
Review of Poliovirus Transmission and Economic Modeling to Support Global Polio Eradication: 2020–2024



Abstract
1. Introduction
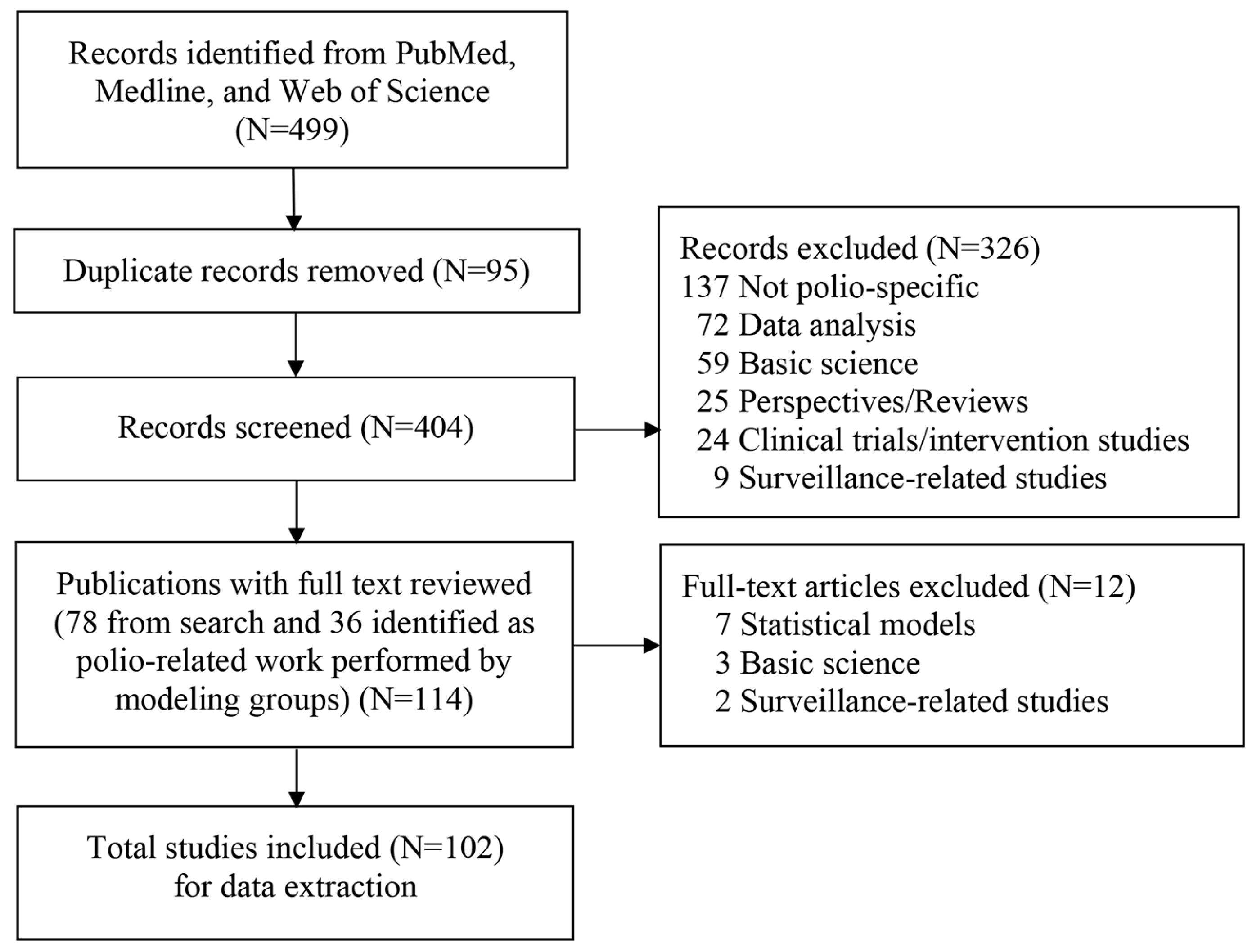
2. Materials and Methods
3. Results
3.1. Studies That Met Inclusion Criteria Published 2020–2024.25
3.1.1. KRI
3.1.2. IC
3.1.3. LSHTM
3.1.4. IDM/BMGF
3.1.5. GIT
3.1.6. Economic Analyses Published by Other Groups
3.1.7. Poliovirus Transmission Modeling Studies Published by Other Groups
3.2. Trends in Characteristics of Polio Modeling Studies
3.3. Modeling in GPEI Annual Reports or SAGE Conclusions and Recommendations
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Thompson, K.M.; Kalkowska, D.A. Review of poliovirus modeling performed from 2000 to 2019 to support global polio eradication. Expert Rev. Vaccines 2020, 19, 661–686. [Google Scholar] [CrossRef]
- Badizadegan, K.; Goodson, J.L.; Rota, P.A.; Thompson, K.M. The potential role of using vaccine patches to induce immunity: Platform and pathways to innovation and commercialization. Expert Rev. Vaccines 2020, 19, 175–194. [Google Scholar] [CrossRef]
- Thompson, K.M.; Orenstein, W.A.; Hinman, A.R. Performance of the United States Vaccine Injury Compensation Program (VICP): 1988–2019. Vaccine 2020, 38, 2136–2143. [Google Scholar] [CrossRef]
- Thompson, K.M.; Orenstein, W.A.; Hinman, A.R. An opportunity to incentivize innovation to increase vaccine safety in the United States by improving vaccine delivery using vaccine patches. Vaccine 2020, 38, 4060–4065. [Google Scholar] [CrossRef]
- Ochalek, J.; Claxton, K.; Lomas, J.; Thompson, K.M. Valuing health outcomes: Developing better defaults based on health opportunity costs. Expert Rev. Pharmacoecon. Outcomes Res. 2021, 21, 729–736. [Google Scholar] [CrossRef]
- Thompson, K.M. Modeling and managing poliovirus risks: We are where we are. Risk Anal. 2021, 41, 223–228. [Google Scholar] [CrossRef]
- Kalkowska, D.A.; Pallansch, M.A.; Wassilak, S.G.F.; Cochi, S.L.; Thompson, K.M. Global transmission of live polioviruses: Updated dynamic modeling of the polio endgame. Risk Anal. 2021, 41, 248–265. [Google Scholar] [CrossRef]
- Thompson, K.M.; Kalkowska, D.A. Reflections on modeling poliovirus transmission and the polio eradication endgame. Risk Anal. 2021, 41, 229–247. [Google Scholar] [CrossRef]
- Kalkowska, D.A.; Thompson, K.M. Insights from modeling preventive supplemental immunization activities as a strategy to eliminate wild poliovirus transmission in Pakistan and Afghanistan. Risk Anal. 2021, 41, 266–272. [Google Scholar] [CrossRef]
- Kalkowska, D.A.; Franka, R.; Higgins, J.; Kovacs, S.D.; Forbi, J.C.; Wassilak, S.G.F.; Pallansch, M.A.; Thompson, K.M. Modeling poliovirus transmission in Borno and Yobe, Northeast Nigeria. Risk Anal. 2021, 41, 289–302. [Google Scholar] [CrossRef]
- Kalkowska, D.A.; Thompson, K.M. Modeling undetected live poliovirus circulation after apparent interruption of transmission: Borno and Yobe in Northeast Nigeria. Risk Anal. 2021, 41, 303–311. [Google Scholar] [CrossRef]
- Kalkowska, D.A.; Pallansch, M.A.; Cochi, S.L.; Kovacs, S.D.; Wassilak, S.G.F.; Thompson, K.M. Updated characterization of post-OPV cessation risks: Lessons from 2019 serotype 2 outbreaks and implications for the probability of OPV restart. Risk Anal. 2021, 41, 320–328. [Google Scholar] [CrossRef]
- Thompson, K.M.; Kalkowska, D.A. Potential future use, costs, and value of poliovirus vaccines. Risk Anal. 2021, 41, 349–363. [Google Scholar] [CrossRef]
- Kalkowska, D.A.; Thompson, K.M. Expected implications of globally coordinated cessation of serotype 3 oral poliovirus vaccine (OPV) before serotype 1 OPV. Risk Anal. 2021, 41, 312–319. [Google Scholar] [CrossRef]
- Kalkowska, D.A.; Pallansch, M.A.; Wilkinson, A.; Bandyopadhyay, A.S.; Konopka-Anstadt, J.L.; Burns, C.C.; Oberste, M.S.; Wassilak, S.G.F.; Badizadegan, K.; Thompson, K.M. Updated characterization of outbreak response strategies for 2019–2029: Impacts of using a novel type 2 oral poliovirus vaccine strain. Risk Anal. 2021, 41, 329–348. [Google Scholar] [CrossRef]
- Thompson, K.M. Poliovirus vaccine options: Another step forward. Lancet 2020, 397, 2–3. [Google Scholar] [CrossRef]
- Thompson, K.M.; Kalkowska, D.A. An updated economic analysis of the Global Polio Eradication Initiative. Risk Anal. 2021, 41, 393–406. [Google Scholar] [CrossRef]
- Kalkowska, D.A.; Thompson, K.M. Health and economic outcomes associated with polio vaccine policy options: 2019–2029. Risk Anal. 2021, 41, 364–375. [Google Scholar] [CrossRef]
- Thompson, K.M.; Kalkowska, D.A.; Badizadegan, K. A health economic analysis for oral poliovirus vaccine to prevent COVID-19 in the United States. Risk Anal. 2021, 41, 376–386. [Google Scholar] [CrossRef]
- Kalkowska, D.A.; Voorman, A.; Pallansch, M.A.; Wassilak, S.G.F.; Cochi, S.L.; Badizadegan, K.; Thompson, K.M. The impact of disruptions caused by the COVID-19 pandemic on global polio eradication. Vaccine 2021, 41, A12–A18. [Google Scholar] [CrossRef]
- Thompson, K.M.; Kalkowska, D.A.; Badizadegan, K. Hypothetical emergence of poliovirus in 2020: Part 1. consequences of policy decisions to respond using nonpharmaceutical interventions. Expert Rev. Vaccines 2021, 20, 465–481. [Google Scholar] [CrossRef]
- Thompson, K.M.; Kalkowska, D.A.; Badizadegan, K. Hypothetical emergence of poliovirus in 2020: Part 2. exploration of the potential role of vaccines in control and eradication. Expert Rev. Vaccines 2021, 20, 449–460. [Google Scholar] [CrossRef]
- Kalkowska, D.A.; Pallansch, M.A.; Cochi, S.L.; Thompson, K.M. Updated Characterization of Poliovirus Transmission in Pakistan and Afghanistan and the Impacts of Different Outbreak Response Vaccine Options. J. Infect. Dis. 2021, 224, 1529–1538. [Google Scholar] [CrossRef]
- Kalkowska, D.A.; Pallansch, M.A.; Cochi, S.L.; Thompson, K.M. Modeling Poliovirus Surveillance and Immunization Campaign Quality Monitoring Costs for Pakistan and Afghanistan for 2019–2023. Open Forum Infect. Dis. 2021, 8, ofab264. [Google Scholar] [CrossRef]
- Kalkowska, D.A.; Pallansch, M.A.; Wassilak, S.G.F.; Cochi, S.L.; Thompson, K.M. Serotype 2 oral poliovirus vaccine (OPV2) choices and the consequences of delaying outbreak response. Vaccine 2023, 41 (Suppl. 1), A136–A141. [Google Scholar] [CrossRef]
- Thompson, K.M. Polio eradication: What kind of world do we want? Lancet Infect. Dis. 2022, 22, 161–163. [Google Scholar] [CrossRef]
- Thompson, K.M. Effectiveness of a new vaccine for outbreak response and the increasingly complicated polio endgame. Lancet Glob. Health 2022, 10, e1697–e1698. [Google Scholar] [CrossRef]
- Thompson, K.M.; Badizadegan, K. Health economic analyses of secondary vaccine effects: A systematic review and policy insights. Expert Rev. Vaccines 2022, 21, 297–312. [Google Scholar] [CrossRef]
- Thompson, K.M.; Kalkowska, D.A.; Badizadegan, K. Polio health economics: Assessing the benefits and costs of polio, non-polio, and integrated activities of the Global Polio Eradication Initiative. Gates Open Res. 2022, 6, 5. [Google Scholar] [CrossRef]
- Badizadegan, K.; Kalkowska, D.A.; Thompson, K.M. Polio by the numbers—A global perspective. J. Infect. Dis. 2022, 226, 1309–1318. [Google Scholar] [CrossRef]
- Thompson, K.M.; Kalkowska, D.A.; Badizadegan, K. Health economic analysis of vaccine options for the polio eradication endgame: 2022-2036. Expert Rev. Vaccines 2022, 21, 1667–1674. [Google Scholar] [CrossRef] [PubMed]
- Kalkowska, D.A.; Badizadegan, K.; Thompson, K.M. Modeling scenarios for ending poliovirus transmission in Pakistan and Afghanistan. Risk Anal. 2023, 43, 660–676. [Google Scholar] [CrossRef] [PubMed]
- Kalkowska, D.A.; Badizadegan, K.; Thompson, K.M. Modeling undetected live type 1 wild poliovirus circulation after apparent interruption of transmission: Pakistan and Afghanistan. Risk Anal. 2023, 43, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Kalkowska, D.A.; Wassilak, S.G.F.; Pallansch, M.A.; Burns, C.C.; Wiesen, E.; Durry, E.; Badizadegan, K.; Thompson, K.M. Outbreak response strategies with type 2-containing oral poliovirus vaccines. Vaccine 2023, 41 (Suppl. 1), A142–A152. [Google Scholar] [CrossRef] [PubMed]
- Kalkowska, D.A.; Badizadegan, K.; Thompson, K.M. Outbreak management strategies for cocirculation of multiple poliovirus types. Vaccine 2023, 41, 3718–3727. [Google Scholar] [CrossRef] [PubMed]
- Thompson, K.M.; Kalkowska, D.A.; Badizadegan, K. Looking back at prospective modeling of outbreak response strategies for managing global type 2 oral poliovirus vaccine (OPV2) cessation. Front. Public Health 2023, 11, 1098419. [Google Scholar] [CrossRef] [PubMed]
- Kalkowska, D.; Wassilak, S.; Wiesen, E.; F Estivariz, C.; Burns, C.; Badizadegan, K.; Thompson, K. Complexity of options related to restarting oral poliovirus vaccine (OPV) in national immunization programs after OPV cessation. Gates Open Res. 2023, 7, 55. [Google Scholar] [CrossRef] [PubMed]
- Thompson, K.M.; Lauring, A.S.; Pollard, A.J.; Andino, R.; Bandyopadhyay, A.S.; Berkley, S.; Bhutta, Z.A.; Routh, J.; Benn, C.S. Polio eradication: Addressing the hurdles on the last mile. Cell 2023, 186, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Thompson, K.M. Polio endgame complexity: Updating expectations for nOPV2. Lancet Infect. Dis. 2023, 23, 992–994. [Google Scholar] [CrossRef] [PubMed]
- Thompson, K.M.; Kalkowska, D.A.; Badizadegan, K. Oral polio vaccine stockpile modeling: Insights from recent experience. Expert Rev. Vaccines 2023, 22, 813–825. [Google Scholar] [CrossRef]
- Kalkowska, D.A.; Wassilak, S.G.F.; Wiesen, E.; Burns, C.C.; Pallansch, M.A.; Badizadegan, K.; Thompson, K.M. Coordinated global cessation of oral poliovirus vaccine use: Options and potential consequences. Risk Anal. 2023, 44, 366–378. [Google Scholar] [CrossRef] [PubMed]
- Kalkowska, D.A.; Wiesen, E.; Wassilak, S.G.F.; Burns, C.C.; Pallansch, M.A.; Badizadegan, K.; Thompson, K.M. Worst-case scenarios: Modeling uncontrolled type 2 polio transmission. Risk Anal. 2023, 44, 379–389. [Google Scholar] [CrossRef] [PubMed]
- Badizadegan, K.; Kalkowska, D.A.; Thompson, K.M. Health economic analysis of antiviral drugs in the global polio eradication endgame. Med. Decis. Mak. 2023, 43, 850–862. [Google Scholar] [CrossRef] [PubMed]
- Thompson, K.M.; Kalkowska, D.A.; Routh, J.A.; Brenner, I.R.; Rosenberg, E.S.; Zucker, J.R.; Langdon-Embry, M.; Sugerman, D.E.; Burns, C.C.; Badizadegan, K. Modeling poliovirus transmission and responses in New York State. J. Infect. Dis. 2024, 229, 1097–1106. [Google Scholar] [CrossRef] [PubMed]
- Kalkowska, D.A.; Badizadegan, K.; Routh, J.A.; Burns, C.C.; Rosenberg, E.S.; Brenner, I.R.; Zucker, J.R.; Langdon-Embry, M.; Thompson, K.M. Modeling undetected poliovirus circulation following the 2022 outbreak in the United States. Expert Rev. Vaccines 2023, 23, 186–195. [Google Scholar] [CrossRef] [PubMed]
- Thompson, K.M.; Kalkowska, D.A.; Kidd, S.E.; Burns, C.C.; Badizadegan, K. Trade-offs of different poliovirus vaccine options for outbreak response in the United States and other countries that only use inactivated poliovirus vaccine (IPV) in routine immunization. Vaccine 2024, 42, 819–827. [Google Scholar] [CrossRef] [PubMed]
- Molodecky, N.A.; Jafari, H.; Safdar, R.M.; Ahmed, J.A.; Mahamud, A.; Bandyopadhyay, A.S.; Shukla, H.; Quddus, A.; Zaffran, M.; Sutter, R.W.; et al. Modelling the spread of serotype-2 vaccine derived-poliovirus outbreak in Pakistan and Afghanistan to inform outbreak control strategies in the context of the COVID-19 pandemic. Vaccine 2023, 41, A93–A104. [Google Scholar] [CrossRef] [PubMed]
- Molodecky, N.A.; Usman, A.; Javaid, A.; Wahdan, A.; Parker, E.P.K.; Ahmed, J.A.; Shah, N.; Agbor, J.; Mahamud, A.; Safdar, R.M. Quantifying movement patterns and vaccination status of high risk mobile populations in Pakistan and Afghanistan to inform poliovirus risk and vaccination strategy. Vaccine 2021, 39, 2124–2132. [Google Scholar] [CrossRef] [PubMed]
- Babji, S.; Manickavasagam, P.; Chen, Y.H.; Jeyavelu, N.; Jose, N.V.; Praharaj, I.; Syed, C.; Kaliappan, S.P.; John, J.; Giri, S.; et al. Immune predictors of oral poliovirus vaccine immunogenicity among infants in South India. NPJ Vaccines 2020, 5, 27. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, D.; Pons-Salort, M.; Shaw, A.G.; Grassly, N.C. The role of genetic sequencing and analysis in the polio eradication programme. Virus Evol. 2020, 6, veaa040. [Google Scholar] [CrossRef] [PubMed]
- Hamisu, A.W.; Blake, I.M.; Sume, G.; Braka, F.; Jimoh, A.; Dahiru, H.; Bonos, M.; Dankoli, R.; Mamuda Bello, A.; Yusuf, K.M.; et al. Characterizing environmental surveillance sites in Nigeria and their sensitivity to detect poliovirus and other enteroviruses. J. Infect. Dis. 2022, 225, 1377–1386. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.V.; Bandyopadhyay, A.; Gumede-Moeletsi, N.; Mach, O.; Mkanda, P.; Ndoutabé, M.; Okiror, S.O.; Ramirez-Gonzalez, A.; Touray, K.; Wanyoike, S.; et al. Risk factors for spread of vaccine-derived type 2 polioviruses in Africa following global withdrawal of trivalent oral poliovirus vaccine and impact of outbreak response with monovalent vaccine: A retrospective analysis of surveillance data. Lancet Infect. Dis. 2022, 22, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Gray, E.J.; Cooper, L.V.; Bandyopadhyay, A.S.; Blake, I.M.; Grassly, N.C. The origins and risk factors for serotype-2 vaccine-derived poliovirus (VDPV2) emergences in Africa during 2016–2019. J. Infect. Dis. 2023, 228, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Grassly, N.C.; Andrews, N.; Cooper, G.; Stephens, L.; Waight, P.; Jones, C.E.; Heath, P.T.; Calvert, A.; Southern, J.; Martin, J.; et al. Effect of maternal immunisation with multivalent vaccines containing inactivated poliovirus vaccine (IPV) on infant IPV immune response: A phase 4, multi-centre randomised trial. Vaccine 2023, 41, 1299–1302. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.V.; Erbeto, T.B.; Danzomo, A.A.; Abdullahi, H.W.; Boateng, K.; Adamu, U.S.; Shuaib, F.; Modjirom, N.; Gray, E.J.; Bandyopadhyay, A.S.; et al. Effectiveness of poliovirus vaccines against circulating vaccine-derived type 2 poliomyelitis in Nigeria between 2017 and 2022: A case-control study. Lancet Infect. Dis. 2024, 24, 427–436. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.V.; Blake, I.M. First Africa-based clinical trial for novel type 2 oral poliovirus vaccine. Lancet 2024, 403, 1113–1115. [Google Scholar] [CrossRef] [PubMed]
- Bandyopadhyay, A.S.; Cooper, L.V.; Zipursky, S. One billion doses and WHO prequalification of nOPV2: Implications for the global polio situation and beyond. PLOS Glob. Public Health 2024, 4, e0002920. [Google Scholar] [CrossRef] [PubMed]
- Kurji, F.D.; Bandyopadhyay, A.S.; Zipursky, S.; Cooper, L.V.; Gast, C.; Toher, M.; Clemens, R.; Clemens, S.A.C.; Prasad, R.; Azhari, A. Novel oral polio vaccine type 2 use for polio outbreak response: A global effort for a global health emergency. Pathogens 2024, 13, 273. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.G.; Majumdar, M.; Troman, C.; O’Toole, A.; Benny, B.; Abraham, D.; Praharaj, I.; Kang, G.; Sharif, S.; Alam, M.M.; et al. Rapid and sensitive direct detection and identification of poliovirus from stool and environmental surveillance samples by use of nanopore sequencing. J. Clin. Microbiol. 2020, 58, 10-1128. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.G.; Cooper, L.V.; Gumede, N.; Bandyopadhyay, A.S.; Grassly, N.C.; Blake, I.M. Time taken to detect and respond to polio outbreaks in Africa and the potential impact of direct molecular detection and nanopore sequencing. J. Infect. Dis. 2022, 226, 453–462. [Google Scholar] [CrossRef]
- Akello, J.O.; Bujaki, E.; Shaw, A.G.; Khurshid, A.; Arshad, Y.; Troman, C.; Majumdar, M.; O’Toole, A.; Rambaut, A.; Alam, M.M.; et al. Comparison of eleven RNA extraction methods for poliovirus direct molecular detection in stool samples. Microbiol. Spectr. 2023, 11, e0425222. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.G.; Mampuela, T.K.; Lofiko, E.L.; Pratt, C.; Troman, C.; Bujaki, E.; O’Toole, A.; Akello, J.O.; Aziza, A.A.; Lusamaki, E.K.; et al. Sensitive poliovirus detection using nested PCR and nanopore sequencing: A prospective validation study. Nat. Microbiol. 2023, 8, 1634–1640. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.G.; Troman, C.; Akello, J.O.; O’Reilly, K.M.; Gauld, J.; Grow, S.; Grassly, N.; Steele, D.; Blazes, D.; Kumar, S.; et al. Defining a research agenda for environmental wastewater surveillance of pathogens. Nat. Med. 2023, 29, 2155–2157. [Google Scholar] [CrossRef] [PubMed]
- Grassly, N.C. Polio’s detection in London is a wake-up call. BMJ 2022, 377, o1589. [Google Scholar] [CrossRef] [PubMed]
- Klapsa, D.; Wilton, T.; Zealand, A.; Bujaki, E.; Saxentoff, E.; Troman, C.; Shaw, A.G.; Tedcastle, A.; Majumdar, M.; Mate, R.; et al. Sustained detection of type 2 poliovirus in London sewage between February and July, 2022, by enhanced environmental surveillance. Lancet 2022, 400, 1531–1538. [Google Scholar] [CrossRef] [PubMed]
- Bandyopadhyay, A.S.; Cavestany, R.L.; Blake, I.M.; Macklin, G.; Cooper, L.V.; Grassly, N.C.; Nery, A.L.; Mach, O. Use of inactivated poliovirus vaccine for poliovirus outbreak response. Lancet Infect. Dis. 2023, 24, e328–e342. [Google Scholar] [CrossRef] [PubMed]
- Vallejo, C.; Pearson, C.A.B.; Koopman, J.S.; Hladish, T.J. Effect of population partitioning on the probability of silent circulation of poliovirus. Bull. Math. Biol. 2022, 84, 62. [Google Scholar] [CrossRef] [PubMed]
- Macklin, G.R.; O’Reilly, K.M.; Grassly, N.C.; Edmunds, W.J.; Mach, O.; Santhana Gopala Krishnan, R.; Voorman, A.; Vertefeuille, J.F.; Abdelwahab, J.; Gumede, N.; et al. Evolving epidemiology of poliovirus serotype 2 following withdrawal of the serotype 2 oral poliovirus vaccine. Science 2020, 368, 401–405. [Google Scholar] [CrossRef]
- O’Reilly, K.M.; Grassly, N.C.; Allen, D.J.; Bannister-Tyrrell, M.; Cameron, A.; Carrion Martin, A.I.; Ramsay, M.; Pebody, R.; Zambon, M. Surveillance optimisation to detect poliovirus in the pre-eradication era: A modelling study of England and Wales. Epidemiol. Infect. 2020, 148, e157. [Google Scholar] [CrossRef]
- Macklin, G.R.; Goel, A.K.; Mach, O.; Tallis, G.; Ahmed, J.A.; O’Reilly, K.M.; Grassly, N.C.; Diop, O.M. Epidemiology of type 2 vaccine-derived poliovirus outbreaks between 2016 and 2020. Vaccine 2023, 41, A19–A24. [Google Scholar] [CrossRef]
- Auzenbergs, M.; Fountain, H.; Macklin, G.; Lyons, H.; O’Reilly, K.M. The impact of surveillance and other factors on detection of emergent and circulating vaccine derived polioviruses. Gates Open Res. 2021, 5, 94. [Google Scholar] [CrossRef] [PubMed]
- Bandyopadhyay, A.S.; Macklin, G.R. Final frontiers of the polio eradication endgame. Curr. Opin. Infect. Dis. 2020, 33, 404–410. [Google Scholar] [CrossRef]
- Macklin, G.R.; Peak, C.; Eisenhawer, M.; Kurji, F.; Mach, O.; Konz, J.; Gast, C.; Bachtiar, N.S.; Bandyopadhyay, A.S.; Zipursky, S.; et al. Enabling accelerated vaccine roll-out for Public Health Emergencies of International Concern (PHEICs): Novel oral polio vaccine type 2 (nOPV2) experience. Vaccine 2023, 41 (Suppl. 1), A122–A127. [Google Scholar] [CrossRef] [PubMed]
- Fine, P.E.M. Population immunity and polio eradication. Pathogens 2024, 13, 183. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, K.M.; Allen, D.J.; Fine, P.; Asghar, H. The challenges of informative wastewater sampling for SARS-CoV-2 must be met: Lessons from polio eradication. Lancet Microbe 2020, 1, e189–e190. [Google Scholar] [CrossRef] [PubMed]
- Bandyopadhyay, A.S.; Gast, C.; Brickley, E.B.; Rüttimann, R.; Clemens, R.; Oberste, M.S.; Weldon, W.C.; Ackerman, M.E.; Connor, R.I.; Wieland-Alter, W.F.; et al. A randomized phase 4 study of immunogenicity and safety after monovalent oral type 2 Sabin poliovirus vaccine challenge in children vaccinated with inactivated poliovirus vaccine in Lithuania. J. Infect. Dis. 2021, 223, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Brickley, E.B.; Connor, R.I.; Wieland-Alter, W.; Weiner, J.A.; Ackerman, M.E.; Arita, M.; Gast, C.; De Coster, I.; Van Damme, P.; Bandyopadhyay, A.S.; et al. Intestinal antibody responses to 2 novel live attenuated type 2 oral poliovirus vaccines in healthy adults in Belgium. J. Infect. Dis. 2022, 226, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Connor, R.I.; Brickley, E.B.; Wieland-Alter, W.F.; Ackerman, M.E.; Weiner, J.A.; Modlin, J.F.; Bandyopadhyay, A.S.; Wright, P.F. Mucosal immunity to poliovirus. Mucosal Immunol. 2022, 15, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Famulare, M.; Wong, W.; Haque, R.; Platts-Mills, J.A.; Saha, P.; Aziz, A.B.; Ahmed, T.; Islam, M.O.; Uddin, M.J.; Bandyopadhyay, A.S.; et al. Multiscale model for forecasting Sabin 2 vaccine virus household and community transmission. PLoS Comput. Biol. 2021, 17, e1009690. [Google Scholar] [CrossRef] [PubMed]
- Wong, W.; Gauld, J.; Famulare, M. From vaccine to pathogen: Modeling Sabin 2 vaccine virus reversion and evolutionary epidemiology in Matlab, Bangladesh. Virus Evol. 2023, 9, vead044. [Google Scholar] [CrossRef]
- Brouwer, A.F.; Eisenberg, M.C.; Shulman, L.M.; Famulare, M.; Koopman, J.S.; Kroiss, S.J.; Hindiyeh, M.; Manor, Y.; Grotto, I.; Eisenberg, J.N.S. The role of time-varying viral shedding in modelling environmental surveillance for public health: Revisiting the 2013 poliovirus outbreak in Israel. J. R. Soc. Interface 2022, 19, 20220006. [Google Scholar] [CrossRef] [PubMed]
- Valesano, A.L.; Taniuchi, M.; Fitzsimmons, W.J.; Islam, M.O.; Ahmed, T.; Zaman, K.; Haque, R.; Wong, W.; Famulare, M.; Lauring, A.S. The early evolution of oral poliovirus vaccine Is shaped by strong positive selection and tight transmission bottlenecks. Cell Host Microbe 2021, 29, 32–43.e34. [Google Scholar] [CrossRef] [PubMed]
- Scott, R.P.; Cullen, A.C.; Chabot-Couture, G. Disease surveillance investments and administration: Limits to information value in Pakistan polio eradication. Risk Anal. 2021, 41, 273–288. [Google Scholar] [CrossRef] [PubMed]
- Voorman, A.; O’Reilly, K.; Lyons, H.; Goel, A.K.; Touray, K.; Okiror, S. Real-time prediction model of cVDPV2 outbreaks to aid outbreak response vaccination strategies. Vaccine 2023, 41, A105–A112. [Google Scholar] [CrossRef] [PubMed]
- Voorman, A.; Lyons, H.; Bennette, C.; Kovacs, S.; Makam, J.K.; F Vertefeuille, J.; Tallis, G. Analysis of population immunity to poliovirus following cessation of trivalent oral polio vaccine. Vaccine 2023, 41, A85–A92. [Google Scholar] [CrossRef] [PubMed]
- Voorman, A.; Lyons, H.; Shuaib, F.; Adamu, U.S.; Korir, C.; Erbeto, T.; Bandyopadhyay, A.S.; Okiror, S. Impact of supplementary immunization activities using novel oral polio vaccine type 2 during a large outbreak of circulating vaccine-derived poliovirus in Nigeria. J. Infect. Dis. 2024, 229, 805–812. [Google Scholar] [CrossRef]
- Sun, Y.; Keskinocak, P.; Steimle, L.N.; Kovacs, S.D.; Wassilak, S.G. A compartmental simulation model to improve interventions for controlling poliovirus outbreaks. In Proceedings of the 2023 Winter Simulation Conference (WSC), San Antonio, TX, USA, 10–13 December 2023; pp. 1184–1195. [Google Scholar]
- Sun, Y.; Keskinocak, P.; Steimle, L.N.; Kovacs, S.D.; Wassilak, S.G. Modeling the spread of circulating vaccine-derived poliovirus type 2 outbreaks and interventions: A case study of Nigeria. Vaccine X 2024, 18, 100476. [Google Scholar] [CrossRef] [PubMed]
- Cheng, E.; Gambhirrao, N.; Patel, R.; Zhowandai, A.; Rychtář, J.; Taylor, D. A game-theoretical analysis of poliomyelitis vaccination. J. Theor. Biol. 2020, 499, 110298. [Google Scholar] [CrossRef] [PubMed]
- Wells, C.R.; Huppert, A.; Fitzpatrick, M.C.; Pandey, A.; Velan, B.; Singer, B.H.; Bauch, C.T.; Galvani, A.P. Prosocial polio vaccination in Israel. Proc. Natl. Acad. Sci. USA 2020, 117, 13138–13144. [Google Scholar] [CrossRef] [PubMed]
- Ren, J.; Maimaiti, H.; Sun, X.; Huang, Z.; Liu, J.; Yang, J.; Li, Z.; Bai, Q.; Lu, Y. Cost-effectiveness of three poliovirus immunization schedules in Shanghai, China. Vaccines 2021, 9, 1062. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Liu, Y.; Wang, J.; Che, X.; Du, J.; Zhang, X.; Gu, W.; Zhang, X.; Jiang, W. Cost-effectiveness of various immunization schedules with inactivated Sabin strain polio vaccine in Hangzhou, China. Front. Public Health 2022, 10, 990042. [Google Scholar] [CrossRef] [PubMed]
- Chang, A.Y.; Aaby, P.; Avidan, M.S.; Benn, C.S.; Bertozzi, S.M.; Blatt, L.; Chumakov, K.; Khader, S.A.; Kottilil, S.; Nekkar, M.; et al. One vaccine to counter many diseases? Modeling the economics of oral polio vaccine against child mortality and COVID-19. Front. Public Health 2022, 10, 967920. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, N.; Macias-Diaz, J.E.; Shahid, N.; Raza, A.; Rafiq, M. A dynamically consistent computational method to solve numerically a mathematical model of polio propagation with spatial diffusion. Comput. Methods Programs Biomed. 2022, 218, 106709. [Google Scholar] [CrossRef] [PubMed]
- Alrawajeh, F.A.; Allehiany, F.M.; Raza, A.; Abdelmohsen, S.A.M.; Cheema, T.N.; Rafiq, M.; Mohsin, M. Bio-inspired computational methods for the polio virus epidemic model. CMC-Comput. Mater. Contin. 2022, 72, 2357–2374. [Google Scholar] [CrossRef]
- Liu, X.; Rahman, M.U.; Arfan, M.; Tchier, F.; Ahmad, S.; Inc, M.; Akinyemi, L. Fractional mathematical modeling to the spread of polio with the role of vaccination under non-singular kernal. Fractals-Complex Geom. Patterns Scaling Nat. Soc. 2022, 30, 17. [Google Scholar] [CrossRef]
- Naveed, M.; Baleanu, D.; Raza, A.; Rafiq, M.; Soori, A.H. Treatment of polio delayed epidemic model via computer simulations. CMC-Comput. Mater. Contin. 2022, 70, 3415–3431. [Google Scholar] [CrossRef]
- Raza, A.; Baleanu, D.; Khan, Z.U.; Mohsin, M.; Ahmed, N.; Rafiq, M.; Anwar, P. Stochastic analysis for the dynamics of a poliovirus epidemic model. CMES-Comput. Model. Eng. Sci. 2022, 136, 257–275. [Google Scholar] [CrossRef]
- Bornaa, C.S.; Seidu, B.; Makinde, O.D. Mathematical analysis of the impact of vaccination and poor sanitation on the dynamics of poliomyelitis. Int. J. Nonlinear Sci. Numer. Simul. 2023, 24, 161–169. [Google Scholar] [CrossRef]
- Iqbal, M.S.; Ahmed, N.; Akgül, A.; Satti, A.M.; Iqbal, Z.; Raza, A.; Rafiq, M.; Anjum, R.; Zakarya, M.; Park, C. Analysis of the fractional polio model with the Mittag-Leffler kernels. Alex. Eng. J. 2023, 64, 957–967. [Google Scholar] [CrossRef]
- Karaagac, B.; Owolabi, K.M. Numerical analysis of polio model: A mathematical approach to epidemiological model using derivative with Mittag-Leffler Kernel. Math. Methods Appl. Sci. 2023, 46, 8175–8192. [Google Scholar] [CrossRef]
- Wang, X.J.; Lin, G. Spreading speeds in two reaction-diffusion models for polio disease. Commun. Nonlinear Sci. Numer. Simul. 2023, 118, 18. [Google Scholar] [CrossRef]
- World Health Assembly. Global Eradication of Poliomyelitis by the Year 2000; World Health Organization: Geneva, Switzerland, 1988. [Google Scholar]
- Thompson, K.M.; Badizadegan, K. Evolution of global polio eradication strategies: Targets, vaccines, and supplemental immunization activities (SIAs). Expert Rev. Vaccines, 2024; In press. [Google Scholar]
- World Health Organization. Vaccines & Biologicals Annual Report 1999; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Fine, P.E.M. Herd immunity: History, theory, practice. Epidemiol. Rev. 1993, 15, 265–302. [Google Scholar] [CrossRef] [PubMed]
- Fine, P.E.; Carneiro, I.A. Transmissibility and persistence of oral polio vaccine viruses: Implications for the global poliomyelitis eradication initiative. Am. J. Epidemiol. 1999, 150, 1001–1021. [Google Scholar] [CrossRef]
- Eichner, M.; Hadeler, K.P. Deterministic models for the eradication of poliomyelitis: Vaccination with the inactivated (IPV) and attenuated (OPV) polio virus vaccine. Math. Biosci. 1995, 127, 149–166. [Google Scholar] [CrossRef] [PubMed]
- Eichner, M.; Hadeler, K.P.; Dietz, K. Stochastic models for the eradication of poliomyelitis: Minimum population size for polio virus persistence. In Models for Infectious Human Diseases: Their Structure and Relation to Data; Isham, V., Medley, G.F., Eds.; Cambridge University Press: New York, NY, USA, 1996; pp. 315–327. [Google Scholar]
- Bart, K.J.; Foulds, J.; Patriarca, P. Global eradication of poliomyelitis: Benefit-cost analysis. Bull. World Health Organ. 1996, 74, 35–45. [Google Scholar] [PubMed]
- O’Reilly, K.M.; Verity, R.; Durry, E.; Asghar, H.; Sharif, S.; Zaidi, S.Z.; Wadood, M.Z.M.; Diop, O.M.; Okayasu, H.; Safdar, R.M.; et al. Population sensitivity of acute flaccid paralysis and environmental surveillance for serotype 1 poliovirus in Pakistan: An observational study. BMC Infect. Dis. 2018, 18, 176. [Google Scholar] [CrossRef] [PubMed]
- Macklin, G.R.; Grassly, N.C.; Sutter, R.W.; Mach, O.; Bandyopadhyay, A.S.; Edmunds, W.J.; O’Reilly, K.M. Vaccine schedules and the effect on humoral and intestinal immunity against poliovirus: A systematic review and network meta-analysis. Lancet Infect. Dis. 2019, 19, 1121–1128. [Google Scholar] [CrossRef] [PubMed]
- Fine, P.E.; Sutter, R.W.; Orenstein, W.A. Stopping a polio outbreak in the post-eradication era. Dev. Biol. 2001, 105, 129–147; discussion 149–150. [Google Scholar]
- Wringe, A.; Fine, P.E.; Sutter, R.W.; Kew, O.M. Estimating the extent of vaccine-derived poliovirus infection. PLoS ONE 2008, 3, e3433. [Google Scholar] [CrossRef] [PubMed]
- Wright, P.F.; Connor, R.I.; Wieland-Alter, W.F.; Hoen, A.G.; Boesch, A.W.; Ackerman, M.E.; Oberste, M.S.; Gast, C.; Brickley, E.B.; Asturias, E.J.; et al. Vaccine-induced mucosal immunity to poliovirus: Analysis of cohorts from an open-label, randomised controlled trial in Latin American infants. Lancet Infect. Dis. 2016, 16, 1377–1384. [Google Scholar] [CrossRef] [PubMed]
- Brickley, E.B.; Strauch, C.B.; Wieland-Alter, W.F.; Connor, R.I.; Lin, S.; Weiner, J.A.; Ackerman, M.E.; Arita, M.; Oberste, M.S.; Weldon, W.C.; et al. Intestinal immune responses to type 2 oral polio vaccine (OPV) challenge in infants previously immunized with bivalent OPV and either high-dose or standard inactivated polio vaccine. J. Infect. Dis. 2018, 217, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Brickley, E.B.; Connor, R.I.; Wieland-Alter, W.F.; Collett, M.S.; Hartford, M.; Van Der Avoort, H.; Boesch, A.W.; Weiner, J.A.; Ackerman, M.E.; McKinlay, M.A.; et al. Intestinal antibody responses to a live oral poliovirus vaccine challenge among adults previously immunized with inactivated polio vaccine in Sweden. BMJ Glob. Health 2019, 4, e001613. [Google Scholar] [CrossRef] [PubMed]
- Brickley, E.B.; Wieland-Alter, W.; Connor, R.I.; Ackerman, M.E.; Boesch, A.W.; Arita, M.; Weldon, W.C.; O’Ryan, M.G.; Bandyopadhyay, A.S.; Wright, P.F. Intestinal immunity to poliovirus following sequential trivalent inactivated polio vaccine/bivalent oral polio vaccine and trivalent inactivated polio vaccine-only immunization schedules: Analysis of an open-label, randomized, controlled trial in Chilean infants. Clin. Infect. Dis. 2018, 67, S42–S50. [Google Scholar] [CrossRef] [PubMed]
- Fine, P.E.M. Gaps in our knowledge about transmission of vaccine-derived polioviruses. Bull. World Health Organ. 2000, 78, 358–359. [Google Scholar] [PubMed]
- Nathanson, N.; Fine, P.E.M. Virology. Poliomyelitis eradication—A dangerous endgame. Science 2002, 296, 269–270. [Google Scholar] [CrossRef] [PubMed]
- Fine, P.E.; Ritchie, S. Perspective: Determinants of the severity of poliovirus outbreaks in the post eradication era. Risk Anal. 2006, 26, 1533–1540. [Google Scholar] [CrossRef] [PubMed]
- Fine, P.E.M.; Oblapenko, G.; Sutter, R.W. Polio control after certification: Major issues outstanding. Bull. World Health Organ. 2004, 82, 47–52. [Google Scholar] [PubMed]
- Fine, P.E. Poliomyelitis: Very small risks and very large risks. Lancet Neurol. 2004, 3, 703. [Google Scholar] [CrossRef] [PubMed]
- Fine, P.E.; Griffiths, U.K. Global poliomyelitis eradication: Status and implications. Lancet 2007, 369, 1321–1322. [Google Scholar] [CrossRef]
- Fine, P.E. Polio: Measuring the protection that matters most. J. Infect. Dis. 2009, 200, 673–675. [Google Scholar] [CrossRef]
- Fine, P. Commentary: An unexpected finding that needs confirmation or rejection. BMJ 2000, 321, 1439. [Google Scholar] [PubMed]
- Brickley, E.B.; Wright, P.F. Maximising the impact of inactivated polio vaccines. Lancet Infect. Dis. 2017, 17, 680–681. [Google Scholar] [CrossRef] [PubMed]
- Voorman, A.; Hoff, N.A.; Doshi, R.H.; Alfonso, V.; Mukadi, P.; Muyembe-Tamfum, J.J.; Wemakoy, E.O.; Bwaka, A.; Weldon, W.; Gerber, S.; et al. Polio immunity and the impact of mass immunization campaigns in the Democratic Republic of the Congo. Vaccine 2017, 35, 5693–5699. [Google Scholar] [CrossRef] [PubMed]
- Alfonso, V.H.; Voorman, A.; Hoff, N.A.; Weldon, W.C.; Gerber, S.; Gadoth, A.; Halbrook, M.; Goldsmith, A.; Mukadi, P.; Doshi, R.H.; et al. Poliovirus immunity among adults in the Democratic Republic of the Congo: A cross-sectional serosurvey. BMC Infect. Dis. 2022, 22, 30. [Google Scholar] [CrossRef] [PubMed]
- Voorman, A.; Habib, M.A.; Hussain, I.; Muhammad Safdar, R.; Ahmed, J.A.; Weldon, W.C.; Ahmed, I.; Umer, M.; Partridge, J.; Soofi, S.B. Immunity and field efficacy of type 2-containing polio vaccines after cessation of trivalent oral polio vaccine: A population-based serological study in Pakistan. Vaccine X 2020, 5, 100067. [Google Scholar] [CrossRef] [PubMed]
- VanderEnde, K.; Voorman, A.; Khan, S.; Anand, A.; Snider, C.J.; Goel, A.; Wassilak, S. New analytic approaches for analyzing and presenting polio surveillance data to supplement standard performance indicators. Vaccine X 2020, 4, 100059. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Strategic Advisory Group of Experts on Immunization Meetings. Available online: https://www.who.int/groups/strategic-advisory-group-of-experts-on-immunization/meetings (accessed on 28 March 2024).
- Global Polio Eradication Initiative. Progress 1999: Every Child Counts. Available online: https://iris.who.int/bitstream/handle/10665/66964/WHO_POLIO_00.03.pdf (accessed on 13 November 2023).
- Global Polio Eradication Initiative. Progress 2000. Available online: https://iris.who.int/bitstream/handle/10665/66763/WHO_POLIO_01.03.pdf (accessed on 13 November 2023).
- Global Polio Eradication Initiative. Progress 2001. Available online: https://iris.who.int/bitstream/handle/10665/67417/WHO_POLIO_02.08.pd (accessed on 13 November 2023).
- Global Polio Eradication Initiative. Progress 2002. Available online: https://iris.who.int/bitstream/handle/10665/67931/WHO_POLIO_03.02.pdf (accessed on 13 November 2023).
- Global Polio Eradication Initiative. Progress 2003. Available online: https://iris.who.int/bitstream/handle/10665/68653/WHO_POLIO_04.02.pdf (accessed on 13 November 2023).
- Global Polio Eradication Initiative. 2004 Annual Report. Available online: https://iris.who.int/bitstream/handle/10665/69055/WHO_POLIO_05.03.pdf (accessed on 13 November 2023).
- Global Polio Eradication Initiative. 2005 Annual Report. Available online: https://iris.who.int/bitstream/handle/10665/70869/WHO_Polio_06.02_eng.pdf (accessed on 13 November 2023).
- Global Polio Eradication Initiative. 2006 Annual Report. Available online: https://iris.who.int/bitstream/handle/10665/70868/WHO_Polio_07.02_eng.pdf (accessed on 13 November 2023).
- Global Polio Eradication Initiative. 2007 Annual Report. Available online: https://iris.who.int/bitstream/handle/10665/70867/WHO_Polio_08.02_eng.pdf (accessed on 13 November 2023).
- Global Polio Eradication Initiative. 2008 Annual Report. Available online: https://iris.who.int/bitstream/handle/10665/70866/WHO_POLIO_09.03_eng.pdf (accessed on 13 November 2023).
- Global Polio Eradication Initiative. 2009 Annual Report. Available online: https://iris.who.int/bitstream/handle/10665/70865/WHO_Polio_10.05_eng.pdf (accessed on 13 November 2023).
- Global Polio Eradication Initiative. 2010 Annual Report: Every Last Child. Available online: https://iris.who.int/bitstream/handle/10665/70849/WHO_POLIO_11.02_eng.pdf (accessed on 13 November 2023).
- Global Polio Eradication Initiative. 2011 Annual Report. Available online: https://iris.who.int/bitstream/handle/10665/276243/WHO-POLIO-12.02-eng.pdf (accessed on 13 November 2023).
- Global Polio Eradication Initiative. 2012 Annual Report. Available online: https://iris.who.int/bitstream/handle/10665/276241/WHO-POLIO-13.03-eng.pdf (accessed on 13 November 2023).
- Global Polio Eradication Initiative. 2013 Annual Report. Available online: https://iris.who.int/bitstream/handle/10665/276239/WHO-POLIO-14.02-eng.pdf (accessed on 13 November 2023).
- Global Polio Eradication Initiative. 2014 Annual Report: On the Threshold of a Polio Free World. Available online: https://iris.who.int/bitstream/handle/10665/276238/WHO-POLIO-15.01-eng.pdf (accessed on 13 November 2023).
- Global Polio Eradication Initiative. 2015 Annual Report: Eradication within Reach. Available online: https://iris.who.int/bitstream/handle/10665/250145/WHO-POLIO-16.01-eng.pdf (accessed on 13 November 2023).
- Global Polio Eradication Initiative. 2016 Annual Report: Eradication within Reach. Available online: https://iris.who.int/bitstream/handle/10665/276236/WHO-POLIO-17.03-eng.pdf (accessed on 13 November 2023).
- Global Polio Eradication Initiative. 2017 Annual Report: Securing a Lasting World Free of All Polioviruses. Available online: https://iris.who.int/bitstream/handle/10665/276237/WHO-POLIO-18.01-eng.pdf (accessed on 13 November 2023).
- Global Polio Eradication Initiative. 2018 Annual Report: To Achieve Lasting Success. Available online: https://polioeradication.org/wp-content/uploads/2016/07/Annual-report-2018.pdf (accessed on 13 November 2023).
- Global Polio Eradication Initiative. 2019 Annual Report and Semi-Annual Status Updates, January–June and July–December 2019. Available online: https://iris.who.int/bitstream/handle/10665/336693/9789240013117-eng.pdf (accessed on 13 November 2023).
- Global Polio Eradication Initiative. 2020 Annual Report and Semi-Annual Status Updates, January–June and July–December 2020. Available online: https://iris.who.int/bitstream/handle/10665/344329/9789240030763-eng.pdf (accessed on 13 November 2023).
- Global Polio Eradication Initiative. 2021 Annual Report. Available online: https://iris.who.int/bitstream/handle/10665/364215/9789240058934-eng.pdf (accessed on 13 November 2023).
- Global Polio Eradication Initiative. 2022 Annual Report. Available online: https://polioeradication.org/wp-content/uploads/2023/06/GPEI_2022_Expenditure_Report.pdf (accessed on 13 November 2023).
- Polio Oversight Board. Meeting of the Polio Oversight Board, Global Polio Eradication Initiative, 12 December 2014. Available online: https://polioeradication.org/wp-content/uploads/2016/07/POB_Minutes_Mtg20141212.pdf (accessed on 10 April 2023).
- Polio Oversight Board. Meeting of the Polio Oversight Board (Call), 13 January 2016. Available online: https://polioeradication.org/wp-content/uploads/2016/07/POB_Minutes_Mtg20160113.pdf (accessed on 10 April 2023).
- Polio Oversight Board. Meeting of the Polio Oversight Board (POB)—Teleconference, 18 December 2020. Available online: https://polioeradication.org/wp-content/uploads/2021/02/POB-minutes-20201218.pdf (accessed on 10 April 2024).
- Kalkowska, D.A.; Pallansch, M.A.; Thompson, K.M. Updated modelling of the prevalence of immunodeficiency-associated long-term vaccine-derived poliovirus (iVDPV) excreters. Epidemiol. Infect. 2019, 147, e295. [Google Scholar] [CrossRef] [PubMed]
- Global Polio Eradication Initiative; World health organization. Polio Endgame Strategy 2019–2023: Eradication, Integration, Certification and Containment; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Global Polio Eradication Initiative. Polio Post-Certification Strategy: A Risk Mitigation Strategy for a Polio-Free World; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Duintjer Tebbens, R.J.; Pallansch, M.A.; Cochi, S.L.; Wassilak, S.G.F.; Thompson, K.M. An economic analysis of poliovirus risk management policy options for 2013–2052. BMC Infect. Dis. 2015, 15, 389. [Google Scholar] [CrossRef] [PubMed]
- Duintjer Tebbens, R.J.; Pallansch, M.A.; Wassilak, S.G.; Cochi, S.L.; Thompson, K.M. Characterization of outbreak response strategies and potential vaccine stockpile needs for the polio endgame. BMC Infect. Dis. 2016, 16, 137. [Google Scholar] [CrossRef] [PubMed]
- Duintjer Tebbens, R.J.; Pallansch, M.A.; Cochi, S.L.; Ehrhardt, D.T.; Farag, N.H.; Hadler, S.C.; Hampton, L.M.; Martinez, M.; Wassilak, S.G.F.; Thompson, K.M. Modeling poliovirus transmission in Pakistan and Afghanistan to inform vaccination strategies in undervaccinated subpopulations. Risk Anal. 2018, 38, 1701–1717. [Google Scholar] [CrossRef]
- Kalkowska, D.A.; Duintjer Tebbens, R.J.; Thompson, K.M. Environmental surveillance system characteristics and impacts on confidence about no undetected serotype 1 wild poliovirus circulation. Risk Anal. 2019, 39, 414–425. [Google Scholar] [CrossRef] [PubMed]
- Kalkowska, D.A.; Duintjer Tebbens, R.J.; Pallansch, M.A.; Thompson, K.M. Modeling undetected live poliovirus circulation after apparent interruption of transmission: Pakistan and Afghanistan. Risk Anal. 2019, 39, 402–413. [Google Scholar] [CrossRef] [PubMed]
- Duintjer Tebbens, R.J.; Thompson, K.M. Evaluation of proactive and reactive strategies for polio eradication activities in Pakistan and Afghanistan. Risk Anal. 2019, 39, 389–401. [Google Scholar] [CrossRef] [PubMed]
- African Regional Commission for the Certification of Poliomyelitis Eradication. Certifying the interruption of wild poliovirus transmission in the WHO African region on the turbulent journey to a polio-free world. Lancet Glob. Health 2020, 8, e1345–e1351. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Report from the Twentieth Meeting of the Global Commission for Certification of Poliomyelitis Eradication, Geneva, Switzerland, 17–18 October 2019. Available online: http://polioeradication.org/wp-content/uploads/2016/07/20th-meeting-of-the-Global-Commission-for-the-Certification-of-Eradication-of-Poliomyelitis-17-18-October-2019.pdf (accessed on 31 December 2019).
- Global Polio Eradication Initiative; World Health Organization. Strategy for the Response to Type 2 Circulating Vaccine-Derived Poliovirus 2020–2021: An Addendum to the Polio Endgame Strategy 2019-2023; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Duintjer Tebbens, R.J.; Pallansch, M.A.; Cochi, S.L.; Wassilak, S.G.; Linkins, J.; Sutter, R.W.; Aylward, R.B.; Thompson, K.M. Economic analysis of the Global Polio Eradication Initiative. Vaccine 2010, 29, 334–343. [Google Scholar] [CrossRef] [PubMed]
- Chumakov, K.; Benn, C.S.; Aaby, P.; Kottilil, S.; Gallo, R. Can existing live vaccines prevent COVID-19? Science 2020, 368, 1187–1188. [Google Scholar] [CrossRef] [PubMed]
- Gallo, R.; Arbess, D.J. An Old Vaccine May Help against Coronavirus: A Tablet for Polio Boosts Innate Immunity, Which Fights Other Viruses. Available online: https://www.wsj.com/articles/an-old-vaccine-may-help-against-coronavirus-11593557168 (accessed on 1 July 2020).
- Thompson, K.M.; Kalkowska, D.A.; Badizadegan, K. No role for reintroducing OPV into the United States with respect to controlling COVID-19 [Response to the letter to the Editor by Chumakov et al.]. Risk Anal. 2021, 41, 389–392. [Google Scholar] [CrossRef] [PubMed]
- Global Polio Eradication Initiative; World Health Organization. Polio Eradication Strategy 2022–2026: Delivering on a Promise; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Thompson, K.M.; Duintjer Tebbens, R.J. Eradication versus control for poliomyelitis: An economic analysis. Lancet 2007, 369, 1363–1371. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Report from the Twenty-Second Meeting of the Global Commission for Certification of Poliomyelitis Eradication, Geneva, Switzerland, 3 June 2022. Available online: https://polioeradication.org/wp-content/uploads/2022/09/22nd-GCC-report-20220907.pdf (accessed on 12 September 2022).
- Kidd, S.; Clark, T.; Routh, J.; Cineas, S.; Bahta, L.; Brooks, O. Use of inactivated polio vaccine among U.S. qdults: Updated recommendations of the Advisory Committee on Immunization Practices—United States, 2023. MMWR Morb. Mortal. Wkly. Rep. 2023, 72, 1327–1330. [Google Scholar] [CrossRef]
- Bunimovich-Mendrazitsky, S.; Stone, L. Modeling polio as a disease of development. J. Theor. Biol. 2005, 237, 302–315. [Google Scholar] [CrossRef]
- Duintjer Tebbens, R.J.; Pallansch, M.A.; Kew, O.M.; Caceres, V.M.; Sutter, R.W.; Thompson, K.M. A dynamic model of poliomyelitis outbreaks: Learning from the past to help inform the future. Am. J. Epidemiol. 2005, 162, 358–372. [Google Scholar] [CrossRef] [PubMed]
- Thompson, K.M.; Duintjer Tebbens, R.J. The case for cooperation in managing and maintaining the end of poliomyelitis: Stockpile needs and coordinated OPV cessation. Medscape J. Med. 2008, 10, 190. [Google Scholar] [PubMed]
- Thompson, K.M.; Tebbens, R.J.; Pallansch, M.A.; Kew, O.M.; Sutter, R.W.; Aylward, R.B.; Watkins, M.; Gary, H.E., Jr.; Alexander, J.; Jafari, H.; et al. The risks, costs, and benefits of possible future global policies for managing polioviruses. Am. J. Public Health 2008, 98, 1322–1330. [Google Scholar] [CrossRef] [PubMed]
- Grassly, N.C.; Fraser, C.; Wenger, J.; Deshpande, J.M.; Sutter, R.W.; Heymann, D.L.; Aylward, R.B. New strategies for the elimination of polio from India. Science 2006, 314, 1150–1153. [Google Scholar] [CrossRef]
- Grassly, N.C.; Wenger, J.; Durrani, S.; Bahl, S.; Deshpande, J.M.; Sutter, R.W.; Heymann, D.L.; Aylward, R.B. Protective efficacy of a monovalent oral type 1 poliovirus vaccine: A case-control study. Lancet 2007, 369, 1356–1362. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, H.E.; Aylward, R.B.; Gasasira, A.; Donnelly, C.A.; Abanida, E.A.; Koleosho-Adelekan, T.; Grassly, N.C. Effectiveness of immunization against paralytic poliomyelitis in Nigeria. N. Engl. J. Med. 2008, 359, 1666–1674. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, H.E.; Aylward, R.B.; Gasasira, A.; Donnelly, C.A.; Mwanza, M.; Corander, J.; Garnier, S.; Chauvin, C.; Abanida, E.; Pate, M.A.; et al. Implications of a circulating vaccine-derived poliovirus in Nigeria. N. Engl. J. Med. 2010, 326, 2360–2369. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.; Hagedorn, B.; Lyons, H. Projection of costs of polio eradication compared to permanent control. J. Infect. Dis. 2020, 221, 561–565. [Google Scholar] [CrossRef] [PubMed]
- Global Polio Eradication Initiative. Investment Case 2022–2026; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- World Health Organization. Status of polio outbreaks in 2005. Polio Erad. Initiat.—Polio News 2005, 25, 2–3. [Google Scholar]
- Thompson, K.M.; Duintjer Tebbens, R.J.; Pallansch, M.A. Evaluation of response scenarios to potential polio outbreaks using mathematical models. Risk Anal. 2006, 26, 1541–1556. [Google Scholar] [CrossRef] [PubMed]
- Thompson, K.M. Poliomyelitis and the role of risk analysis in global infectious disease policy and management. Risk Anal. 2006, 26, 1419–1421. [Google Scholar] [CrossRef] [PubMed]
- Dowdle, W.; van der Avoort, H.; de Gourville, E.; Delpeyroux, F.; Desphande, J.; Hovi, T.; Martin, J.; Pallansch, M.; Kew, O.; Wolff, C. Containment of polioviruses after eradication and OPV cessation: Characterizing risks to improve management. Risk Anal. 2006, 26, 1449–1469. [Google Scholar] [CrossRef]
- Duintjer Tebbens, R.J.; Pallansch, M.A.; Kew, O.M.; Caceres, V.M.; Jafari, H.; Cochi, S.L.; Sutter, R.W.; Aylward, R.B.; Thompson, K.M. Risks of paralytic disease due to wild or vaccine-derived poliovirus after eradication. Risk Anal. 2006, 26, 1471–1505. [Google Scholar] [CrossRef] [PubMed]
- Grassly, N.C.; Jafari, H.; Bahl, S.; Sethi, R.; Deshpande, J.M.; Wolff, C.; Sutter, R.W.; Aylward, R.B. Waning intestinal immunity after vaccination with oral poliovirus vaccines in India. J. Infect. Dis. 2012, 205, 1554–1561. [Google Scholar] [CrossRef] [PubMed]
- Thompson, K.M.; Duintjer Tebbens, R.J. Modeling the dynamics of oral poliovirus vaccine cessation. J. Infect. Dis. 2014, 210 (Suppl. 1), S475–S484. [Google Scholar] [CrossRef] [PubMed]
- Pons-Salort, M.; Molodecky, N.A.; O’Reilly, K.M.; Wadood, M.Z.; Safdar, R.M.; Etsano, A.; Vaz, R.G.; Jafari, H.; Grassly, N.C.; Blake, I.M. Population immunity against serotype-2 poliomyelitis leading up to the global withdrawal of the oral poliovirus vaccine: Spatio-temporal modelling of surveillance data. PLOS Med. 2016, 13, e1002140. [Google Scholar] [CrossRef]
- Grassly, N.C. Immunogenicity and effectiveness of routine immunization with 1 or 2 doses of inactivated poliovirus vaccine: Systematic review and meta-analysis. J. Infect. Dis. 2014, 210 (Suppl. 1), S439–S446. [Google Scholar] [CrossRef] [PubMed]
- Macklin, G.; Liao, Y.; Takane, M.; Dooling, K.; Gilmour, S.; Mach, O.; Kew, O.M.; Sutter, R.W.; iVDPV Working Group. Prolonged excretion of poliovirus among individuals with primary immunodeficiency disorder: An analysis of the World Health Organization registry. Front. Immunol. 2017, 8, 1103. [Google Scholar] [CrossRef] [PubMed]
- Taniuchi, M.; Famulare, M.; Zaman, K.; Uddin, M.J.; Upfill-Brown, A.M.; Ahmed, T.; Saha, P.; Haque, R.; Bandyopadhyay, A.S.; Modlin, J.F.; et al. Community transmission of type 2 poliovirus after cessation of trivalent oral polio vaccine in Bangladesh: An open-label cluster-randomised trial and modelling study. Lancet Infect. Dis. 2017, 17, 1069–1079. [Google Scholar] [CrossRef]
- Parker, E.P.; Molodecky, N.A.; Pons-Salort, M.; O’Reilly, K.M.; Grassly, N.C. Impact of inactivated poliovirus vaccine on mucosal immunity: Implications for the polio eradication endgame. Expert Rev. Vaccines 2015, 14, 1113–1123. [Google Scholar] [CrossRef] [PubMed]
- Mangal, T.D.; Aylward, R.B.; Grassly, N.C. The potential impact of routine immunization with inactivated poliovirus vaccine on wild-type or vaccine-derived poliovirus outbreaks in a posteradication setting. Am. J. Epidemiol. 2013, 178, 1579–1587. [Google Scholar] [CrossRef] [PubMed]
- Shirreff, G.; Wadood, M.Z.; Vaz, R.G.; Sutter, R.W.; Grassly, N.C. Estimated effect of inactivated poliovirus vaccine campaigns, Nigeria and Pakistan, January 2014–April 2016. Emerg. Infect. Dis. 2017, 23, 258–263. [Google Scholar] [CrossRef]
- Grassly, N.C.; Wadood, M.Z.; Safdar, R.M.; Mahamud, A.S.; Sutter, R.W. Effect of inactivated poliovirus vaccine campaigns, Pakistan, 2014–2017. Emerg. Infect. Dis. 2018, 24, 2113–2115. [Google Scholar] [CrossRef] [PubMed]
- Thompson, K.M.; Duintjer Tebbens, R.J. Retrospective cost-effectiveness analyses for polio vaccination in the United States. Risk Anal. 2006, 26, 1423–1440. [Google Scholar] [CrossRef] [PubMed]
- Duintjer Tebbens, R.J.; Sangrujee, N.; Thompson, K.M. The costs of future polio risk management policies. Risk Anal. 2006, 26, 1507–1531. [Google Scholar] [CrossRef] [PubMed]
- Duintjer Tebbens, R.J.; Pallansch, M.A.; Kew, O.M.; Sutter, R.W.; Bruce Aylward, R.; Watkins, M.; Gary, H.; Alexander, J.; Jafari, H.; Cochi, S.L.; et al. Uncertainty and sensitivity analyses of a decision analytic model for posteradication polio risk management. Risk Anal. 2008, 28, 855–876. [Google Scholar] [CrossRef] [PubMed]
- Sangrujee, N.; Duintjer Tebbens, R.J.; Caceres, V.M.; Thompson, K.M. Policy decision options during the first 5 years following certification of polio eradication. MedGenMed 2003, 5, 35. [Google Scholar] [PubMed]
- Duintjer Tebbens, R.J.; Thompson, K.M. Modeling the potential role of inactivated poliovirus vaccine to manage the risks of oral poliovirus vaccine cessation. J. Infect. Dis. 2014, 210 (Suppl. 1), S485–S497. [Google Scholar] [CrossRef] [PubMed]
- Kalkowska, D.A.; Duintjer Tebbens, R.J.; Thompson, K.M. Modeling strategies to increase population immunity and prevent poliovirus transmission in the high-risk area of northwest Nigeria. J. Infect. Dis. 2014, 210 (Suppl. 1), S412–S423. [Google Scholar] [CrossRef] [PubMed]
- Pons-Salort, M.; Burns, C.C.; Lyons, H.; Blake, I.M.; Jafari, H.; Oberste, M.S.; Kew, O.M.; Grassly, N.C. Preventing vaccine-derived poliovirus emergence during the polio endgame. PLoS Pathog. 2016, 12, e1005728. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Time Period | 2000–2019 [1] | 2020–2024.25 | |
|---|---|---|---|
| Modeling group (first publication year) KRI (2003) IC (2006) LSHTM (2000) * IDM/BMGF (2014/2021) * SACEMA (2022) * GIT (2024) * Other economic analyses (2000) Other transmission modeling (2000) | Count (number excluded) 78 44 a,b (1 c) 17 c (1 b) 19 (2 a) NA NA 9 23 | Count (number excluded) [References] 46 [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46] 20 (3 d) [47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66] 12 d,e,f [67,68,69,70,71,72,73,74,75,76,77,78] 8 (1 e) [79,80,81,82,83,84,85,86] 0 (1 f) [67] 2 [87,88] 5 [89,90,91,92,93] 9 [94,95,96,97,98,99,100,101,102] | |
| Publication year 2000–2004 2005–2009 2010–2014 2015–2019 2020–2024.25 | Count {Rate per year} 10 {2} 26 {5} 45 {9} 109 {22} | Count {Rate per year} 102 {24} | |
| Study type Integrated (DEB and economic) DEB SC IB DES, DEB DEB, SC DEB, IC Economic/cost analysis only ** Risk assessment ** Vaccine effectiveness ** Mucosal immunity ** Reviews ** Discussions of policy options ** Perspectives/commentaries ** | Count 12 42 14 9 3 2 1 15 20 17 6 14 5 30 | Count 6 g 34 4 1 0 0 0 10 18 3 3 8 1 14 |
| Modeling Group | KRI | IC | LSHTM | IDM /BMGF | GIT | Other | |
|---|---|---|---|---|---|---|---|
| Theme | |||||||
| Outbreak response speed/quality | [7,12,15,23,25,34,35,36,44,46] | [47,52,53,55,60,62] | [70] | [84,86] | [87,88] | [90] | |
| Expanded age group SIAs | [34] | ||||||
| Population immunity* | [7,9,10,11,12,14,15,17,18,19,20,21,22,23,25,30,31,32,33,34,35,36,41,42,43,44,45,46] | [47,52,53] | [70,74] | [82,83,84,85,86] | [87,88] | ||
| OPV cessation dynamics | [14,41,42] | ||||||
| Silent transmission on an IPV | [44,45,46] | [52,53] | [68,70,71] | [80,85] | |||
| background/delayed detection | |||||||
| of transmission due to IPV use | |||||||
| Role of IPV after OPV cessation | [17,18] | [54] | [91,92] | ||||
| Undetected circulation | [11,33,45] | [67,69] | |||||
| Role of IPV in oSIAs | [22,31,44,46] | [55,66] | [87,88] | ||||
| (Environmental) surveillance | [10,11,24,33,44,45] | [50,51,59,60,61,62,63,64,65] | [69,71,75] | [81,83] | |||
| Vaccine stockpile | [40] | ||||||
| iVDPVs | [43] | ||||||
| Novel OPV (nOPV) | [13,15,16,20,22,23,25,26,27,34,35,36,37,38,39,40,41,42,43,46] | [55,56,57,58] | [72,73] | [86] | [87,88] | ||
| COVID-19/pandemic modeling | [19,20,21,22] | ||||||
| Secondary effects of OPV | [19,20,28,29] | [47] | [93] | ||||
| GPEI transition/integration | [29] | ||||||
| Containment | [12] | ||||||
| Geographic area modeled for studies with poliovirus transmission models | |||||||
| Global | [7,12,14,15,17,20,21,22,25,30,31,34,36,41,42,43] | ||||||
| Pakistan/Afghanistan | [9,19,23,32,33] | [47] | |||||
| Nigeria | [10,11] | [87,88] | |||||
| Bangladesh | [79,80] | ||||||
| Israel | |||||||
| United States | [18,44,45,46] | ||||||
| Hypothetical | [35] | [67] | [89,94,95,96,97,98,99,100,101,102] | ||||
| Year | Excerpt | Group | Study |
|---|---|---|---|
| 2000 | Refers to plans to develop a “strategy for stopping vaccination that will evaluate a number of proposed strategies, including routine immunization with the inactivated polio vaccine (IPV) or an OPV ‘pulse’ immunization followed by cessation” | ||
| 2001 | “WHO will develop policy decision models over the next 12 months that reflect how the range of possible research outcomes would affect post-certification policy development” | ||
| 2002 | A “framework has now been developed that summarizes these risks into two major categories, including (a) those due to VDPV, and (b) those due to the handling of wild poliovirus stocks” | ||
| 2003 | Key decisions in 2003: 1. Cessation of oral polio vaccine (OPV) 2. No universal introduction of the inactivated polio vaccine (IPV) 3. Strategies for the Safe Cessation of OPV “Guidelines for national decision-making on OPV cessation will be completed, outlining: (a) rationale for OPV cessation; (b) risks of polio in the post-OPV era; (c) surveillance requirements; (d) post-OPV stockpile and response; and (e) implications of IPV introduction” | ||
| 2004 | Concluded that “eradicating all forms of poliomyelitis paralysis will require eventually stopping use of OPV globally and that the cessation of OPV must be implemented simultaneously across the world” | ||
| 2005 | “A comprehensive approach must be taken to optimize the management of the risks of either the re-emergence of polio due to a cVDPV or the re-introduction of either a wild or Sabin poliovirus, following the global interruption of wild poliovirus transmission.” “The ACPE, in October 2005, issued new international standards for polio outbreak response to guide countries in planning and responding to any importations of virus” and “further expansion of mOPV use in supplementary immunization activities”, and “assessment was conducted on the consequences of a poliovirus release during or after OPV cessation (Fine P. E. M. and Ritchie S., Consequences of release/reintroduction of polioviruses in different geographic areas after OPV cessation. Risk Analysis, 2006)” | LSHTM, KRI | [121,181] a,b |
| 2006 | “Research published in Science magazine indicates monovalent OPV can boost immunity enough to stop polio in northern India.” “The humanitarian and economic case for finishing eradication is sound. A new study from Harvard University demonstrates that over a 20-year period, controlling polio at high levels would cost more in human suffering and dollars than finishing eradication.” | IC, KRI a | [177,184] |
| 2007 | “To examine the assumptions underpinning current planning for the mOPV stockpile, a Harvard University/Massachusetts Institute of Technology collaboration continues to conduct mathematical modeling of outbreak response activities for polioviruses following OPV cessation.” “In close collaboration with the Imperial College of London, studies were undertaken to better estimate the efficacy of mOPV 1 and 3 in different field settings (India, Nigeria, and Pakistan).” | KRI a, IC | [182,185] |
| 2008 | “Studies showing increased efficacy of monovalent type 1 oral polio vaccine (mOPV1) over trivalent oral polio vaccine (tOPV) in Nigeria are published in the New England Journal of Medicine, affirming the feasibility of rapidly stopping polio in that country.” “In 2008, the PRC made a grant to Kid Risk Inc., formerly part of a Harvard University and Massachusetts Institute of Technology collaboration, to continue mathematical modeling of outbreak response scenarios for polioviruses following OPV cessation to further inform policy in this area.” | IC, KRI | [183,186] |
| 2009 | “…An extensive program of research was accelerated in 2009 to develop the tools and policies to minimize and manage the long-term risks of polio.” “To prepare for the management of long-term poliovirus risks, the GPEI is focusing research and policy development on three major areas: (1) better characterizing the primary long-term poliovirus risks (ie cVDPVs, VAPP, iVDPVs, and residual stocks of WPVs, VDPVs and Sabin viruses); (2) developing new products to manage the risks associated with OPV cessation, including the development of an international stockpile of mOPVs for cVDPV response and affordable IPV options for low-income countries that perceive the medium or long-term risks of poliovirus warrant continued routine immunization after OPV, cessation. (3) Establishing mechanisms to internationally coordinate risk management strategies, particularly the application of appropriate safeguards and bio-containment conditions for the handling and storage of residual polioviruses and potentially poliovirus-infected materials, the synchronization of the cessation of routine immunization with OPV and the adherence to internationally-agreed processes for the post-eradication use of OPV in response to new cVDPVs.” | ||
| 2010 | “In a rigorous evaluation of the benefits and costs of eradicating polio, a study published in Vaccine finds that the program could provide net benefits of at least US$40–50 billion by 2035, mostly in low-income countries, if transmission of wild polioviruses is interrupted within the next five years.” “Jenkins et al, published in the New England Journal of Medicine in June 2010, analyzed the largest-ever recorded cVDPV outbreak detected in Nigeria.” | KRI, IC | [172,187] |
| 2011 | “Mathematical modeling shows that failure to eradicate the remaining 1% puts the world at significant risk of polio resurgence, potentially leading to over 200,000 children paralyzed annually within a decade.” | [177] c | |
| 2012 | “On one side of the balance, a lasting world free of polio where no child will ever know the pain of polio paralysis and US$ 50 billion in economic benefits; on the other, a resurgence of the disease resulting in 200,000 cases every year within 10 years. All countries will benefit equally from global success.” | [177] c | |
| 2013 | “Type 2 outbreak response principles were endorsed by the SAGE in November 2013. It was decided that outbreak response should utilize both monovalent OPV type 2 and IPV to rapidly boost and establish population immunity around the outbreak response zone to prevent the emergence of cVDPV. The use of mOPV2 is needed to induce intestinal immunity among those who have not been vaccinated against type-2 previously.” | ||
| 2014 | “In 2006, the World Health Assembly issued international outbreak response guidelines with specific measures countries should take upon detection of a polio outbreak in any polio-free area. Full implementation of these guidelines reduced the extent (in time and number of cases) of new outbreaks by 50% compared to previous outbreaks. Outbreak response is now more critical than ever, as the world is now closer than ever to being polio-free and the phased removal of oral polio vaccines (OPV) is beginning. That is why the GPEI has issued revised international outbreak response guidelines to countries, building on those from 2006.” | b | |
| 2015 | “A polio-free world will reap savings of more than US$ 50 billion, funds that can be used to address other pressing public health and development needs.” | [172] c | |
| 2016 | “A polio-free world will result in global savings of US$ 50 billion (mostly in developing countries).” | [172] c | |
| 2017 | “Failure to eradicate polio would result in a drastic resurgence of the disease globally, and within the next 10 years, the world could again see 200,000 new cases every single year.” “A world without polio will result in savings of more than US $50 million.” “"Globally, a polio-free world will reap savings of over US$50 billion, funds that can be used to address other pressing public health needs”. “Even if it has taken longer and cost more than all had anticipated, the goal of a polio-free world — so near at hand — is worth pursuing, for the benefit of all generations of children to come.” “In addition to the significant humanitarian benefits associated with polio eradication, the effort is also associated with substantial economic benefits. A world free of polio will result in savings of more than US$50 billion, which can be used to address other critical public health and development needs.” | [177] c [172] c | |
| 2018 | “Achieving a polio-free world will generate an estimated US$14 billion in cumulative cost savings by 2050, compared to the cost countries would incur to control the virus indefinitely. In financial terms, the global effort to eradicate polio has already saved more than US$ 27 billion in health costs since 1988.” | [188] | |
| 2019 | “…The continued spread of existing cVDPV2 outbreaks and the emergence of new cVDPV2s pointed to the insufficient quality of outbreak response with monovalent oral polio vaccine type 2 (mOPV2). The risk that these strains spread further or that new strains emerge was magnified by an ever-increasing mucosal immunity gap to type 2 poliovirus on the continent, following the switch from trivalent oral polio vaccine (tOPV) to bivalent oral polio vaccine in 2016.” | ||
| 2020 | “Analysis of data for 2020 shows an increase of 0 dose cases and a decrease in 3 plus doses case both in endemic and outbreak countries. This is probably a consequence of the COVID-19 pandemic and related disruptions of immunization campaigns.” | d | |
| 2021 | “A statistical analysis of zero-dose children was performed in 2021 using 2016–2020 sex-disaggregated surveillance data for children aged 0–36 months. It was conducted through an intra-cluster correlation coefficient and adjusted multiple regression analysis to calculate risk at the province and district levels in endemic countries (Afghanistan and Pakistan). Age and sex were used as risk variables to calculate the risk of children being among those who do not receive any dose and to calculate if this risk was equally distributed across the countries. The results were mapped to showcase the districts in which children had a higher risk of not receiving any doses.” | d | |
| 2022 | “The poliovirus is cornered to just a few high-risk geographies, but there is no room for complacency. Continuing to invest in polio eradication could save the world over US$ 30 billion in health care cost savings this century, compared to the cost of just controlling polio.” | e | |
| 2023 | NA |
| Meeting Date | Excerpt | Study/Review | Presented at the Meeting |
|---|---|---|---|
| November-1999 | “A delay in achieving the polio eradication target would increase the cost of the initiative by as much as US$ 100 million per year. In addition, it would be very difficult to sustain current funding levels for more than 24–36 months, a crucial point for those polio-free countries that would need to continue holding national immunization days beyond the target date to assure freedom from wild poliovirus” | ||
| June-2002 | “SAGE reaffirms the importance of the substantial programme of work now devoted to the development of polio immunization policy for the post-certification era. The immediate focus of this policy work should be in evaluating the feasibility of eventually stopping the routine use of oral polio-vaccine (OPV) worldwide” “SAGE recommends that the framework be supplemented by: [1] a peer review of the estimated burden of VAPP, cVDPV, and iVDPV; [2] a geopolitical/cultural understanding of how the ‘perceived risks’ that can not be answered by the scientific research agenda alone (e.g., bioterrorism, VAPP) may affect the post-certification policy in OPV-using countries; [3] an economic assessment of the various options; and [4] the completion of the research agenda to better define the risks in the post-certification era and the strengths and weaknesses of the risk management strategies” | ||
| June-2004 | “SAGE recommended that, to assist its deliberations on post-OPV immunization policy, WHO should keep it fully informed of: all related policy decisions made by the oversight groups responsible for other aspects of the OPV cessation work (i.e. the Ad-hoc Advisory Committee on Polio Eradication, the Global Commission on Certification of Polio Eradication, the Biosafety Advisory Group); the evolving understanding of the nature and magnitude of the risks of circulating polioviruses following interruption of wild poliovirus transmission and OPV cessation; and the outcomes of the continuing work to model these risks over time.” | ||
| November-2005 | “SAGE also applauded the work in progress on the post-eradication strategies” | ||
| April-2006 | “SAGE noted the ratification by ACPE of the new international standards for outbreak response” | ||
| April-2007 | “An independent analysis was presented to SAGE that supported the humanitarian and economic case for investing heavily to finish eradication. The study, published in the Lancet, showed that polio “control” would cost more over a 20-year period in human and financial terms than achieving eradication.” | [177] | |
| November-2007 | “New studies in India and Nigeria showed that monovalent OPVs afford a 3-fold to 4-fold higher effectiveness per dose than trivalent OPV.” | [184,185] | |
| November-2008 | “SAGE recommends that the mathematical model(s) of post-eradication risks be evaluated by Quantitative Immunization and Vaccine Related Research Advisory Committee (QUIVER).” | ||
| April-2009 | “Areas for further study include … models for estimating the risk of outbreaks of vaccine-derived polio in the post-eradication era, …. SAGE underlined the need for close interaction with QUIVER, given the relevance of its work to policy-making. SAGE must be fully briefed on critical assumptions and assured of the adequacy of data and methods for models that are used to inform policy decisions.” “The IPV working group presented a framework for evaluating post-eradication options for vaccination policy. SAGE was impressed with the work, but urged the working group to pay particular attention to uncertainties in mathematical modelling on the risks of emergence of vaccine-derived poliovirus.” | [182] | |
| April-2010 | “SAGE noted that the positive current epidemiological situation, the new strategic plan, and the sound economic argument for completing eradication together form a particularly appealing product for donors, warranting substantial further investment.” | [172] | |
| November-2010 | Extended the term [for the SPWG] to “… allow the working group to benefit from considering … further mathematical modelling of post-eradication risks…” “SAGE expanded the working group’s remit by requesting it to assess whether, in view of the apparent eradication of type-2 wild poliovirus and the preponderance of circulating type-2 vaccine-derived polioviruses in recent years, trivalent OPV should be replaced with bivalent OPV for routine vaccination.” | ||
| April-2012 | “SAGE also received a report from the SAGE polio working group regarding a switch from trivalent oral poliovirus vaccine (tOPV) to bivalent OPV (bOPV types 1 and 3) and related policy and technical issues, and proposed recommendations for consideration by SAGE.” | [194] | |
| April-2014 | “Upon reviewing the relevant scientific evidence, SAGE endorsed updates to the existing WHO recommendations for travellers from polio-infected countries” | [195] | |
| October-2014 | “Lastly, SAGE endorsed the proposed risk-based approach for boosting immunity to type 2 poliovirus prior to OPV2 withdrawal, by ensuring that sufficient tOPV campaigns are planned and conducted to raise population immunity above the estimated threshold for transmission in areas at highest risk of cVDPV2 emergence. SAGE emphasized that planning for this risk-based approach should be done on a subnational basis.” | [191,196] | |
| April-2015 | “SAGE noted the increased scope of planned tOPV SIAs that will be implemented to reduce the risk of emergence of new cVDPV2, building on the risk-based approach endorsed by SAGE in October 2014. SAGE endorsed the proposed cVDPV2 elimination strategies in Nigeria and Pakistan and the programme’s risk-based approach to prevent and respond to new cVDPV2 emergence in any location.” | ||
| October-2015 | “The GPEI has optimized its strategy to prevent emergence of VDPV2 through an extensive set of tOPV campaigns, more sensitive definitions of cVDPV2, immediate response to any VDPV2 detection and updated its guidelines for responding to any cVDPV outbreak.” | [197] a | |
| April-2016 | “SAGE reviewed the Polio Working Group discussion on future polio immunization policy. The Working Group proposed to work on the following recommendations: (i) an explicit decision on whether polio vaccination should be continued after global certification of eradication; (ii) the recommended IPV schedule (number of doses, timing, formulation) after OPV withdrawal; and (iii) the criteria for when countries could stop polio vaccination (e.g. surveillance capacity, absence of immunodeficiency-related vaccine-derived poliovirus), based on vaccine and funding availability and expected vaccine price” | ||
| April-2017 | “SAGE also reviewed the risk of reintroduction of polioviruses after global OPV cessation. The modelling and epidemiology suggest that VDPV may emerge 0–4 years after the global cessation of OPV use.” | a,b [198] c | |
| October-2017 | “SAGE acknowledged WHO’s work with Imperial College, London, to grade risks in Tier 3 and 4 countries based on susceptibility, transmission, exposure, and primary immunodeficiency-associated vaccine-derived poliovirus (iVDPV) prevalence.” | IC d | |
| April-2019 | “SAGE proposed that the GPEI determine the criteria for requesting that OPV2- containing vaccine production be resumed. SAGE agreed that discussions on the criteria are important and should be further explored during future working group meetings” | [199] e | |
| March-2020 | “SAGE reviewed and agreed with the new GPEI strategy for responding to cVDPV2 outbreaks” (i.e., [160])… “SAGE recommended the strategy be more cautious about setting timelines for the introduction of nOPV2… [and] that tOPV be made available to countries for cVDPV2 outbreak response in subnational areas where there is co-circulation…. SAGE requested that GPEI further elaborate scenarios for using IPV in outbreak responses” | [68,200] a,b | |
| October-2020 | “SAGE recommended that IPV should not be used for outbreak response because evidence demonstrates that IPV campaigns are unlikely to reach children not reached with OPV campaigns, have limited impact on stopping transmission and have a high programmatic cost. The priority of outbreak response is to stop transmission; therefore, activities should focus on rapidly achieving high coverage with OPV.” | [47] | |
| March-2021 | “SAGE acknowledged that countries are faced with complex decisions with regards to options for cVDPV2 outbreak response: should they use Sabin-based monovalent OPV type 2 (mOPV2) immediately and risk seeding new VDPV2s, or should they delay outbreak response until the country is programmatically prepared to use nOPV2? SAGE was presented with a modelling analysis of these options and agreed with the conclusion that countries facing cVDPV2 outbreaks should avoid delay and prioritize rapid, high-quality cVDPV2 outbreak response with whichever oral polio vaccine is available to them.” | [25] | |
| October-2022 | “SAGE was presented with a literature review and programme experience of using IPV for poliovirus outbreak control, and the role of IPV in preventing faecal-oral and oral-oral poliovirus transmission, as requested at the April 2022 SAGE meeting.” | [66] | [201,202] f |
| March-2023 | “SAGE reiterated its recommendation that outbreak responses be conducted without delay. For response using oral vaccines, nOPV2 should be preferred. However, mOPV2 could be used under exceptional conditions, e.g., if supplies of nOPV2 are inadequate, if emergency use listing (EUL) readiness cannot be achieved, and tOPV in the event of co-circulation of other poliovirus serotypes” “SAGE was presented with evidence of the role of IPV in areas of persistent poliovirus transmission” | [201,203,204] g | |
| September-2023 | “Modelling analysis suggests that, if mOPV2 had been used instead of nOPV2 since March 2021, an estimated 43 new cVDPV2 emergences would have been detected by August 2023 compared with the 7 observed with nOPV2.” | h,i,j [33] k | |
| February-2024 | NA | [52,68] a |
| Meeting | Roles a | Information Extracted from the Note for the Record | |||||
|---|---|---|---|---|---|---|---|
| N | Date | KRI | IC | LSHTM | IDM/BMGF | Presentation Topic (Presenting Modeling Group) | Group [Source(s)] |
| 1 | October-08 | M * | M * | Modeling the risks: past and future (KRI) Modeling: The next frontiers (IC) | KRI [183] | ||
| 2 | June-09 | M | M | P * | Cost-effectiveness of routine polio vaccination (LSHTM) Poliovirus transmission potential (LSHTM) | KRI [177,181,182,183,194,205,206,207,208], LSHTM [107], IC [185,186] | |
| 3 | March-11 | M * | M | P * | Modeling cVDPV risks/post-eradication policies (KRI) Options, risks, and prerequisites for OPV2 cessation (KRI) Modeling tools for cVDPV emergence (IDM) | ||
| 4 | February-12 | M * | M * | P * | Wide-spread transmission of type 2 cVDPV in Nigeria (IC) cVDPV emergence risks pre- and post-eradication (IDM) Modeling and managing VDPV risks: known and not (KRI) | NA | |
| 5 | November-12 | M | M | ||||
| 6 | June-13 | M | M | P * | VDPV emergence risk for mOPV2 post-OPV2 cessation (IDM) | NA | |
| 7 | October-13 | M | M * | P * | Post-cessation outbreak response, OPV use, cVDPV risk (IDM) | ||
| 8 | February-14 | M | M * | Review of the duration of mucosal immunity to poliovirus (IC) | |||
| 9 | July-14 | M * | M * | P * | Modeling the risk of cVDPV emergence (KRI) Risk of VDPV emergence and spread (IC) Non-polio-AFP population immunity projections (IDM) tOPV campaigns pre-OPV2 cessation (IDM) | KRI [196,209,210] IC b | |
| 10 | September-15 | M | M * | P | Serotype 2 vaccine-derived poliovirus risk assessment (IC) | ||
| 11 | January-16 | M ^ | M ^ | P | Type 2 outbreak protocol c Risks of cVDPV emergence, based on modeling (IDM) | ||
| 12 | August-16 | M * | M * | P * | Detection of type 2 Sabin virus after the switch (IC) Needs for bOPV campaigns prior to OPV13 withdrawal (KRI) Assessment of risks and implications of bOPV use (IDM) | ||
| 13 | February-17 | M * | M * | P * | Roles of different vaccines in outbreaks and the endgame (KRI) Polio endgame modeling, IPV in SIAs (IDM) Impact of IPV in RI and SIA following OPV2 withdrawal (IC) | ||
| 14 | September-17 | M | M | P * | OPV13 cessation and SIA planning (IDM) | ||
| 15 | February-18 | M | M * | Risk assessment for bOPV cessation (IDM), Role of bOPV preventive SIAs pre-bOPV cessation d | |||
| 16 | September-18 | M * | R | M | Country prioritization of IPV catchup immunization (IC) | ||
| 17 | February-19 | M | R | M | Risks and the role of bOPV preventive SIAs pre-cessation d | ||
| 18 | September-19 | M | P * | M | VAPP analysis (LSHTM) | ||
| 19 | February-20 | M * | P * | M | Role of IPV for outbreak response (IC), Scenarios for initial nOPV2 use under EUL (LSHTM) | ||
| 20 | September-20 | P * | M * | M * | Impacts of polio eradication activity disruption (LSHTM) e IPV use for cVDPV and WPV outbreak response (IC) Tracing infections and micro vaccination campaigns (IDM) | ||
| 21 | February-21 | P * | M * | M | nOPV2 versus mOPV2 for outbreak response (IC) Transition from initial to wider nOPV2 use criteria (LSHTM) | ||
| 22 | August-21 | M * | M | Update on nOPV2 policy (LSHTM) | |||
| 23 | March-22 | P * | M * | M | Field seroprevalence and immunogenicity studies (LSHTM) nOPV2 effectiveness study (IC) | ||
| 24 | August-22 | M * | M | Review of data on use of IPV for outbreak response (LSHTM) | |||
| 25 | March-23 | M * | M | Update on iVDPV epidemiology (LSHTM) | |||
| 26 | August-23 | M * | M | Options for type 1 and 2 co-circulation outbreaks (LSHTM) | |||
| 27 | February-24 | M | M | bOPV cessation planning summary of modeling f | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thompson, K.M.; Badizadegan, K. Review of Poliovirus Transmission and Economic Modeling to Support Global Polio Eradication: 2020–2024. Pathogens 2024, 13, 435. https://doi.org/10.3390/pathogens13060435
Thompson KM, Badizadegan K. Review of Poliovirus Transmission and Economic Modeling to Support Global Polio Eradication: 2020–2024. Pathogens. 2024; 13(6):435. https://doi.org/10.3390/pathogens13060435
Chicago/Turabian StyleThompson, Kimberly M., and Kamran Badizadegan. 2024. "Review of Poliovirus Transmission and Economic Modeling to Support Global Polio Eradication: 2020–2024" Pathogens 13, no. 6: 435. https://doi.org/10.3390/pathogens13060435
APA StyleThompson, K. M., & Badizadegan, K. (2024). Review of Poliovirus Transmission and Economic Modeling to Support Global Polio Eradication: 2020–2024. Pathogens, 13(6), 435. https://doi.org/10.3390/pathogens13060435