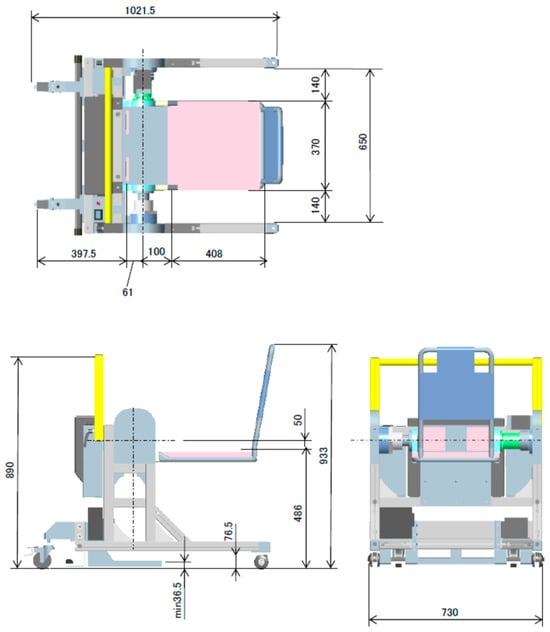
Figure 1.
Three views of proposed transfer assistive device (Unit: mm).
2.1. Proposed Device Mechanism
Table 1 summarizes the mechanism of the extracted device functions and constraints. The device mechanism is illustrated in Figure 2a.

Table 1.
The function and mechanism of proposed transfer assistive device.
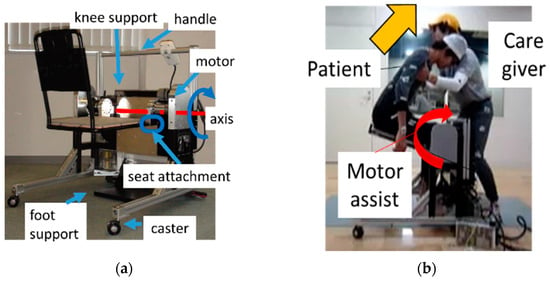
Figure 2.
Proposed transfer assistive device: (a) appearance of the proposed device; (b) assist control methodology.
As a distinctive feature of the transfer assistance device, we proposed a mechanism designed to add torque around the knee joint of the elderly person to compensate for their weight. As shown in Figure 2b, caregivers perform assistive operations while receiving assistance from the device (assist control methodology). A torque is applied by a servomotor around the knee joint of the elderly person. The rated torque is set to 250 Nm to allow the elderly person to weigh up to 80 kg. We implemented a control program in the servo motor controller’s internal program, which obtains output torque information based on the motor’s position, rotation speed, and servo motor current value from the encoder’s output and processes it with the controller. Control is executed by issuing commands to the motor based on current or pulse waves. Additionally, recording is performed by outputting servo motor information obtained from the controller to the notebook computer.
2.2. Existing Problems
In the previous practical experiments [16] of our study, we employed three control methodologies (manual assistance, automatic lifting, assisted rising) to assess the operation of the developed transfer assistive device. In comparison with the method of simply helping the elderly stand up or sit down by human power without any assistive device (manual assistance), we observed that the elderly person could sit on the device and the device could run automatically (automatic lifting) without the assistance of caregivers. During this time, there was no burden on the caregiver’s waist. However, for the elderly, especially those with cognitive disorders, allowing them to sit on the device without anyone for support or touch might induce anxiety [6] and even lead to panic, hindering the normal use of the proposed device.
As mentioned in the last part of Section 1, we have fully considered factors such as the psychological resistance of the elderly when using transfer assistance devices and the benchmark value of the caregiver’s lumbar burden not exceeding 3400 N in the design and development of a human–machine cooperative transfer system. Under the premise of ensuring that the elderly can use the device safely and securely, the caregivers touch the body of the elderly, and at the same time, the device itself provides control assistance at an appropriate angle, thereby effectively reducing the burden on the caregiver’s waist. This design fully embodies the concept of human–machine cooperation, aiming to achieve care and protection for both caregivers and the elderly.
In summary, this study quantitatively explores the relationship between the transfer assistance movements of caregivers during transferring and their lumbar burden using a three-dimensional motion measurement device. We describe the development process of a collaborative transfer system that fully considers the lumbar burden of caregivers and the cognitive factors of the elderly and adopts the mechanisms and functions of the already-developed transfer assistance device.
3. Control Algorithm for Collaborative Transfer System
Based on the proposed device requirements, “reducing the lumbar burden of caregivers when assisting the elderly from a sitting to a standing position” is established as a necessary function of the control algorithm. The prerequisite for the operation is “the elderly person is always touched by the caregiver”. Therefore, we propose a control algorithm that considers the relationship of lumbar burden factors to alleviate lumbar burden while caregivers assist the elderly person in transferring. The evaluation of lumbar burden will be detailed in Section 4.1, and the quantitative requirement for reducing lumbar load is set as “the lumbar disc compression force of caregivers should not exceed the evaluation reference value (3400 N)” (ideal conditions) [17].
3.1. Control System
The overview diagram of the collaborative assistive algorithm is shown in Figure 3. The nominal model is for calculating a target value based on Equation (1) in Section 3.2.
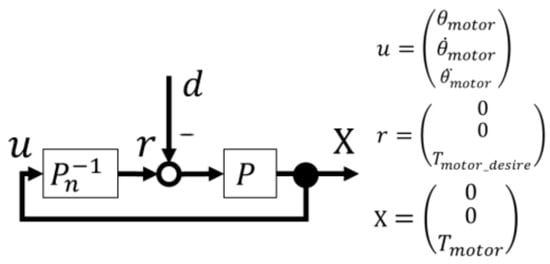
Figure 3.
Block diagram of the proposed collaborative assistive algorithm. represents the input, is the command value, is the output, is the disturbance, represents the plant (caregiver, elderly, motor, seat), and is the nominal model of the plant that determines the target value . The variables , , and represent the rotation angle, rotation angular velocity, and rotation angular acceleration of the motor, respectively. is the motor torque, and is the motor torque that satisfies the ideal conditions.
Figure 4 illustrates the flow of the proposed control algorithm. The control system consists of two processes: the Calibration Process and the Motion Control Process. In the Calibration process, the motor torque to maintain the elderly person in the seated state is obtained from the measured motor current. By comparing this value with the estimated holding torque in the range of heights below 2 m, the height h is set as the elderly person’s height using the nearest value. In Motion Control process, motor operation control is performed. Simply raising the seat automatically can be considered a motor operation control method to reduce the caregiver’s lumbar burden. However, to support the elderly in standing up freely at the caregiver’s timing while holding them, it is important for the device to provide collaborative assistance by responding to the caregiver’s force input, not just by automatically raising the seat. Considering the ideal condition of reducing the caregiver’s lumbar burden, we propose modifying the operation based on the caregiver’s trunk forward tilt angle . A threshold for is determined from the quantitative evaluation index of the lumbar burden factor, as detailed in Section 4.3. When is in the range of or above, the automatic lift algorithm (Lift up) is implemented. On the other hand, when is below , the collaborative assistive algorithm (Torque assist) is applied.
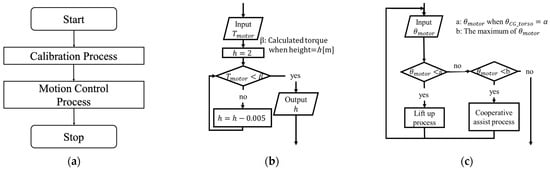
Figure 4.
Block diagram of the proposed control system. (a) System flow; (b) calibration process; (c) motion control process.
3.2. Setting up a Rigid Link Model
The control model Equation (1) is derived from the motion equation around the elderly’s knee joint, summing the inertia term , gravity term , and friction term . It calculates by subtracting the desired caregiver torque and the elderly person’s exerted torque to satisfy the ideal conditions.
Figure 5 illustrates the rigid body link model and variables used in the collaborative assistive algorithm. In the derivation of Equation (1), a two-link model is employed for the elderly person’s thigh, seat, and upper torso. Organizing the necessary variables for each term in the model equation, variables such as , , , the elderly person’s upper body joint angle , and the caregiver’s trunk forward tilt angle are identified as essential. While motor-related variables are sequentially obtained, other variables need to be set.
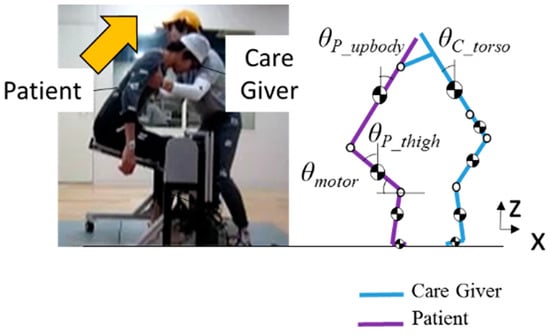
Figure 5.
The link model of plant.
Therefore, regarding the configuration of joint angles and , an experimental study in Section 4.1 established a similar trend between the elderly person’s thigh angle for four subjects. Based on the experimental values of the subjects, an approximate formula for joint angles was formulated as shown in Equations (2) and (3). Assuming that the seat and the elderly person’s thigh move together, the value of the elderly person’s thigh angle is approximated as 90 − (). Through Equation (3), the setting of for to be is determined.
where 0.0011, , , , , and .
The estimated segment weight and estimated moment of inertia of the human body were referenced from [18], and the segment length of the human body was referenced from [19].
4. Experimental Results and Discussion
In last section, we introduced a control algorithm aimed at satisfying ideal conditions and reducing the lumbar burden of caregivers. In this section, our focus is on quantitatively understanding the lumbar burden factors of caregivers during the transfer operation by implementing control objectives that fulfill the ideal conditions. This allows us to obtain control indices and target values for the transfer movement. Through experiments, we define a threshold for the caregiver’s trunk forward tilt angle to facilitate the seamless transition between the automatic lift algorithm and the collaborative assistive algorithm in the developed human–machine collaborative transfer system.
4.1. Establishment of Lumbar Burden Evaluation Method and Consideration of Caregiver’s Lumbar Burden Factor
The lumbar pain factor was set at 3400 N according to NIOSH for the lumbar intervertebral disc compression force [17]. In the motion analysis, the lumbar disc compression force was estimated, and the lumbar burden was evaluated using Equation (4) proposed by Yamazaki et al. [20]. , , , and represent the forward bending moment, side bending moment, turning moment, self-weight component, and external force component applied to the center of the lumbar joint. The rigid link model used divided the human body into nine parts: the head, trunk, upper limbs, waist, both thighs, both lower legs, and both legs. Additionally, as a characteristic of the caregiver’s standing support movement obtained in the experiments in Section 4.2, it was assumed that the elbow joint angle of the caregiver did not change significantly during the movement due to the immobility of the upper limbs. Consider a link that integrates the trunk and upper limbs.
The transfer movement by one caregiver using the front holding method is two-dimensional [18]. Therefore, the dominant term in Equation (4) is the forward bending moment on the caregiver’s waist. Equation (5) presents the expression for calculating the forward bending moment .
represents the caregiver’s upper limb exertion force, is the moment arm (vector from the waist joint to the gripping point), is the combined weight of the caregiver’s head and upper torso, is the combined length of the caregiver’s upper torso and head, and is the caregiver’s trunk forward tilt angle. As the transfer movement is a relatively slow motion [20], we consider excluding dynamic terms in this Equation (5). In this equation, the variables that change during the movement are , , and . Therefore, these three variables are set as the lumbar burden factors.
4.2. Experiment: Extracting Lumbar Burden Factors in Caregiver’s Transfer Movements
An experiment was conducted to extract the timing of the increase in lumbar burden and the lumbar burden factor when the caregiver assisted the elderly person in standing up under the condition of knee fixation.
The subjects included four male caregiver workers without back pain disorders (D1 to D4, including three physical therapists and one social worker: height 1.76 ± 0.03 m, weight 69.8 ± 2.9 kg) and two students (E1, E2: height 1.72 ± 0.03 m, weight 65.0 ± 4.3 kg). The experiment utilized a three-dimensional motion measurement device, a floor reaction force plate, infrared reflective markers, and a mock-up as shown in Figure 6a, allowing the elderly person to sit down with knee fixation functionality and a treading force sensor. The experimental setup is illustrated in Figure 6b. The participants performed the standing support movement using the front holding method for the simulated elderly person, and the movement was recorded. To simulate characteristics of the elderly person, the simulated elderly were instructed to relax their entire body while maintaining a seated position.
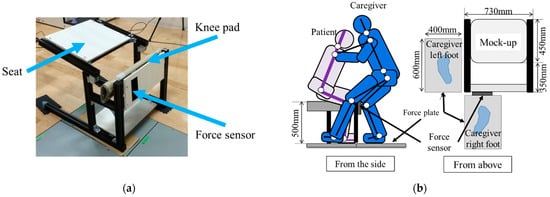
Figure 6.
The experimental setup included the use of a mock-up, as well as schematic diagrams illustrating the subjects’ posture, placement of items, etc.: (a) appearance of mock-up; (b) position of subjects and mock-up.
4.2.1. Results
This experiment was conducted with the approval of the University of Tokyo Life Science Committee. The experimental results are presented in Figure 7 and Figure 8.
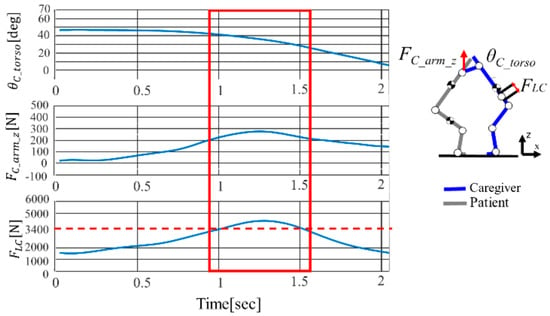
Figure 7.
Representative of experimental caregiver’s D1 relationship graph of the trunk forward tilt angle , upper limb exertion force , and lumbar intervertebral disc compression force when helping the elderly person to stand up with fixed knees.
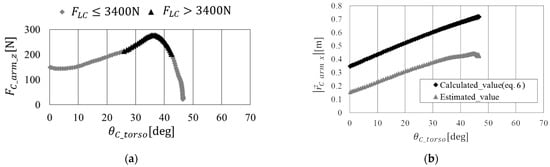
Figure 8.
Representation of the relationship between the lumbar burden factors of caregiver D1 when the knee of the elderly person is fixed. (a) Relationship between and ; (b) relationship between and .
The duration of the movement was defined as the time from when the caregiver began to lift the trunk until the elderly person was fully upright. The average duration of the movement was 2.76 ± 0.30 s. Figure 7 illustrates the time-series responses of the caregiver’s trunk forward tilt angle , the caregiver’s upper limb exertion force , and their lumbar intervertebral disc compression force during a standing assistive movement for representative participant D1 (height 1.72 m, weight 71.0 kg). As the standing assistive movement progressed over time, the of the caregiver decreased. An increasing trend in was observed simultaneously with the increase in . Moreover, at the moment indicated by the red square in Figure 7, exceeded the evaluation criterion of 3400 N, indicating a heightened risk of lumbar pain during the standing assistive movement.
4.2.2. Discussion
In order to understand the relationship between lumbar factors, we depicted the relationships between and as well as and in the standing assistive movement of D1, as shown in Figure 8a and Figure 8b, respectively.
During the standing assistive movement, when was around 35 degrees, reached its maximum value, and exceeded the evaluation reference value. From Figure 8a, it is evident that is significant during the movement intervals with large values of and . The line made of triangles (the lower line in Figure 8b) in Figure 8b indicates a linear relationship between and based on the measured values. Additionally, assuming the horizontal component of the moment arm between the caregiver and the elderly in the transfer movement is the sum of the trunk length and forearm length, we calculated the theoretical value of using Equation (3) and represented it with the line made of rhombuses (the upper line in Figure 8b) in Figure 8b.
When comparing the theoretical and experimental values in Figure 8b, there is a difference in the y-intercept, which can be attributed to the assumption in the theoretical value calculation, where the distance along the x-axis from the caregiver’s shoulder joint to the gripping point was considered as the upper arm length, but in reality, it is shorter than the upper arm length. Moreover, the slopes are nearly identical, and as the theoretical value’s variable is , it can be inferred that and are dependent variables.
However, represents the x-direction component of , where is the caregiver’s upper torso segment length, and is the caregiver’s upper arm segment length.
Therefore, based on the obtained results, it is crucial to quantitatively capture the relationship between and in the intervals where they are significant, as is substantial in those intervals for considering lumbar burden reduction. Additionally, considering that the factor is dependent on , it indicates that caregivers assist the elderly in standing up by elevating the torso while fixing the position of the elderly person with their arms, rather than lifting the patient solely with their arms. In the standing assistive movement, recognizing as dependent on , and to achieve the objectives in this study, lumbar burden factors were set as state variables, consisting of and .
4.3. Experiment: Understanding the Relationship between Lumbar Burden Factors and Lumbar Burden Evaluation Criteria
From Section 4.2, we considered that the lumbar burden factors are and . Therefore, to quantitatively obtain evaluation criteria for meeting the ideal conditions, an experiment was conducted to understand the relationships between , , and . The participants were eight students (height: 1.74 ± 0.08 m, weight: 68.3 ± 0.05 kg). Participants held a weight (w = 8, 13, 18, 23, and 28 kg in five conditions) with both hands, simulating the caregiver’s standing assistive movement. During the movement, they fixed the elbow angle at 90 degrees and were instructed to simulate the standing assistive movement using the front holding method by raising the trunk. Additionally, three conditions (3, 4, 5 s) were set for the movement time to investigate differences due to the duration of the movement. The measurement method was the same as in Section 4.2.
4.3.1. Results
Figure 9 illustrates the relationship between , , and the lumbar burden evaluation criterion for a representative subject. The five lines represent different weights of the weight (w = 8, 13, 18, 23, and 28 kg). As the weight of the weight increases, tends to increase, but the maximum value of , where does not exceed the evaluation criterion, tends to decrease. This trend was observed regardless of body size and movement time, providing consistent results.
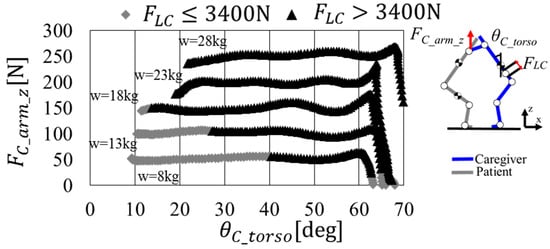
Figure 9.
Representation of the relationship between and in Section 4.3.
4.3.2. Discussion
To obtain the characteristics similar to Figure 9 for each subject, the maximum values of and , where does not exceed the evaluation criterion (), were plotted for each subject. From this relationship shown in Figure 10, an approximation Equation (7) for and was derived. This approximation equation serves as a quantitative boundary to meet the ideal conditions, and using this boundary, the parameter threshold α discussed in Section 3.1 was set. Additionally, a separate experiment was conducted to investigate the scenario where the caregiver holds the assisted elderly to prevent the trunk from falling while in a seated position. It was found that requires approximately 100 N (). Substituting this value into the boundary equation and rearranging, was determined to be 25 degrees (). In other words, the caregiver needs to assist the elderly when is above 25 degrees for to exceed the evaluation criterion of 3400 N.
where = , = .
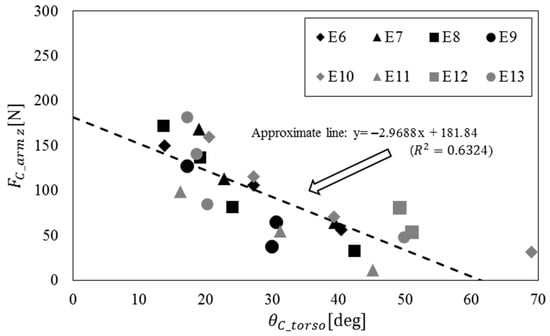
Figure 10.
Relationship between and when .
4.4. Evaluation of the Effectiveness of the Control Algorithm
To assess the effectiveness of the proposed control algorithm considering the lumbar burden factors identified in Section 4.2 and Section 4.3, an experiment was conducted using the developed device. The utility of the control algorithm is defined as “the proposed control algorithm ensures that in the caregiver’s standing assistive movement, is in the range where , and < 3400 N”, as described in Section 3, and the effectiveness of the Calibration Process and Motion Control Process shown in Figure 4 are examined.
4.4.1. Examining the Effectiveness of Calibration Processes
The effectiveness of the Calibration Process is defined as “whether the estimated height corresponds to the measured height based on the proposed control algorithm”, and is examined. Figure 11 illustrates the relationship between the estimated height and the measured height for each subject in the Calibration Process. The subjects consisted of six students (height 1.70 ± 0.06 m, weight 61.3 ± 5.4 kg). As a result, the estimated height of the elderly was obtained with an accuracy of approximately ±0.1 m. Therefore, the Calibration Process enables the estimation of the elderly person’s height, providing valuable results for estimating the inertia term and the gravity term in Equation (1).
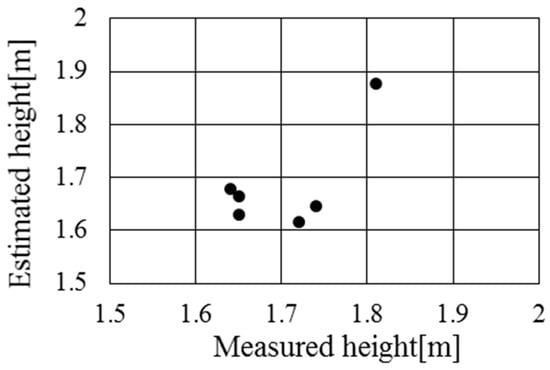
Figure 11.
Measured (actual) height and estimated elderly person’s height during calibration process.
4.4.2. Examining the Effectiveness of Motion Control Processes
The effectiveness of the Motion Control Process is defined as “the proposed control algorithm ensures that does not exceed 3400 N in the range where is smaller than during the stand-up assistive movement of the caregiver”. The subjects included two students (height 1.73 ± 0.08 m, weight 61.0 ± 8.0 kg), who alternately played the roles of caregiver and elderly person in the experiments.
Using the proposed device shown in Figure 2a, the caregiver assistive the standing-up movement using the front holding method. The movement instructions and measurement methods were the same as in Section 4.2, respectively. To ensure that the caregiver performs the movement with within the range smaller than α, the automatic lift algorithm (Lift up) was executed from the state of an elevated seat, followed by the execution of the collaborative assistive algorithm (Torque assist).
Figure 12 illustrates the time-series response of the caregiver’s lumbar burden and the motor operation during the execution of the collaborative assistive algorithm in the movement range where is smaller than . In the case of these two subjects, it was observed that the caregiver applied force to the elderly person, decreasing to assist the standing-up movement. Correspondingly, the motor outputted a torque of approximately 200 Nm, causing the seat to elevate. This indicates that the caregiver’s assistance was provided by reducing , and the motor action resulted in the elevation of the seat.
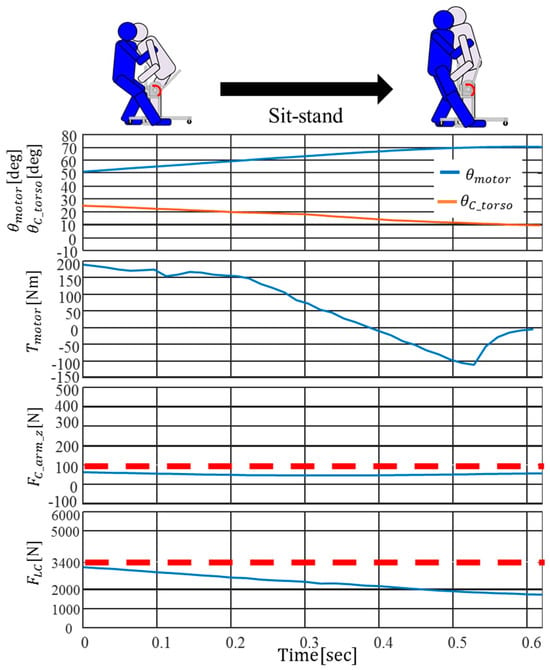
Figure 12.
The time-series response of the caregiver’s lumbar burden and the motor operation during the execution of the collaborative assistive algorithm.
As a result, during the stand-up assistive movement, was found to be less than 100 N, and was less than 3400 N. In other words, it was confirmed that, with the proposed control algorithm, the caregiver and the device collaborate effectively to assist the elderly in standing up. Additionally, in the range of being less than , the proposed control algorithm, through the assistance of the device, resulted in being reduced, meeting the ideal conditions and confirming its effectiveness.
4.5. Discussion
In previous study, we identified the constraints and requirements for a device adapted to the environment of elderly care facilities. We conducted a quantitative assessment of the burden of caregivers’ transfer movements, extracted functional requirements for reducing lumbar burden based on the assessment, and explored specifications for the transfer assistive device [16].
In this study, we aimed to obtain control target values for reducing lumbar burden using the proposed device by understanding the relationship between lumbar burden factors and lumbar burden during transfer movements. Analyzing the relationship between lumbar burden and lumbar burden factors in the transfer movement using the front holding method by a single caregiver under the condition of fixing the patient’s knees, which is one of the device requirements, we identified the correlation between the caregiver’s lumbar disc compression force reaching the evaluation criterion of 3400 N and the caregiver’s trunk forward angle , as well as the upper limb exertion force . The results indicated that the caregiver, assisting the elderly person when was above 25 deg, exceeded the evaluation criterion of 3400 N for .
Furthermore, to reduce the caregiver’s lumbar burden, we proposed a control algorithm considering the correlation of lumbar burden factors. Specifically, based on the condition where was determined to be 3400 N, as identified in Section 4.1, we set the threshold for at 25 deg. In the range where is equal to or greater than , the seat automatic lift algorithm (Lift up) automatically raises the seat. In the range where is less than , the collaborative assistive algorithm (Torque assist) is applied, allowing the device to collaborate with the caregiver’s force input to provide support for standing up.
Utilizing the proposed device and implementing the assistance movement through the collaborative transfer system, a control algorithm for reducing lumbar burden, the results demonstrated the effectiveness of the proposed control algorithm. In the operating range where the caregiver’s trunk forward tilt angle is less than the threshold , it was empirically verified that the evaluation criterion for lumbar intervertebral disc compression force could be reduced to or below the specified standard (3400 N), achieving the ideal condition for lumbar burden reduction.
5. Conclusions
In this study, we have thoroughly considered the physical contact with the elderly under care, aiming to reduce their psychological burden and enhance the acceptance of transfer assistive devices. Taking into account factors such as Parkinson’s disease and cognitive impairments that may hinder effective system utilization, caregivers, in the process of transfer support actions, engage in physical contact with the elderly. This approach is designed not only to assist the elderly in maintaining bodily stability but also to alleviate their anxiety, thereby achieving optimal synergy in the human–machine collaborative transfer system.
It is important to note that the human–machine collaborative transfer system developed in this study is currently in the developmental stage and has not yet entered the clinical trial phase. Therefore, the participants involved in the experiments are not actual elderly people, but rather temporary subjects utilized for system development and performance evaluation. As the research progresses to the clinical trial phase, we will actively invite eligible elderly people to participate in relevant experiments to comprehensively assess the practical utility and applicability of the system. Furthermore, to ensure the rigor of this study, a significant number of professional caregivers will also be required to participate as experimental subjects. Experiments will be conducted with these subjects under various conditions, thereby establishing this research as a robust control and further enhancing its rigor.
However, it is noteworthy that throughout the entire research process, our primary focus was on the quantitative assessment of caregivers’ lumbar load, with limited exploration into the caregivers’ psychological state when utilizing the human–machine collaborative transfer system. Particularly in the context of transfer assistive movements, where caregivers frequently engage in repetitive tasks such as lifting the elderly, the prevalence of bending and twisting motions, coupled with scarce opportunities for rest, exacerbates their psychological burden [21,22,23,24,25]. Especially over the past three years, during the global outbreak of the COVID-19 pandemic, factors such as the pandemic itself, aside from causing direct fatalities, have adversely impacted the mental health of many individuals [26]. In response to these challenges, the recent development of a series of digital mental health tools [27] and welfare devices [28,29] has played a role in emotion regulation, skill development, and education, providing new avenues to address these challenges. Therefore, exploring design methods suitable for caregivers to improve their psychological health becomes the next focal point of our attention.
Author Contributions
Conceptualization, J.W. and M.S.; methodology, J.W. and M.S.; software, J.W.; validation, J.W.; formal analysis, J.W.; investigation, J.W.; resources, M.S.; data curation, J.W.; writing—original draft preparation, J.W.; writing—review and editing, J.W. and M.S.; visualization, J.W.; supervision, M.S.; project administration, M.S.; funding acquisition, M.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by JSPS KAKENHI Grant Number JP20J10461.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy and ethical considerations.
Acknowledgments
This research was partially supported by the J-TEKT Co., Ltd. The authors would like to thank the JSPS Program for Leading Graduate School (Graduate Program in Gerontology, Global Leadership Initiative for an Age Friendly Society, The University of Tokyo) for providing financial support to Jiang Wu.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Reiwa 1st Edition White Paper on Aging Society (Whole Version). Available online: https://www8.cao.go.jp/kourei/whitepaper/w-2023/zenbun/05pdf_index.html (accessed on 24 November 2023).
- Mehrdad, R.; Shams-Hosseini, N.S.; Aghdaei, S.; Yousefian, M. Prevalence of low back pain in health care workers and comparison with other occupational categories in Iran: A systematic review. Iran. J. Med. Sci. 2016, 41, 467. [Google Scholar]
- Study Group Report on Revision and Spread of Low Back Pain Prevention Measures Guidelines in the Workplace. Ministry of Health, Labor and Welfare. 2013. Available online: https://www.mhlw.go.jp/stf/houdou/2r98520000034et4-att/2r98520000034mu2_1.pdf (accessed on 24 November 2023).
- Satoh, H. Transferring-care assistance with robot suit HAL. Trans. Jpn. Soc. Mech. Eng. Ser. C 2010, 76, 227–235. [Google Scholar] [CrossRef]
- Ai Ijo-Kun Mobile Assistance Robot, Art Plan Co., Ltd. Available online: https://www.techno-aids.or.jp/robocare/pdf/jirei_02.pdf (accessed on 24 November 2023).
- Ebbing, T.; Cichosz, M. Innovation for elderly with dementia–localization technology transfer. Int. J. Pharm. Healthc. Mark. 2017, 11, 183–197. [Google Scholar] [CrossRef]
- Sivakanthan, S.; Blaauw, E.; Greenhalgh, M.; Koontz, A.M.; Vegter, R.; Cooper, R.A. Person transfer assist systems: A literature review. Disabil. Rehabil. Assist. Technol. 2021, 16, 270–279. [Google Scholar] [CrossRef] [PubMed]
- Blaauw, E.R.; Greenhalgh, M.; Vegter, R.; Bass, S.; Kulich, H.; Grindle, G.G.; Cooper, R.; Koontz, A.M.; Cooper, R.A. Assessment of Muscle Activation of Caregivers Performing Dependent Transfers with a Novel Robotic-Assisted Transfer Device Compared with the Hoyer Advance. Am. J. Phys. Med. Rehabil. 2021, 100, 885–894. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, R.H.; Pugazhenthi, S. Design and development of a robotic self-transfer device for wheelchair users. J. Enabling Technol. 2017, 11, 59–72. [Google Scholar] [CrossRef]
- Ulrey, B.L.; Fathallah, F.A. Subject-specific, whole-body models of the stooped posture with a personal weight transfer device. J. Electromyogr. Kinesiol. 2013, 23, 206–215. [Google Scholar] [CrossRef]
- Thomas, P.A.; Kim, S. Lost touch? Implications of physical touch for physical health. J. Gerontol. Ser. B 2021, 76, e111–e115. [Google Scholar] [CrossRef] [PubMed]
- Heatley, T.A.; Dunbar, R.I.M.; Montero, M. Physical contact and loneliness: Being touched reduces perceptions of loneliness. Adapt. Hum. Behav. Physiol. 2020, 6, 292–306. [Google Scholar] [CrossRef]
- Eckstein, M.; Mamaev, I.; Ditzen, B.; Sailer, U. Calming effects of touch in human, animal, and robotic interaction—Scientific state-of-the-art and technical advances. Front. Psychiatry 2020, 11, 555058. [Google Scholar] [CrossRef]
- Tomioka, K.; Kumagai, S.; Kosaka, H.; Yoshida, J.; Tabuchi, T.; Kosaka, J.; Arai, Y. Equipment at the Special Nursing Homes for the Elderly: A Workplace Survey of New Nursing Homes in Osaka Prefecture. Sangyo Eiseigaku Zasshi 2006, 48, 49–55. [Google Scholar] [CrossRef][Green Version]
- Wu, J.; Shino, M. Development of Transfer Assist Equipment by Lower Back Burden Reduction Method of Caregiver. In Proceedings of the 2018 IEEE International Conference on Robotics and Biomimetics (ROBIO), Kuala Lumpur, Malaysia, 12–15 December 2018; pp. 691–696. [Google Scholar]
- Wu, J.; Shino, M. Hip lift transfer assistive system for reducing burden on caregiver’s waist. Sensors 2021, 21, 7548. [Google Scholar] [CrossRef] [PubMed]
- NIOSH, National Institute for Occupational Safe and Health. Work Practices Guide for Manual Lifting; No. 81-122; Department of Health and Human Services: Cincinnati, OH, USA, 1981.
- Ae, T.; Tang, H.; Yokoi, T. Estimation of Body Part Inertia Characteristics of Japanese Athletes. Biomechanism 1992, 11, 23–33. [Google Scholar] [CrossRef]
- AIST Human Body Dimension Database 1991–92. Available online: https://www.airc.aist.go.jp/dhrt/91-92/ (accessed on 19 January 2024).
- Yamazaki, N. Measurement of transferring motions and evaluation of caregiver’s lower-back load. Biomechanisms 2002, 16, 195–205. [Google Scholar] [CrossRef][Green Version]
- Kurumatani, N.; Morita, N. Work related movement disorders of nurses—Basic of prevention and Countermeasures (special collection of human care services and ergonomics). J. Labor Sci. 2004, 59, 709–713. [Google Scholar]
- Ebrahim, O.S.; Al-Attar, G.S.; Gabra, R.H.; Osman, D.M. Stigma and burden of mental illness and their correlates among family caregivers of mentally ill patients. J. Egypt. Public Health Assoc. 2020, 95, 31. [Google Scholar] [CrossRef] [PubMed]
- Shetty, J.; Shetty, A.; Mundkur, S.C.; Tantri, K.D.; Prachi, P. Economic burden on caregivers or parents with Down syndrome children—A systematic review protocol. Syst. Rev. 2023, 12, 3. [Google Scholar] [CrossRef]
- Zwar, L.; König, H.H.; Hajek, A. Gender differences in mental health, quality of life, and caregiver burden among informal caregivers during the second wave of the COVID-19 pandemic in Germany: A representative, population-based study. Gerontology 2023, 69, 149–162. [Google Scholar] [CrossRef]
- Kayaalp, A.; Page, K.J.; Rospenda, K.M. Caregiver burden, work-family conflict, family-work conflict, and mental health of caregivers: A mediational longitudinal study. Work Stress 2021, 35, 217–240. [Google Scholar] [CrossRef]
- Panchal, N.; Kamal, R.; Orgera, K.; Cox, C.; Garfield, R.; Hamel, L.; Chidambaram, P. The implications of COVID-19 for mental health and substance use. Kais. Fam. Found. 2020, 21, 1–16. [Google Scholar]
- Petrovic, M.; Gaggioli, A. Digital mental health tools for caregivers of older adults—A scoping review. Front. Public Health 2020, 8, 128. [Google Scholar] [CrossRef] [PubMed]
- KEDAMA, Welfare Equipment Contest 2021. Available online: https://www.resja.or.jp/contest/data/2021/202121.jpg (accessed on 23 February 2024).
- Wu, J.; Yuan, Y.; Dai, Y. Feasibility Study of Portable Simulated Pet ‘KEDAMA’ for Relieving Depression. In International Conference on Human-Computer Interaction; Springer International Publishing: Cham, Switzerland, 2022; pp. 290–304. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).