1. Introduction
Ultrasound (US) is a unique medical imaging technique that is widely used for lesion diagnosis and intraoperative guidance. Compared to other medical imaging methods, US has the advantages of being non-invasive, radiation-free, low-cost, and portable [
1]. However, the traditional US procedure requires sonographers to scan the entire lesion area by using a hand-held probe. To maintain good contact between the US probe and the skin, sonographers must remain in the same position for long periods, which puts them at risk for muscle damage [
2]. In contrast, the probe’s position, orientation, and contact force with the body surface are entirely determined by the sonographer’s experience. Hence, the probe attitude control and scanning path are random. It is difficult to quickly and accurately reproduce previous lesion images for subsequent repeat diagnosis and intraoperative guidance [
3]. In addition, many patients report discomfort during US examinations owing to the sonographer’s shaky hands and inability to control the contact force accurately. US images have a variety of viewpoints, and even different pressures from the same viewpoint can result in clinical differences in US images, making US scanning highly dependent on the physician’s diagnostic imaging experience [
4]. Furthermore, this technical workload has exacerbated the shortage of sonographers [
5], making it difficult for patients in remote rural areas to receive high-level US examinations due to the lack of experienced sonographers.
Robotic US systems have been widely studied as effective solutions [
6]. A robotic US system is mainly composed of a manipulator that drives the movement of the probe and the US imaging device. Currently, robotic US systems are grouped into three categories according to the characteristics of the mode of operation: teleoperated, human–robot cooperation, and autonomous. In the teleoperated mode, a physician remotely controls the robotic arm to examine a patient using a joystick [
7] or a haptic device [
8]. In the human–robot cooperation mode, the basic scanning trajectory is controlled by the operator, whereas the controller provides assistance in terms of contact force or vision [
9]. Our proposed study is based on the autonomous scanning mode, in which the system performs scanning autonomously based on force sensation, vision, and other information without the help of the sonographer. Because the contact posture and contact force between the US probe and human skin greatly influence the US image quality, most studies have been conducted based on these two components. In [
10], the authors studied the relationship between the probe angle and image quality in depth. They concluded that the image quality was significantly improved when the US probe was oriented closer to the normal direction. Thus, the probe should remain in the normal direction when in contact with the surface of the skin tissue. In [
11], the authors approximated the local skin plane by randomly selecting three points around each path point to form a triangle and determine the normal vector of the plane. In [
12], the authors visually optimized the probe orientation using a confidence map, but it was limited to adjusting only the in-plane orientation. In [
13], the authors identified the normal direction using the contact force value estimated from the joint torque; however, the result was affected by the accuracy of the joint sensor.
To obtain high-quality images and ensure patient safety, maintaining appropriate contact between the probe and the skin is another crucial goal for robotic US scanning [
14]. Therefore, many researchers have attempted to control the contact force during scanning, and the controller design can be divided into three main categories. In the first category, compatible probe holders are integrated into a robotic arm [
15,
16,
17,
18], which is designed based on unique mechanical structures. Rational control strategies have been developed for probe steering, force control, and localized scanning. However, the end-effector becomes larger, and motion adjustments become more complex, which are detrimental to the control and scanning efficiency of the robotic arm. In the second category, some systems use built-in force/torque sensors in the manipulator to estimate the contact force and maintain a constant contact force in the probe’s direction [
19,
20,
21,
22,
23]. In the third category, the force/torque (F/T) sensor is mounted between the end of the robotic arm and the probe to measure the force applied to the probe. Compared to the first two approaches, it not only ensures the precision of the contact force data but also makes the system lightweight; however, its disadvantage is that the F/T sensor has a high cost.
Several force control strategies have been introduced to maintain constant force contact with US probes. An adaptive fuzzy PID force control algorithm was proposed in [
24] to maintain the desired contact force during liver scanning. In [
25], the authors proposed an adaptive control strategy based on event triggering and conducted an experiment on a virtual simulation platform for the robotic US system to perform transverse abdominal scanning. In [
26], the authors proposed a variable-rate adaptive admittance control strategy and discussed the effectiveness of the strategy through V-rep. In [
27], an admittance force control system was proposed based on an F/T sensor to compensate for the force required by the sonographer during scanning. In addition, in the field of industrial robotics, a series of force tracking control strategies have been proposed, such as adaptive control [
28,
29], fuzzy logic [
30,
31], and neural networks [
32].
The studies mentioned above improved the force control performance from different perspectives and significantly increased its interaction experience. However, the ability of robots to perform tasks in the unknown complex environment of soft tissue skin is still limited. During human–robot interaction, not only should the response speed of force tracking and the force tracking error at the steady state be considered, but the force overshoot should also be avoided. Excessive contact force can be uncomfortable or even dangerous for patients. Unfortunately, few researchers have simultaneously considered these metrics. Therefore, we propose integral adaptive admittance control algorithms that simultaneously consider these aspects.
In order to help sonographers improve the quality of US examinations and to provide patients with a better interactive experience, this study aims to solve the force tracking problem in robotic US scanning. The key contributions of this research can be encapsulated as follows:
- (1)
A robotic US system is constructed, the scan trajectory is visually acquired, and the real contact force is obtained through gravity compensation.
- (2)
To solve the problems of force tracking accuracy and force overshooting, an integral adaptive admittance control (IAAC) strategy is proposed, which can effectively avoid force overshooting and maintain a stable force during scanning.
- (3)
The proposed IAAC strategy is compared and investigated using traditional admittance (AC) control methods. The proposed control scheme is validated using an experimental platform. It is shown that the performance achieved by the proposed IAAC strategy can satisfy the requirements of soft uncertain environments, such as US scanning, and its adaptability is significantly better than that of an AC controller.
2. Robotic US Scanning System
2.1. System Setup
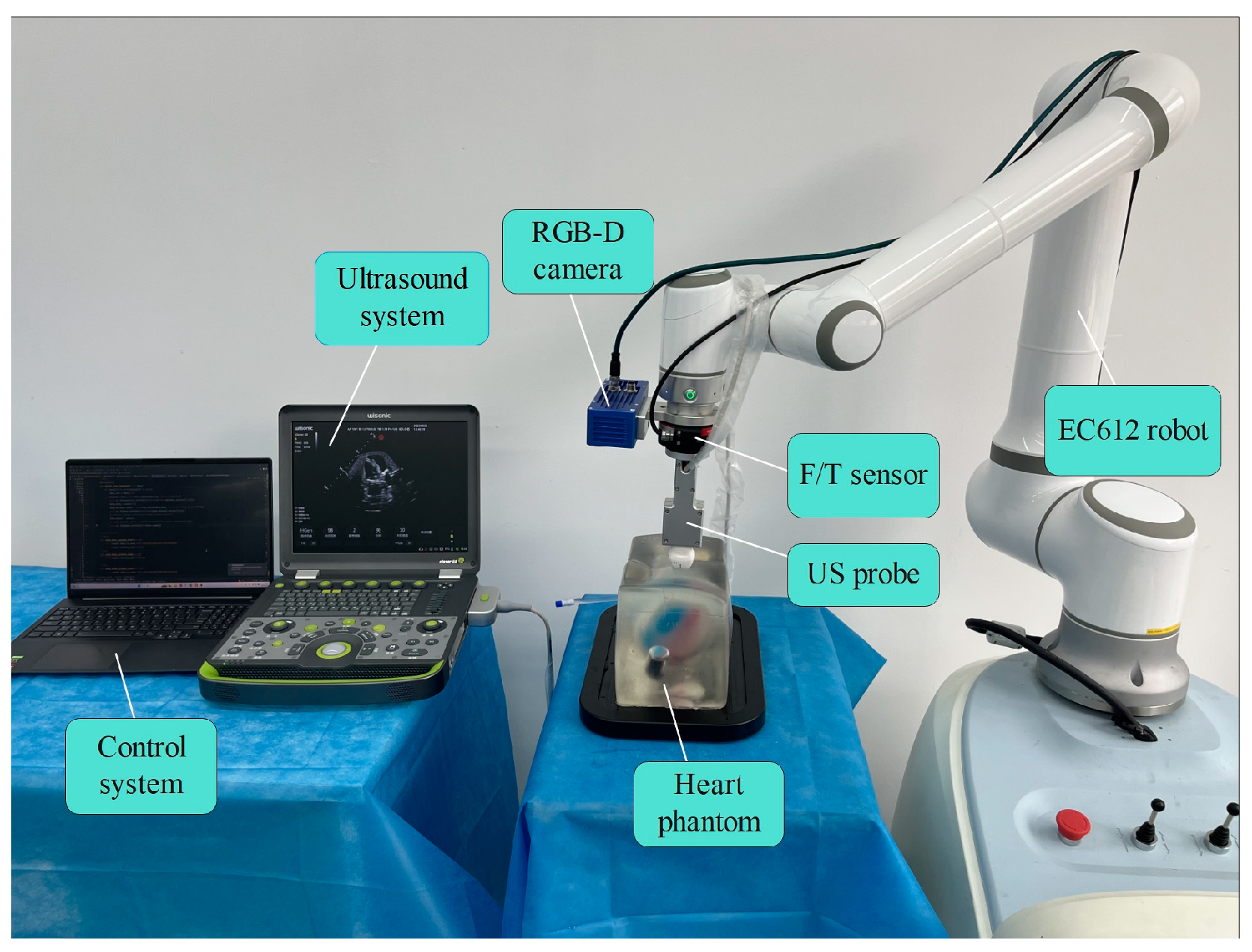
The system comprises five components: a 6-DoF robotic arm (EC612, ELITE, Shanghai, China), a US machine (Clover, Wisonic Medical Technology Company, Ltd., Shenzhen, China) with a linear array probe (C5-1) to acquire the B-scans, an F/T sensor (γ82, DST Sensing System Engineering Company, Ltd., Shenzhen, China), an RGB-D camera (D132s, Zhisensor Technologies Company, Ltd., Xi’an, China), and a heart phantom (BPH700, Intel, Woodruff, NC, USA), as shown in
Figure 1. The system’s control algorithm is completed using Python on an Intel Corei7-5800H 2.5 GHz PC with 16 GB RAM. The US probe is attached to the end of the robot with a customized clamp, and an F/T sensor is installed between them for contact force measurements. The RGB-D camera is also attached to the end of the robot with a clamp on the side of the probe, which is used to capture the point cloud of the heart phantom.
The overall workflow of the system is shown in
Figure 2.
represents the expected reference position,
is the expected position sent to the robotic,
represents the actual position, and
is the position change value of the probe in the vertical direction.
represents the external contact force applied to the probe,
represents the desired force, and
is the difference between them.
represents the joint angle of the robot. When the system operates, the point cloud information of the lesion area is first collected using an RGB-D camera. Then, the probe position is automatically outputted by point cloud processing and path planning. A point cloud normal vector finding framework is established to control the vertical direction of the US probe to ensure that it is perpendicular to the skin surface during the US scanning process. Trajectory planning is then performed for the path points, and the robot’s inner loop controller executes the scanning task. The system can control the probe to fit the skin surface for scanning and adjust the contact force in real time according to the feedback.
2.2. Gravity Compensation
To obtain the real contact force, a gravity compensation process based on the raw force data of the autonomous robotic US scanning system is performed. The coordinate system used in this study is shown in
Figure 3, where the effect of the inertial forces can be disregarded because of the low speed of the robotic US system. The sensor values
are mainly composed of the tool gravity
, the sensor zero value
, and the real contact force
, and the relationship between them is given below:
To obtain reliable US images, it is necessary to keep the normal direction of the probe coinciding with the normal direction of the skin contact surface during the robotic US scanning process, while the human skin is irregularly curved. Therefore, the robot must adjust its attitude, resulting in a change in the probe gravity in . In addition, owing to the sensor’s phenomenon of zero drift, it is necessary to determine the actual zero value of the sensor. In this study, we collected 16 sets of sensor data under the general attitude of the robot and used the least squares method to obtain the sensor zero-point, robot mounting inclination, load gravity, and centre of mass simultaneously, thereby eliminating the influences of the sensor zero-point and load gravity on the force perception, and accurately obtained the real contact force and torque data.
The rotation matrix
from
to
is determined using the following equation:
The definition
is obtained by first rotating
along the
axis by an angle
and then rotating it along the
axis by another angle
.
,
, and
represent the zero of the three-dimensional force;
,
, and
represent the zero of the three-dimensional torque; the load centroid position at
is
; and
is the identity matrix of the third order. Sensor data are obtained using the following equations:
Thus, the sensor zero-point, robot mounting inclination, load gravity, and load centroid position are derived, and the actual contact force can be determined by substituting them into Equation (1).
When the robot is separated from the environment, the external contact force should be 0 N. As shown in
Figure 4,
,
,
,
,
, and
are calculated after gravity compensation to eliminate other influences. The RMSE of the contact force is 0.10981. The RMSE of the contact torque is 0.00832.
2.3. Admittance Control System Description
As shown in
Figure 5a, the probe should be maintained perpendicular to the contact surface of the patient’s skin to obtain high-quality US images. Because the coupling agent with high lubrication is filled between the probe and skin during scanning, the friction in the X and Y-axis directions can be ignored. Therefore, only the contact force in the Z-axis direction must be considered, whereas only the position control is required in the X and Y-axis directions. The probe is equivalent to a second-order mass-damping-spring system to model the contact between the probe and skin. The probe and skin tissue are described as first-order spring models, which assume that the contact force is proportional to the distance of the probe embedded in the environment, as shown in
Figure 5b. The contact process is divided into three stages: free space, collision, and stable contact. Accordingly, the contact force varies, as shown in
Figure 5c,d, and it can be seen that there is a large force overshoot in the collision phase, which is not allowed for human–robot interactions. Although the occurrence of the collision phase is unavoidable, a compliant transition can be achieved as much as possible by improving the performance of the force control strategy. Similarly, the accuracy of force tracking during the stabilized contact phase is also a key consideration.
The actual contact force between the probe and skin tissue is simplified to a first-order spring model as follows:
where
is the actual contact force between the probe and skin;
and
represent the environmental stiffness and position, respectively; and
is the current position of the probe.
Figure 6 depicts the structure of the traditional admittance control, which was first proposed in [
33]. The system consists of an inner position control loop and an outer admittance control loop. Because the current position controllers for cooperative robots that are used in practice have good control accuracy and tracking capability, it is considered that
. Based on the force feedback information, the desired position can be calculated by adding the position deviation calculated using the admittance control outer loop to the reference position
. Subsequently, the manipulator’s inner-loop position controller ensures that the robot reaches the desired position, thereby achieving compliance.
The traditional admittance formula is constructed as follows:
where
,
, and
are the user-specified n-order mass and damping and stiffness diagonal matrix admittance models, respectively. Given the decoupling of the admittance control model across each degree of freedom, our focus can be exclusively directed towards the degrees of freedom along the z-axis. As a result, the matrix and vector in Equation (8) are simplified into scalars. For the sake of simplification,
,
,
,
,
,
,
, and
are replaced by
,
,
,
,
,
,
, and
respectively. Then, Equation (8) can be written as follows:
Similarly,
,
, and
are replaced with
,
, and
, respectively, and
is replaced with
. Then, Equation (7) can be written as follows:
From Equation (10), the correlation between the current probe position and the force can be expressed as follows:
The resultant formula, derived from the amalgamation of Equations (11) and (12), is presented as follows:
Assuming that the ambient stiffness is constant, the derivative and second-order derivative of Equation (13) can be calculated as follows:
By substituting Equations (13)–(15) into Equation (9), the new formula can be expressed as follows:
The Laplace transform of Equation (16) can be obtained as follows:
For convenience, assume that the inputs are all step inputs; that is,
,
, and
. The steady-state error of the contact force deviation is obtained as follows:
From Equation (18), there are two methods to fulfil the condition of a zero steady-state error: the first is to ensure that the admittance parameter satisfies
, and the other is to ensure that
satisfies the following:
Because is the key parameter in the control system, this study will be conducted using the latter approach. As shown in Equation (19), can be computed if the exact position of the environment and the exact value of the environmental stiffness are known. However, in most cases, the environmental stiffness and precise environmental position are unknown. Therefore, it is difficult to realize precise force control during the contraction process by using a traditional admittance controller.
3. Integral Adaptive Admittance Controller
3.1. Adaptive Admittance Control Strategy
In practice,
and
are unknown due to the uncertainty of the contact environment. It is assumed that
and
denote the estimates of
and
, respectively. Therefore, the estimates of the reference trajectory are as follows:
The actual contact force is estimated as follows:
The estimation error of the contact force is
Simplifying Equation (22) yields
where
,
,
, and
.
Therefore, the control strategy dynamically adjusts
and
based on the contact force error. When
tends toward infinity,
approaches
. When
, from Equations (20) and (21), we obtain
Combining Equations (9) and (24) yields
According to Equation (25), when , or . Obviously, and ; in other words, Equation (25) is satisfied by , that is, .
Based on the above analysis, the Lyapunov function is designed as follows:
where
is a diagonal positive definite matrix.
and
are the positive constants.
The first-order derivative of
is denoted as follows:
is as follows:
where
represents the change rate of the estimated parameter.
The further computation of Equation (28) can be obtained:
Applying the second method of Lyapunov and combining Equations (27) and (29) yields
Since the system satisfies the stability condition
, the system is stable. Furthermore, the adaptive algorithm can be expressed as follows:
where
and
, and they are positive scalar constants.
Finally,
can be expressed as follows:
In conclusion, the designed adaptive admittance control (AAC) algorithm estimates the environmental information parameters and in real time based on the robot end-effector position and the actual contact force, and then is calculated, improving the robot’s force tracking performance.
The AAC structure is shown in
Figure 7. However, steady-state tracking errors still exist because of soft unknown skin tissue. Therefore, in order to further improve the performance of the system, an integral controller is designed on the basis of AAC.
3.2. Integral Adaptive Admittance Control Strategy
The AAC controller can make the steady-state error almost zero when the environmental position and the desired force are constant. However, adaptive admittance control has a significant force tracking error when the environmental position continuously changes.
To eliminate steady-state errors and improve the accuracy of force tracking, an integral controller with an improved admittance model is proposed and designed as follows:
where
is the integral coefficient of force error.
It can be obtained from Equation (34) as follows:
The stability of Equation (35) can be ensured through the following characteristics:
According to the Routh criterion, the Routh array is obtained as follows:
If the stability of the system is to be satisfied, it can be obtained according to the principle of the Routh judging stability:
Simplifying Equation (38) shows that it is bounded by the following:
In the current interactive environment, the environmental stiffness is significantly greater than the admittance stiffness, which can be obtained as follows:
Equations (39) and (40) show that IAAC can maintain stability, provided that the appropriate value is chosen.
The value changes due to the complex environment; suppose , where represents a constant.
Similarly, through the application of the Laplace transform to (34) and using the final value theorem, we obtain the following:
Therefore, when , . In other words, adding an integral controller makes the control system converge to the desired force.
By comparing (18) and (42), it can be seen that with the introduction of an integral controller, the expression of the reference trajectory represented by the numerator in (42) remains unchanged. Due to the introduction of the integral term, the order of the numerator is increased, and the adaptability to the environment is improved. At the same time, the increase in the denominator reduces the steady-state error. Therefore, we conclude that it is reasonable to introduce an integral controller to improve the admittance model. This is because it not only does not weaken the control effect of AAC, but it also further reduces the steady-state error. The block diagram of IAAC is shown in
Figure 8.
3.3. The Algorithm Implementation of IAAC
To facilitate its application in collaborative robots, the control algorithm needs to be discretized according to the sampling time.
Figure 9 shows the implementation of the IAAC control algorithm. First, the relevant parameters of the system are initialized. Second, the scan path of the probe is sent to the robot. Third, the external contact force
of the probe is collected from the F/T sensor, and the force error values
and force error gradient
are computed. Fourth, the values of
,
, and
are obtained using the adaptive strategy. Fifth, the reference trajectory
is calculated. Sixth,
is substituted into the integral admittance controller, and the value of
is obtained by double integration. Finally, the command trajectory
at the next time is obtained and executed. From Step 3 to Step 6, a closed loop is executed cyclically. The entire control cycle period is 2 ms.
5. Experimental Studies
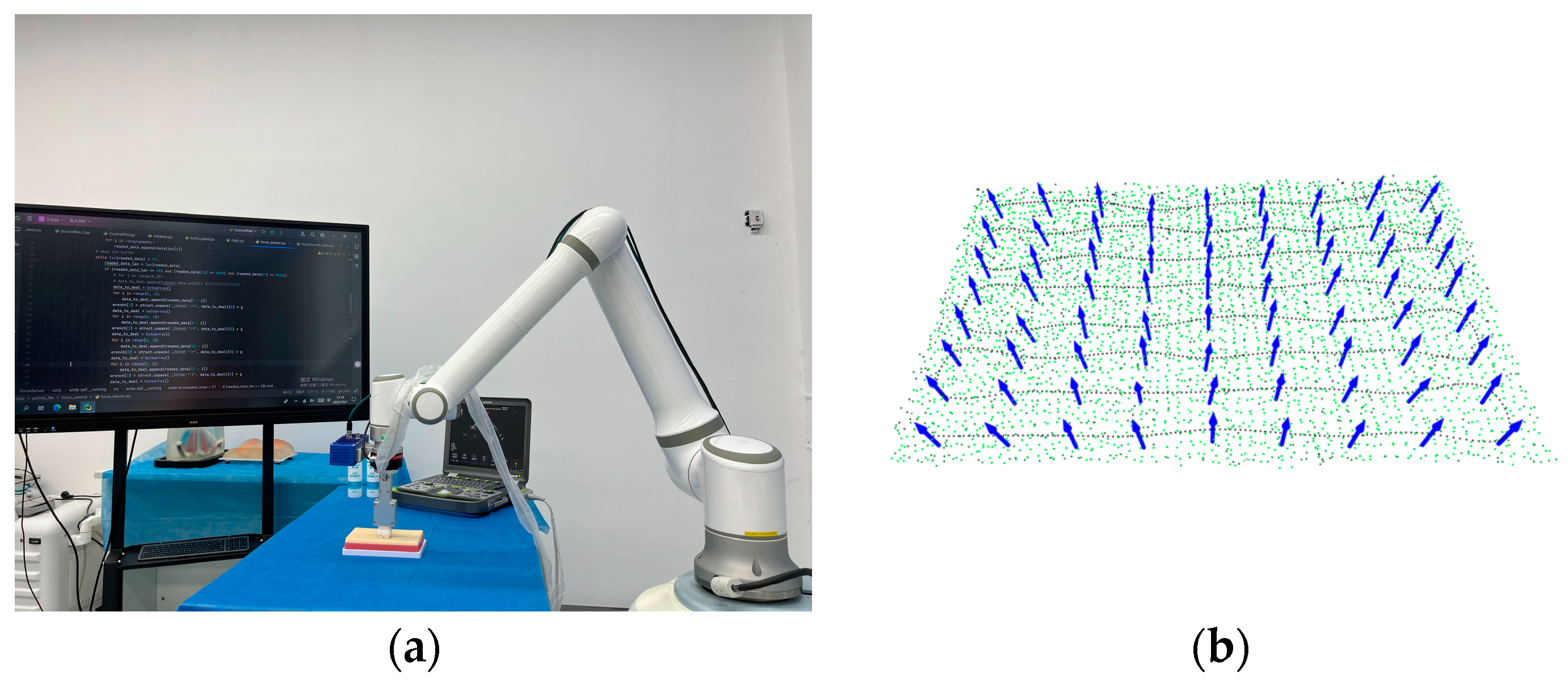
In order to confirm the above simulation study, we conducted experiments on a test bed, as shown in
Figure 14. The composition of this test bed is detailed in
Section 2, in which the RGB-D camera, robot motion controller, six-dimensional force sensor, and industrial PC communicate via an Ethernet switch. The US system and the industrial PC transmit US images using HDMI. Meanwhile, the robot and RGB-D camera communicate through the TCP/IP protocol. The F/T sensor relays the collected force information to the industrial PC via the Modbus communication protocol. Subsequently, the industrial PC combines the trajectory plan’s position with the probe position correction, calculated using the proposed force algorithm, and transmits the command to the robot motion controller.
As shown in
Figure 15,
Figure 16 and
Figure 17, in order to verify the accuracy of our simulation study, we conducted experiments on different tissue models, including a flat skin model, a kidney model, and a heart model. Additionally, we also presented the trajectory point cloud information of the probe on each model. Note that the stiffness values of the three models are unknown and different. To ensure the stability of the system, the relevant parameters of the controller are as follows:
,
,
,
,
,
, and
.
is obtained using an RGB-D camera. Given the quality of US imaging, we set the desired force
in the Z-axis direction during probe scanning. This decision was based on our previous probe pressure experiment and the advice we received from the sonographer.
The first experiment was conducted to test the performances of AC and IAAC on flat surface skin, and the experimental results are shown in
Figure 18 and
Figure 19, respectively. The second and third experiments were performed on a kidney model and a heart model, respectively, as shown in
Figure 20 and
Figure 21, demonstrating the performance of IAAC. In the initial state, the probe moves from free space to a point above the starting point of the scan, and the desired contact force drives the robot into contact with the model. Comparing
Figure 18 and
Figure 19, when in contact with the flat surface skin model, AC has an initial overshoot of approximately 2 N, whereas IAAC has almost no overshoot. Both schemes stabilize at 6 N in approximately 1 s. In the steady-state phase, the contact force fluctuation range is 5.885 ± 0.315 N (5.57–6.20 N) for AC and 5.96 ± 0.14 N (5.82–6.10 N) for IAAC. Compared to AC, the force fluctuation range of IAAC is reduced by 55.6%. So, IAAC can compensate for the steady-state error of AC. Furthermore, in the kidney and heart models, the force overshoots of IAAC are 8.3% and 2.6% of the desired force, respectively. In other words, IAAC is able to track the changes in the environment position in real time by modifying the reference trajectory, which significantly reduces the fluctuation range of the contact force during the change in the environment position, and quickly realizes the desired force tracking with almost no overshoot, as shown in
Figure 20 and
Figure 21. In summary, the control algorithm exhibits good force tracking performance in a soft uncertain environment.
6. Conclusions
A robotic US system plays a vital role in improving the efficiency of US scanning and reducing the work intensity of doctors. An integral adaptive admittance control strategy is designed in this study with the aim of solving the problem of the traditional admittance control being unable to adapt to the complex and changing environment and being unable to realize the high-precision force tracking effect. The proposed control scheme has many significant advantages over other existing methods. Firstly, the proposed strategy can estimate the environmental information in real time, respond quickly, and reduce the force overshoot effectively. Secondly, the introduction of the integral controller further improves the system’s ability to adapt to complex environments. In addition, the proposed control scheme is scalable and equally applicable to scenarios that require force interaction, such as industrial robot grinding.
In order to obtain the external actual contact force of the probe, the raw data of the force sensor are gravity compensated. The final value theorem is used to obtain the conditions under which the contact force reaches the desired force; that is, the suitable reference trajectory is required. In order to solve the problem of force tracking control under the condition of insufficient or unknown environmental information, this paper designs an adaptive control strategy from the perspective of real-time estimation of the environmental position and stiffness so as to predict and generate the subsequent reference trajectory points. Subsequently, the convergence proof of the proposed control strategy is provided in conjunction with the Lyapunov stability theory. In addition, in order to improve the system’s ability to handle complex environments, an integral controller is introduced, and the boundary conditions are obtained by combining the Routh criterion. Finally, through the final value theorem, the validity of the introduced integral controller is proven.
Through simulation experiments of three control strategies in different scenarios, it is proven that IAAC can achieve the fast and compliant adjustment of the contact force. The results show that the force overshoot is significantly reduced, and the force tracking mean square error is the smallest in IAAC compared to AC. Finally, the experiments are carried out on the robotic ultrasonic scanning system. The results show that the force overshot of IAAC is reduced by 69.2%, and the steady-state force fluctuation range is reduced by 55.6% compared with AC on the flat skin surface. On the kidney and heart models, the force overshooting values of IAAC are 8.3% and 2.6% of the desired force, respectively, and high force tracking accuracy is maintained. In conclusion, the proposed strategy can significantly improve the force control performance of a robotic US system in a soft uncertain environment. This is a promising and meaningful study because it shows that the proposed system can partially play the role of a sonographer and act as a medical assistant to reduce the workload. Future work should consider the influence of patient motions, such as breathing and heartbeats, and consider the ultrasound image quality as one of the control objectives to improve the applicability of the control strategy further.

























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}