Serotypes and Vaccine Coverage of Streptococcus Pneumoniae Colonization in the Nasopharynx of Thai Children in Congested Areas in Chiang Mai


 , ,
, ,  , and
, and
Abstract
1. Introduction
2. Results
2.1. Nasopharyngeal Colonization
2.2. Antimicrobial Susceptibility
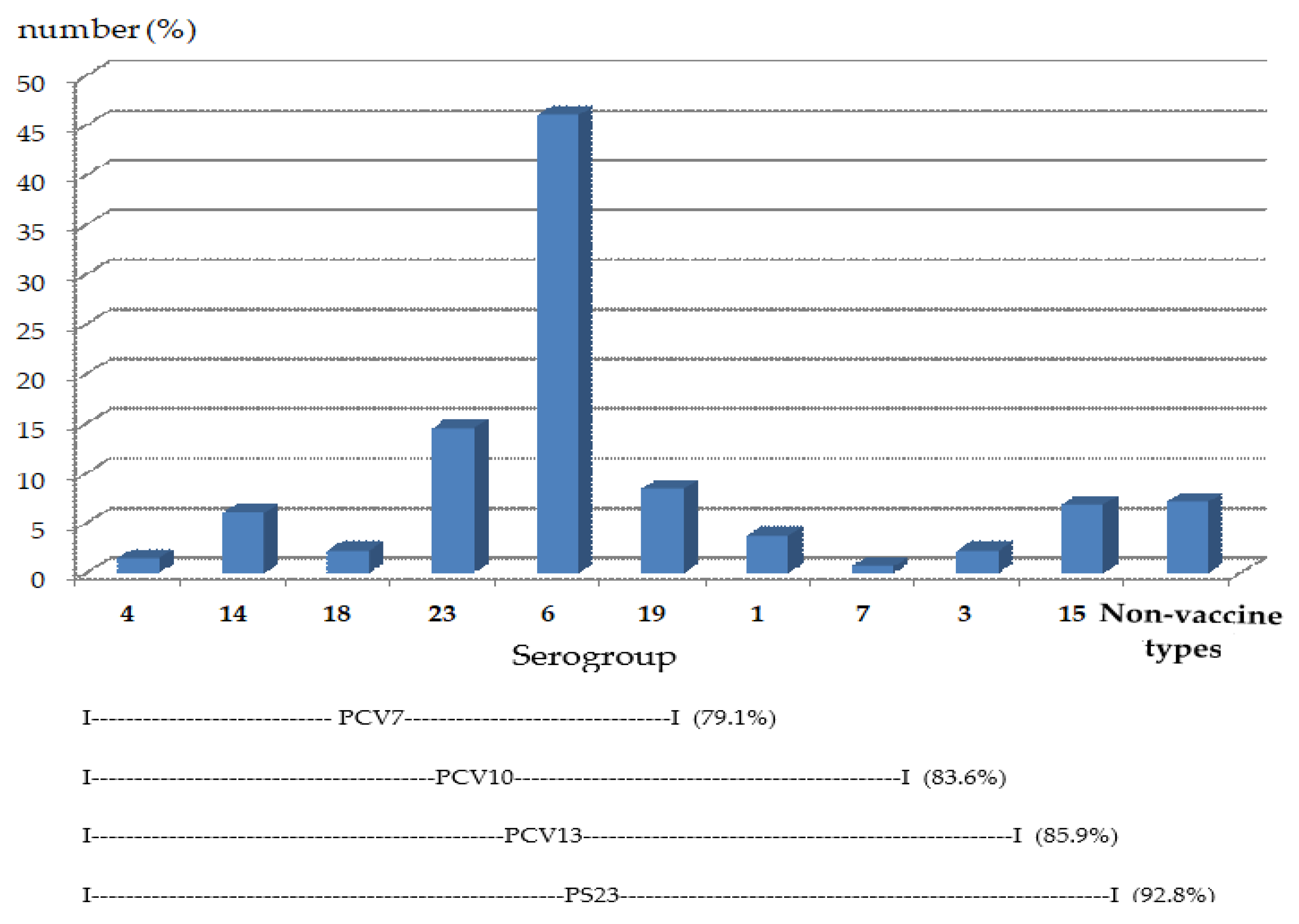
2.3. Serotypes of Nasopharyngeal Pneumococcal Colonization
3. Discussion
4. Materials and Methods
4.1. Study Population and Data Collection
4.1.1. Sample Size Calculation
4.1.2. Data Collection
4.2. Specimen Collection and Isolation of S. pneumoniae
4.3. Bacterial Identification and Characterization
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Advisory Committee on Immunization Practices. Preventing pneumococcal disease among infants and young children. Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2000, 49, 1–35. [Google Scholar]
- Whitney, C.G.; Farley, M.M.; Hadler, J.; Harrison, L.H.; Bennett, N.M.; Lynfield, R.; Reingold, A.; Cieslak, P.R.; Pilishvili, T.; Jackson, D.; et al. Active Bacterial Core Surveillance of the Emerging Infections Program Network. Decline in invasive pneumococcal disease after the introduction of protein-polysaccharide conjugate vaccine. N. Engl. J. Med. 2003, 348, 1737–1746. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Direct and indirect effects of routine vaccination of children with 7-valent pneumococcal conjugate vaccine on incidence of invasive pneumococcal disease—United States, 1998–2003. MMWR Morb. Mortal. Wkly. Rep. 2005, 54, 893. [Google Scholar]
- Poehling, K.A.; Talbot, T.R.; Griffin, M.R.; Craig, A.S.; Whitney, C.G.; Zell, E.; Lexau, C.A.; Thomas, A.R.; Harrison, L.H.; Reingold, A.L.; et al. Invasive pneumococcal disease among infants before and after introduction of pneumococcal conjugate vaccine. JAMA 2006, 295, 1668–1674. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Invasive pneumococcal disease in children 5 years after conjugate vaccine introduction—Eight states, 1998–2005. MMWR Morb. Mortal. Wkly. Rep. 2008, 57, 144–148. [Google Scholar]
- Hsu, H.E.; Shutt, K.A.; Moore, M.R.; Beall, B.W.; Bennett, N.M.; Craig, A.S.; Farley, M.M.; Jorgensen, J.H.; Lexau, C.A.; Petit, S.; et al. Effect of pneumococcal conjugate vaccine on pneumococcal meningitis. N. Engl. J. Med. 2009, 360, 244–256. [Google Scholar] [CrossRef]
- Pavia, M.; Bianco, A.; Nobile, C.G.; Marinelli, P.; Angelillo, I.F. Efficacy of pneumococcal vaccination in children younger than 24 months: A meta-analysis. Pediatrics 2009, 123, e1103–e1110. [Google Scholar] [CrossRef]
- Cherian, T. WHO expert consultation on serotype composition of pneumococcal conjugate vaccines for use in resource-poor developing countries, 26–27 October 2006, Geneva. Vaccine 2007, 25, 6557–6564. [Google Scholar] [CrossRef]
- Watson, D.A.; Musher, D.M. A brief history of the pneumococcus in biomedical research. Semin. Respir. Infect. 1999, 14, 198–208. [Google Scholar]
- Hausdorff, W.P.; Bryant, J.; Paradiso, P.R.; Siber, G.R. Which pneumococcal serogroups cause the most invasive disease: Implications for conjugate vaccine formulation and use, part I. Clin. Infect. Dis. 2000, 30, 100–121. [Google Scholar] [CrossRef]
- Bratcher, P.E.; Park, I.H.; Hollingshead, S.K.; Nahm, M.H. Production of a unique pneumococcal capsule serotype belonging to serogroup 6. Microbiology 2009, 155, 576–583. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Brueggemann, A.B.; Peto, T.E.; Crook, D.W.; Butler, J.C.; Kristinsson, K.G.; Spratt, B.G. Temporal and geographic stability of the serogroup-specific invasive disease potential of Streptococcus pneumoniae in children. J. Infect. Dis. 2004, 190, 1203–1211. [Google Scholar] [CrossRef] [PubMed]
- Harboe, Z.B.; Benfield, T.L.; Valentiner-Branth, P.; Hjuler, T.; Lambertsen, L.; Kaltoft, M.; Krogfelt, K.; Slotved, H.C.; Christensen, J.J.; Konradsen, H.B. Temporal trends in invasive pneumococcal disease and pneumococcal serotypes over 7 decades. Clin. Infect. Dis. 2010, 50, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Miller, E.; Andrews, N.J.; Waight, P.A.; Slack, M.P.; George, R.C. Herd immunity and serotype replacement 4 years after seven-valent pneumococcal conjugate vaccination in England and Wales: An observational cohort study. Lancet Infect. Dis. 2011, 11, 760–768. [Google Scholar] [CrossRef]
- Reinert, R.R.; Paradiso, P.; Fritzell, B. Advances in pneumococcal vaccines: The 13-valent pneumococcal conjugate vaccine received market authorization in Europe. Expert Rev. Vaccines 2010, 9, 229–236. [Google Scholar] [CrossRef]
- Johnson, H.L.; Deloria-Knoll, M.; Levine, O.S.; Stoszek, S.K.; Freimanis, H.L.; Reithinger, R.; Muenz, L.R.; O’Brien, K.L. Systematic evaluation of serotypes causing invasive pneumococcal disease among children under five: The pneumococcal global serotype project. PLoS Med. 2010, 7, e1000348. [Google Scholar] [CrossRef]
- Lehmann, D.; Willis, J.; Moore, H.C.; Giele, C.; Murphy, D.; Keil, A.D.; Harrison, C.; Bayley, K.; Watson, M.; Richmond, P. The changing epidemiology of invasive pneumococcal disease in aboriginal and non-aboriginal western Australians from 1997 through 2007 and emergence of nonvaccine serotypes. Clin. Infect. Dis. 2010, 50, 1477–1486. [Google Scholar] [CrossRef]
- Hsu, K.K.; Shea, K.M.; Stevenson, A.E.; Pelton, S.I. Massachusetts Department of Public Health. Changing serotypes causing childhood invasive pneumococcal disease: Massachusetts, 2001–2007. Pediatr. Infect. Dis. J. 2010, 29, 289–293. [Google Scholar]
- Weinberger, D.M.; Malley, R.; Lipsitch, M. Serotype replacement in disease after pneumococcal vaccination. Lancet 2011, 378, 1962–1973. [Google Scholar] [CrossRef]
- Hanquet, G.; Kissling, E.; Fenoll, A.; George, R.; Lepoutre, A.; Lernout, T.; Tarragó, D.; Varon, E.; Verhaegen, J. Pneumococcal serotypes in children in 4 European countries. Emerg. Infect. Dis. 2010, 16, 1428–1439. [Google Scholar] [CrossRef]
- Roche, P.W.; Krause, V.; Cook, H.; Barralet, J.; Coleman, D.; Sweeny, A.; Fielding, J.; Giele, C.; Gilmour, R.; Holland, R.; et al. Invasive pneumococcal disease in Australia; 2006. Commun. Dis. Intell. Q Rep. 2008, 32, 18–30. [Google Scholar] [PubMed]
- Ho, P.L.; Chiu, S.S.; Ang, I.; Lau, Y.L. Serotypes and antimicrobial susceptibilities of invasive Streptococcus pneumoniae before and after introduction of 7-valent pneumococcal conjugate vaccine, Hong Kong, 1995–2009. Vaccine 2011, 29, 3270–3275. [Google Scholar] [CrossRef] [PubMed]
- Jauneikaite, E.; Jefferies, J.M.; Hibberd, M.L.; Clarke, S.C. Prevalence of Streptococcus pneumoniae serotypes causing invasive and non-invasive disease in South East Asia: A review. Vaccine 2012, 30, 3503–3514. [Google Scholar] [CrossRef] [PubMed]
- Srifeungfung, S.; Tribuddharat, C.; Comerungsee, S.; Chatsuwan, T.; Treerauthanaweeraphong, V.; Rungnobhakhun, P.; Nunthapisud, P.; Chokephaibulkit, K. Serotype coverage of pneumococcal conjugate vaccine and drug susceptibility of Streptococcus pneumoniae isolated from invasive or non-invasive diseases in central Thailand, 2006–2009. Vaccine 2010, 28, 3440–3444. [Google Scholar] [CrossRef] [PubMed]
- Phongsamart, W.; Srifeungfung, S.; Dejsirilert, S.; Chatsuwan, T.; Nunthapisud, P.; Treerauthaweeraphong, V.; Rungnobhakhun, P.; Chokephaibulkit, K. Serotype distribution and antimicrobial susceptibility of S. pneumoniae causing invasive disease in Thai children younger than 5 years old, 2000–2005. Vaccine 2007, 25, 1275–1280. [Google Scholar] [CrossRef] [PubMed]
- Dejsirilert, S.; Sirinavin, S.; Sawanpanyalert, P.; Saengsuk, L.; Polwichai, P.; Tienkrim, S.; Ubonyaem, N. A nationwide study on serotypes of invasive strains of pneumococcus in Thailand, 1998–2008. In Proceedings of the 7th International Symposium on Pneumococci and Pneumococcal Diseases, Tel Aviv, Israel, 14–18 March 2010. [Google Scholar]
- Suwanpakdee, D.; Samakoses, R.; Sirinavin, S.; Kerdpanich, A.; Simasathien, S.; Thunyaharn, S.; Dejsirilert, S.; Watanaveeradej, V. Invasive pneumococcal disease in Phramongkutklao Hospital 2004–2008: Clinical data, serotype distribution and antimicrobial resistance patterns. J. Med. Assoc. Thai. 2010, 93, S40-5. [Google Scholar]
- Levine, S.; Dejsirilert, S.; Sangsuk, L.; Chantra, S.; Feikin, D.R.; Dowell, S.F.; Olsen, S.J. Serotypes and antimicrobial resistance of streptococcus pneumoniae in Thailand 2002–2004. Pediatr. Infect. Dis. J. 2006, 25, 176–178. [Google Scholar] [CrossRef]
- Srifeungfung, S.; Chokephaibulkit, K.; Tribuddharat, C. Serotypes and antimicrobial susceptibilities of Streptococcus pneumoniae isolated from hospitalized patients in Thailand. Southeast Asian J. Trop. Med. Public Health 2007, 38, 469–477. [Google Scholar]
- Song, J.H.; Lee, N.Y.; Ichiyama, S.; Yoshida, R.; Hirakata, Y.; Fu, W.; Chongthaleong, A.; Aswapokee, N.; Chiu, C.H.; Lalitha, M.K.; et al. Spread of drug-resistant Streptococcus pneumoniae in Asian countries: Asian Network for Surveillance of Resistant Pathogens (ANSORP) Study. Clin. Infect. Dis. 1999, 28, 1206–1211. [Google Scholar] [CrossRef]
- Song, J.H.; Jung, S.I.; Ko, K.S.; Kim, N.Y.; Son, J.S.; Chang, H.H.; Ki, H.K.; Oh, W.S.; Suh, J.Y.; Peck, K.R.; et al. High prevalence of antimicrobial resistance among clinical Streptococcus pneumoniae isolates in Asia (an ANSORP study). Antimicrob. Agents Chemother. 2004, 48, 2101–2107. [Google Scholar] [CrossRef]
- Kim, S.H.; Song, J.H.; Chung, D.R.; Thamlikitkul, V.; Yang, Y.; Wang, H.; Lu, M.; So, T.M.; Hsueh, P.R.; Yasin, R.M.; et al. Changing trends in antimicrobial resistance and serotypes of Streptococcus pneumoniae isolates in Asian countries: An Asian Network for Surveillance of Resistant Pathogens (ANSORP) study. Antimicrob. Agents Chemother. 2012, 56, 1418–1426. [Google Scholar] [CrossRef] [PubMed]
- Baggett, H.C.; Peruski, L.F.; Olsen, S.J.; Thamthitiwat, S.; Rhodes, J.; Dejsirilert, S.; Wongjindanon, W.; Dowell, S.F.; Fischer, J.E.; Areerat, P.; et al. Incidence of pneumococcal bacteremia requiring hospitalization in rural Thailand. Clin. Infect. Dis. 2009, 48, S65–S74. [Google Scholar] [CrossRef] [PubMed]
- Bogaert, D.; Engelen, M.N.; Timmers-Reker, A.J.; Elzenaar, K.P.; Peerbooms, P.G.; Coutinho, R.A.; de Groot, R.; Hermans, P.W. Pneumococcal carriage in children in The Netherlands: A molecular epidemiological study. J. Clin. Microbiol. 2001, 39, 3316–3320. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Dagan, R.; O’Brien, K.L. Modeling the association between pneumococcal carriage and child-care center attendance. Clin. Infect. Dis. 2005, 40, 1223–1226. [Google Scholar] [CrossRef] [PubMed]
- De Lencastre, H.; Kristinsson, K.G.; Brito-Avô, A.; Sanches, I.S.; Sá-Leão, R.; Saldanha, J.; Sigvaldadottir, E.; Karlsson, S.; Oliveira, D.; Mato, R.; et al. Carriage of respiratory tract pathogens and molecular epidemiology of Streptococcus pneumoniae colonization in healthy children attending day care centers in Lisbon, Portugal. Microb. Drug Resist. 1999, 5, 19–29. [Google Scholar] [CrossRef]
- Huang, S.S.; Finkelstein, J.A.; Lipsitch, M. Modeling community and individual-level effects of child-care center attendance on pneumococcal carriage. Clin. Infect. Dis. 2005, 40, 1215–1222. [Google Scholar] [CrossRef][Green Version]
- Sá-Leão, R.; Tomasz, A.; Sanches, I.S.; Nunes, S.; Alves, C.R.; Avô, A.B.; Saldanha, J.; Kristinsson, K.G.; de Lencastre, H. Genetic diversity and clonal patterns among antibiotic-susceptible and -resistant Streptococcus pneumoniae colonizing children: Day care centers as autonomous epidemiological units. J. Clin. Microbiol. 2000, 38, 4137–4144. [Google Scholar] [CrossRef]
- Yagupsky, P.; Porat, N.; Fraser, D.; Prajgrod, F.; Merires, M.; McGee, L.; Klugman, K.P.; Dagan, R. Acquisition; carriage, and transmission of pneumococci with decreased antibiotic susceptibility in young children attending a day care facility in southern Israel. J. Infect. Dis. 1998, 177, 1003–1012. [Google Scholar] [CrossRef][Green Version]
- American Academy of Pediatrics. [Pneumococcal infections]. In Red Book: 2012 Report of the Committee on Infectious Diseases; Pickering, L.K., Baker, C.J., Kimberlin, D.W., Long, S.S., Eds.; American Academy of Pediatrics: Village, IL, USA; Elk Groove, CA, USA, 2012; pp. 572–578. [Google Scholar]
- Thummeepak, R.; Leerach, N.; Kunthalert, D.; Tangchaisuriya, U.; Thanwisai, A.; Sitthisak, S. High prevalence of multi-drug resistant Streptococcus pneumoniae among healthy children in Thailand. J. Infect. Public Health 2015, 8, 274–281. [Google Scholar] [CrossRef]
- Piralam, B.; Prosperi, C.; Thamthitiwat, S.; Bunthi, C.; Sawatwong, P.; Sangwichian, O.; Higdon, M.M.; Watson, N.L.; Deloria Knoll, M.; Paveenkittiporn, W.; et al. Pneumococcal colonization prevalence and density among Thai children with severe pneumonia and community controls. PLoS ONE 2020, 15, e0232151. [Google Scholar] [CrossRef]
- Hicks, L.A.; Chien, Y.W.; Taylor, T.H.; Haber, M.; Klugman, K.P. Active Bacterial Core Surveillance (ABCs) Team. Outpatient antibiotic prescribing and nonsusceptible Streptococcus pneumoniae in the United States, 1996–2003. Clin. Infect. Dis. 2011, 53, 631–639. [Google Scholar] [CrossRef] [PubMed]
- Soeters, H.M.; von Gottberg, A.; Cohen, C.; Quan, V.; Klugman, K.P. Trimethoprim-sulfamethoxazole prophylaxis and antibiotic nonsusceptibility in invasive pneumococcal disease. Antimicrob. Agents Chemother. 2012, 56, 1602–1605. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Arason, V.A.; Kristinsson, K.G.; Sigurdsson, J.A.; Stefánsdóttir, G.; Mölstad, S.; Gudmundsson, S. Do antimicrobials increase the carriage rate of penicillin resistant pneumococci in children? Cross sectional prevalence study. BMJ 1996, 313, 387–391. [Google Scholar] [CrossRef] [PubMed]
- Nelson, K.N.; Grijalva, C.G.; Chochua, S.; Hawkins, P.A.; Gil, A.I.; Lanata, C.F.; Griffin, M.R.; Edwards, K.M.; Klugman, K.P.; Vidal, J.E. Dynamics of Colonization of Streptococcus pneumonia Strains in Healthy Peruvian Children. Open Forum Infect. Dis. 2018, 5, ofy039. [Google Scholar] [CrossRef] [PubMed]
- Sutcliffe, C.G.; Shet, A.; Varghese, R.; Veeraraghavan, B.; Manoharan, A.; Wahl, B.; Chandy, S.; Sternal, J.; Khan, R.; Singh, R.K.; et al. Nasopharyngeal carriage of Streptococcus pneumoniae serotypes among children in India prior to the introduction of pneumococcal conjugate vaccines: A cross-sectional study. BMC Infect. Dis. 2019, 19, 605. [Google Scholar] [CrossRef] [PubMed]
- Bogaert, D.; Sluijter, M.; Toom, N.L.; Mitchell, T.J.; Goessens, W.; Clarke, S.C.; de Groot, R.; Hermans, P. Dynamics of pneumococcal colonization in healthy Dutch children. Microbiology 2006, 152, 377–385. [Google Scholar] [CrossRef][Green Version]
- Lynch, J.P.; Zhanel, G.G. Streptococcus pneumoniae: Epidemiology and risk factors, evolution of antimicrobial resistance, and impact of vaccines. Curr. Opin. Pulm. Med. 2010, 16, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Hausdorff, W.P. Invasive pneumococcal disease in children: Geographic and temporal variations in incidence and serotype distribution. Eur. J. Pediatr. 2002, 161, S135–S139. [Google Scholar] [CrossRef] [PubMed]
- Ghaffar, F.; Barton, T.; Lozano, J.; Muniz, L.S.; Hicks, P.; Gan, V.; Ahmad, N.; McCracken, G.H., Jr. Effect of the 7-valent pneumococcal conjugate vaccine on nasopharyngeal colonization by Streptococcus pneumoniae in the first 2 years of life. Clin. Infect. Dis. 2004, 39, 930–938. [Google Scholar] [CrossRef]
- Douglas, R.M.; Paton, J.C.; Duncan, S.J.; Hansman, D.J. Antibody response to pneumococcal vaccination in children younger than five years of age. J. Infect. Dis. 1983, 148, 131–137. [Google Scholar] [CrossRef]
- Nuorti, J.P.; Whitney, C.G.; Centers for Disease Control and Prevention (CDC). Prevention of pneumococcal disease among infants and children—Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine—Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm. Rep. 2010, 59, 1–18. [Google Scholar] [PubMed]
- Doern, G.V.; Richter, S.S.; Miller, A.; Miller, N.; Rice, C.; Heilmann, K.; Beekmann, S. Antimicrobial resistance among Streptococcus pneumoniae in the United States: Have we begun to turn the corner on resistance to certain antimicrobial classes? Clin. Infect. Dis. 2005, 41, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Dejsirilert, S.; Overweg, K.; Sluijter, M.; Saengsuk, L.; Gratten, M.; Ezaki, T.; Hermans, P.W. Nasopharyngeal carriage of penicillin-resistant Streptococcus pneumoniae among children with acute respiratory tract infections in Thailand: A molecular epidemiological survey. J. Clin. Microbiol. 1999, 37, 1832–1838. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.Y.; Song, J.H.; Kim, S.; Peck, K.R.; Ahn, K.M.; Lee, S.I.; Yang, Y.; Li, J.; Chongthaleong, A.; Tiengrim, S.; et al. Carriage of antibiotic-resistant pneumococci among Asian children: A multinational surveillance by the Asian Network for Surveillance of Resistant Pathogens (ANSORP). Clin. Infect. Dis. 2001, 32, 1463–1469. [Google Scholar] [CrossRef] [PubMed]
- Chokephaibulkit, K.; Srifuengfung, S.; Mingbanjerdsuk, J.; Tosasuk, K.; Vanprapar, N.; Chearskul, S.; Dhiraputra, C. Evaluation of susceptibility status of invasive pneumococcal isolates to various antibiotics and risk factors associated with invasive penicillin-nonsusceptible pneumococcal infection: Bangkok 1997-1998. Southeast Asian J. Trop. Med. Public Health 2000, 31, 498–505. [Google Scholar] [PubMed]
- Pancharoen, C.; Chongthaleong, A.; Reinprayoon, S.; Thisyakorn, U. Invasive pneumococcal infection and drug-resistant Streptococcus pneumoniae in Thai children. J. Med. Assoc. Thai. 2001, 84, 1246–1250. [Google Scholar]
- Centers for Disease Control and Prevention. Active Bacterial Core Surveillance Report, Emerging Infections Program Network, Streptococcus pneumonia. 2009. Available online: http://www.cdc.gov/abcs/reports-findings/survreports/spneu09.pdf (accessed on 28 June 2012).
- Jacobs, M.R.; Good, C.E.; Windau, A.R.; Bajaksouzian, S.; Biek, D.; Critchley, I.A.; Sader, H.S.; Jones, R.N. Activity of ceftaroline against recent emerging serotypes of Streptococcus pneumoniae in the United States. Antimicrob. Agents Chemother. 2010, 54, 2716–2719. [Google Scholar] [CrossRef]
- Bogaert, D.; De Groot, R.; Hermans, P.W. Streptococcus pneumoniae colonisation: The key to pneumococcal disease. Lancet Infect. Dis. 2004, 4, 144–154. [Google Scholar] [CrossRef]
- Lee, H.; Nahm, M.H.; Burton, R.; Kim, K.H. Immune response in infants to the heptavalent pneumococcal conjugate vaccine against vaccinerelated serotypes 6A and 19A. Clin. Vaccine Immunol. 2009, 16, 376–381. [Google Scholar] [CrossRef]
- Swenson, J.M.; Hill, B.C.; Thornsberry, C. Screening pneumococci for penicillin resistance. J. Clin. Microbiol. 1986, 24, 749–752. [Google Scholar] [CrossRef]
- Robbins, J.B.; Austrian, R.; Lee, C.J.; Rastogi, S.C.; Schiffman, G.; Henrichsen, J.; Mäkelä, P.H.; Broome, C.V.; Facklam, R.R.; Tiesjema, R.H. Considerations for formulating the second-generation pneumococcal capsular polysaccharide vaccine with emphasis on the cross-reactive types within groups. J. Infect. Dis. 1983, 148, 1136–1159. [Google Scholar] [CrossRef] [PubMed]
- Sanz, J.C.; Culebras, E.; Ríos, E.; Rodríguez-Avial, I.; Wilhelmi, I.; Ramos, B.; Ordobás, M.; Picazo, J.J. Direct serogrouping of Streptococcus pneumoniae strains in clinical samples by use of a latex agglutination test. J. Clin. Microbiol. 2010, 48, 593–595. [Google Scholar] [CrossRef] [PubMed]
- Whitney, C.G.; Pilishvili, T.; Farley, M.M.; Schaffner, W.; Craig, A.S.; Lynfield, R.; Nyquist, A.C.; Gershman, K.A.; Vazquez, M.; Bennett, N.M.; et al. Effectiveness of seven-valent pneumococcal conjugate vaccine against invasive pneumococcal disease: A matched case-control study. Lancet 2006, 368, 1495–1502. [Google Scholar] [CrossRef]
- Yu, X.; Gray, B.; Chang, S.; Ward, J.I.; Edwards, K.M.; Nahm, M.H. Immunity to cross-reactive serotypes induced by pneumococcal conjugate vaccines in infants. J. Infect. Dis. 1999, 180, 1569–1576. [Google Scholar] [CrossRef] [PubMed]
- Poolman, J.; Frasch, C.; Nurkka, A.; Käyhty, H.; Biemans, R.; Schuerman, L. Impact of the conjugation method on the immunogenicity of Streptococcus pneumoniae serotype 19F polysaccharide in conjugate vaccines. Clin. Vaccine Immunol. 2011, 18, 327–336. [Google Scholar] [CrossRef] [PubMed]
- National Committee for Clinical Laboratory Standards. Performance Standards for Antimicrobial Disk Susceptibility Tests, 6th ed.; Approved standard M2-A6; National Committee for Clinical Laboratory Standards: Villanova, PA, USA, 1997. [Google Scholar]
- National Committee for Clinical Laboratory Standards. Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria that Grow Aerobically, 4th ed.; Approved standard M7-A4; National Committee for Clinical Laboratory Standards: Villanova, PA, USA, 1997. [Google Scholar]
- World Health Organization and Centers for Disease Control and Prevention (U.S.). Chapter 8 Identification and Characterization of Streptococcus pneumoniae. In Laboratory Methods for the Diagnosis of Meningitis caused by Neisseria meningitides, Streptococcus Pneumoniae, and Haemophilus Influenzae, WHO Manual, 2nd ed.; WHO: Geneva, Switzerland, 2011; pp. 73–86. [Google Scholar]
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing; CLSI supplement M100-S22; Clinical Laboratory Standard Institute: Wayne, PA, USA, 2012. [Google Scholar]


{kind=link}
| Organisms | Number (%) (Total = 292) |
|---|---|
| Bacteria | |
| Moraxella catarrhalis | 172 (58.9) |
| Streptococcus pneumoniae | 130 (44.5) |
| Corynebacterium spp. (Diphtheroids) | 105 (35.9) |
| Staphylococcus aureus | 87 (29.8) |
| Coagulase-negative Staphylococcus | 80 (27.4) |
| Haemophilus influenzae (not type B) | 47 (16.1) |
| α-hemolytic streptococci | 36 (12.3) |
| Micrococcus spp. | 30 (10.3) |
| Non-hemolytic streptococci | 26 (8.9) |
| Neisseria spp. | 26 (8.9) |
| Haemophilus parainfluenzae | 15 (5.1) |
| Others * | 15 (5.1) |
| Fungi | 10 (3.4) |
| Antimicrobial Agents | Sensitivity (%) | |||
|---|---|---|---|---|
| S. pneumoniae | H. influenzae | M. catarrhalis | S. aureus | |
| Chloramphenicol | - | 87.2 | 97.6 | - |
| Co-trimoxazole | 10.8 | 46.8 | 42.4 | 96 |
| Penicillin | 16.9 | - | - | - |
| Oxacillin | - | - | - | 98.6 |
| Ampicillin | - | 68.1 | 94.2 | - |
| Amoxicillin/clavulanate | - | 95.7 | 100 | - |
| Erythromycin | 61.5 | - | - | 93.3 |
| Clindamycin | 69.2 | - | - | 100 |
| Cefotaxime | - | 100 | 100 | - |
| Ciprofloxacin | - | 100 | 100 | - |
| Vancomycin | - | - | - | 100 |
| Fusidic acid | - | - | - | 100 |
| Levofloxacin | 100 | - | - | - |
| Serogroups/Serotypes | Number of S. pneumoniae Isolates Found in Children at Different Ages (%) | |||
|---|---|---|---|---|
| <5 Years | 6–10 Years | 11–15 Years | Total | |
| Vaccine Types | ||||
| 1 | 5 (3.8) | - | - | 5 (3.8) |
| 3 | 1 (0.7) | - | 2 (1.5) | 3 (2.3) |
| 4 | 1 (0.7) | 1 (0.7) | - | 2 (1.5) |
| 6 (6A, 6B, 6C) | 41 (31.5) | 7 (5.4) | 12 (9.2) | 60 (46.1) |
| 7 (7F, 7A, 7B, 7C) | - | - | 1 (0.7) | 1 (0.7) |
| 14 | 7 (5.4) | 1 (0.7) | - | 8 (6.1) |
| 15 (15F, 15A, 15B, 15C) | 9 (6.9) | - | - | 9 (6.9) |
| 18 (18F, 18A, 18B, 18C) | 2 (1.5) | 1 (0.7) | - | 3 (2.3) |
| 19 (19F, 19A, 19B, 19C) | 7 (5.4) | - | 4 (3.1) | 11 (8.5) |
| 23 (23F, 23A, 23B) | 9 (6.9) | 4 (3.1) | 6 (4.6) | 19 (14.6) |
| Non Vaccine Types | ||||
| 13, 28 (28F, 28A) | 1 (0.7) | - | - | 1 (0.7) |
| 21, 39 | - | 1 (0.7) | - | 1 (0.7) |
| 24 (24F, 24A, 24B), 31, 40 | 1 (0.7) | - | - | 1 (0.7) |
| 25 (25F, 25A), 38, 43, 44, 45, 46, 48 | 1 (0.7) | 1 (0.7) | - | 2 (1.5) |
| 29, 34, 35 (35F, 35A, 35B, 35C), 42, 47 (47F, 47A) | 2 (1.5) | 1 (0.7) | 1 (0.7) | 4 (3.1) |
| Total | 87 (66.9) | 17 (13.1) | 26 (20) | 130 (100) |
| Factor | Adjusted OR (95% CI) | p-Value |
|---|---|---|
| History | ||
| Upper respiratory tract infection one month before collection of specimen | 68.91 (6.48–732.87) | 0.001 * |
| Eczema one month before collection of specimen | 0.59 (0.01–26.07) | 0.784 |
| Physical examination | ||
| Anemia | 0.46 (0.09–2.45) | 0.361 |
| Tonsil enlargement | 2.19 (0.74–6.52) | 0.155 |
| Dental caries | 1.26 (0.55–2.87) | 0.585 |
| Abnormal skin lesions | 4.01 (1.51–10.64) | 0.005 * |
| Comorbidity | ||
| Upper respiratory tract infection | 0.77 (0.13–4.74) | 0.780 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wangirapan, A.; Ayuthaya, S.I.n.; Katip, W.; Kasatpibal, N.; Mektrirat, R.; Anukool, U.; Oberdorfer, P. Serotypes and Vaccine Coverage of Streptococcus Pneumoniae Colonization in the Nasopharynx of Thai Children in Congested Areas in Chiang Mai. Pathogens 2020, 9, 988. https://doi.org/10.3390/pathogens9120988
Wangirapan A, Ayuthaya SIn, Katip W, Kasatpibal N, Mektrirat R, Anukool U, Oberdorfer P. Serotypes and Vaccine Coverage of Streptococcus Pneumoniae Colonization in the Nasopharynx of Thai Children in Congested Areas in Chiang Mai. Pathogens. 2020; 9(12):988. https://doi.org/10.3390/pathogens9120988
Chicago/Turabian StyleWangirapan, Anchalee, Satja Issaranggoon na Ayuthaya, Wasan Katip, Nongyao Kasatpibal, Raktham Mektrirat, Usanee Anukool, and Peninnah Oberdorfer. 2020. "Serotypes and Vaccine Coverage of Streptococcus Pneumoniae Colonization in the Nasopharynx of Thai Children in Congested Areas in Chiang Mai" Pathogens 9, no. 12: 988. https://doi.org/10.3390/pathogens9120988
APA StyleWangirapan, A., Ayuthaya, S. I. n., Katip, W., Kasatpibal, N., Mektrirat, R., Anukool, U., & Oberdorfer, P. (2020). Serotypes and Vaccine Coverage of Streptococcus Pneumoniae Colonization in the Nasopharynx of Thai Children in Congested Areas in Chiang Mai. Pathogens, 9(12), 988. https://doi.org/10.3390/pathogens9120988