Chandipura Virus Causing Large Viral Encephalitis Outbreaks in India



Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Menghani, S.; Chikhale, R.; Raval, A.; Wadibhasme, P.; Khedekar, P. Chandipura Virus: An emerging tropical pathogen. Acta Trop. 2012, 124, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, P.N.; Rodrigues, F.M. Chandipura: A new arbovirus isolated in India from patients with febrile illness. 1967. Indian J. Med. Res. 2012, 136, 890. [Google Scholar] [PubMed]
- Rao, B.L.; Basu, A.; Wairagkar, N.S.; Gore, M.M.; Arankalle, V.A.; Thakare, J.P.; Jadi, R.S.; Rao, K.A.; Mishra, A.C. A large outbreak of acute encephalitis with high fatality rate in children in Andhra Pradesh, India, in 2003, associated with Chandipura virus. Lancet 2004, 364, 869–874. [Google Scholar] [CrossRef] [PubMed]
- Van Ranst, M. Chandipura virus: An emerging human pathogen? Lancet 2004, 364, 821–822. [Google Scholar] [CrossRef] [PubMed]
- Devi, S. India facing largest Chandipura virus outbreak in 20 years. Lancet 2024, 404, 919. [Google Scholar] [CrossRef]
- Pareek, A.; Singhal, R.; Pareek, A.; Chuturgoon, A.; Sah, R.; Mehta, R.; Al-Tawfiq, J.A.; Apostolopoulos, V. Re-emergence of Chandipura virus in India: Urgent need for public health vigilance and proactive management. New Microbes New Infect. 2024, 62, 101507. [Google Scholar] [CrossRef] [PubMed]
- DGHS. Union Health Ministry, Along with Experts Reviews the Chandipura Virus Cases and Acute Encephalitis Syndrome Cases in Gujarat, Rajasthan, and Madhya Pradesh; Press Information Bureau, Government of India: Delhi, India, 2024.
- World Health Organization. Acute Encephalitis Syndrome Due to Chandipura Virus—India; World Health Organization: Geneva, Switzerland, 2024. [Google Scholar]
- Chadha, M.S.; Arankalle, V.A.; Jadi, R.S.; Joshi, M.V.; Thakare, J.P.; Mahadev, P.V.; Mishra, A.C. An outbreak of Chandipura virus encephalitis in the eastern districts of Gujarat state, India. Am. J. Trop. Med. Hyg. 2005, 73, 566–570. [Google Scholar] [CrossRef] [PubMed]
- Dinesh, D.; Topno, R.; Pandey, K.; Kumar, R.; Sahoo, G.; Kumar, M.; Singh, B.; Paswan, W.; Das, P. Chandipura Virus Recognized among AES for the First Time in Bihar, India. Int. J. Curr. Microbiol. App Sci. 2018, 7, 3658–3663. [Google Scholar] [CrossRef]
- Gurav, Y.K.; Tandale, B.V.; Jadi, R.S.; Gunjikar, R.S.; Tikute, S.S.; Jamgaonkar, A.V.; Khadse, R.K.; Jalgaonkar, S.V.; Arankalle, V.A.; Mishra, A.C. Chandipura virus encephalitis outbreak among children in Nagpur division, Maharashtra, 2007. Indian J. Med. Res. 2010, 132, 395–399. [Google Scholar] [PubMed]
- Tandale, B.V.; Tikute, S.S.; Arankalle, V.A.; Sathe, P.S.; Joshi, M.V.; Ranadive, S.N.; Kanojia, P.C.; Eshwarachary, D.; Kumarswamy, M.; Mishra, A.C. Chandipura virus: A major cause of acute encephalitis in children in North Telangana, Andhra Pradesh, India. J. Med. Virol. 2008, 80, 118–124. [Google Scholar] [CrossRef]
- Dwibedi, B.; Sabat, J.; Hazra, R.K.; Kumar, A.; Dinesh, D.S.; Kar, S.K. Chandipura virus infection causing encephalitis in a tribal population of Odisha in eastern India. Natl. Med. J. India 2015, 28, 185–187. [Google Scholar]
- Kanabar, B.; Malek, S.; Piparva, K. Temporal Trends in Outbreaks of Chandipura Viral Infection in India: A Systematic Review. Cureus 2024, 16, e68097. [Google Scholar] [CrossRef] [PubMed]
- Chari, M.V.; Swamy, T.V. Jamshedpur fever. Br. Med. J. 1955, 2, 1298–1303. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, F.M.; Patankar, M.R.; Banerjee, K.; Bhatt, P.N.; Goverdhan, M.K.; Pavri, K.M.; Vittal, M. Etiology of the 1965 epidemic of febrile illness in Nagpur city, Maharashtra State, India. Bull. World Health Organ. 1972, 46, 173–179. [Google Scholar] [PubMed]
- Shaikh, N.J.; Wairagkar, N.S.; Reddy, S.V.; Thakare, J.P.; Gadkari, D.A. Acute encephalitis without rash in Warangal, Andhra Pradesh and Vadodara, Gujarat associated with measles virus. J. Assoc. Physicians India 2002, 50, 1198. [Google Scholar]
- Tandale, B.V.; Tomar, S.J.; Bondre, V.P.; Sapkal, G.N.; Damle, R.G.; Narang, R.; Qazi, M.S.; Goteti, P.V.; Jain, M.; Jain, D.; et al. Infectious causes of acute encephalitis syndrome hospitalizations in Central India, 2018–2020. J. Clin. Virol. 2022, 153, 105194. [Google Scholar] [CrossRef] [PubMed]
- Fontenille, D.; Traore-Lamizana, M.; Trouillet, J.; Leclerc, A.; Mondo, M.; Ba, Y.; Digoutte, J.P.; Zeller, H.G. First isolations of arboviruses from phlebotomine sand flies in West Africa. Am. J. Trop. Med. Hyg. 1994, 50, 570–574. [Google Scholar] [CrossRef] [PubMed]
- Clewley, J.P.; Bishop, D.H.; Kang, C.Y.; Coffin, J.; Schnitzlein, W.M.; Reichmann, M.E.; Shope, R.E. Oligonucleotide fingerprints of RNA species obtained from rhabdoviruses belonging to the vesicular stomatitis virus subgroup. J. Virol. 1977, 23, 152–166. [Google Scholar] [CrossRef] [PubMed]
- Kraemer, M.U.; Sinka, M.E.; Duda, K.A.; Mylne, A.Q.; Shearer, F.M.; Barker, C.M.; Moore, C.G.; Carvalho, R.G.; Coelho, G.E.; Van Bortel, W.; et al. The global distribution of the arbovirus vectors Aedes aegypti and Ae. albopictus. Elife 2015, 4, e08347. [Google Scholar] [CrossRef] [PubMed]
- Balakrishnan, A.; Mun, A.B. Ribavirin inhibits Chandipura virus replication in Vero cells. J. Med. Virol. 2020, 92, 2969–2975. [Google Scholar] [CrossRef]
- Pavitrakar, D.V.; Bondre, V.P. Antiviral effect of Favipiravir against Chandipura virus in vitro and in vivo. J. Med. Virol. 2023, 95, e28840. [Google Scholar] [CrossRef] [PubMed]
- Ogino, M.; Fedorov, Y.; Adams, D.J.; Okada, K.; Ito, N.; Sugiyama, M.; Ogino, T. Vesiculopolins, a New Class of Anti-Vesiculoviral Compounds, Inhibit Transcription Initiation of Vesiculoviruses. Viruses 2019, 11, 856. [Google Scholar] [CrossRef] [PubMed]
- Kitaura, S.; Tobiume, M.; Kawahara, M.; Satoh, M.; Kato, H.; Nakayama, N.; Nakajima, N.; Komeno, T.; Furuta, Y.; Suzuki, T.; et al. Evaluation of a novel severe combined immunodeficiency mouse model for antiviral drug evaluation against Chandipura virus infection. Antivir. Res. 2023, 213, 105582. [Google Scholar] [CrossRef]

{kind=link}
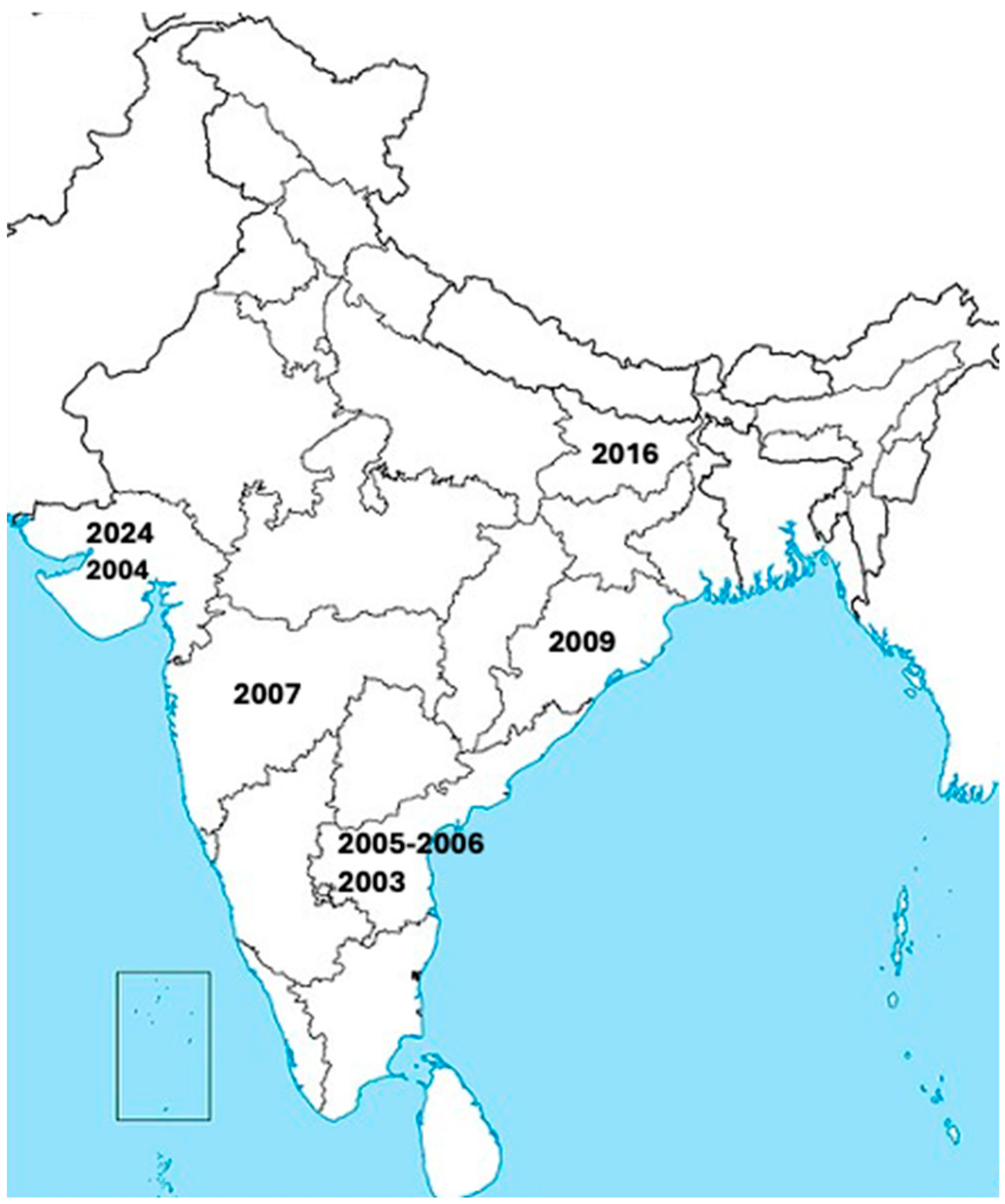
| Date * | Regions # | AES Cases ^ | Ages Affected ~ | CFR ” |
|---|---|---|---|---|
| 2024 | Gujurat | 245 | Under 15 years | 33% |
| 2016 | Bihar | 24 | 1-15 years | 20.8% |
| 2009 | Odisha | 21 | Under 10 years to over 18 years | 28.6% |
| 2007 | Maharashtra | 78 | Under 15 years | 43.6% |
| 2005–2006 | Andhra Pradesh | 52 | Under 15 years | 54.4% |
| 2004 | Gujurat | 20 | 2 to 16 years | 78.3% |
| 2003 | Andhra Pradesh | 55 | 2.5 months to 15 years | 54.9% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brisse, M.E.; Ly, H. Chandipura Virus Causing Large Viral Encephalitis Outbreaks in India. Pathogens 2024, 13, 1110. https://doi.org/10.3390/pathogens13121110
Brisse ME, Ly H. Chandipura Virus Causing Large Viral Encephalitis Outbreaks in India. Pathogens. 2024; 13(12):1110. https://doi.org/10.3390/pathogens13121110
Chicago/Turabian StyleBrisse, Morgan E., and Hinh Ly. 2024. "Chandipura Virus Causing Large Viral Encephalitis Outbreaks in India" Pathogens 13, no. 12: 1110. https://doi.org/10.3390/pathogens13121110
APA StyleBrisse, M. E., & Ly, H. (2024). Chandipura Virus Causing Large Viral Encephalitis Outbreaks in India. Pathogens, 13(12), 1110. https://doi.org/10.3390/pathogens13121110