Frequency of Group A Streptococcus Infection and Analysis of Antibiotic Use in Patients with Pharyngitis—A Retrospective, Multicenter Study


 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
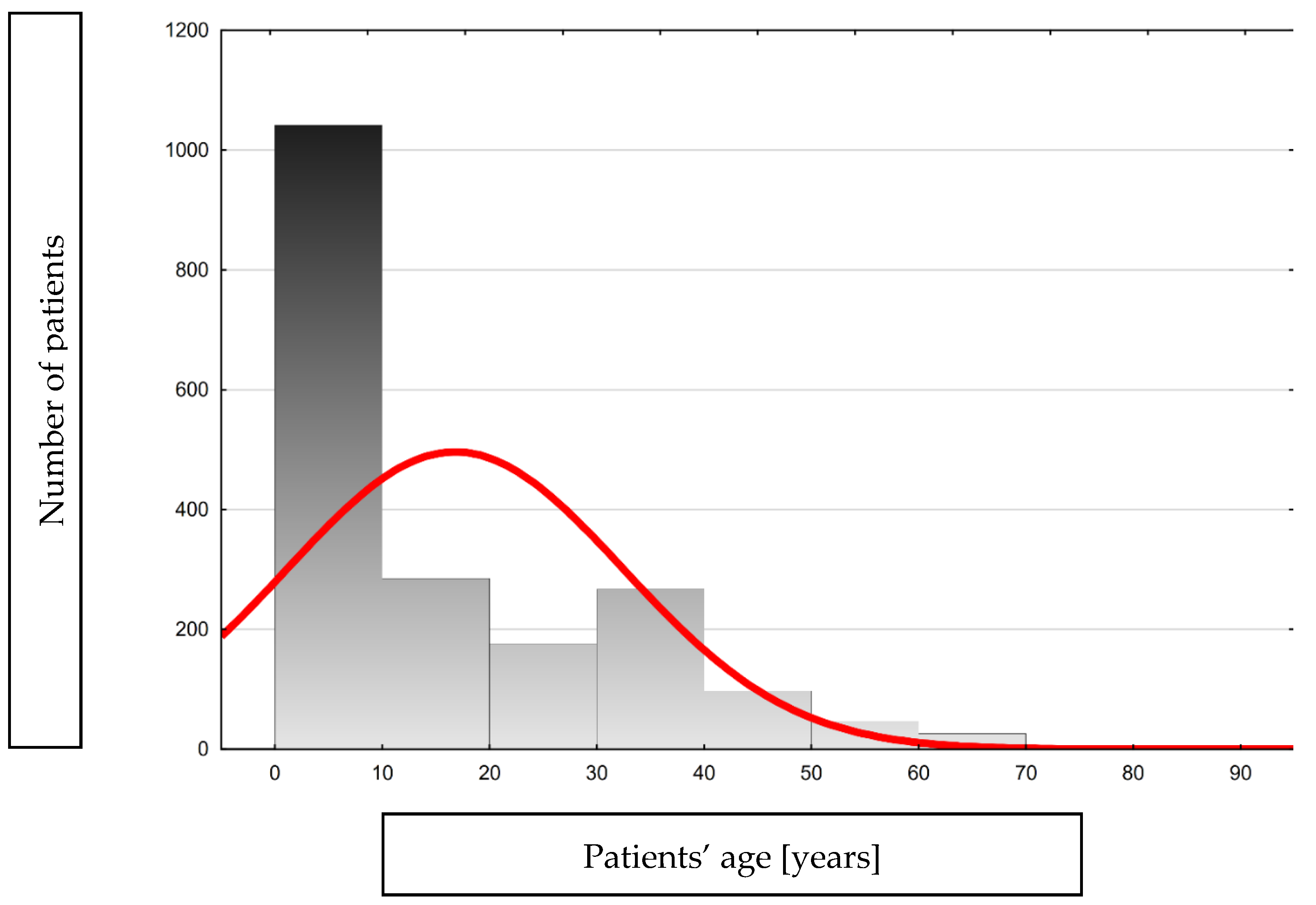
3.1. Characteristics of Analyzed Data
3.1.1. Viral Infection Prophylaxis
3.1.2. Comorbidity
3.2. Streptococcus Pyogenes’ Infection
3.3. Antibiotics Usage
3.4. Statistical Analysis of Rapid Strep Test Results and Sociodemographic and Clinical Indicators
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kanwal, S.; Vaitla, P. Streptococcus Pyogenes. In StatPearls [Internet]; National Library of Medicine: Bethesda, MD, USA, 2024. [Google Scholar] [PubMed]
- Guy, R.; Henderson, K.L.; Coelho, J.; Hughes, H.; Mason, E.L.; Gerver, S.M.; Demirjian, A.; Watson, C.; Sharp, A.; Brown, C.S.; et al. Increase in invasive group A streptococcal infection notifications, England, 2022. Eurosurveillance 2023, 28, 2200942. [Google Scholar] [CrossRef] [PubMed]
- de Gier, B.; Marchal, N.; de Beer-Schuurman, I.; Te Wierik, M.; Hooiveld, M.; de Melker, H.E.; van Sorge, N.M.; Members of the GAS Study Group; Members of the ISIS-AR Study Group. Increase in invasive group A streptococcal (Streptococcus pyogenes) infections (iGAS) in young children in The Netherlands, 2022. Eurosurveillance 2023, 28, 2200941. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Regional Office for Europe (WHO/Europe). Increase in Invasive Group A Streptococcal Infections among Children in Europe, Including Fatalities 2022. Available online: https://www.who.int/europe/news/item/12-12-2022-increase-in-invasive-group-a-streptococcal-infections-among-children-in-europe--including-fatalities (accessed on 21 July 2024).
- European Centre for Disease Prevention and Control. Communicable Diseases Threat. Week 12, 17–23 March 2024. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/communicable-disease-threats-report-week-12-2024.pdf (accessed on 21 July 2024).
- Shulman, S.T.; Bisno, A.L.; Clegg, H.W.; Gerber, M.A.; Kaplan, E.L.; Lee, G.; Martin, J.M.; Van Beneden, C. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2012, 55, 1279–1282. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Clinical Guidance for Group A Streptococcal Pharyngitis. Available online: https://www.cdc.gov/group-a-strep/hcp/clinical-guidance/strep-throat.html?CDC_AAref_Val=https://www.cdc.gov/groupastrep/diseases-hcp/strep-throat.html (accessed on 21 July 2024).
- Carapetis, J.R.; Steer, A.C.; Mulholland, E.K.; Weber, M. The global burden of group A streptococcal diseases. Lancet Infect Dis. 2005, 5, 685–694. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, M.D.S.; Koziatek, C.A.; Rajnik, M. Acute Rheumatic Fever. [Updated 2 August 2023]. In StatPearls [Internet]; National Library of Medicine: Bethesda, MD, USA, 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK594238/ (accessed on 22 July 2024).
- Hryniewicz, W.; Albrecht, P.; Radzikowski, A. Rekomendacje Postepowania w Pozaszoitalnych Zakażeniach Układu Oddechowego 2016. Available online: https://antybiotyki.edu.pl/rekomendacje/rekomendacje-diagnostyki-i-terapii-zakazen/ (accessed on 22 July 2024).
- Johannesen, T.B.; Munkstrup, C.; Edslev, S.M.; Baig, S.; Nielsen, S.; Funk, T.; Kristensen, D.K.; Jacobsen, L.H.; Ravn, S.F.; Bindslev, N.; et al. Increase in invasive group A streptococcal infections and emergence of novel, rapidly expanding sub-lineage of the virulent Streptococcus pyogenes M1 clone, Denmark, 2023. Eurosurveillance 2023, 28, 2300291. [Google Scholar] [CrossRef] [PubMed]
- HSE. HSE Expert Advisory Committee: Antibiotic Prescribing, Pharyngitis/Sore Throat/Tonsillitis. 2021. Available online: https://www.hse.ie/eng/services/list/2/gp/antibiotic-prescribing/conditions-and-treatments/upper-respiratory/pharyngitis-sore-throat-tonsillitis/ (accessed on 30 July 2024).
- de Paor, M.; Boland, F.; Fahey, T.; Smith, S.; MacDonncha, E.; Vellinga, A. Management of sore throat (with focus on GAS) in young adults. Clin. Infect. Pract. 2024, 23, 100368. [Google Scholar] [CrossRef]
- Casey, J.R.; Pichichero, M.E. Meta-analysis of cephalosporins versus penicillin for treatment of group A streptococcal tonsillopharyngitis in adults. Clin. Infect. Dis. 2004, 38, 1526–1534. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, E.L.; Chhatwal, G.S.; Rohde, M. Reduced ability of penicillin to eradicate ingested group A streptococci from epithelial cells: Clinical and pathogenetic implications. Clin. Infect. Dis. 2006, 43, 1398–1406. [Google Scholar] [CrossRef] [PubMed]
- Muhtarova, A.; Gergova, R.; Mitov, I. Distribution of macrolide resistance mechanisms in Bulgarian clinical isolates of Streptococcus pyogenes during the years of 2013–2016. J. Glob. Antimicrob. Resist. 2017, 10, 238–242. [Google Scholar] [CrossRef] [PubMed]
- Arêas, G.P.; Schuab, R.B.; Neves, F.P.; Barros, R.R. Antimicrobial susceptibility patterns, emm type distribution and genetic diversity of Streptococcus pyogenes recovered in Brazil. Mem. Inst. Oswaldo Cruz 2014, 109, 935–939. [Google Scholar] [CrossRef] [PubMed]
- Gajdács, M.; Ábrók, M.; Lázár, A.; Burián, K. Beta-Haemolytic Group A, C and G Streptococcal Infections in Southern Hungary: A 10-Year Population-Based Retrospective Survey (2008–2017) and a Review of the Literature. Infect. Drug. Resist. 2020, 13, 4739–4749. [Google Scholar] [CrossRef] [PubMed]
- Meletis, G.; Soulopoulos Ketikidis, A.L.; Floropoulou, N.; Tychala, A.; Kagkalou, G.; Vasilaki, O.; Mantzana, P.; Skoura, L.; Protonotariou, E. Antimicrobial resistance rates of Streptococcus pyogenes in a Greek tertiary care hospital: 6-year data and literature review. New Microbiol. 2023, 46, 37–42. [Google Scholar] [PubMed]
- Butler, T.A.J.; Story, C.; Green, E.; Williamson, K.M.; Newton, P.; Jenkins, F.; Varadhan, H.; van Hal, S. Insights gained from sequencing Australian non-invasive and invasive Streptococcus pyogenes isolates. Microb. Genom. 2024, 10, 001152. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Rivers, J.; Mathis, S.; Li, Z.; Velusamy, S.; Nanduri, S.A.; Van Beneden, C.A.; Snippes-Vagnone, P.; McGee, L.; Chochua, S.; et al. Genomic Surveillance of Streptococcus pyogenes Strains Causing Invasive Disease, United States, 2016–2017. Front. Microbiol. 2020, 11, 1547. [Google Scholar] [CrossRef] [PubMed]
- Gergova, R.; Boyanov, V.; Muhtarova, A.; Alexandrova, A. A Review of the Impact of Streptococcal Infections and Antimicrobial Resistance on Human Health. Antibiotics 2024, 13, 360. [Google Scholar] [CrossRef] [PubMed]
- Langley, G.; Hao, Y.; Pondo, T.; Miller, L.; Petit, S.; Thomas, A.; Lindegren, M.L.; Farley, M.M.; Dumyati, G.; Como-Sabetti, K.; et al. The Impact of Obesity and Diabetes on the Risk of Disease and Death due to Invasive Group A Streptococcus Infections in Adults. Clin. Infect. Dis. 2016, 62, 845–852. [Google Scholar] [CrossRef] [PubMed]
- Alexandre, M.; Wang’ondu, R.; Cooney, L.M., Jr. Group A Streptococcal Bacteremia following Streptococcal Pharyngitis in an Older Patient with Diabetes: A Case Report. Yale J. Biol. Med. 2017, 90, 337–340. [Google Scholar] [PubMed] [PubMed Central]
- Stevens, D.L.; Bryant, A.E. Severe Group A Streptococcal Infections. 2016 Feb 10. In Streptococcus pyogenes: Basic Biology to Clinical Manifestations [Internet]; Ferretti, J.J., Stevens, D.L., Fischetti, V.A., Eds.; University of Oklahoma Health Sciences Center: Oklahoma City, OK, USA, 2016. Available online: https://www.ncbi.nlm.nih.gov/books/NBK333425/ (accessed on 30 July 2024).


{kind=link}
{kind=link}
| N | Mean | Median | Minimum | Maximum | 25Q | 75Q | SD | |
|---|---|---|---|---|---|---|---|---|
| Age [years] | 1949 | 16.8 | 10.0 | 0.0 | 83.0 | 5.0 | 28.0 | 15.7 |
| N | Mean | Median | Min. | Max. | 25Q | 75Q | SD | |
|---|---|---|---|---|---|---|---|---|
| Time from symptom onset to rapid strep test | 1637 | 2.67 | 2.00 | 0.00 | 30.00 | 1.00 | 3.00 | 2.23 |
| Antibiotic (Name of Active Substance) | No. | % |
|---|---|---|
| clarithromycin | 46 | 4.4 |
| penicillin V | 431 | 41.0 |
| azithromycin | 33 | 3.1 |
| amoxicillin | 219 | 20.8 |
| cefuroxime axetil | 71 | 6.7 |
| amoxicillin-clavulanate | 90 | 8.6 |
| levofloxacin | 1 | 0.1 |
| cefadroxil | 131 | 12.5 |
| cefaclor | 11 | 1.0 |
| cefixime | 2 | 0.2 |
| clindamycin | 17 | 1.6 |
| Antibiotics | Negative Strep Test Result | Positive Strep Test Result |
|---|---|---|
| Clarithromycin | 18 | 28 |
| penicillin V | 25 | 406 |
| Azithromycin | 22 | 11 |
| Amoxicillin | 78 | 141 |
| cefuroxime axetil | 24 | 47 |
| amoxicillin-clavulanate | 33 | 57 |
| Levofloxacin | 1 | 0 |
| Cefadroxil | 15 | 116 |
| Cefaclor | 3 | 8 |
| Cefixime | 2 | 0 |
| Clindamycin | 3 | 14 |
| Indicators: | Positive Strep Test Results (n) | Negative Strep Test Results (n) | p Value |
|---|---|---|---|
| Sex: | |||
| Women | 462 | 629 | |
| Men | 368 | 490 | 0.809 |
| Age: | |||
| 0–18 years | 579 | 735 | |
| >18 years | 251 | 384 | 0.0577 |
| Vaccination status against influenza: | |||
| No vaccination | 670 | 927 | |
| Vaccinated | 65 | 63 | |
| No data | 95 | 129 | 0.151 |
| Vaccination status against COVID-19: | |||
| No vaccination | 504 | 673 | |
| Vaccinated | 227 | 329 | |
| No data | 99 | 117 | 0.436 |
| Diabetes: | |||
| Yes | 5 | 17 | |
| No | 825 | 1102 | 0.0582 |
| Chronic respiratory diseases: | |||
| Yes | 42 | 62 | |
| No | 788 | 1057 | 0.641 |
| Cardiovascular diseases: | |||
| Yes | 8 | 13 | |
| No | 822 | 1106 | 0.676 |
| Hypertension: | |||
| Yes | 29 | 50 | |
| No | 801 | 1069 | 0.281 |
| Congenital or acquired immunodeficiencies: | |||
| Yes | 5 | 7 | |
| No | 825 | 1112 | 0.948 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biała, M.; Babicki, M.; Malchrzak, W.; Janiak, S.; Gajowiak, D.; Żak, A.; Kłoda, K.; Gibas, P.; Ledwoch, J.; Myśliwiec, A.; et al. Frequency of Group A Streptococcus Infection and Analysis of Antibiotic Use in Patients with Pharyngitis—A Retrospective, Multicenter Study. Pathogens 2024, 13, 846. https://doi.org/10.3390/pathogens13100846
Biała M, Babicki M, Malchrzak W, Janiak S, Gajowiak D, Żak A, Kłoda K, Gibas P, Ledwoch J, Myśliwiec A, et al. Frequency of Group A Streptococcus Infection and Analysis of Antibiotic Use in Patients with Pharyngitis—A Retrospective, Multicenter Study. Pathogens. 2024; 13(10):846. https://doi.org/10.3390/pathogens13100846
Chicago/Turabian StyleBiała, Martyna, Mateusz Babicki, Wojciech Malchrzak, Sandra Janiak, Dominik Gajowiak, Alan Żak, Karolina Kłoda, Piotr Gibas, Justyna Ledwoch, Anna Myśliwiec, and et al. 2024. "Frequency of Group A Streptococcus Infection and Analysis of Antibiotic Use in Patients with Pharyngitis—A Retrospective, Multicenter Study" Pathogens 13, no. 10: 846. https://doi.org/10.3390/pathogens13100846
APA StyleBiała, M., Babicki, M., Malchrzak, W., Janiak, S., Gajowiak, D., Żak, A., Kłoda, K., Gibas, P., Ledwoch, J., Myśliwiec, A., Kopyt, D., Węgrzyn, A., Knysz, B., & Leśnik, P. (2024). Frequency of Group A Streptococcus Infection and Analysis of Antibiotic Use in Patients with Pharyngitis—A Retrospective, Multicenter Study. Pathogens, 13(10), 846. https://doi.org/10.3390/pathogens13100846