

Association of Altered Baseline Hematological Parameters with Adverse Tuberculosis Treatment Outcomes

 , , , , , ,
, , , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Hematological Parameters
2.3. Statistical Data Analysis
3. Results
3.1. Characteristics of the Study Population
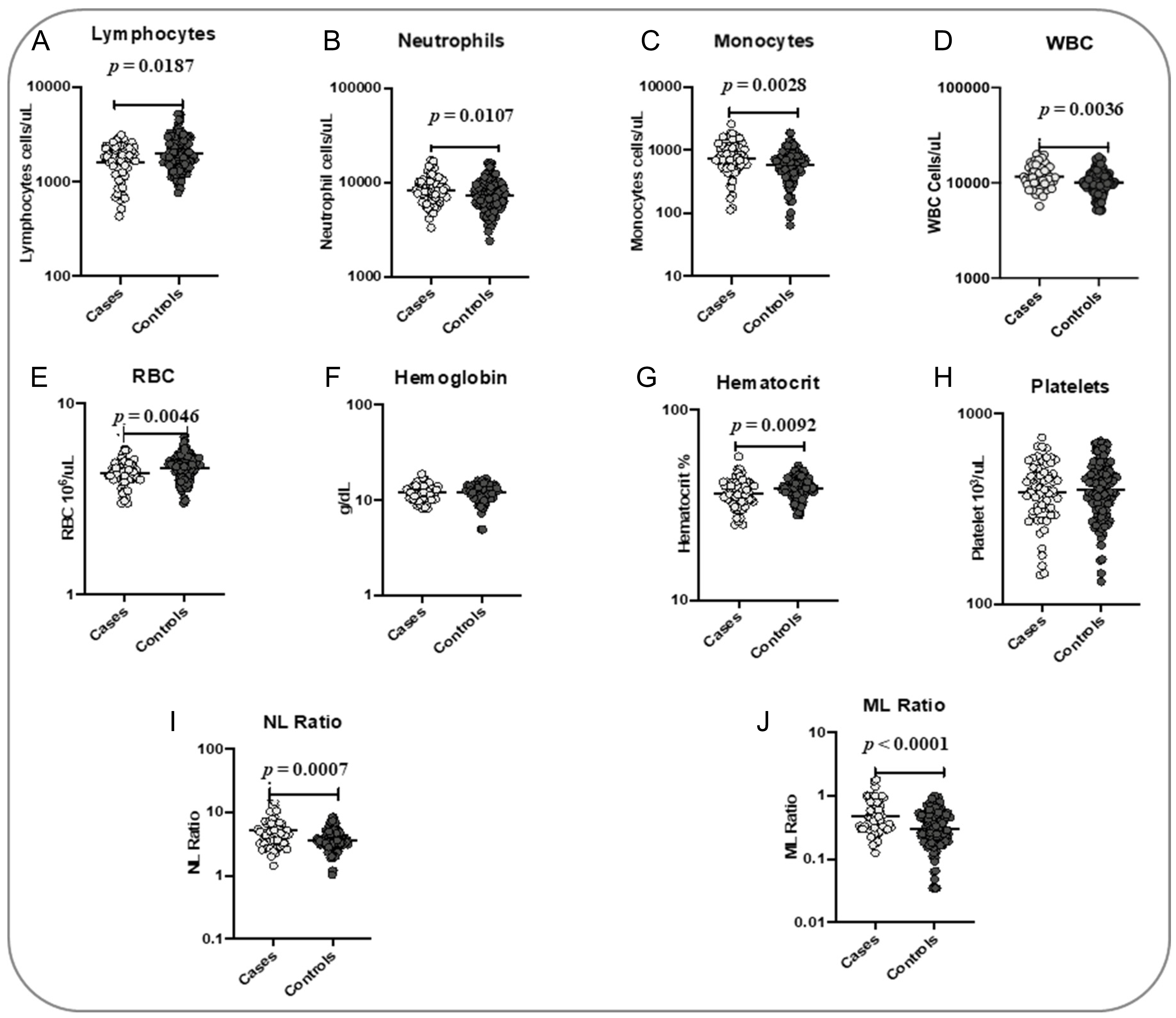
3.2. Association of Hematological Parameters with Poor Treatment Outcomes
3.3. Logistic Regression Analysis of the Association of Hematological Parameters with Treatment Outcomes
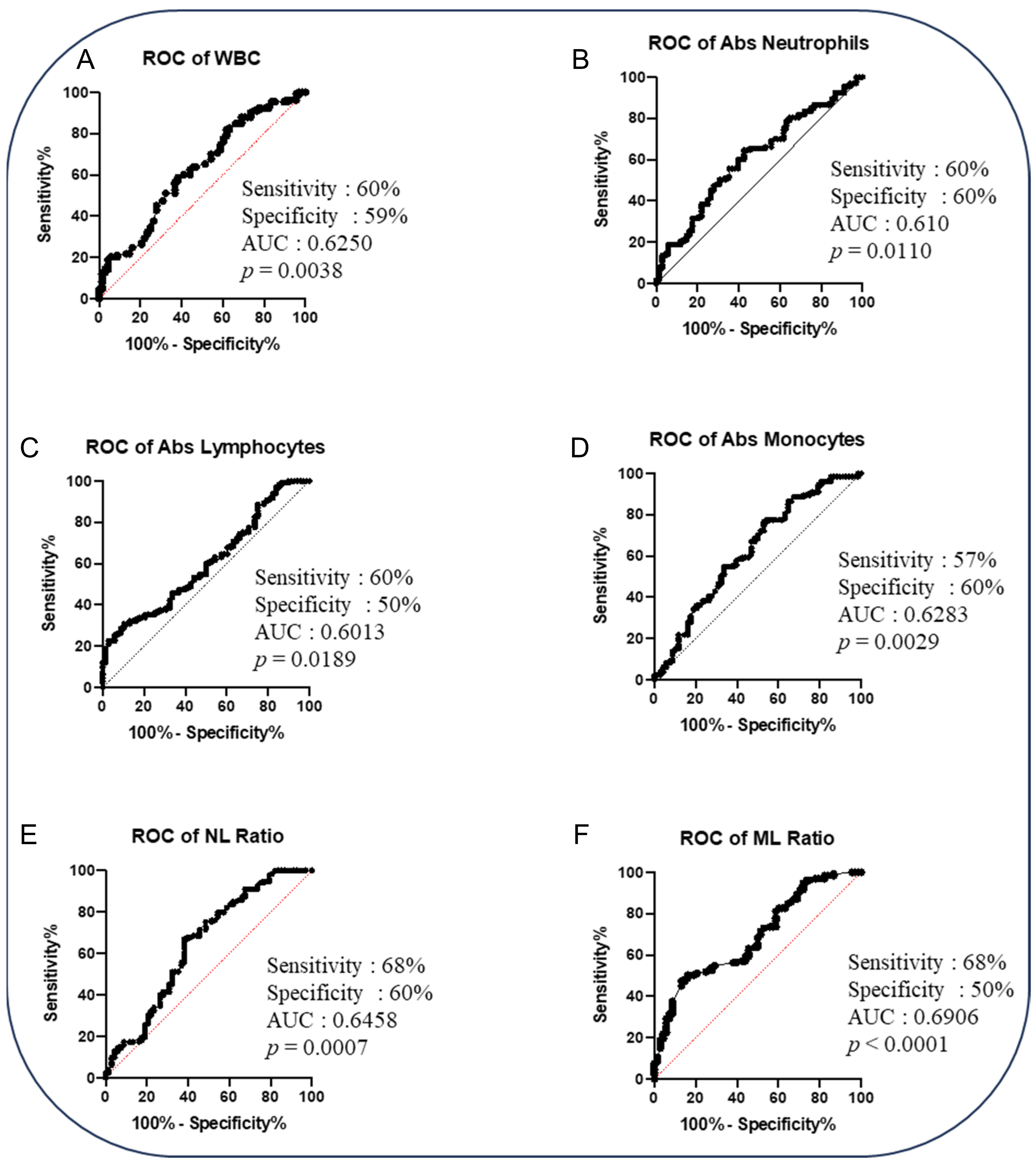
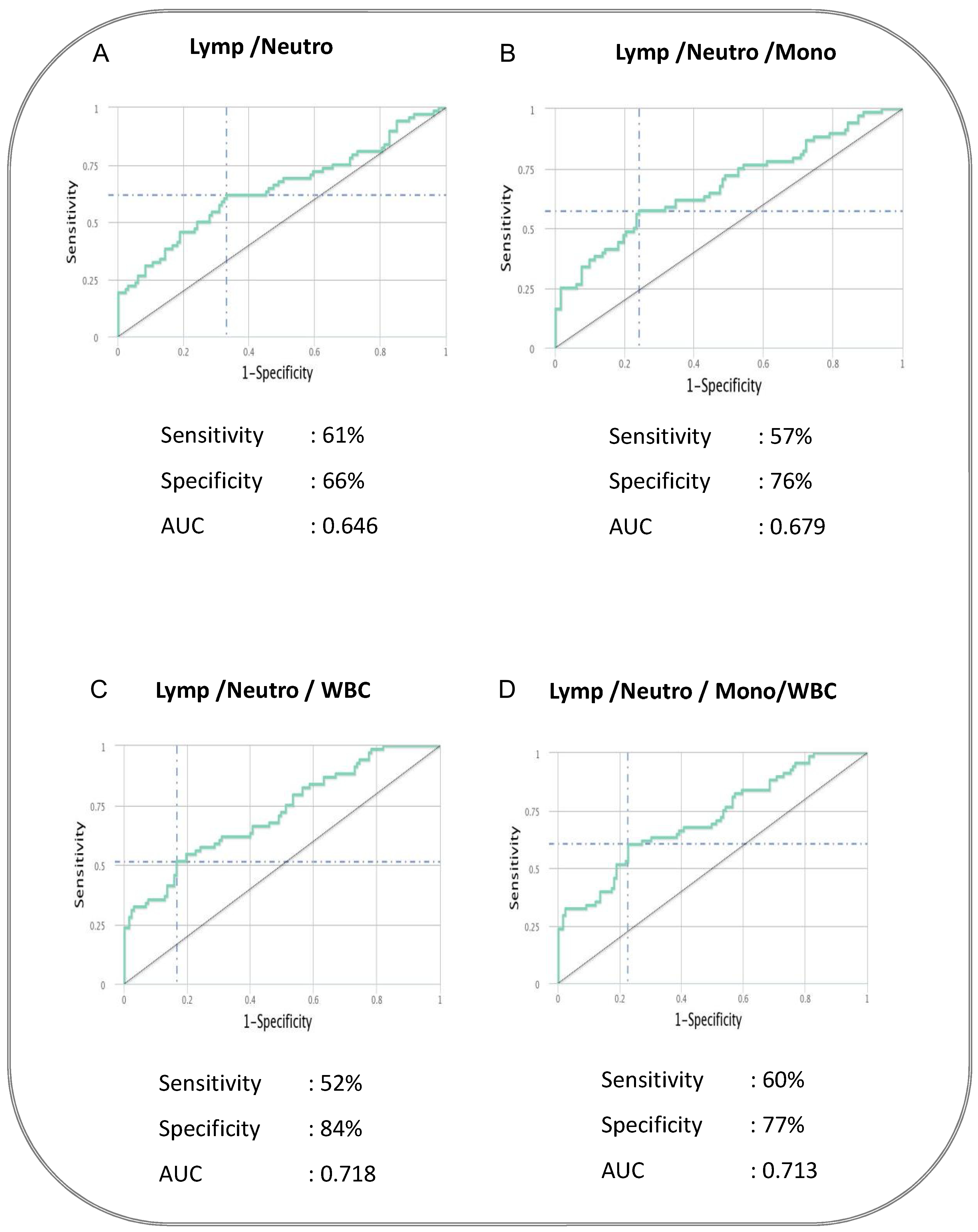
3.4. Baseline Signature of Two or Three Hematological Parameters Could Be a Predictive Biomarker Discriminating Adverse TB Treatment Outcome from PTB Cured Controls
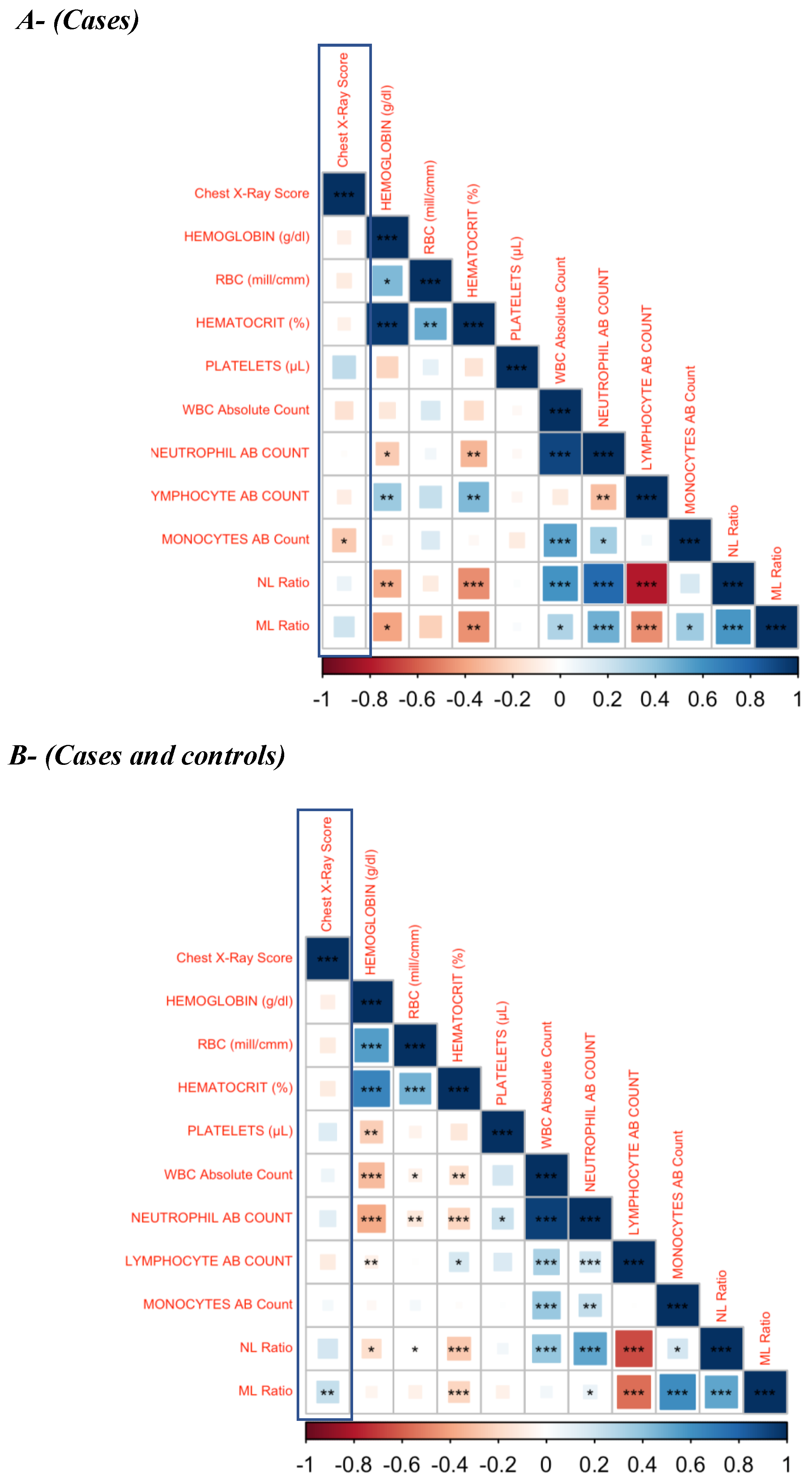
3.5. Baseline Hematological Parameters Are Weakly Correlated with the Chest X-Ray Score in Active PTB Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| TB | tuberculosis |
| PTB | pulmonary tuberculosis |
| WBC | white blood cells |
| ML | monocyte to lymphocyte |
| NL | neutrophil to lymphocyte |
| DOTS | Directly observed therapy short-course |
| CXR | Chest X-ray |
| NIRT | National Institute for Research in Tuberculosis |
| EDOT | Effect of Diabetes on Tuberculosis Severity |
| NTEP | National Tuberculosis Elimination Program |
| BMI | body mass index |
| CBC | Complete blood count |
| aOR | adjusted odds ratio |
| Hb | Hemoglobin |
| ESR | erythrocyte sedimentation rate |
| PCV | packed cell volume |
References
- WHO. Global Tuberculosis Report 2022; WHO Report; WHO: Gevena, Switzerland, 2022. [Google Scholar]
- Chakaya, J.; Petersen, E.; Nantanda, R.; Mungai, B.N.; Migliori, G.B.; Amanullah, F.; Lungu, P.; Ntoumi, F.; Kumarasamy, N.; Maeurer, M. The WHO Global Tuberculosis 2021 Report—Not so good news and turning the tide back to End TB. Int. J. Infect. Dis. 2022, 124 (Suppl. S1), S26–S29. [Google Scholar] [CrossRef] [PubMed]
- Report IT. India TB Report 2022; Report IT: New Delhi, India, 2022. [Google Scholar]
- Narasimhan, P.; Wood, J.; Macintyre, C.R.; Mathai, D. Risk factors for tuberculosis. Pulm. Med. 2013, 2013, 828939. [Google Scholar] [CrossRef]
- Feleke, B.E.; Feleke, T.E.; Biadglegne, F. Nutritional status of tuberculosis patients, a comparative cross-sectional study. BMC Pulm. Med. 2019, 19, 182. [Google Scholar] [CrossRef]
- Anuradha, R.; Munisankar, S.; Bhootra, Y.; Kumar, N.P.; Dolla, C.; Babu, S. Malnutrition is associated with diminished baseline and mycobacterial antigen—Stimulated chemokine responses in latent tuberculosis infection. J Infect. 2018, 77, 410–416. [Google Scholar] [CrossRef]
- Anuradha, R.; Munisankar, S.; Bhootra, Y.; Kumar, N.P.; Dolla, C.; Kumaran, P.; Babu, S. Coexistent Malnutrition Is Associated with Perturbations in Systemic and Antigen-Specific Cytokine Responses in Latent Tuberculosis Infection. Clin. Vaccine Immunol. 2016, 23, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Azhar, G.S. DOTS for TB relapse in India: A systematic review. Lung India 2012, 29, 147–153. [Google Scholar] [CrossRef] [PubMed]
- do Socorro Nantua Evangelista, M.; Maia, R.; Toledo, J.P.; Abreu, R.G.d.; Braga, J.U.; Barreira, D.; Trajman, A. Second month sputum smear as a predictor of tuberculosis treatment outcomes in Brazil. BMC Res. Notes 2018, 11, 414. [Google Scholar] [CrossRef]
- Nagu, T.J.; Mboka, M.A.; Nkrumbih, Z.F.; Shayo, G.; Mizinduko, M.M.; Komba, E.V.; Maeurer, M.; Zumla, A.; Mugusi, F. Clinical and Imaging Features of Adults with Recurrent Pulmonary Tuberculosis—A Prospective Case-Controlled Study. Int. J. Infect. Dis. 2021, 113 (Suppl. S1), S33–S39. [Google Scholar] [CrossRef] [PubMed]
- Parida, M.; Sannarangaiah, S.; Dash, P.K.; Rao, P.V.; Morita, K. Loop mediated isothermal amplification (LAMP): A new generation of innovative gene amplification technique; perspectives in clinical diagnosis of infectious diseases. Rev. Med. Virol. 2008, 18, 407–421. [Google Scholar] [CrossRef] [PubMed]
- Abdullahi, U.F.; Naim, R.; Wan Taib, W.R.; Saleh, A.; Muazu, A.; Aliyu, S.; Baig, A.A. Loop-mediated isothermal amplification (LAMP), an innovation in gene amplification: Bridging the gap in molecular diagnostics; a review. Indian J. Sci. Technol. 2015, 8, 17. [Google Scholar] [CrossRef]
- Batool, Y.; Pervaiz, G.; Arooj, A.; Fatima, S. Hematological manifestations in patients newly diagnosed with pulmonary tuberculosis. Pak. J. Med. Sci. 2022, 38, 1968–1972. [Google Scholar] [CrossRef] [PubMed]
- Kornfeld, H.; West, K.; Kane, K.; Kumpatla, S.; Zacharias, R.R.; Martinez-Balzano, C.; Li, W.; Viswanathan, V. High Prevalence and Heterogeneity of Diabetes in Patients with TB in South India: A Report from the Effects of Diabetes on Tuberculosis Severity (EDOTS) Study. Chest 2016, 149, 1501–1508. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.P.; Moideen, K.; Nancy, A.; Viswanathan, V.; Thiruvengadam, K.; Nair, D.; Banurekha, V.V.; Sivakumar, S.; Hissar, S.; Kornfeld, H.; et al. Plasma Chemokines Are Baseline Predictors of Unfavorable Treatment Outcomes in Pulmonary Tuberculosis. Clin. Infect. Dis. 2021, 73, e3419–e3427. [Google Scholar] [CrossRef]
- Koo, H.K.; Min, J.; Kim, H.W.; Lee, J.; Kim, J.S.; Park, J.S.; Lee, S.S. Prediction of treatment failure and compliance in patients with tuberculosis. BMC Infect. Dis. 2020, 20, 622. [Google Scholar] [CrossRef] [PubMed]
- Rahimi, B.A.; Rahimy, N.; Mukaka, M.; Ahmadi, Q.; Hayat, M.S.; Wasiq, A.W. Determinants of treatment failure among tuberculosis patients in Kandahar City, Afghanistan: A 5-year retrospective cohort study. Int. J. Mycobacteriol. 2019, 8, 359–365. [Google Scholar] [CrossRef]
- Rohini, K.; Surekha Bhat, M.; Srikumar, P.S.; Mahesh Kumar, A. Assessment of Hematological Parameters in Pulmonary Tuberculosis Patients. Indian J. Clin. Biochem. 2016, 31, 332–335. [Google Scholar] [CrossRef]
- Abay, F.; Yalew, A.; Shibabaw, A.; Enawgaw, B. Hematological Abnormalities of Pulmonary Tuberculosis Patients with and without HIV at the University of Gondar Hospital, Northwest Ethiopia: A Comparative Cross-Sectional Study. Tuberc. Res. Treat. 2018, 2018, 5740951. [Google Scholar] [CrossRef] [PubMed]
- Mendonca, E.B.; Stanis, C.A.S.; Schmaltz, S.; Sant’Anna, F.M.; Vizzoni, A.G.; Mendes-de-Almeida, D.P.; Carvalhaes de Oliveira, R.d.V.; Rolla, V.C. Anemia in tuberculosis cases: A biomarker of severity? PLoS ONE 2021, 16, e0245458. [Google Scholar] [CrossRef]
- Petruccioli, E.; Scriba, T.J.; Petrone, L.; Hatherill, M.; Cirillo, D.M.; Joosten, S.A.; Ottenhoff, T.H.; Denkinger, C.M.; Goletti, D. Correlates of tuberculosis risk: Predictive biomarkers for progression to active tuberculosis. Eur. Respir. J. 2016, 48, 1751–1763. [Google Scholar] [CrossRef] [PubMed]
- Sahin, F.; Yazar, E.; Yildiz, P. Prominent features of platelet count, plateletcrit, mean platelet volume and platelet distribution width in pulmonary tuberculosis. Multidiscip. Respir. Med. 2012, 7, 38. [Google Scholar] [CrossRef]
- Xu, F.; Qu, S.; Wang, L.; Qin, Y. Mean platelet volume (MPV): New diagnostic indices for co-morbidity of tuberculosis and diabetes mellitus. BMC Infect. Dis. 2021, 21, 461. [Google Scholar] [CrossRef] [PubMed]
- Kurup, R.; Flemming, K.; Daniram, S.; Marks-James, S.; Roberts Martin, R. Hematological and Biochemistry Profile and Risk Factors Associated with Pulmonary Tuberculosis Patients in Guyana. Tuberc. Res. Treat. 2016, 2016, 6983747. [Google Scholar] [CrossRef]
- Mabrouk, M.E.; Exany Samuel, A.A.; Badri Mohamed, A.M. Hematological Parameters Among Tuberculosis Patient Under Treatment; LAP LAMBERT Academic Publishing: Saarbrücken, Germany, 2017. [Google Scholar]
- Atomsa, D.; Abebe, G.; Sewunet, T. Immunological markers and hematological parameters among newly diagnosed tuberculosis patients at Jimma University Specialized Hospital. Ethiop. J. Health Sci. 2014, 24, 311–318. [Google Scholar] [CrossRef]
- Akpan, P.; AkpotuzorJosephine, O.; Akwiwu, E.C. Some Haematological Parameters of Tuberculosis (TB). J. Nat. Sci. Res. 2012, 2, 51. [Google Scholar]
- Kahase, D.; Solomon, A.; Alemayehu, M. Evaluation of Peripheral Blood Parameters of Pulmonary Tuberculosis Patients at St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia: Comparative Study. J. Blood Med. 2020, 11, 115–121. [Google Scholar] [CrossRef]
- Wang, W.; Wang, L.F.; Liu, Y.Y.; Yang, F.; Zhu, L.; Zhang, X.H. Value of the Ratio of Monocytes to Lymphocytes for Monitoring Tuberculosis Therapy. Can. J. Infect. Dis. Med. Microbiol. 2019, 2019, 3270393. [Google Scholar] [CrossRef]
- Stefanescu, S.; Cocoş, R.; Turcu-Stiolica, A.; Mahler, B.; Meca, A.-D.; Giura, A.M.C.; Bogdan, M.; Shelby, E.-S.; Zamfirescu, G.; Pisoschi, C.-G. Evaluation of prognostic significance of hematological profiles after the intensive phase treatment in pulmonary tuberculosis patients from Romania. PLoS ONE 2021, 16, e0249301. [Google Scholar] [CrossRef]
- Manjunath, M.R.S. Abdul Rub Patwegar: Comparative study of hematological parameters in newly diagnosed tuberculosis patient’s pre-att & after intensive phase of ATT. IP Arch. Cytol. Histopathol. Res. 2018, 3, 185–191. [Google Scholar] [CrossRef]
- Dada, M.O.; Umeh, O.E.; Ifeanyichukwu, O.M.; Okudo, U.; Ezema, N. Assessment of Some Haematological Parameters among Pre-Treatment, 2 Months, 4 Months and 6 Months Treatment in Pulmonary Tuberculosis Infected Individuals in Anambra State University Teaching Hospital, Awka. Anambra State, Nigeria. Texila Int. J. Clin. Res. 2017, 3, 20. [Google Scholar] [CrossRef]
- Gopalan, N.; Srinivasalu, V.A.; Chinnayan, P.; Velayutham, B.; Bhaskar, A.; Santhanakrishnan, R.; Senguttuvan, T.; Rathinam, S.; Ayyamperumal, M.; Satagopan, K.; et al. Predictors of unfavorable responses to therapy in rifampicin-sensitive pulmonary tuberculosis using an integrated approach of radiological presentation and sputum mycobacterial burden. PLoS ONE 2021, 16, e0257647. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Cases (n = 133) | Controls (n = 68) | p-Value |
|---|---|---|---|
| Age in years | 45 (36–50) | 45 (38–52) | 0.268 |
| Gender | |||
| Female | 23 (17.3) | 8 (11.8) | 0.305 |
| Male | 110 (82.7) | 60 (88.2) | |
| BMI | 18 (1620) | 17 (15–19) | 0.149 |
| Diabetes Status | |||
| Non-Diabetes | 59 (44.4) | 26 (38.2) | 0.406 |
| Diabetes | 74 (55.6) | 42 (61.8) | |
| Cough | |||
| Absence | 2 (1.5) | 1 (1.5) | 0.985 |
| Presence | 131 (98.5) | 67 (98.5) | |
| Dyslipidaemia | |||
| Absence | 133 (100) | 68 (100) | NA |
| Presence | 0 (0) | 0 (0) | |
| Smoking | |||
| Never | 74 (55.6) | 26 (38.2) | 0.034 |
| Past | 26 (19.5) | 14 (20.6) | |
| Current | 33 (24.8) | 28 (41.2) | |
| Alcohol | |||
| Never | 42 (31.6) | 16 (23.5) | 0.466 |
| Past | 25 (18.8) | 13 (19.1) | |
| Current | 66 (49.6) | 39 (57.4) | |
| Cavity | |||
| Absence | 78 (58.6) | 40 (58.8) | >0.990 |
| Presence | 36 (27.1) | 18 (26.5) | |
| Not Known | 19 (14.3) | 10 (14.7) | |
| Smear a | |||
| 1+ | 90 (67.7) | 36 (52.9) | 0.057 |
| 2+ | 40 (30.1) | 27 (39.7) | |
| 3+ | 3 (2.3) | 5 (7.4) | |
| Culture b | |||
| 1+ | 61 (45.9) | 25 (36.8) | 0.158 |
| 2+ | 26 (19.5) | 10 (14.7) | |
| 3+ | 46 (34.6) | 33 (48.5) | |
| Chest X-ray Score median (IQR) | 38 (5–130) | 37 (2–125) | 0.1943 |
| Marker | Univariable Model | Multivariable Model | ||
|---|---|---|---|---|
| OR (95% CL) | p-Value | aOR * (95% CL) | p-Value | |
| Hemoglobin (g/dl) | 0.91 (0.34–2.41) | 0.85 | 0.91 (0.31–2.63) | 0.859 |
| RBC (mill/cm) | 0.14 (0.03–0.55) | 0.005 | 0.15 (0.04–0.65) | 0.011 |
| Haematocrit | 0.13 (0.03–0.55) | 0.006 | 0.14 (0.03–0.65) | 0.012 |
| Platelets (ul) | 0.84 (0.47–1.49) | 0.541 | 0.85 (0.46–1.56) | 0.593 |
| WBC absolute count | 3.51 (1.62–7.59) | 0.001 | 3.14 (1.39–7.08) | 0.006 |
| Neutrophil absolute count | 2.19 (1.20–3.98) | 0.011 | 1.91 (1.01–3.62) | 0.046 |
| Lymphocyte absolute count | 0.44 (0.27–0.74) | 0.002 | 0.45 (0.26–0.77) | 0.003 |
| Monocyte absolute count | 1.68 (1.14–2.47) | 0.008 | 1.63 (1.08–2.46) | 0.019 |
| NL Ratio | 2.68 (1.68–4.26) | <0.001 | 2.52 (1.55–4.09) | <0.001 |
| ML Ratio | 2.32 (1.59–3.39) | <0.001 | 2.30 (1.54–3.45) | <0.001 |
| Chest X-Ray Score | p-Value | R Value | Correlation |
|---|---|---|---|
| HEMOGLOBIN (g/dl) | 0.654 | −0.083 | Very Weak |
| HEMATOCRIT (%) | 0.741 | −0.073 | Very Weak |
| PLATELETS (µL) | 0.064 | 0.259 | Weak |
| RBC | 0.239 | −0.103 | Weak |
| WBC Absolute Count | 0.29 | −0.151 | Weak |
| NEUTROPHIL Absolute Count | 0.616 | −0.01 | Very Weak |
| LYMPHOCYTE Absolute Count | 0.285 | −0.091 | Weak |
| MONOCYTES Absolute Count | 0.039 * | −0.269 | Weak |
| NL Ratio | 0.336 | 0.089 | Very Weak |
| ML Ratio | 0.061 | 0.2 | Weak |
| Chest X-Ray Score | p-Value | R Value | Correlation |
|---|---|---|---|
| HEMOGLOBIN (g/dl) | 0.144 | −0.09 | Very Weak |
| HEMATOCRIT (%) | 0.088 | −0.101 | Very Weak |
| PLATELETS (µL) | 0.067 | 0.146 | Very Weak |
| RBC | 0.058 | −0.106 | Very Weak |
| WBC Absolute Count | 0.421 | 0.074 | Very Weak |
| NEUTROPHIL Absolute Count | 0.072 | 0.123 | Very Weak |
| LYMPHOCYTE Absolute Count | 0.389 | −0.104 | Very Weak |
| MONOCYTES Absolute Count | 0.978 | 0.045 | Very Weak |
| NL Ratio | 0.055 | 0.183 | Very Weak |
| ML Ratio | 0.002 ** | 0.236 | Weak |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nancy Pandiarajan, A.; Kumar, N.P.; Moideen, K.; Thiruvengadam, K.; Hissar, S.; Sivakumar, S.; Bethunaickan, R.; Viswanathan, V.; Kornfeld, H.; Babu, S. Association of Altered Baseline Hematological Parameters with Adverse Tuberculosis Treatment Outcomes. Pathogens 2025, 14, 146. https://doi.org/10.3390/pathogens14020146
Nancy Pandiarajan A, Kumar NP, Moideen K, Thiruvengadam K, Hissar S, Sivakumar S, Bethunaickan R, Viswanathan V, Kornfeld H, Babu S. Association of Altered Baseline Hematological Parameters with Adverse Tuberculosis Treatment Outcomes. Pathogens. 2025; 14(2):146. https://doi.org/10.3390/pathogens14020146
Chicago/Turabian StyleNancy Pandiarajan, Arul, Nathella Pavan Kumar, Kadar Moideen, Kannan Thiruvengadam, Syed Hissar, Shanmugam Sivakumar, Ramalingam Bethunaickan, Vijay Viswanathan, Hardy Kornfeld, and Subash Babu. 2025. "Association of Altered Baseline Hematological Parameters with Adverse Tuberculosis Treatment Outcomes" Pathogens 14, no. 2: 146. https://doi.org/10.3390/pathogens14020146
APA StyleNancy Pandiarajan, A., Kumar, N. P., Moideen, K., Thiruvengadam, K., Hissar, S., Sivakumar, S., Bethunaickan, R., Viswanathan, V., Kornfeld, H., & Babu, S. (2025). Association of Altered Baseline Hematological Parameters with Adverse Tuberculosis Treatment Outcomes. Pathogens, 14(2), 146. https://doi.org/10.3390/pathogens14020146