Retrospective Case-Control Study of 2017 G2P[4] Rotavirus Epidemic in Rural and Remote Australia

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Study Design
2.3. Data Sources
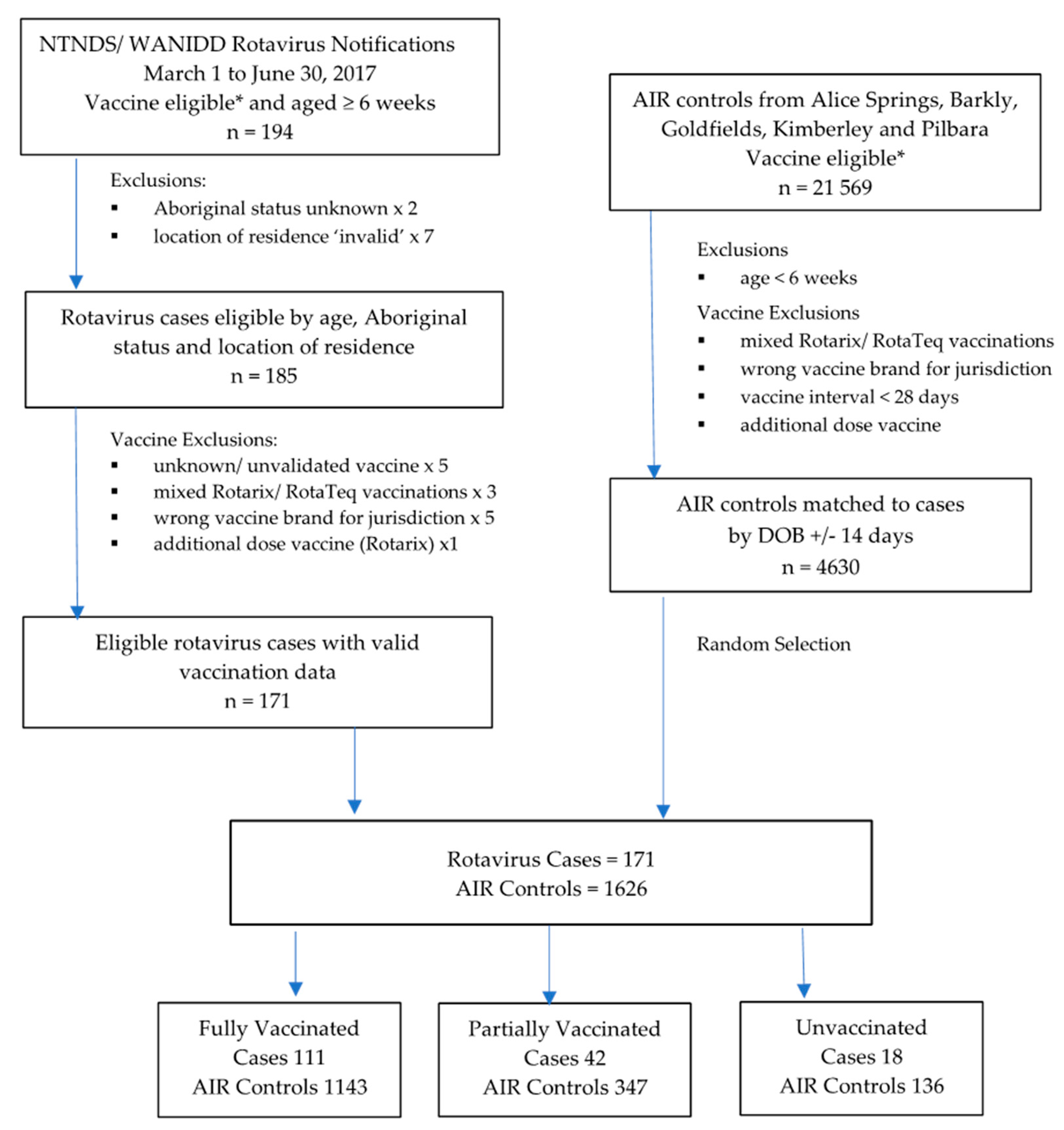
2.4. Participants
2.4.1. Population-Based Analysis
2.4.2. Disease Register Analysis
2.5. Immunisation Status
2.6. Statistical Analysis
2.7. Ethics Committee Approvals
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Troeger, C.; Khalil, I.A.; Rao, P.C.; Cao, S.; Blacker, B.F.; Ahmed, T.; Armah, G.; Bines, J.E.; Brewer, T.G.; Colombara, D.V.; et al. Rotavirus Vaccination and the Global Burden of Rotavirus Diarrhea among Children Younger Than 5 Years. JAMA Pediatr. 2018, 172, 958–965. [Google Scholar] [CrossRef] [PubMed]
- Burnett, E.; Parashar, U.D.; Tate, J.E. Real-world effectiveness of rotavirus vaccines, 2006–2019: A literature review and meta-analysis. Lancet Glob. Health 2020, 8, e1195–e1202. [Google Scholar] [CrossRef]
- WHO. Rotavirus vaccines WHO position paper: January 2013—Recommendations. Vaccine 2013, 31, 6170–6171. [Google Scholar] [CrossRef] [PubMed]
- Armah, G.E.; Sow, S.O.; Breiman, R.F.; Dallas, M.J.; Tapia, M.D.; Feikin, D.R.; Binka, F.N.; Steele, A.D.; Laserson, K.F.; Ansah, N.A.; et al. Efficacy of pentavalent rotavirus vaccine against severe rotavirus gastroenteritis in infants in developing countries in sub-Saharan Africa: A randomised, double-blind, placebo-controlled trial. Lancet 2010, 376, 606–614. [Google Scholar] [CrossRef]
- Madhi, S.A.; Cunliffe, N.A.; Steele, D.; Witte, D.; Kirsten, M.; Louw, C.; Ngwira, B.; Victor, J.C.; Gillard, P.H.; Cheuvart, B.B.; et al. Effect of human rotavirus vaccine on severe diarrhea in African infants. N. Engl. J. Med. 2010, 362, 289–298. [Google Scholar] [CrossRef]
- Zaman, K.; Anh, D.D.; Victor, J.C.; Shin, S.; Yunus; Dallas, M.J.; Podder, G.; Thiem, V.D.; Mai, L.T.P.; Luby, S.P.; et al. Efficacy of pentavalent rotavirus vaccine against severe rotavirus gastroenteritis in infants in developing countries in Asia: A randomised, double-blind, placebo-controlled trial. Lancet 2010, 376, 615–623. [Google Scholar] [CrossRef]
- Dey, A.; Wang, H.; Menzies, R.; Macartney, K. Changes in hospitalisations for acute gastroenteritis in Australia after the national rotavirus vaccination program. Med. J. Aust. 2012, 197, 453–4547. [Google Scholar] [CrossRef]
- Snelling, T.L.; Andrews, R.M.; Kirkwood, C.D.; Culvenor, S.; Carapetis, J.R. Case-control evaluation of the effectiveness of the G1P[8] human rotavirus vaccine during an outbreak of rotavirus G2P[4] infection in central Australia. Clin. Infect. Dis. 2011, 52, 191–199. [Google Scholar] [CrossRef]
- ABS. 2016 Census QuickStats (SA3); Australian Bureau of Statistics: Canberra, Australia, 2017. Available online: https://www.abs.gov.au/websitedbs/censushome.nsf/home/quickstats?opendocument&navpos=220 (accessed on 20 July 2020).
- Hull, B.P.; Lawrence, G.; MacIntyre, C.R.; McIntyre, P.B. Estimating immunisation coverage: Is the ‘third dose assumption’ still valid? Commun. Dis. Intell. Q. Rep. 2003, 27, 357–361. [Google Scholar]
- Field, E.J.; Vally, H.; Grimwood, K.; Lambert, S. Pentavalent rotavirus vaccine and prevention of gastroenteritis hospitalizations in Australia. Pediatrics 2010, 126, e506–e512. [Google Scholar] [CrossRef]
- Fathima, P.; Snelling, T.L.; Gibbs, R.A. Effectiveness of rotavirus vaccines in an Australian population: A case-control study. Vaccine 2019, 37, 6048–6053. [Google Scholar] [CrossRef] [PubMed]
- Maguire, J.E.; Glasgow, K.; Glass, K.; Roczo-Farkas, S.; Bines, J.E.; Sheppeard, V.; Macartney, K.; Quinn, H.E. Rotavirus Epidemiology and Monovalent Rotavirus Vaccine Effectiveness in Australia: 2010–2017. Pediatrics 2019, 144, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Australian Technical Advisory Group on Immunisation (ATAGI). Australian Immunisation Handbook; Australian Government Department of Health: Canberra, Australia, 2018.
- Payne, D.C.; Boom, J.A.; Staat, M.A.; Edwards, K.M.; Szilagyi, P.G.; Klein, E.J.; Selvarangan, R.; Azimi, P.H.; Harrison, C.; Moffatt, M.; et al. Effectiveness of pentavalent and monovalent rotavirus vaccines in concurrent use among US children <5 years of age, 2009–2011. Clin. Infect. Dis. 2013, 57, 13–20. [Google Scholar] [PubMed]
- Castilla, J.; Beristain, X.; Martínez-Artola, V.; Ortega, A.N.; Cenoz, M.G.; Álvarez, N.; Polo, I.; Mazón, A.; Gil-Setas, A.; Barricarte, A. Effectiveness of rotavirus vaccines in preventing cases and hospitalizations due to rotavirus gastroenteritis in Navarre, Spain. Vaccine 2012, 30, 539–543. [Google Scholar] [CrossRef]
- Muhsen, K.; Shulman, L.; Kasem, E.; Rubinstein, U.; Shachter, J.; Kremer, A.; Goren, S.; Zilberstein, I.; Chodick, G.; Ephros, M.; et al. Effectiveness of rotavirus vaccines for prevention of rotavirus gastroenteritis-associated hospitalizations in Israel: A case-control study. Hum. Vaccines 2010, 6, 450–454. [Google Scholar] [CrossRef]
- Leshem, E.; Lopman, B.; Glass, R.; Gentsch, J.; Banyai, K.; Parashar, U.; Patel, M. Distribution of rotavirus strains and strain-specific effectiveness of the rotavirus vaccine after its introduction: A systematic review and meta-analysis. Lancet Infect. Dis. 2014, 14, 847–856. [Google Scholar] [CrossRef]
- Correia, J.B.; Patel, M.M.; Nakagomi, O.; Montenegro, F.M.U.; Germano, E.M.; Correia, N.B.; Cuevas, L.E.; Parashar, U.D.; Cunliffe, N.A.; Nakagomi, T. Effectiveness of monovalent rotavirus vaccine (Rotarix) against severe diarrhea caused by serotypically unrelated G2P[4] strains in Brazil. J. Infect. Dis. 2010, 201, 363–369. [Google Scholar] [CrossRef]
- Zeller, M.; Rahman, M.; Heylen, E.; De Coster, S.; De Vos, S.; Arijs, I.; Novo, L.; Verstappen, N.; Van Ranst, M.; Matthijnssens, J. Rotavirus incidence and genotype distribution before and after national rotavirus vaccine introduction in Belgium. Vaccine 2010, 28, 7507–7513. [Google Scholar] [CrossRef]
- Doro, R.; László, B.; Martella, V.; Leshem, E.; Gentsch, J.; Parashar, U.; Banyai, K. Review of global rotavirus strain prevalence data from six years post vaccine licensure surveillance: Is there evidence of strain selection from vaccine pressure? Infect. Genet. Evol. 2014, 28, 446–461. [Google Scholar] [CrossRef]
- Roczo-Farkas, S.; Kirkwood, C.D.; Cowley, D.; Barnes, G.L.; Bishop, R.F.; Bogdanovic-Sakran, N.; Boniface, K.; Donato, C.M.; E Bines, J. The Impact of Rotavirus Vaccines on Genotype Diversity: A Comprehensive Analysis of 2 Decades of Australian Surveillance Data. J. Infect. Dis. 2018, 218, 546–554. [Google Scholar] [CrossRef]
- Santos, V.S.; Nóbrega, F.A.; Soares, M.W.S.; Moreira, R.D.; Cuevas, L.E.; Gurgel, R.Q. Rotavirus Genotypes Circulating in Brazil Before and After the National Rotavirus Vaccine Program: A Review. Pediatr. Infect. Dis. J. 2018, 37, e63–e65. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.; Glass, R.I.; Jiang, B.; Santosham, M.; Lopman, B.; Parashar, U. A systematic review of anti-rotavirus serum IgA antibody titer as a potential correlate of rotavirus vaccine efficacy. J. Infect. Dis. 2013, 208, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Velasquez, D.E.; Parashar, U.; Jiang, B. Decreased performance of live attenuated, oral rotavirus vaccines in low-income settings: Causes and contributing factors. Expert Rev. Vaccines 2018, 17, 145–161. [Google Scholar] [CrossRef] [PubMed]
- Peter, G.; Myers, M.G. Intussusception, rotavirus, and oral vaccines: Summary of a workshop. Pediatrics 2002, 110, e67. [Google Scholar] [CrossRef]
- Moore, H.C.; Fathima, P.; Gidding, H.F.; De Klerk, N.; Liu, B.; Sheppeard, V.; Effler, P.V.; Snelling, T.L.; McIntyre, P.; Blyth, C.C.; et al. Assessment of on-time vaccination coverage in population subgroups: A record linkage cohort study. Vaccine 2018, 36, 4062–4069. [Google Scholar] [CrossRef]
- Fathima, P.; Gidding, H.F.; Snelling, T.L.; McIntyre, P.; Blyth, C.C.; Sheridan, S.; Liu, B.; De Klerk, N.; Moore, H.C. Timeliness and factors associated with rotavirus vaccine uptake among Australian Aboriginal and non-Aboriginal children: A record linkage cohort study. Vaccine 2019, 37, 5835–5843. [Google Scholar] [CrossRef]
- Orenstein, W.A.; Bernier, R.H.; Hinman, A.R. Assessing vaccine efficacy in the field. Further observations. Epidemiol. Rev. 1988, 10, 212–241. [Google Scholar] [CrossRef]
- Izzo, M.M.; Kirkland, P.D.; Gu, X.; Lele, Y.; Gunn, A.A.; House, J. Comparison of three diagnostic techniques for detection of rotavirus and coronavirus in calf faeces in Australia. Aust. Vet. J. 2012, 90, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Middleton, B.F.; Jones, M.A.; Waddington, C.S.; Danchin, M.; McCallum, C.; Gallagher, S.; Leach, A.J.; Andrews, R.; Kirkwood, C.; Cunliffe, N.; et al. The ORVAC trial protocol: A phase IV, double-blind, randomised, placebo-controlled clinical trial of a third scheduled dose of Rotarix rotavirus vaccine in Australian Indigenous infants to improve protection against gastroenteritis. BMJ Open 2019, 9, e032549. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Rotavirus Cases | |
|---|---|---|
| NT | WA | |
| n = 83 | n = 88 | |
| Age | ||
| Median age (months) | 18 | 19 |
| Age range (months) | 1 to 72 | 1 to 94 |
| 6 weeks to <24 wks (NT only) | 12 (14%) | |
| 6 weeks to <32 wks (WA only) | 10 (11%) | |
| 6 weeks to <1 year | 25 (30%) | 23 (26%) |
| 1 year to <2 years | 36 (44%) | 34 (39%) |
| 2 years to <3 years | 11 (13%) | 15 (17%) |
| 3 years to <4 years | 7 (8%) | 5 (6%) |
| 4 years to <5 years | 3 (4%) | 5 (6%) |
| ≥5 years | 1 (1%) | 6 (6%) |
| Sex | ||
| Female | 42 (51%) | 43 (49%) |
| Male | 41 (49%) | 45 (51%) |
| Aboriginal Status | ||
| Aboriginal | 71 (86%) | 66 (75%) |
| Non-Aboriginal | 12 (14%) | 22 (25%) |
| Location of Residence | ||
| Alice Springs | 70 (84%) | |
| Barkly | 13 (16%) | |
| Goldfields | 17 (19%) | |
| Kimberley | 49 (56%) | |
| Pilbara | 22 (25%) | |
| Genotype | ||
| G2P[4] | 44 (53%) | 59 (67%) |
| Unknown | 39 (47%) | 29 (33%) |
| Hospitalisation | ||
| Yes | 65 (78%) | 34 (39%) |
| No | 18 (22%) | 41 (46%) |
| Unknown | 13 (15%) | |
| Vaccination | ||
| 0 doses | 8 (10%) | 10 (11%) |
| 1 doses | 15 (18%) | 8 (9%) |
| 2 doses | 60 (72%) | 19 (22%) |
| 3 doses | 51 (58%) | |
| Immunisation Register Analysis | Disease Register Analysis | |||||
|---|---|---|---|---|---|---|
| Immunisation Status | Cases | Controls | Odds Ratio (95% CI) | Cases | Controls | Odds Ratio (95% CI) |
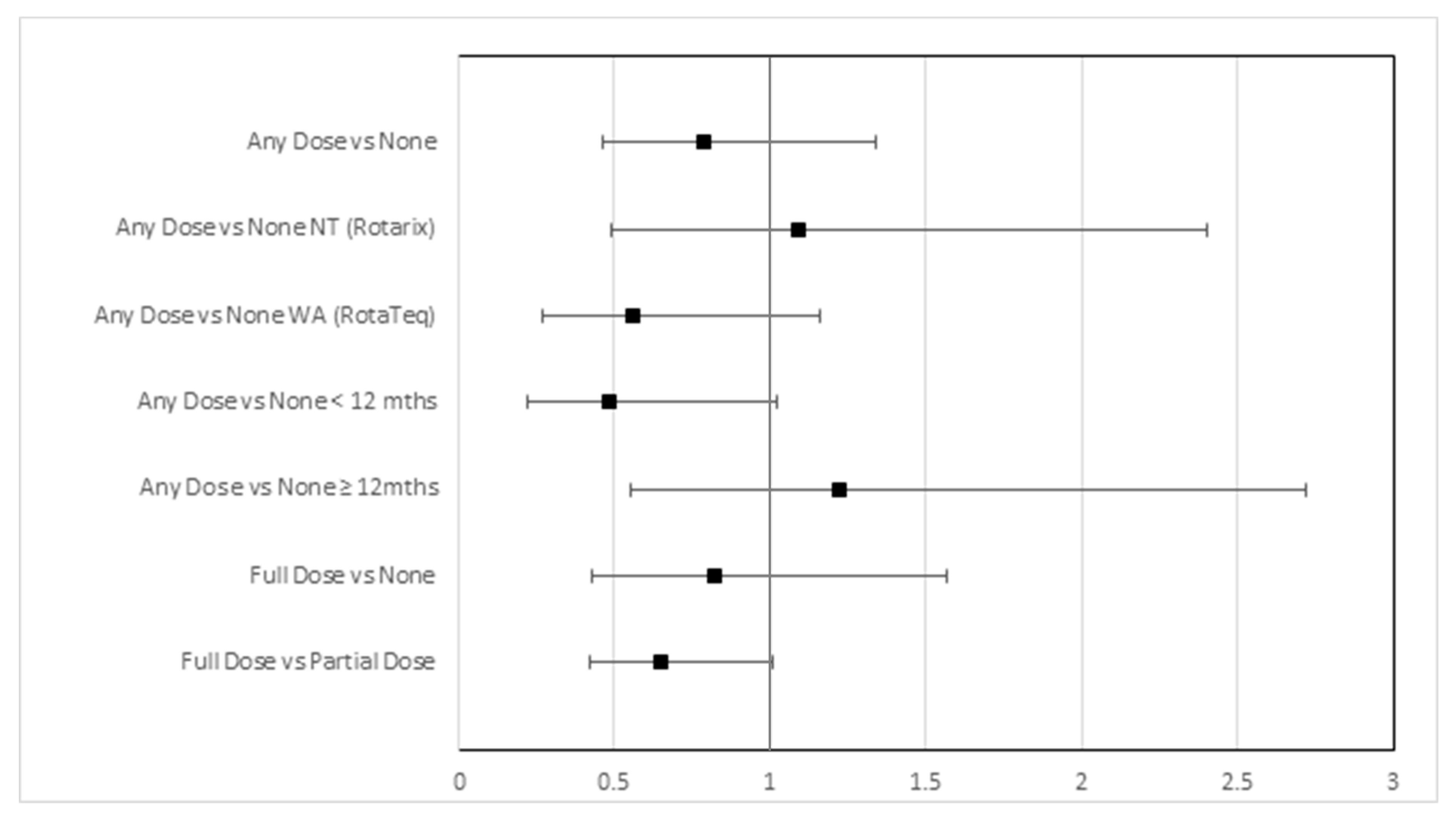
| Any Dose vs. None | n = 171 | n = 1626 | 0.79 (0.46, 1.34) | n = 149 | n = 299 | 0.58 (0.24, 1.39) |
| ≥One Dose Vaccine | 153 | 1490 | 137 | 283 | ||
| Unvaccinated | 18 | 136 | 12 | 16 | ||
| Any Dose vs. None NT (Rotarix) | n = 83 | n = 753 | 1.10 (0.50, 2.41) | n = 71 | n = 123 | 1.40 (0.34, 5.80) |
| ≥One Dose Vaccine | 75 | 676 | 68 | 114 | ||
| Unvaccinated | 8 | 77 | 3 | 9 | ||
| Any Dose vs. None WA (RotaTeq) | n = 88 | n = 873 | 0.56 (0.27, 1.16) | n = 78 | n = 176 | 0.30 (0.09, 0.98) |
| ≥One Dose Vaccine | 78 | 814 | 69 | 169 | ||
| Unvaccinated | 10 | 59 | 9 | 7 | ||
| Any Dose vs. None < 12 mths | n = 48 | n = 449 | 0.48 (0.22, 1.02) | n = 26 | n = 37 | 0.28 (0.03, 2.83) |
| ≥One Dose Vaccine | 37 | 392 | 21 | 36 | ||
| Unvaccinated | 11 | 57 | 5 | 1 | ||
| Any Dose vs. None ≥12mths | n = 123 | n = 1177 | 1.22 (0.55, 2.73) | n = 123 | n = 262 | 0.81 (0.29, 2.28) |
| ≥One Dose Vaccine | 116 | 1098 | 116 | 247 | ||
| Unvaccinated | 7 | 79 | 7 | 15 | ||
| Full Dose vs. None | n = 129 | n = 1008 | 0.83 (0.43, 1.58) | n = 121 | n = 264 | 0.55 (0.23, 1.32) |
| Fully Vaccinated | 111 | 913 | 109 | 248 | ||
| Unvaccinated | 18 | 95 | 12 | 16 | ||
| Full Dose vs. None NT (Rotarix) | n = 68 | n = 529 | 2.06 (0.62, 6.83) | n = 61 | n = 117 | 1.27 (0.31, 5.23) |
| Fully Vaccinated | 60 | 469 | 58 | 108 | ||
| Unvaccinated | 8 | 60 | 3 | 9 | ||
| Full Dose vs. None WA (RotaTeq) | n = 61 | n = 479 | 0.40 (0.18, 0.93) | n = 60 | n = 147 | 0.29 (0.09, 0.96) |
| Fully Vaccinated | 51 | 444 | 51 | 140 | ||
| Unvaccinated | 10 | 35 | 9 | 7 | ||
| Full Dose vs. Partial Dose | n = 153 | n = 1350 | 0.65 (0.42, 1.01) | n = 137 | n = 283 | 0.63 (0.35, 1.13) |
| Fully Vaccinated | 111 | 1060 | 109 | 248 | ||
| Partially Vaccinated | 42 | 290 | 28 | 35 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Middleton, B.F.; Danchin, M.; Quinn, H.; Ralph, A.P.; Pingault, N.; Jones, M.; Estcourt, M.; Snelling, T. Retrospective Case-Control Study of 2017 G2P[4] Rotavirus Epidemic in Rural and Remote Australia. Pathogens 2020, 9, 790. https://doi.org/10.3390/pathogens9100790
Middleton BF, Danchin M, Quinn H, Ralph AP, Pingault N, Jones M, Estcourt M, Snelling T. Retrospective Case-Control Study of 2017 G2P[4] Rotavirus Epidemic in Rural and Remote Australia. Pathogens. 2020; 9(10):790. https://doi.org/10.3390/pathogens9100790
Chicago/Turabian StyleMiddleton, Bianca F., Margie Danchin, Helen Quinn, Anna P. Ralph, Nevada Pingault, Mark Jones, Marie Estcourt, and Tom Snelling. 2020. "Retrospective Case-Control Study of 2017 G2P[4] Rotavirus Epidemic in Rural and Remote Australia" Pathogens 9, no. 10: 790. https://doi.org/10.3390/pathogens9100790
APA StyleMiddleton, B. F., Danchin, M., Quinn, H., Ralph, A. P., Pingault, N., Jones, M., Estcourt, M., & Snelling, T. (2020). Retrospective Case-Control Study of 2017 G2P[4] Rotavirus Epidemic in Rural and Remote Australia. Pathogens, 9(10), 790. https://doi.org/10.3390/pathogens9100790