
Detection of Human Papillomavirus in Urogenital Swabs from Male Patients in Northern Serbia

 ,
,  ,
,  , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
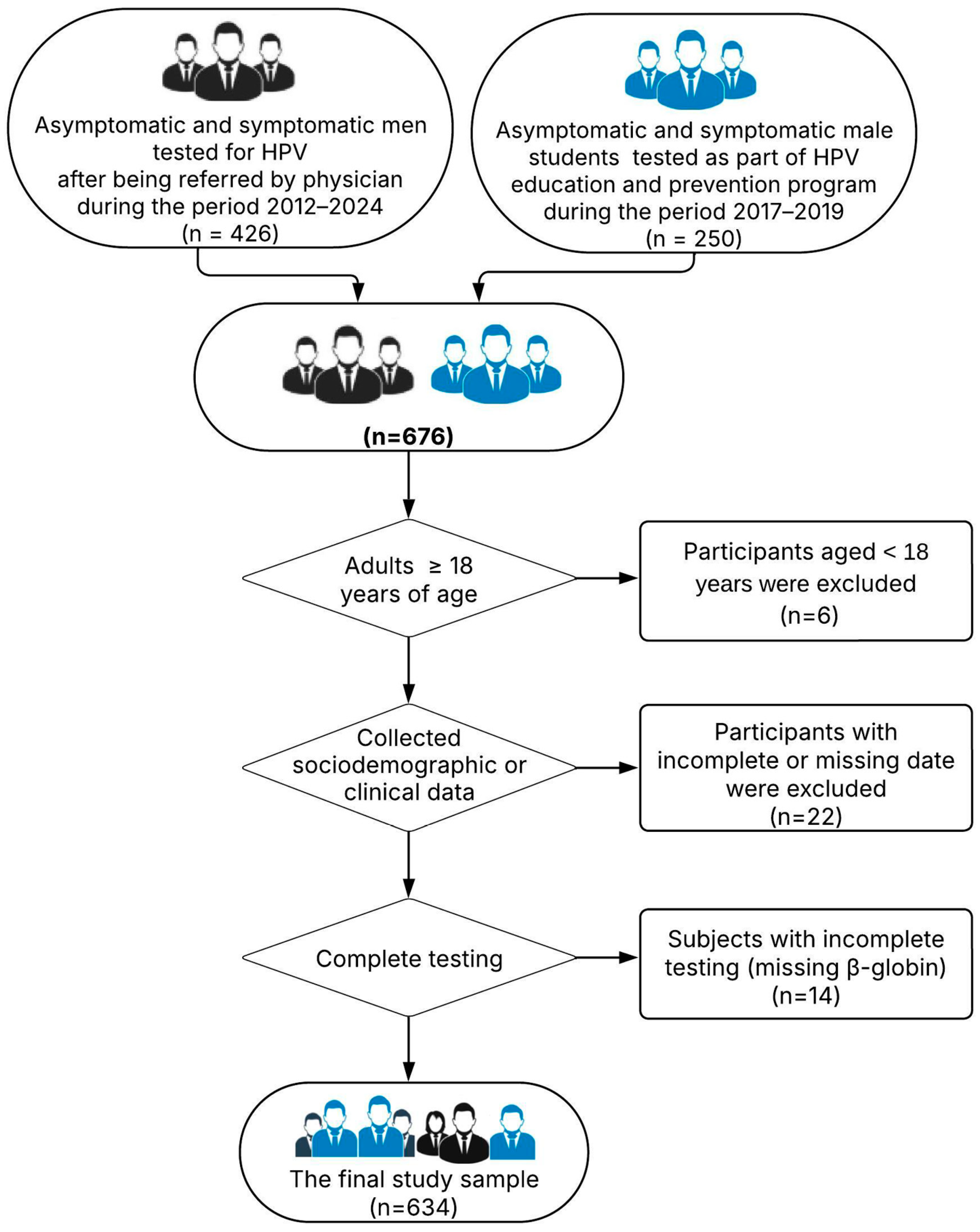
2.1. Study Design
2.2. Sample Collection
2.3. HPV Detection and Genotyping
2.4. Ethical Aspect
2.5. Statistical Analyses
3. Results
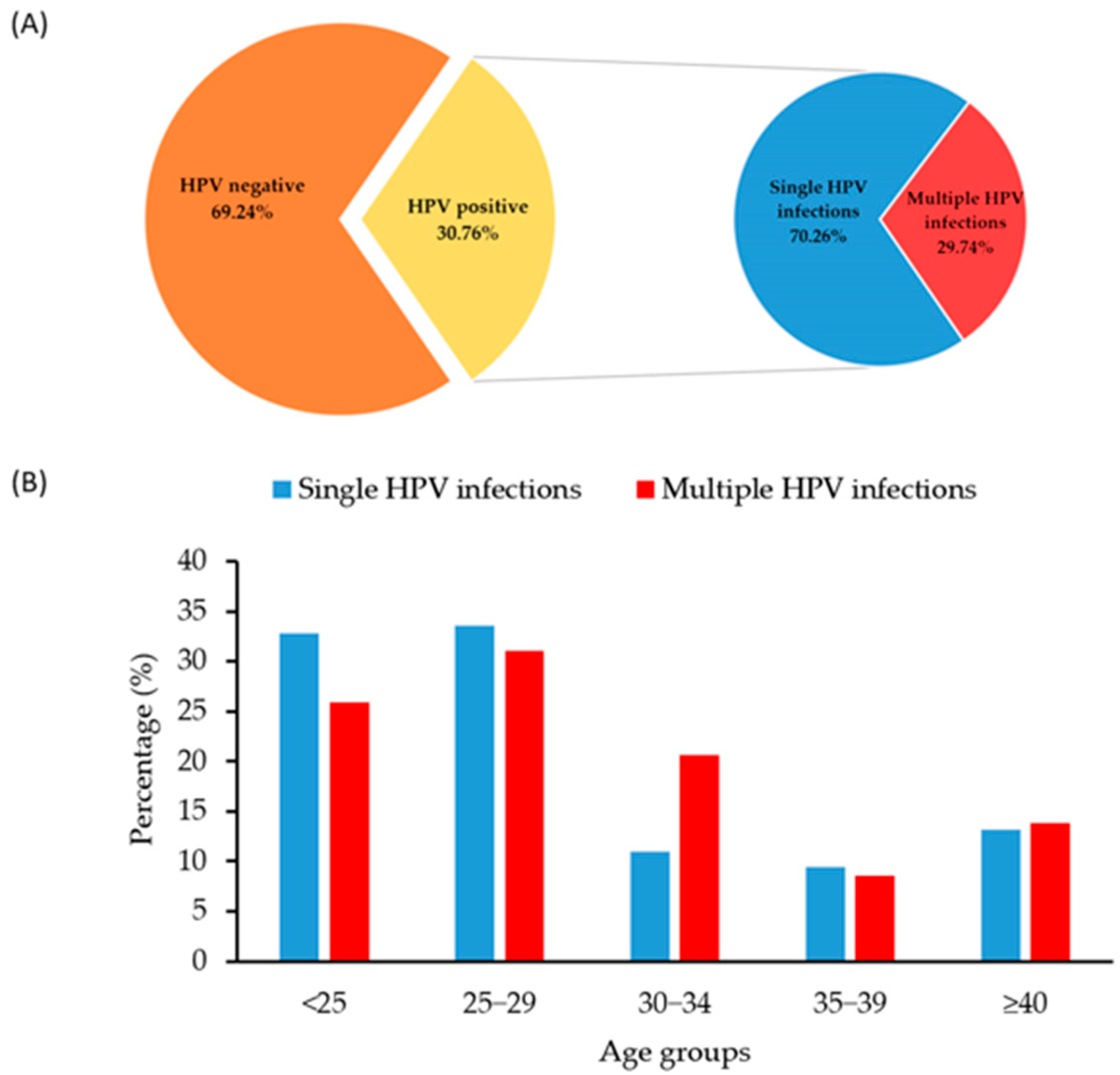
3.1. Overall HPV Distribution in the Analysed Samples
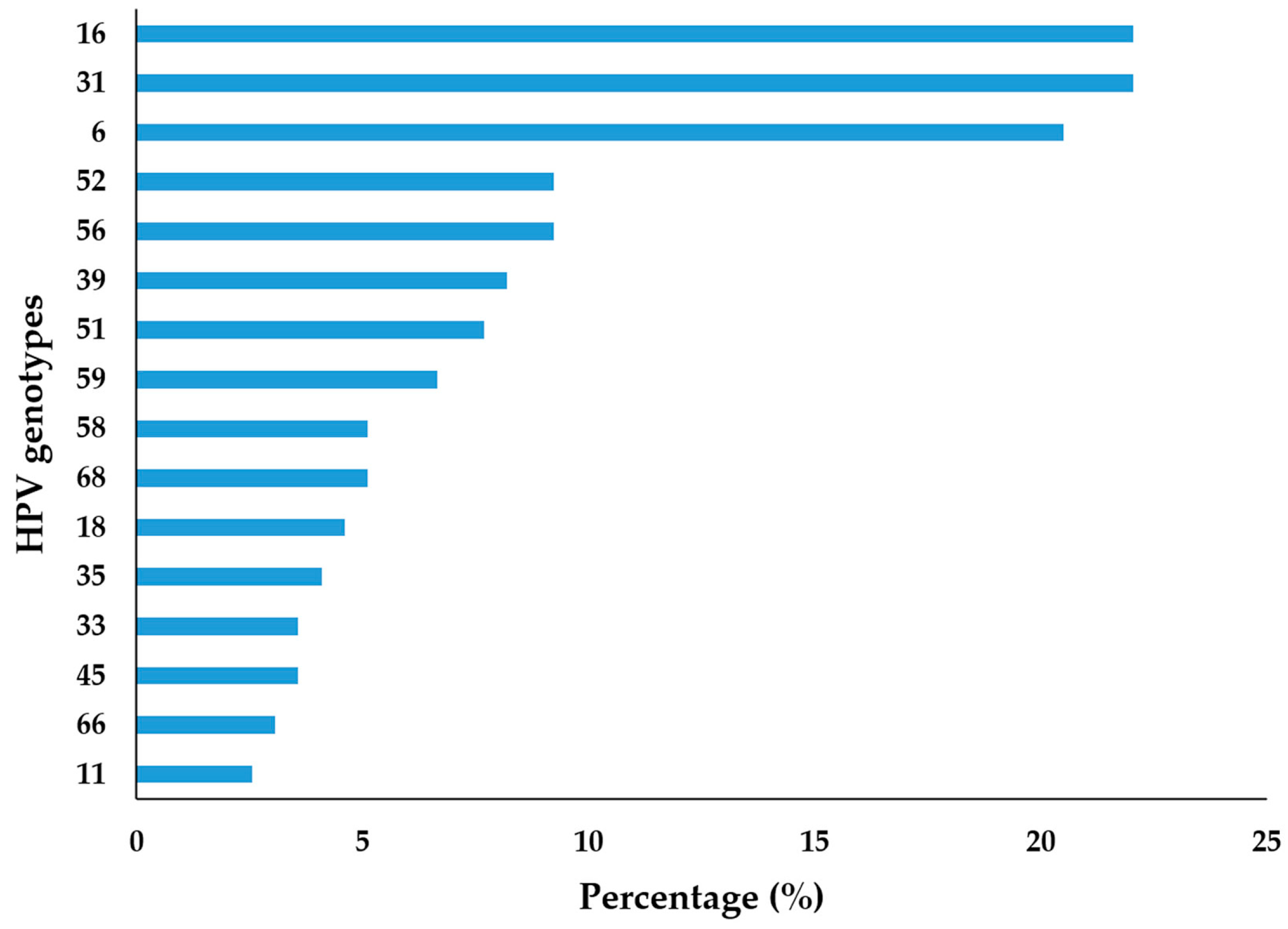
3.2. Genotype–Specific Distribution of Detected HPVs
3.3. Age–Specific Distribution of HPV
3.4. HPV Genotype Distribution According to Clinical Manifestation
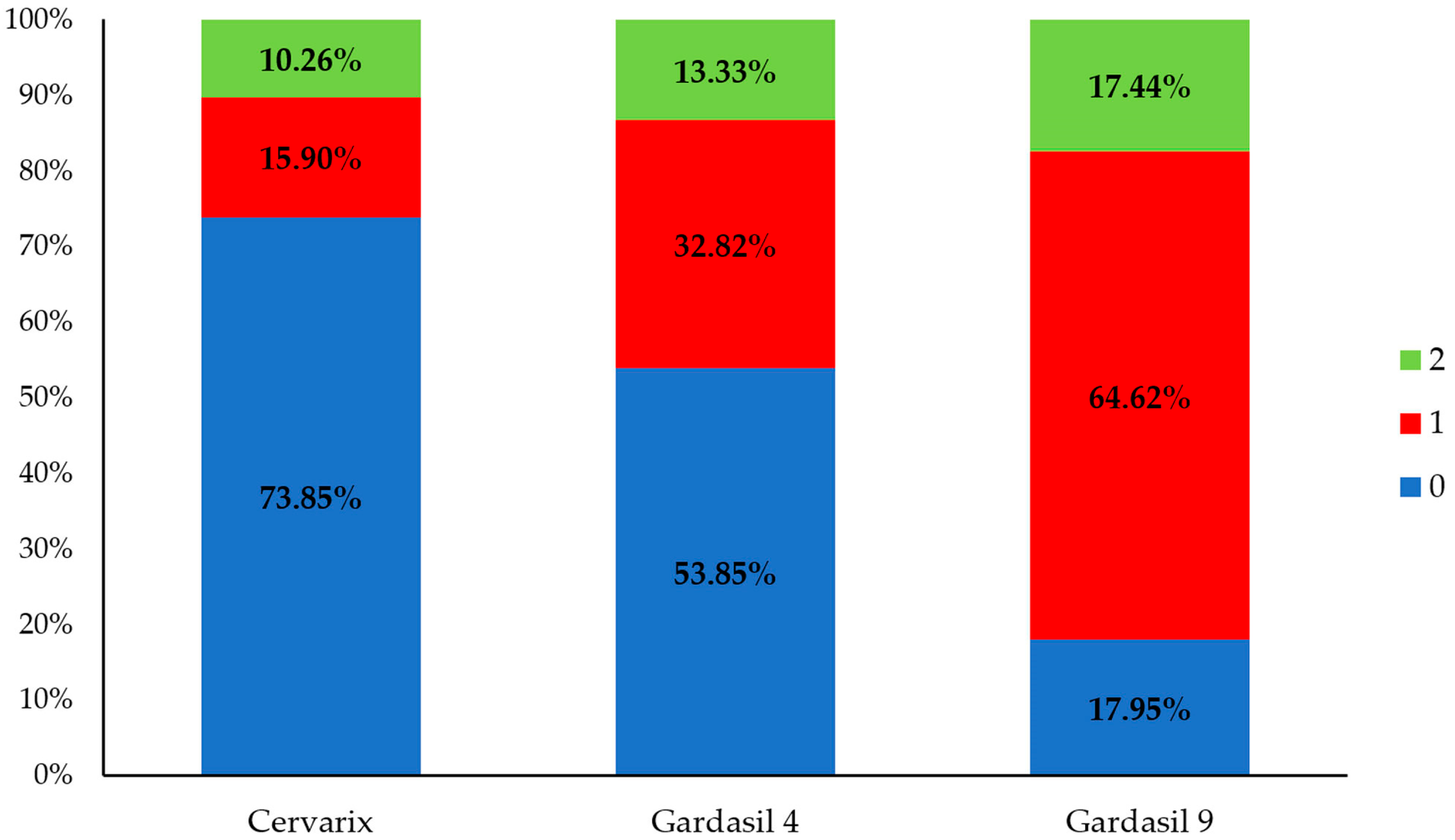
3.5. The Frequency of HPV Genotypes Covered by Some Licensed Prophylactic Vaccines
3.6. Association Between Age and HPV Positive Result
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| HPV | Human papillomavirus |
| HR–HPV | High–risk HPV types |
| LR–HPV | Low–risk HPV types |
| IPHIV | Institute for Public Health of Vojvodina |
References
- Milano, G.; Guarducci, G.; Nante, N.; Montomoli, E.; Manini, I. Human Papillomavirus Epidemiology and Prevention: Is There Still a Gender Gap? Vaccines 2023, 11, 1060. [Google Scholar] [CrossRef]
- Bruni, L.; Albero, G.; Rowley, J.; Alemany, L.; Arbyn, M.; Giuliano, A.R.; Markowitz, L.E.; Broutet, N.; Taylor, M. Global and regional estimates of genital human papillomavirus prevalence among men: A systematic review and meta-analysis. Lancet Glob. Health 2023, 11, e1345–e1362. [Google Scholar] [CrossRef]
- Giuliano, A.R.; Tortolero-Luna, G.; Ferrer, E.; Burchell, A.N.; de Sanjose, S.; Kjaer, S.K.; Muñoz, N.; Schiffman, M.; Bosch, F.X. Epidemiology of human papillomavirus infection in men, cancers other than cervical and benign conditions. Vaccine 2008, 26 (Suppl. 10), K17–K28. [Google Scholar] [CrossRef]
- de Martel, C.; Georges, D.; Bray, F.; Ferlay, J.; Clifford, G.M. Global burden of cancer attributable to infections in 2018: A worldwide incidence analysis. Lancet Glob. Health 2020, 8, e180–e190. [Google Scholar] [CrossRef]
- Deshmukh, A.A.; Damgacioglu, H.; Georges, D.; Sonawane, K.; Clifford, G.M. Human Papillomavirus-Associated Anal Cancer Incidence and Burden Among US Men, According to Sexual Orientation, Human Immunodeficiency Virus Status, and Age. Clin. Infect. Dis. 2023, 77, 419–424. [Google Scholar] [CrossRef]
- Lechner, M.; Liu, J.; Masterson, L.; Fenton, T.R. HPV-associated oropharyngeal cancer: Epidemiology, molecular biology and clinical management. Nat. Rev. Clin. Oncol. 2022, 19, 306–327. [Google Scholar] [CrossRef]
- Isaguliants, M.; Krasnyak, S.; Smirnova, O.; Colonna, V.; Apolikhin, O.; Buonaguro, F.M. Genetic instability and anti-HPV immune response as drivers of infertility associated with HPV infection. Infect. Agents Cancer 2021, 16, 29. [Google Scholar] [CrossRef]
- Cao, X.; Wei, R.; Zhang, X.; Zhou, J.; Lou, J.; Cui, Y. Impact of human papillomavirus infection in semen on sperm progressive motility in infertile men: A systematic review and meta-analysis. Reprod. Biol. Endocrinol. 2020, 18, 38. [Google Scholar] [CrossRef]
- de Martel, C.; Plummer, M.; Vignat, J.; Franceschi, S. Worldwide burden of cancer attributable to HPV by site, country and HPV type. Int. J. Cancer 2017, 141, 664–670. [Google Scholar] [CrossRef]
- Galati, L.; Chiocca, S.; Duca, D.; Tagliabue, M.; Simoens, C.; Gheit, T.; Arbyn, M.; Tommasino, M. HPV and head and neck cancers: Towards early diagnosis and prevention. Tumor Virus Res. 2022, 14, 200245. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. HPV and Men. CDC Fact Sheet. 2022. Available online: https://www.cdc.gov/sti/?CDC_AAref_Val=https://www.cdc.gov/std/hpv/stdfact-hpv-and-men.htm (accessed on 18 April 2022).
- Vives, A.; Cosentino, M.; Palou, J. The role of human papilloma virus test in men: First exhaustive review of literature. Actas Urol. Esp. (Engl. Ed.) 2020, 44, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Zou, K.; Huang, Y.; Li, Z. Prevention and treatment of human papillomavirus in men benefits both men and women. Front. Cell Infect. Microbiol. 2022, 12, 1750. [Google Scholar] [CrossRef] [PubMed]
- Meites, E.; Szilagyi, P.G.; Chesson, H.W.; Unger, E.R.; Romero, J.R.; Markowitz, L.E. Human Papillomavirus Vaccination for Adults: Updated Recommendations of the Advisory Committee on Immunization Practices. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 698–702. [Google Scholar] [CrossRef]
- Naidoo, D.; Govender, K.; Mantell, J.E. Breaking barriers: Why including boys and men is key to HPV prevention. BMC Med. 2024, 22, 525. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health of the Republic of Serbia. Law on the Protection of the Population from Infectious Diseases: 15/2016-31, 68/2020-4, 136/2020-3. Available online: https://www.pravno-informacioni-sistem.rs/SlGlasnikPortal/eli/rep/sgrs/skupstina/zakon/2016/15/8/reg (accessed on 16 January 2023).
- Štrbac, M.; Vuković, V.; Pustahija, T.; Nikolić, N.; Rajčević, S.; Ilić, S.; Dugandžija, T.; Patić, A.; Ristić, M.; Petrović, V. Motives and attitudes of parents towards HPV vaccination: Results from the initial period of HPV vaccine rollout in Serbia. PLoS ONE 2023, 18, e0287295. [Google Scholar] [CrossRef]
- Bosnjak, Z.; Peric, M.; Krizan, I.R.; Džijan, S.; Ružman, N.; Pastuović, T.; Šarkanj, B.; Bertić, V.; Burian, S.; Vuković, D. Prevalence and genotype distribution of high-risk human papillomavirus (HR HPV) in male genital samples of Osijek-Baranja County. Coll. Anthropol. 2013, 37, 1203–1208. [Google Scholar]
- Jaworek, H.; Koudelakova, V.; Oborna, I.; Zborilova, B.; Brezinova, J.; Ruzickova, D.; Vrbkova, J.; Kourilova, P. Prevalence and genotype distribution of human papillomavirus in Czech non-vaccinated heterosexual couples. Virol. J. 2021, 18, 80. [Google Scholar] [CrossRef]
- Golob, B.; Poljak, M.; Verdenik, I.; Kolbezen Simoniti, M.; Vrtačnik Bokal, E.; Zorn, B. High HPV infection prevalence in men from infertile couples and lack of relationship between seminal HPV infection and sperm quality. Biomed Res. Int. 2014, 2014, 956901. [Google Scholar] [CrossRef]
- Giuliano, A.R.; Nielson, C.M.; Flores, R.; Dunne, E.F.; Abrahamsen, M.; Papenfuss, M.R.; Harris, R.B. The optimal anatomic sites for sampling heterosexual men for human papillomavirus (HPV) detection: The HPV detection in men study. J. Infect. Dis. 2007, 196, 1146–1152. [Google Scholar] [CrossRef]
- Nicolau, S.M.; Camargo, C.G.; Stavale, J.N.; Castelo, A.; Dôres, G.B.; Lörincz, A.; de Lima, G.R. Human papillomavirus DNA detection in male sexual partners of women with genital human papillomavirus infection. Urology 2005, 65, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Nikolic, N.; Basica, B.; Strbac, M.; Terzic, L.; Patic, A.; Kovacevic, G.; Velicki, R.; Petrovic, D.; Mandic, A.; Petrovic, V. Prevalence of Carcinogenic Genotypes of HPV-Infected Women in a Ten-Year Period (2014-2023) in Vojvodina, Serbia. Medicina 2024, 60, 922. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ingles, D.J.; Lin, H.Y.; Fulp, W.J.; Sudenga, S.L.; Lu, B.; Schabath, M.B.; Papenfuss, M.R.; Abrahamsen, M.E.; Salmeron, J.; Villa, L.L.; et al. An Analysis of HPV Infection Incidence and Clearance by Genotype and Age in Men: The HPV Infection in Men (HIM) Study. Papillomavirus Res. 2015, 1, 126–135. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bogani, G.; Ghelardi, A.; Sopracordevole, F.; Annoni, M.; Ciavattini, A.; Giannella, L.; De Vincenzo, R.; Cattani, P.; Barbero, M.; Vercellini, P.; et al. Human papillomavirus (HPV) vaccination: A call for action in Italy. Int. J. Gynecol. Cancer 2023, 33, 1132–1139. [Google Scholar] [CrossRef]
- Rosen, B.L.; Gorbach, P.; Ding, L.; Covert, C.; Ermel, A.C.; Chandler, E.; Malagón, T.; Kahn, J.A. Sexual Network Patterns and Their Association With Genital and Anal Human Papillomavirus Infection in Adolescent and Young Men. J. Adolesc. Health 2021, 68, 696–704. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kjaer, S.K.; Munk, C.; Falck Winther, J.; Jørgensen, H.O.; Meijer, C.J.; van den Brule, A.J. Acquisition and Persistence of Human Papillomavirus Infection in Younger Men: A Prospective Follow-Up Study Among Danish Soldiers. Cancer Epidemiol. Biomark. Prev. 2005, 14, 1528–1533. [Google Scholar] [CrossRef]
- Dunne, E.F.; Nielson, C.M.; Stone, K.M.; Markowitz, L.E.; Giuliano, A.R. Prevalence of HPV Infection Among Men: A Systematic Review of the Literature. J. Infect. Dis. 2006, 194, 1044–1057. [Google Scholar] [CrossRef]
- Anic, G.M.; Lee, J.H.; Villa, L.L.; Lazcano-Ponce, E.; Gage, C.; José, C.; Silva, R.; Baggio, M.L.; Quiterio, M.; Salmerón, J.; et al. Risk Factors for Incident Condyloma in a Multinational Cohort of Men: The HIM Study. J. Infect. Dis. 2012, 205, 789–793. [Google Scholar] [CrossRef]
- Liu, P.; Yang, X.; Zhao, H.; Liang, L.; Chen, M.; Yin, A. High Burden of Human Papillomavirus Infection Among Men in Guangzhou, South China: Implications for HPV Vaccination Strategies. Hum. Vaccin. Immunother. 2024, 20, 2337161. [Google Scholar] [CrossRef]
- Shapiro, S.B.; Wissing, M.D.; Khosrow-Khavar, F.; El-Zein, M.; Burchell, A.N.; Tellier, P.P.; Coutlée, F.; Franco, E.L. Male Circumcision and Genital Human Papillomavirus (HPV) Infection in Males and Their Female Sexual Partners: Findings From the HPV Infection and Transmission Among Couples Through Heterosexual Activity (HITCH) Cohort Study. J. Infect. Dis. 2022, 226, 1184–1194. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Stuhmer, A. Balanitis Xerotica Obliterans (Post-Operationem) und Ihre Beziehungen zur “Kraurosis Glandis et Praeputic Penis”. Arch. Dermatol. Syp. 1998, 156, 613–623. [Google Scholar] [CrossRef]
- Kidd, L.C.; Chaing, S.; Chipollini, J.; Giuliano, A.R.; Spiess, P.E.; Sharma, P. Relationship Between Human Papillomavirus and Penile Cancer-Implications for Prevention and Treatment. Transl. Androl. Urol. 2017, 6, 791–802. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Opeyemi Bello, R.; Willis-Powell, L.; James, O.; Sharma, A.; Marsh, E.; Ellis, L.; Gaston, K.; Siddiqui, Y. Does Human Papillomavirus Play a Causative Role in Prostate Cancer? A Systematic Review Using Bradford Hill’s Criteria. Cancers 2023, 15, 3897. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Khatami, A.; Salavatiha, Z.; Razizadeh, M.H. Bladder Cancer and Human Papillomavirus Association: A Systematic Review and Meta-Analysis. Infect. Agents Cancer 2022, 17, 3. [Google Scholar] [CrossRef]
- Baker, P.; Winterflood, D. Boys, Men and HPV: A Call for Global Gender-Neutral HPV Vaccination. Global Action on Men’s Health and NOMAN Is an Island: Race to End HPV; London, UK, 2024. Available online: https://www.endhpvglobal.org/_files/ugd/8024e3_e31b0f82ada74f44bb0033bdd625d4b8.pdf (accessed on 11 December 2024).
- Burd, E.M. Human Papillomavirus and Cervical Cancer. Clin. Microbiol. Rev. 2003, 16, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Dykens, J.A.; Peterson, C.E.; Holt, H.K.; Harper, D.M. Gender Neutral HPV Vaccination Programs: Reconsidering Policies to Expand Cancer Prevention Globally. Front. Public Health 2023, 11, 1067299. [Google Scholar] [CrossRef]
- Williamson, A.L. Recent Developments in Human Papillomavirus (HPV) Vaccinology. Viruses 2023, 15, 1440. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Group | HPV (Any) Positive, n (%) | HPV Negative, n (%) | Total, n (%) | p-Value * | HR–HPV, n (%) | (Only) LR–HPV, n (%) | Total, n (%) | p-Value * |
|---|---|---|---|---|---|---|---|---|
| <25 | 60 (30.77) | 168 (38.27) | 228 (35.96) | 0.256 | 41 (24.85) | 19 (63.33) | 60 (30.77) | <0.001 |
| 25–29 | 64 (32.82) | 109 (24.83) | 173 (27.29) | 57 (34.55) | 7 (23.33) | 64 (32.82) | ||
| 30–34 | 27 (13.85) | 63 (14.35) | 90 (14.20) | 26 (15.76) | 1 (3.33) | 27 (13.85) | ||
| 35–39 | 18 (9.23) | 42 (9.57) | 60 (9.46) | 15 (9.09) | 3 (10.00) | 18 (9.23) | ||
| ≥40 | 26 (13.33) | 57 (12.98) | 83 (13.09) | 26 (15.76) | 0 (0) | 26 (13.33) | ||
| total | 195 (100) | 439 (100) | 634 (100) | 165 (100) | 30 (100) | 195 (100) |
| HPV Genotype | Total, n (%) | Age Category, n (%) | p-Value * | |
|---|---|---|---|---|
| 18–30 Years | >30 Years | |||
| HPV 6 | 40 (20.51) | 37 (28.91) | 3 (4.48) | <0.001 |
| HPV 11 | 5 (2.56) | 4 (3.13) | 1 (1.49) | 0.662 |
| HPV 16 | 43 (22.05) | 28 (21.88) | 15 (22.39) | 0.935 |
| HPV 18 | 9 (4.62) | 4 (3.13) | 5 (7.46) | 0.279 |
| HPV 31 | 43 (22.05) | 21 (16.41) | 22 (32.84) | 0.009 |
| HPV 33 | 7 (3.59) | 6 (4.69) | 1 (1.49) | 0.425 |
| HPV 35 | 8 (4.10) | 6 (4.69) | 2 (2.99) | 0.717 |
| HPV 39 | 16 (8.21) | 7 (5.47) | 9 (13.43) | 0.054 |
| HPV 45 | 8 (4.10) | 5 (3.91) | 3 (4.48) | 0.999 |
| HPV 51 | 15 (7.69) | 11 (8.59) | 4 (5.97) | 0.514 |
| HPV 52 | 18 (9.23) | 12 (9.38) | 6 (8.96) | 0.923 |
| HPV 56 | 18 (9.23) | 12 (9.38) | 6 (8.96) | 0.923 |
| HPV 58 | 10 (5.13) | 6 (4.69) | 4 (5.97) | 0.739 |
| HPV 59 | 13 (6.67) | 5 (3.91) | 8 (11.94) | 0.065 |
| HPV 66 | 6 (3.08) | 3 (2.34) | 3 (4.48) | 0.415 |
| HPV 68 | 10 (5.13) | 2 (1.56) | 8 (11.94) | 0.003 |
| Diagnostic Category | Age Category (Years), n (%) | Total n (%) | χ2 | p-Value | ||||
|---|---|---|---|---|---|---|---|---|
| <25 | 25–29 | 30–34 | 35–39 | ≥40 | ||||
| Asymptomatic | 36 (60.00) | 36 (56.25) | 12 (44.44) | 5 (27.78) | 6 (23.08) | 95 (48.72) | 14.71 | 0.0053 ** |
| Symptomatic | 24 (40.00) | 28 (43.75) | 15 (55.56) | 13 (72.22) | 20 (76.92) | 100 (51.28) | ||
| Total | 60 (30.77) | 64 (32.82) | 27 (13.85) | 18 (9.23) | 26 (13.33) | 195 (100) | ||
| Variables | Any HPV | Multiple HPV | HR–HPV Tip | |||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| age, years | 1.01 (0.99–1.03) | 0.222 | 1.01 (0.98–1.03) | 0.593 | 1.02 (1.01–1.04) | 0.01 |
| Age category | ||||||
| <25 | ref | ref | ref | |||
| 25–29 | 1.64 (1.07–2.52) | 0.022 | 1.65 (0.81–3.37) | 0.171 | 2.24 (1.41–3.56) | 0.001 |
| 30–34 | 1.20 (0.70–2.06) | 0.507 | 2.18 (0.98–4.87) | 0.056 | 1.85 (1.05–3.27) | 0.033 |
| 35–39 | 1.20 (0.64–2.24) | 0.568 | 1.29 (0.45–3.71) | 0.635 | 1.52 (0.77–2.99) | 0.224 |
| ≥40 | 1.28 (0.74–2.21) | 0.383 | 1.52 (0.62–3.72) | 0.365 | 2.08 (1.17–3.69) | 0.012 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kovačević, G.; Vuković, V.; Nikolić, N.; Bašica, B.; Radovanov, J.; Čolović Popadić, A.; Pejaković Budinski, M.; Dugandžija, T.; Golušin, Z.; Patić, A. Detection of Human Papillomavirus in Urogenital Swabs from Male Patients in Northern Serbia. Pathogens 2025, 14, 558. https://doi.org/10.3390/pathogens14060558
Kovačević G, Vuković V, Nikolić N, Bašica B, Radovanov J, Čolović Popadić A, Pejaković Budinski M, Dugandžija T, Golušin Z, Patić A. Detection of Human Papillomavirus in Urogenital Swabs from Male Patients in Northern Serbia. Pathogens. 2025; 14(6):558. https://doi.org/10.3390/pathogens14060558
Chicago/Turabian StyleKovačević, Gordana, Vladimir Vuković, Nataša Nikolić, Branka Bašica, Jelena Radovanov, Aleksandra Čolović Popadić, Milica Pejaković Budinski, Tihomir Dugandžija, Zoran Golušin, and Aleksandra Patić. 2025. "Detection of Human Papillomavirus in Urogenital Swabs from Male Patients in Northern Serbia" Pathogens 14, no. 6: 558. https://doi.org/10.3390/pathogens14060558
APA StyleKovačević, G., Vuković, V., Nikolić, N., Bašica, B., Radovanov, J., Čolović Popadić, A., Pejaković Budinski, M., Dugandžija, T., Golušin, Z., & Patić, A. (2025). Detection of Human Papillomavirus in Urogenital Swabs from Male Patients in Northern Serbia. Pathogens, 14(6), 558. https://doi.org/10.3390/pathogens14060558