
Evaluation of the Standard M10 MTB/NTM Molecular Test for the Rapid Identification of Tuberculous and Nontuberculous Mycobacteria in Liquid Cultures

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Clinical Samples
2.2. All-in-One Mycobacteria Real-Time PCR System
- (1)
- Stability time was determined by evaluating the reliability of the MTB/NTM culture sample treated with the sample reagent (SR) at a 1:3 dilution (as recommended by the manufacturer [17]) at various times (from 15 min to 4 h) before performing real-time PCR using the MTB/NTM cartridge. The manufacturer suggested an incubation time of about 15 min.
- (2)
- The culture dilution process is a crucial aspect of the overall methodology. The manufacturer’s recommended sample dilution was 1:3 with the sample reagent when applied to sputum. To assess any potential loss of sensitivity in the culture setting, higher dilutions of the MGIT culture were performed, ranging from 1:2 to 1:16.
- (3)
- The impact of mixed strains on interferences and sensitivity was investigated. The specificity of the SD Biosensor Standard M10 MTB/NTM Kit (SD Biosensor Inc., Suwon, Republic of Korea) was examined by creating mixed cultures (MTB/NTM ratio 4:8–4:16, and vice versa) to confirm the system’s capacity to detect these cultures appropriately.
- (4)
- The safety of operators was assessed by evaluating the inactivating capacity of the solubilizing reagent against mycobacterial cultures. A portion of the aliquot treated with the sample reagent was re-cultured to ascertain the inactivating capacity of the reagent.
2.3. Immunochromatography Test for MPT64 Antigen Detection
2.4. Statistical Analysis
3. Results
3.1. Preliminary Results Described Good Specificity and Stability of the SD Biosensor Standard M10 MTB/NTM Test on MGIT Culture
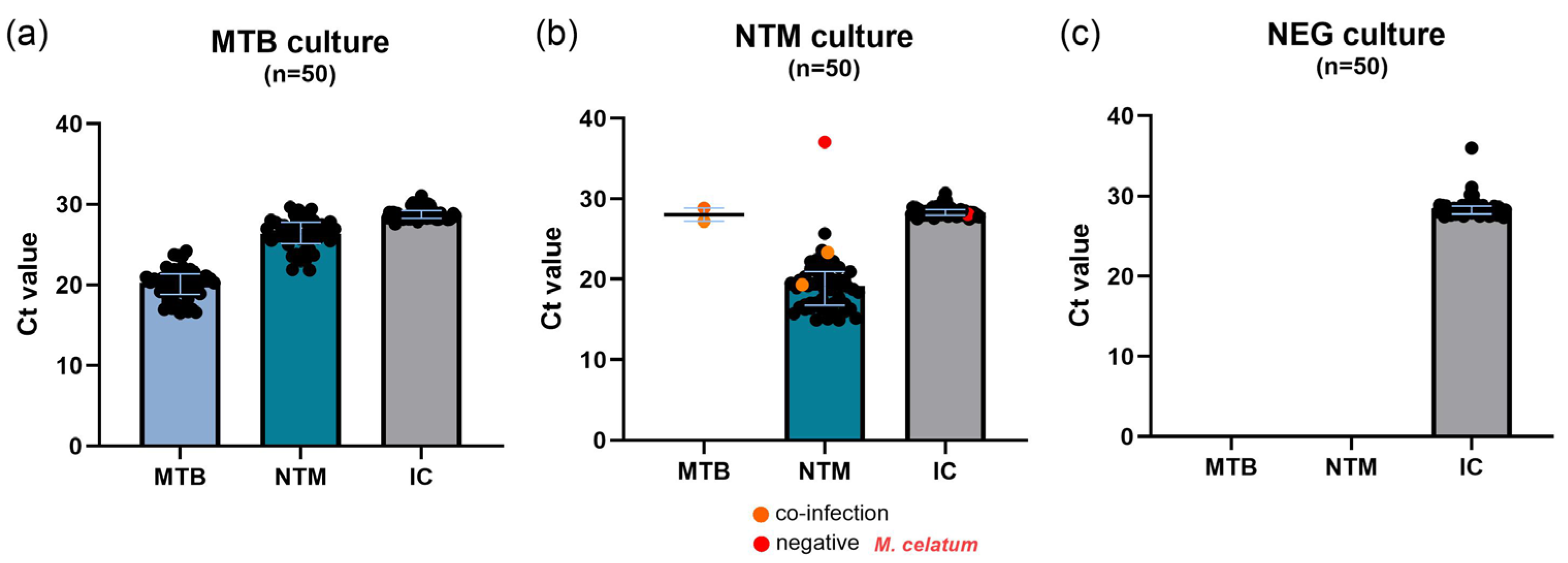
3.2. The SD Biosensor Standard M10 MTB/NTM Test Shows High Specificity for MTB on MGIT Culture
3.3. The Antigenic Test Correctly Identified the MTB Culture
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| MTBC | Mycobacterium tuberculosis complex |
| MTB | Mycobacterium tuberculosis |
| NTM | Non-Tuberculous Mycobacteria |
| MGIT | Mycobacteria Growth Indicator Tube |
| PCR | Polymerase Chain Reaction |
| WHO | World Health Organization |
| POCT | Point Of Care Test |
| ICTs | Immunochromatography Tests |
| TB | Tuberculosis |
| RIF | Rifampicin |
| Ct | Cycle Threshold |
| BSL3 | BioSafety Level 3 Laboratory |
| SD | Standard Deviation |
| CIs | Confidence Intervals |
References
- Tobin, E.H.; Tristram, D. Tuberculosis Overview. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2025. Available online: https://www.ncbi.nlm.nih.gov/books/NBK441916/ (accessed on 15 March 2025).
- Bethencourt Mirabal, A.; Nguyen, A.D.; Ferrer, G. Lung Nontuberculous Mycobacterial Infections. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2025. Available online: https://www.ncbi.nlm.nih.gov/books/NBK551583/ (accessed on 15 March 2025).
- Loebinger, M.R.; Welte, T. Current Perspectives in the Diagnosis and Treatment of Nontuberculous Mycobacterial Pulmonary Disease. Eur. Respir. Pulm. Dis. 2016, 2, 54. [Google Scholar] [CrossRef]
- Jing, H.; Wang, H.; Wang, Y.; Deng, Y.; Li, X.; Liu, Z.; Graviss, E.A.; Ma, X. Prevalence of Nontuberculous Mycobacteria Infection, China, 2004–2009. Emerg. Infect. Dis. 2012, 18, 527–528. [Google Scholar] [CrossRef] [PubMed]
- Gopalaswamy, R.; Shanmugam, S.; Mondal, R.; Subbian, S. Of Tuberculosis and Non-Tuberculous Mycobacterial Infections—A Comparative Analysis of Epidemiology, Diagnosis and Treatment. J. Biomed. Sci. 2020, 27, 74. [Google Scholar] [CrossRef]
- Kumar, K.; Ponnuswamy, A.; Capstick, T.G.; Chen, C.; McCabe, D.; Hurst, R.; Morrison, L.; Moore, F.; Gallardo, M.; Keane, J.; et al. Non-Tuberculous Mycobacterial Pulmonary Disease (NTM-PD): Epidemiology, Diagnosis and Multidisciplinary Management. Clin. Med. 2024, 24, 100017. [Google Scholar] [CrossRef] [PubMed]
- Aliberti, S.; Codecasa, L.R.; Gori, A.; Sotgiu, G.; Spotti, M.; Di Biagio, A.; Calcagno, A.; Nardini, S.; Assael, B.M.; Tortoli, E.; et al. The Italian Registry of Pulmonary Non-Tuberculous Mycobacteria—IRENE: The Study Protocol. Multidiscip. Respir. Med. 2018, 13, 33. [Google Scholar] [CrossRef]
- Giannoni, F.; Lanni, A.; Iacobino, A.; Fattorini, L.; Italian Multicentre Study on Nontuberculous Mycobacteria (IMS-NTM); members of the IMS-NTM laboratory network. Epidemiology and Drug Susceptibility of Nontuberculous Mycobacteria (NTM) in Italy in 2016–2020. Ann. Ist. Super. Sanita 2023, 59, 132–138. [Google Scholar] [CrossRef]
- Sharma, S.K.; Upadhyay, V. Epidemiology, Diagnosis & Treatment of Non-Tuberculous Mycobacterial Diseases. Indian J. Med. Res. 2020, 152, 185–226. [Google Scholar] [CrossRef] [PubMed]
- Stroffolini, G.; Lupia, T.; Gaviraghi, A.; Venuti, F.; Cinnirella, G.; Gori, A.; Spotti, M.; Blasi, F.; Codecasa, L.; Calcagno, A.; et al. Prescription Habits and Drugs Accessibility for the Treatment of Non-Tuberculous Mycobacteria Infections in Italy: A Multicentric Survey from the IRENE Study Group. Infection 2025, 53, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Phunpae, P.; Thongkum, W.; Panyasit, W.; Laopajon, W.; Takheaw, N.; Pata, S.; Yasamut, U.; Kasinrerk, W.; Tayapiwatana, C. Rapid Lateral Flow Test for Mycobacterium tuberculosis Complex and Non-Tuberculous Mycobacteria Differentiation. Appl. Microbiol. Biotechnol. 2024, 108, 456. [Google Scholar] [CrossRef]
- Lwoga, E.T.; Sangeda, R.Z. ICTs and Development in Developing Countries: A Systematic Review of Reviews. Electron. J. Inf. Syst. Dev. Ctries. 2019, 85, e12060. [Google Scholar] [CrossRef]
- Abdullah, A.; Sam, I.-C.; Ong, Y.J.; Theo, C.H.; Pukhari, M.H.; Chan, Y.F. Comparative Evaluation of a Standard M10 Assay with Xpert Xpress for the Rapid Molecular Diagnosis of SARS-CoV-2, Influenza A/B Virus, and Respiratory Syncytial Virus. Diagnostics 2023, 13, 3507. [Google Scholar] [CrossRef] [PubMed]
- Luukinen, B.; Aittoniemi, J.; Miikkulainen-Lahti, T.; Mentula, S.; Pätäri-Sampo, A. Evaluation of the STANDARD M10 MDR-TB and MTB/NTM Assays for the Detection of Mycobacterium Tuberculosis, Rifampicin and Isoniazid Resistance, and Nontuberculous Mycobacteria in a Low-Incidence Setting. J. Clin. Microbiol. 2024, 62, e00402-24. [Google Scholar] [CrossRef] [PubMed]
- Stephen, S.; Kadye, A.; Majuru, X.N.; Madamombe, T.; Sokwe, J.; Madondo, T.; Tinarwo, K.; Tsuvani, L.; Kawome, T.; Malunga, F.; et al. Diagnostic Performance of STANDARDTM M10 Multidrug-Resistant Tuberculosis Assay for Detection of Mycobacterium tuberculosis and Rifampicin and Isoniazid Resistance in Zimbabwe. Int. J. Mycobacteriology 2024, 13, 22–27. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Essential biosafety measures for TB laboratories. In Tuberculosis Laboratory Biosafety Manual; World Health Organization: Geneva, Switzerland, 2012. Available online: https://www.ncbi.nlm.nih.gov/books/NBK179129/ (accessed on 21 April 2025).
- STANDARDTM M10 MTB/NTM Manufacturer’s Recommendations. Available online: https://www.relabsrl.it/product/standard-m10-mtb-ntm/ (accessed on 21 April 2025).
- Banada, P.P.; Sivasubramani, S.K.; Blakemore, R.; Boehme, C.; Perkins, M.D.; Fennelly, K.; Alland, D. Containment of Bioaerosol Infection Risk by the Xpert MTB/RIF Assay and Its Applicability to Point-of-Care Settings. J. Clin. Microbiol. 2010, 48, 3551–3557. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Biological Matrices | NTM, n = 50 | MTB, n = 50 | NEG, n = 50 |
|---|---|---|---|
| Bronchial aspirate | 21 (42%) | 2 (4.0%) | 21 (42%) |
| Sputum | 12 (24%) | 32 (64.0%) | 10 (20%) |
| Bronchial lavage | 16 (32%) | 4 (8.0%) | 18 (36%) |
| Biopsy | 1 (2%) | 6 (12.0%) | 0 (0.0%) |
| Urine | 0 (0.0%) | 4 (8.0%) | 0 (0.0%) |
| Lymph node aspirate | 0 (0.0%) | 0 (0.0%) | 1 (2.0%) |
| Cerebrospinal fluid | 0 (0.0%) | 1 (2.0%) | 0 (0.0%) |
| Pleural fluid | 0 (0.0%) | 1 (2.0%) | 0 (0.0%) |
| NTM Strains | Freqs (% of Total) | |
|---|---|---|
| Mycobaterium avium complex | 21 | (42%) |
| Mycobaterium intracellulare | 7 | (14%) |
| Mycobaterium gordonae | 6 | (12%) |
| Mycobacteriodes abscessus | 4 | (8%) |
| Mycobaterium chimaera | 4 | (8%) |
| Mycolicibacterium fortuitum | 2 | (4%) |
| Mycobacterium intracellulare sub. M. chimaera | 1 | (2%) |
| Mycobaterium xenopi | 1 | (2%) |
| Mycobacteriodes chelonae | 1 | (2%) |
| Mycolicibacterium mucogenicum | 1 | (2%) |
| Mycobaterium simiae | 1 | (2%) |
| Mycobaterium celatum | 1 | (2%) |
| Time | Ct MTB | Ct NTM | Ct IC |
|---|---|---|---|
| 15 min * | neg | 19.76 | 26.85 |
| 1 h | neg | 19.87 | 27.59 |
| 2 h | neg | 19.77 | 27.20 |
| 3 h | neg | 19.71 | 27.86 |
| 4 h | neg | 19.43 | 27.32 |
| Sample:Reagent Ratio | Ct MTB | Ct NTM | Ct IC |
|---|---|---|---|
| 1:2 | neg | 21.39 | 28.26 |
| 1:4 | neg | 23.03 | 29.70 |
| 1:8 | neg | 22.38 | 27.33 |
| 1:16 | neg | 23.30 | 27.55 |
| MTB:NTM Ratio | Ct MTB | Ct NTM | Ct IC |
|---|---|---|---|
| 8:4 | 21.38 | 19.57 | 27.03 |
| 4:8 | 21.37 | 20.86 | 27.37 |
| 4:16 | 20.54 | 21.18 | 27.28 |
| 16:4 | 22.41 | 19.02 | 27.18 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caldrer, S.; Carrara, A.; Ragusa, A.; Nicolini, L.; Pomari, E.; Mazzi, C.; Formenti, F.; Perandin, F. Evaluation of the Standard M10 MTB/NTM Molecular Test for the Rapid Identification of Tuberculous and Nontuberculous Mycobacteria in Liquid Cultures. Pathogens 2025, 14, 517. https://doi.org/10.3390/pathogens14060517
Caldrer S, Carrara A, Ragusa A, Nicolini L, Pomari E, Mazzi C, Formenti F, Perandin F. Evaluation of the Standard M10 MTB/NTM Molecular Test for the Rapid Identification of Tuberculous and Nontuberculous Mycobacteria in Liquid Cultures. Pathogens. 2025; 14(6):517. https://doi.org/10.3390/pathogens14060517
Chicago/Turabian StyleCaldrer, Sara, Alberta Carrara, Andrea Ragusa, Lavinia Nicolini, Elena Pomari, Cristina Mazzi, Fabio Formenti, and Francesca Perandin. 2025. "Evaluation of the Standard M10 MTB/NTM Molecular Test for the Rapid Identification of Tuberculous and Nontuberculous Mycobacteria in Liquid Cultures" Pathogens 14, no. 6: 517. https://doi.org/10.3390/pathogens14060517
APA StyleCaldrer, S., Carrara, A., Ragusa, A., Nicolini, L., Pomari, E., Mazzi, C., Formenti, F., & Perandin, F. (2025). Evaluation of the Standard M10 MTB/NTM Molecular Test for the Rapid Identification of Tuberculous and Nontuberculous Mycobacteria in Liquid Cultures. Pathogens, 14(6), 517. https://doi.org/10.3390/pathogens14060517