


The Modulated Role of Toxoplasma gondii on Eosinophils in Psychiatric Disorders after Cannabis Cessation

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collected
2.3. Data Analyses
3. Results
3.1. Description of the Population
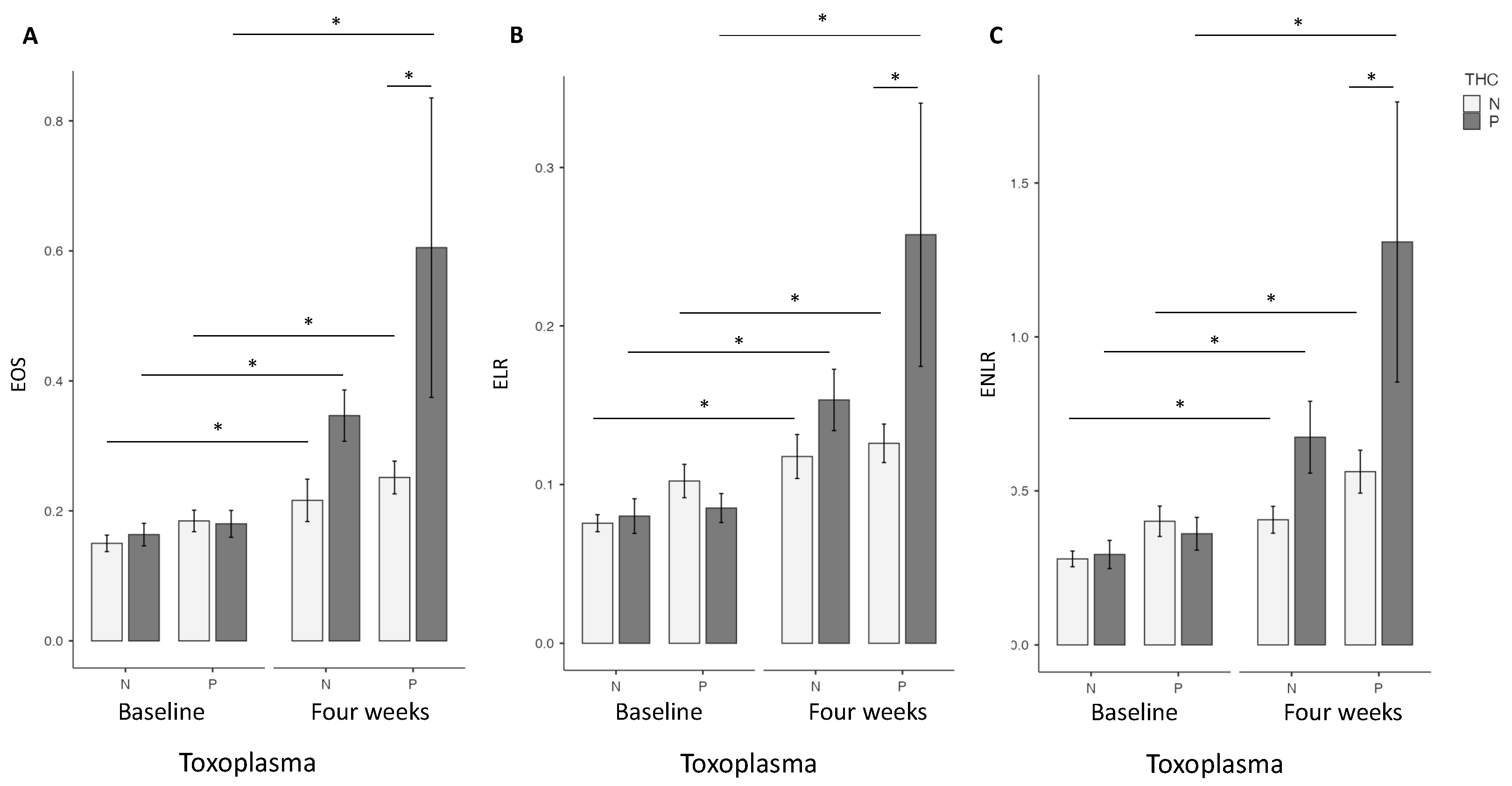
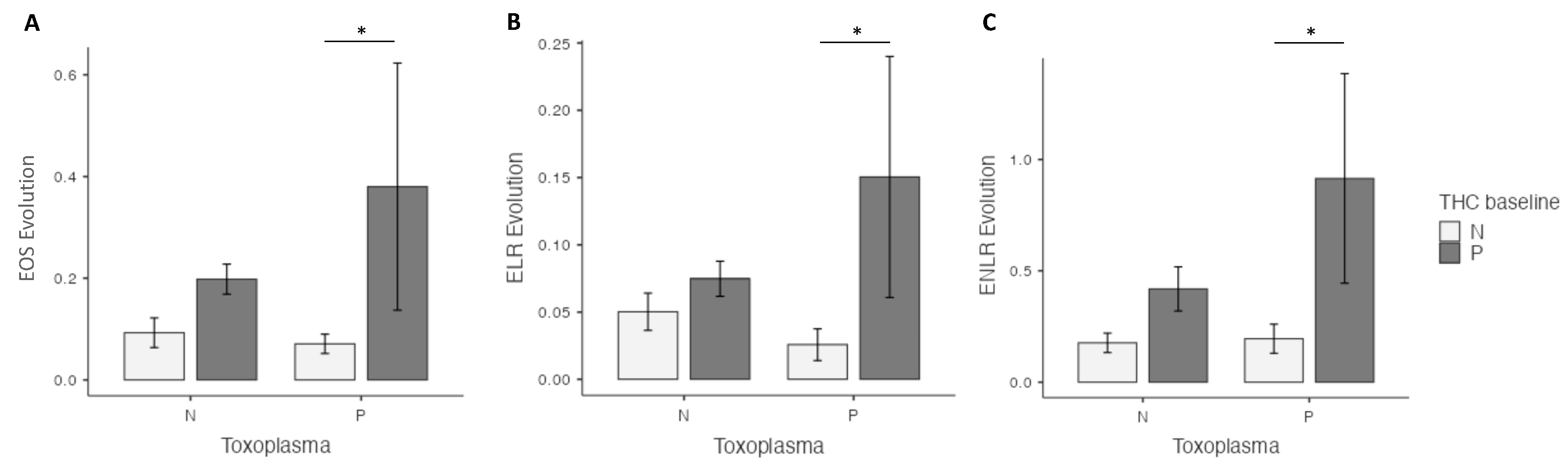
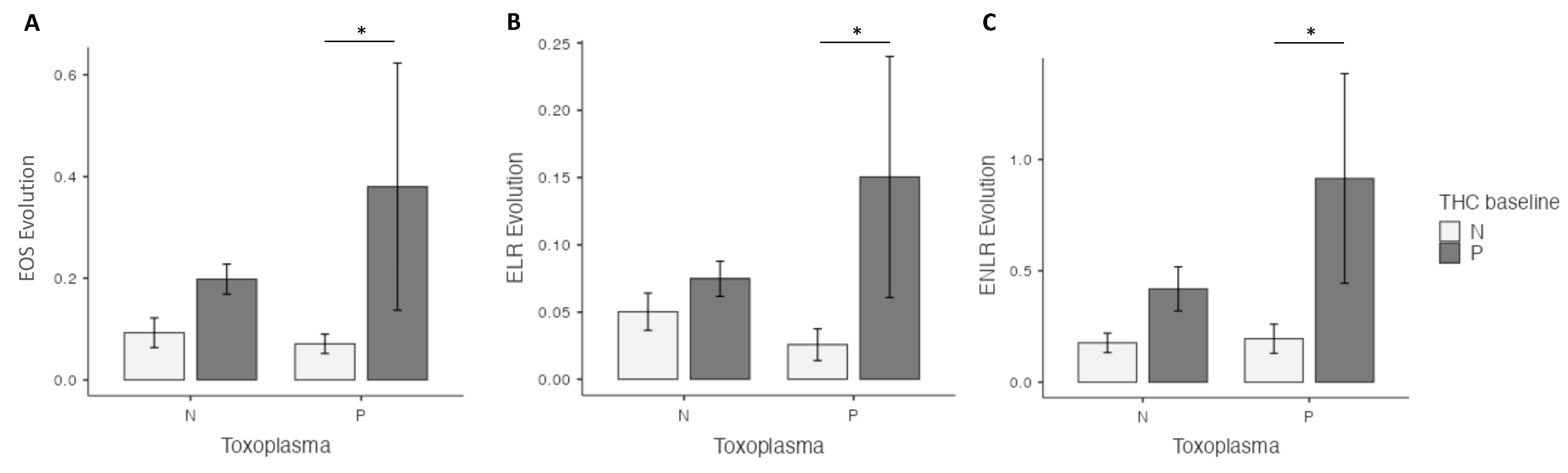
3.2. Comparison of EOS, ELR and ENLR Levels between Cannabis Users and Non-Users in Patients according to the Seropositivy of T. gondii
3.3. Comparison of EOS, ELR and ENLR Levels between Cannabis Users and Non-Users in Patients Seronegative for T. gondii
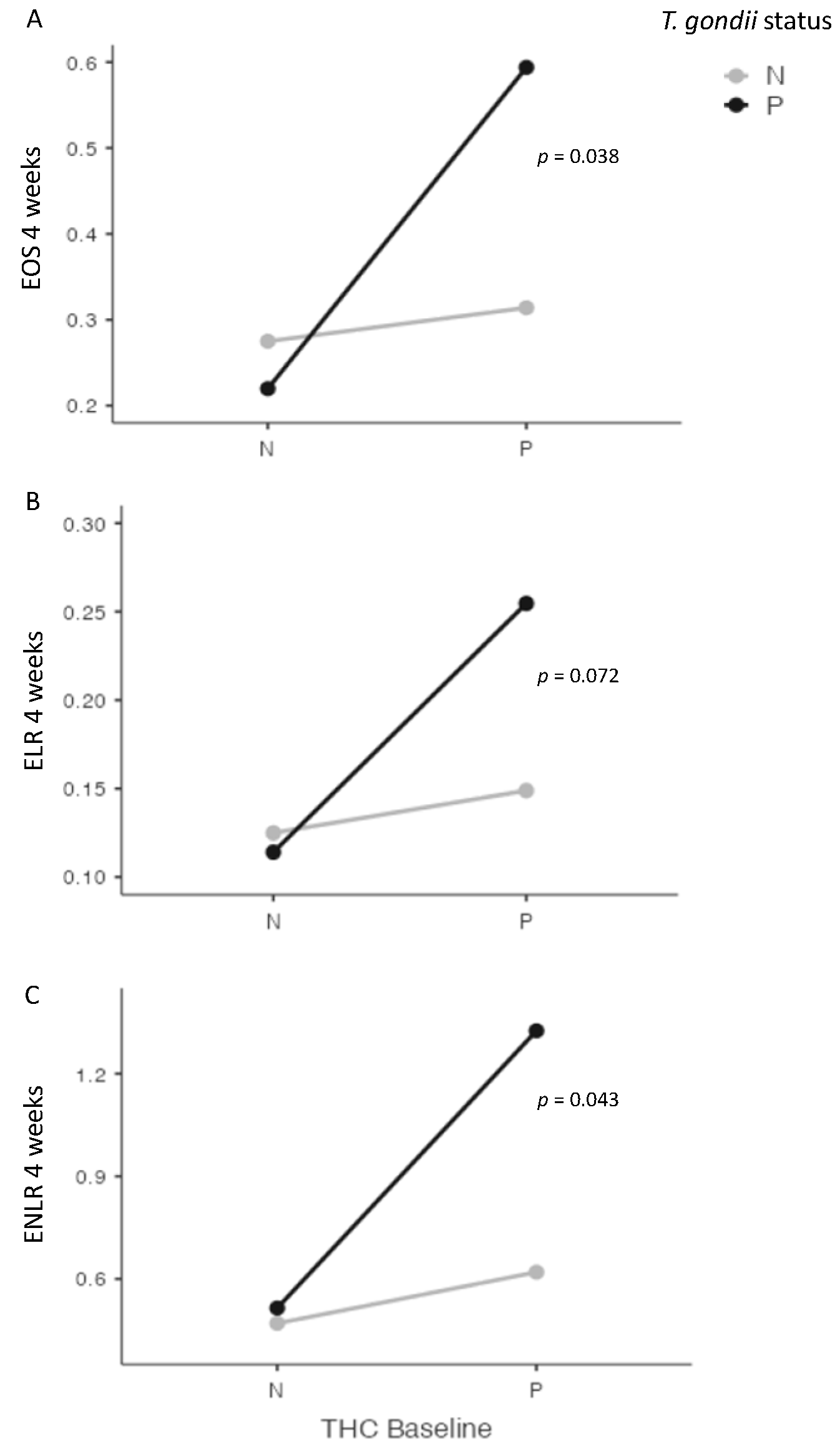
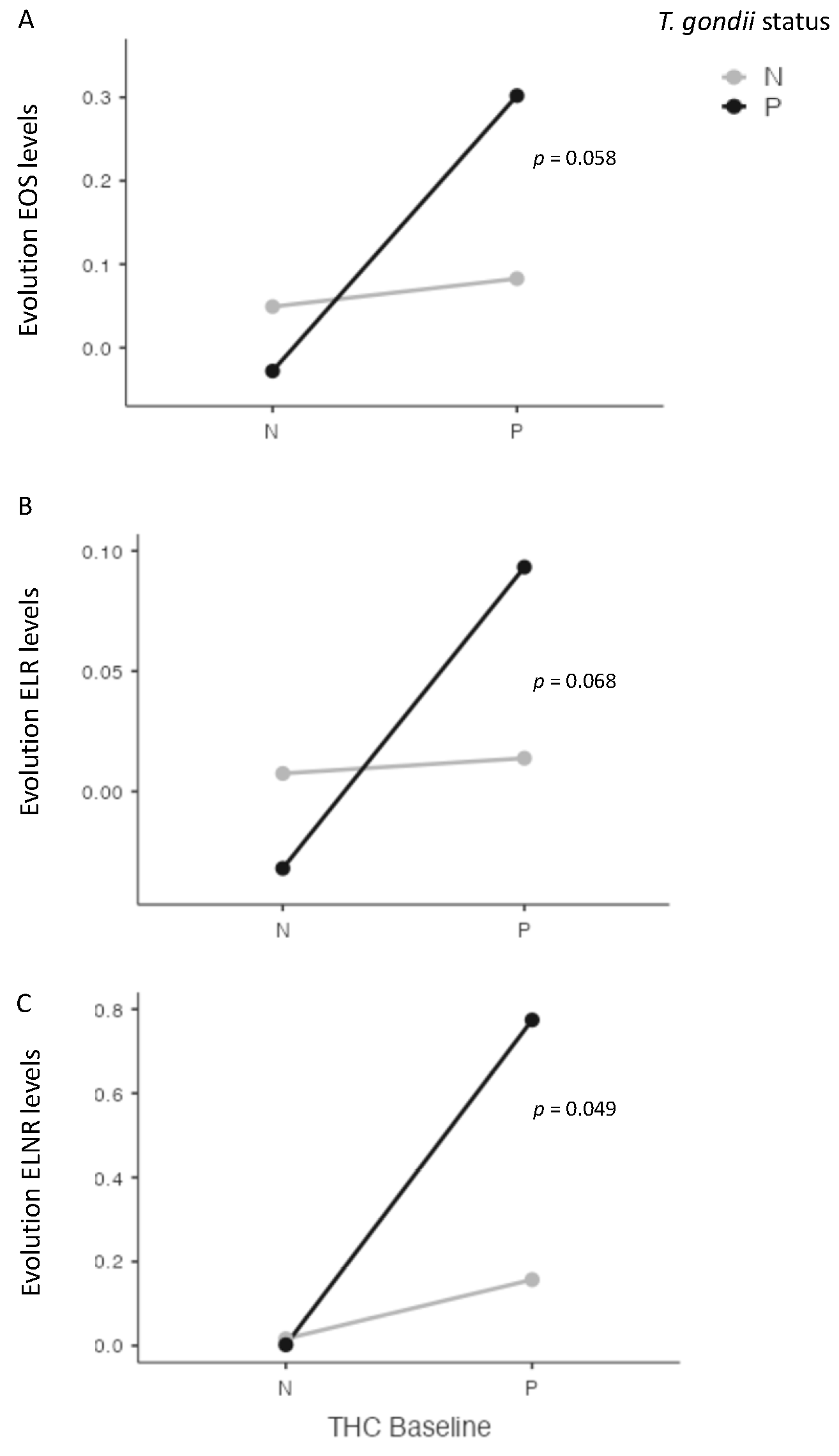
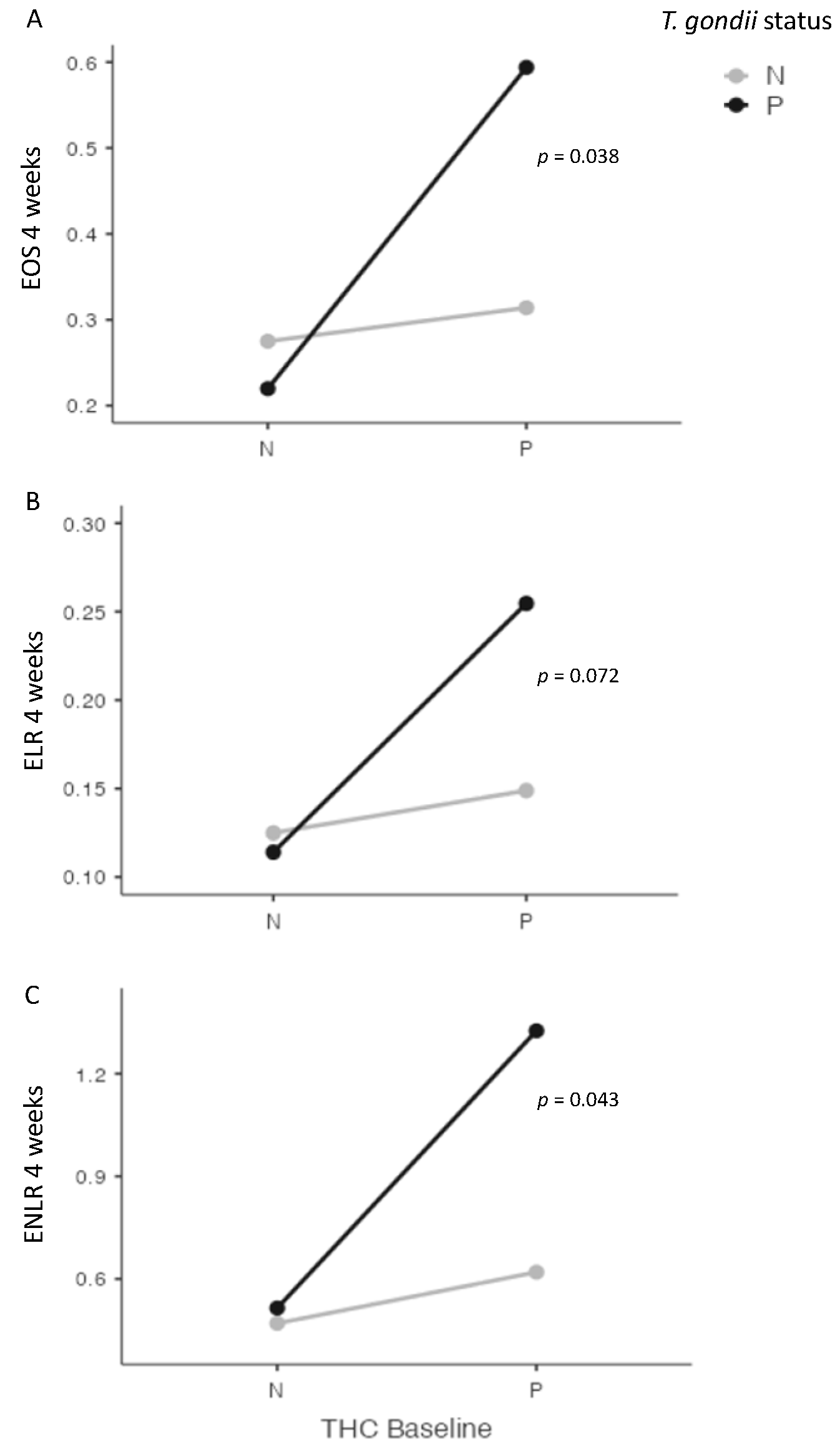
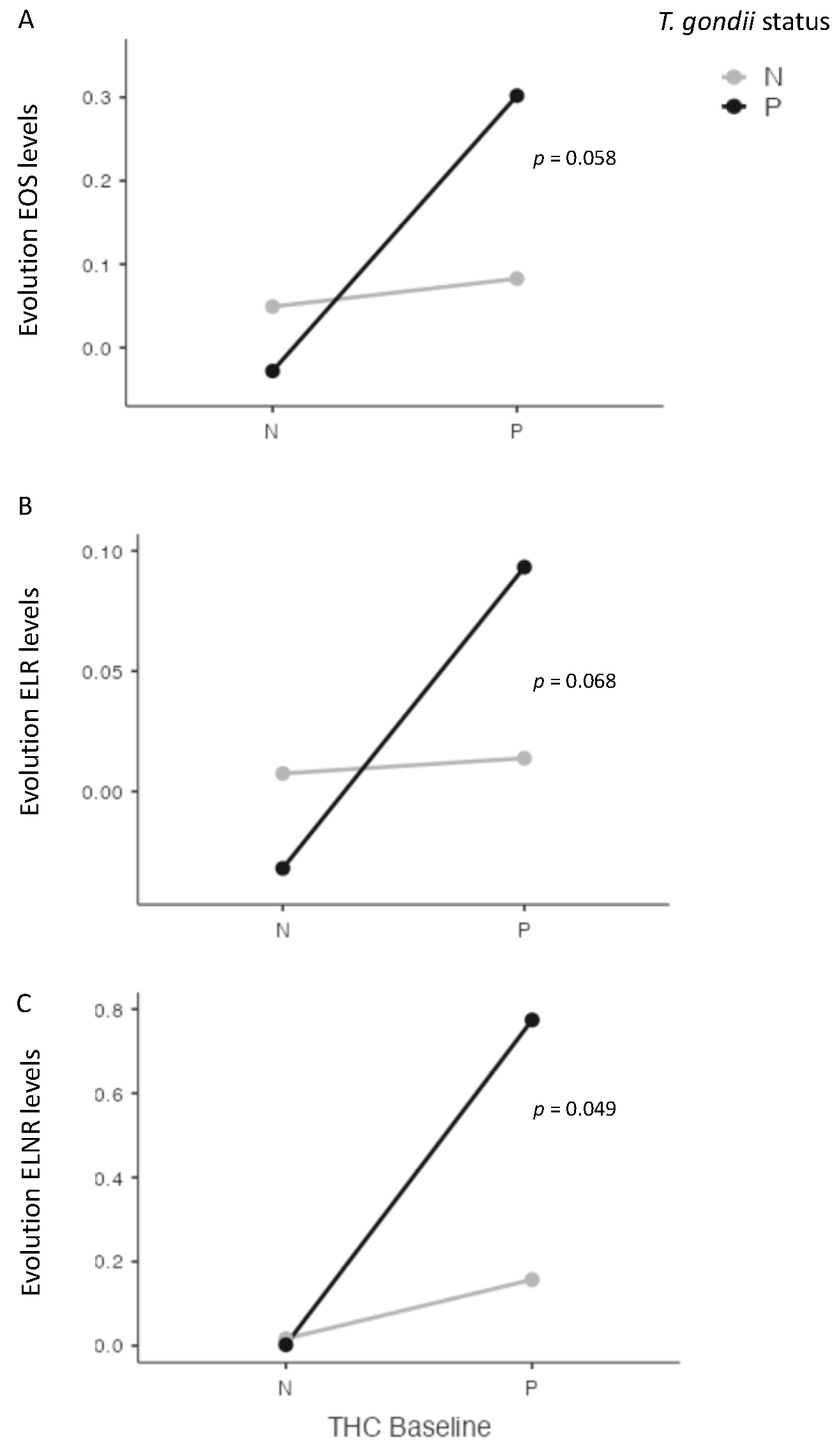
3.4. Interaction between Cannabis and T. gondii Status and EOS, ELR and ENLR
3.5. Correlation between IgG Antibodies against T. gondii, EOS, ELR, ENLR and Clinical Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- de Haan, L.; Sutterland, A.L.; Schotborgh, J.V.; Schirmbeck, F.; de Haan, L. Association of Toxoplasma gondii Seropositivity With Cognitive Function in Healthy People: A Systematic Review and Meta-analysis. JAMA Psychiatry 2021, 78, 1103. [Google Scholar] [CrossRef] [PubMed]
- Nogareda, F.; Le Strat, Y.; Villena, I.; De Valk, H.; Goulet, V. Incidence and prevalence of Toxoplasma gondii infection in women in France, 1980–2020: Model-based estimation. Epidemiol. Infect. 2014, 142, 1661–1670. [Google Scholar] [CrossRef] [PubMed]
- Aguirre, A.A.; Longcore, T.; Barbieri, M.; Dabritz, H.; Hill, D.; Klein, P.N.; Sizemore, G.C. The One Health Approach to Toxoplasmosis: Epidemiology, Control, and Prevention Strategies. EcoHealth 2019, 16, 378–390. [Google Scholar] [CrossRef] [PubMed]
- Cossu, G.; Preti, A.; Gyppaz, D.; Gureje, O.; Carta, M.G. Association between toxoplasmosis and bipolar disorder: A systematic review and meta-analysis. J. Psychiatr. Res. 2022, 153, 284–291. [Google Scholar] [CrossRef]
- Hamdani, N.; Daban-Huard, C.; Lajnef, M.; Richard, J.R.; Delavest, M.; Godin, O.; Leboyer, M. Relationship between Toxoplasma gondii infection and bipolar disorder in a French sample. J. Affect. Disord. 2013, 148, 444–448. [Google Scholar] [CrossRef]
- Sutterland, A.L.; Fond, G.; Kuin, A.; Koeter, M.W.J.; Lutter, R.; Van Gool, T.; De Haan, L. Beyond the association. Toxoplasma gondii in schizophrenia, bipolar disorder, and addiction: Systematic review and meta-analysis. Acta Psychiatr. Scand. 2015, 132, 161–179. [Google Scholar] [CrossRef]
- Chaudhury, A.; Ramana, B. Schizophrenia and bipolar disorders: The Toxoplasma connection. Trop. Parasitol. 2019, 9, 71. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.K.; Johnson, P.T.J. Toxoplasmosis: Recent Advances in Understanding the Link Between Infection and Host Behavior. Annu. Rev. Anim. Biosci. 2021, 9, 249–264. [Google Scholar] [CrossRef]
- Tyebji, S.; Seizova, S.; Hannan, A.J.; Tonkin, C.J. Toxoplasmosis: A pathway to neuropsychiatric disorders. Neurosci. Biobehav. Rev. 2019, 96, 72–92. [Google Scholar] [CrossRef]
- Hamdani, N.; Daban-Huard, C.; Lajnef, M.; Gadel, R.; Le Corvoisier, P.; Delavest, M.; Leboyer, M. Cognitive deterioration among bipolar disorder patients infected by Toxoplasma gondii is correlated to interleukin 6 levels. J. Affect. Disord. 2015, 179, 161–166. [Google Scholar] [CrossRef]
- Fond, G.; Boyer, L.; Schürhoff, F.; Berna, F.; Godin, O.; Bulzacka, E.; Zinetti-Bertschy, A. Latent toxoplasma infection in real-world schizophrenia: Results from the national FACE-SZ cohort. Schizophr. Res. 2018, 201, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Khandaker, G.M.; Cousins, L.; Deakin, J.; Lennox, B.R.; Yolken, R.; Jones, P.B. Inflammation and immunity in schizophrenia: Implications for pathophysiology and treatment. Lancet Psychiatry 2015, 2, 258–270. [Google Scholar] [CrossRef] [PubMed]
- Howes, O.D.; McCutcheon, R. Inflammation and the neural diathesis-stress hypothesis of schizophrenia: A reconceptualization. Transl. Psychiatry 2017, 7, e1024. [Google Scholar] [CrossRef]
- Müller, N. Inflammation in Schizophrenia: Pathogenetic Aspects and Therapeutic Considerations. Schizophr. Bull. 2018, 44, 973–982. [Google Scholar] [CrossRef]
- Mazza, M.G.; Lucchi, S.; Rossetti, A.; Clerici, M. Neutrophil-lymphocyte ratio, monocyte-lymphocyte ratio and platelet-lymphocyte ratio in non-affective psychosis: A meta-analysis and systematic review. World J. Biol. Psychiatry 2020, 21, 326–338. [Google Scholar] [CrossRef]
- Mazza, M.G.; Lucchi, S.; Tringali, A.G.M.; Rossetti, A.; Botti, E.R.; Clerici, M. Neutrophil/lymphocyte ratio and platelet/lymphocyte ratio in mood disorders: A meta-analysis. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2018, 84, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Jackson, A.J.; Miller, B.J. Meta-analysis of total and differential white blood cell counts in schizophrenia. Acta Psychiatr. Scand. 2020, 142, 18–26. [Google Scholar] [CrossRef]
- Miller, B.J.; Mellor, A.; Buckley, P. Total and differential white blood cell counts, high-sensitivity C-reactive protein, and the metabolic syndrome in non-affective psychoses. Brain Behav. Immun. 2013, 31, 82–89. [Google Scholar] [CrossRef]
- do Prado, C.H.; Rizzo, L.B.; Wieck, A.; Lopes, R.P.; Teixeira, A.L.; Grassi-Oliveira, R.; Bauer, M.E. Reduced regulatory T cells are associated with higher levels of Th1/TH17 cytokines and activated MAPK in type 1 bipolar disorder. Psychoneuroendocrinology 2013, 38, 667–676. [Google Scholar] [CrossRef]
- Pietruczuk, K.; Lisowska, K.A.; Grabowski, K.; Landowski, J.; Cubała, W.J.; Witkowski, J.M. Peripheral blood lymphocyte subpopulations in patients with bipolar disorder type II. Sci. Rep. 2019, 9, 5869. [Google Scholar] [CrossRef]
- Becking, K.; Haarman, B.C.; Grosse, L.; Nolen, W.A.; Claes, S.; Arolt, V.; Drexhage, H.A. The circulating levels of CD4+ t helper cells are higher in bipolar disorder as compared to major depressive disorder. J. Neuroimmunol. 2018, 319, 28–36. [Google Scholar] [CrossRef]
- Barbosa, P.C.R.; Tófoli, L.F.; Bogenschutz, M.P.; Hoy, R.; Berro, L.F.; Marinho, E.A.V.; Winkelman, M.J. Assessment of Alcohol and Tobacco Use Disorders Among Religious Users of Ayahuasca. Front. Psychiatry 2018, 9, 136. [Google Scholar] [CrossRef] [PubMed]
- Herrera-Imbroda, J.; Flores-López, M.; Ruiz-Sastre, P.; Gómez-Sánchez-Lafuente, C.; Bordallo-Aragón, A.; Rodríguez de Fonseca, F.; Mayoral-Cleríes, F. The Inflammatory Signals Associated with Psychosis: Impact of Comorbid Drug Abuse. Biomedicines 2023, 11, 454. [Google Scholar] [CrossRef] [PubMed]
- Gibson, C.L.; Nia, A.B.; Spriggs, S.A.; DeFrancisco, D.; Swift, A.; Perkel, C.; Hurd, Y.L. Cannabinoid use in psychotic patients impacts inflammatory levels and their association with psychosis severity. Psychiatry Res. 2020, 293, 113380. [Google Scholar] [CrossRef] [PubMed]
- Miller, B.J.; Buckley, P.F.; McEvoy, J.P. Inflammation, substance use, psychopathology, and cognition in phase 1 of the clinical antipsychotic trials of intervention effectiveness study. Schizophr. Res. 2018, 195, 275–282. [Google Scholar] [CrossRef]
- Romeo, B.; Lestra, V.; Martelli, C.; Benyamina, A.; Hamdani, N. Cannabis Cessation, Inflammatory Markers and Schizophrenia. J. Dual Diagn. 2022, 18, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Goetz, R.L.; Miller, B.J. Total and Differential White Blood Cell Counts, Cocaine, and Marijuana Use in Patients With Schizophrenia. J. Nerv. Ment. Dis. 2019, 207, 633–636. [Google Scholar] [CrossRef]
- Romeo, B.; Lestra, V.; Martelli, C.; Amirouche, A.; Benyamina, A.; Hamdani, N. Increased markers of inflammation after cannabis cessation and their association with psychotic symptoms. Acta Neuropsychiatr. 2023, 1–10. [Google Scholar] [CrossRef]
- Corsi-Zuelli, F.; Marques, L.; da Roza, D.L.; Loureiro, C.M.; Shuhama, R.; Di Forti, M.; Del-Ben, C.M. The independent and combined effects of cannabis use and systemic inflammation during the early stages of psychosis: Exploring the two-hit hypothesis. Psychol. Med. 2022, 52, 3874–3884. [Google Scholar] [CrossRef]
- Long, H.; Liao, W.; Wang, L.; Lu, Q. A Player and Coordinator: The Versatile Roles of Eosinophils in the Immune System. Transfus. Med. Hemotherapy 2016, 43, 96–108. [Google Scholar] [CrossRef]
- Çekici, Y.; Yılmaz, M.; Seçen, Ö. New inflammatory indicators: Association of high eosinophil-to-lymphocyte ratio and low lymphocyte-to-monocyte ratio with smoking. J. Int. Med. Res. 2019, 47, 4292–4303. [Google Scholar] [CrossRef] [PubMed]
- Holub, K.; Biete, A. New pre-treatment eosinophil-related ratios as prognostic biomarkers for survival outcomes in endometrial cancer. BMC Cancer 2018, 18, 1280. [Google Scholar] [CrossRef] [PubMed]
- Dirani, E.; Bou Khalil, R.; Raad, G.; Richa, S. Eosinophils to Lymphocytes Ratio (ELR) as a Potential Inflammatory Biomarker in Patients with Dual Diagnosis of Bipolar and Alcohol Use Disorders: A Retrospective Cohort Study. J. Dual Diagn. 2022, 18, 144–152. [Google Scholar] [CrossRef]
- Kuang, F.L. Approach to Patients with Eosinophilia. Med. Clin. N. Am. 2020, 104, 1–14. [Google Scholar] [CrossRef]
- Kay, S.R.; Fiszbein, A.; Opler, L.A. The Positive and Negative Syndrome Scale (PANSS) for Schizophrenia. Schizophr. Bull. 1987, 13, 261–276. [Google Scholar] [CrossRef] [PubMed]
- Petersen, E.; Borobio, M.V.; Guy, E.; Liesenfeld, O.; Meroni, V.; Naessens, A.; Thulliez, P. European Multicenter Study of the LIAISON Automated Diagnostic System for Determination of Toxoplasma gondii-Specific Immunoglobulin G (IgG) and IgM and the IgG Avidity Index. J. Clin. Microbiol. 2005, 43, 1570–1574. [Google Scholar] [CrossRef]
- Silver, J.S.; Stumhofer, J.S.; Passos, S.; Ernst, M.; Hunter, C.A. IL-6 Mediates the Susceptibility of Glycoprotein 130 Hypermorphs to Toxoplasma gondii. J. Immunol. 2011, 187, 350–360. [Google Scholar] [CrossRef] [PubMed]
- Aceves, S.S.; Ackerman, S.J. Relationships Between Eosinophilic Inflammation, Tissue Remodeling, and Fibrosis in Eosinophilic Esophagitis. Immunol. Allergy Clin. North. Am. 2009, 29, 197–211. [Google Scholar] [CrossRef]
- Fabiani, S.; Pinto, B.; Bonuccelli, U.; Bruschi, F. Neurobiological studies on the relationship between toxoplasmosis and neuropsychiatric diseases. J. Neurol. Sci. 2015, 351, 3–8. [Google Scholar] [CrossRef]
- Melamede, R. Parasitic brain infection, endocannabinoids, and schizophrenia. Med. Hypotheses 2009, 72, 220–222. [Google Scholar] [CrossRef]
- De Marchi, N.; De Petrocellis, L.; Orlando, P.; Daniele, F.; Fezza, F.; Di Marzo, V. Endocannabinoid signalling in the blood of patients with schizophrenia. Lipids Health Dis. 2003, 2, 5. [Google Scholar] [CrossRef]
- Lestra, V.; Romeo, B.; Martelli, C.; Benyamina, A.; Hamdani, N. Could CRP be a differential biomarker of illness stages in schizophrenia? A systematic review and meta-analysis. Schizophr. Res. 2022, 246, 175–186. [Google Scholar] [CrossRef] [PubMed]
- Eljaschewitsch, E.; Witting, A.; Mawrin, C.; Lee, T.; Schmidt, P.M.; Wolf, S.; Ullrich, O. The Endocannabinoid Anandamide Protects Neurons during CNS Inflammation by Induction of MKP-1 in Microglial Cells. Neuron 2006, 49, 67–79. [Google Scholar] [CrossRef] [PubMed]
- Esshili, A.; Thabet, S.; Jemli, A.; Trifa, F.; Mechri, A.; Zaafrane, F.; Jrad, B.B.H. Toxoplasma gondii infection in schizophrenia and associated clinical features. Psychiatry Res. 2016, 245, 327–332. [Google Scholar] [CrossRef]
- Goldsmith, D.R.; Rapaport, M.H. Inflammation and Negative Symptoms of Schizophrenia: Implications for Reward Processing and Motivational Deficits. Front. Psychiatry 2020, 11, 46. [Google Scholar] [CrossRef]
- Hunt, G.E.; Large, M.M.; Cleary, M.; Lai, H.M.X.; Saunders, J.B. Prevalence of comorbid substance use in schizophrenia spectrum disorders in community and clinical settings, 1990–2017: Systematic review and meta-analysis. Drug Alcohol Depend 2018, 191, 234–258. [Google Scholar] [CrossRef] [PubMed]
- Hunt, G.E.; Malhi, G.S.; Lai, H.M.X.; Cleary, M. Prevalence of comorbid substance use in major depressive disorder in community and clinical settings, 1990–2019: Systematic review and meta-analysis. J. Affect. Disord. 2020, 266, 288–304. [Google Scholar] [CrossRef]
- Hunt, G.E.; Malhi, G.S.; Cleary, M.; Lai, H.M.X.; Sitharthan, T. Prevalence of comorbid bipolar and substance use disorders in clinical settings, 1990–2015: Systematic review and meta-analysis. J. Affect. Disord. 2016, 206, 331–349. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Toxo− (n = 106) | Toxo+ (n = 82) | p | ||
|---|---|---|---|---|
| Age (years) | 31.3 (11.2) | 45 (14.7) | <0.01 | |
| Gender F (%) | 55 (51.9) | 34 (41.5) | 0.16 | |
| BMI (kg/m2) | 23.7 (5.2) | 24.1 (4.8) | 0.46 | |
| Diagnosis (%) | Schizophrenia | 30 (28.3) | 32 (39) | 0.18 |
| Schizo-affective disorder | 10 (9.4) | 13 (15.9) | ||
| FEP | 13 (12.3) | 6 (7.3) | ||
| Bipolar Disorder | 19 (17.9) | 13 (15.9) | ||
| MDD with psychotic symptoms | 5 (4.7) | 4 (4.9) | ||
| MDD without psychotic symptoms | 20 (18.9) | 14 (17.1) | ||
| Other Psychotic disorder | 2 (1.9) | 0 (0) | ||
| Anxiety disorder | 1 (0.9) | 0 (0) | ||
| Personality disorder | 6 (5.7) | 0 (0) | ||
| Medication at Baseline (%) | Drug-free | 63 (59.4) | 44 (53.7) | 0.43 |
| Drug-Naïve | 36 (34) | 17 (20.7) | 0.05 | |
| AP | 27 (25.5) | 26 (31.7) | 0.35 | |
| AD | 24 (22.6) | 14 (17.1) | 0.35 | |
| MS | 7 (6.6) | 15 (18.3) | 0.01 | |
| Anxiolytic | 14 (13.2) | 16 (19.5) | 0.24 | |
| PANSS score * | Total | 84.8 (21.2) | 87.2 (21.3) | 0.52 |
| Positive | 24 (8.7) | 24.9 (10.3) | 0.78 | |
| Negative | 18.5 (8.7) | 19.3 (8.8) | 0.60 | |
| General | 42.3 (9.4) | 43 (9.5) | 0.69 | |
| Smoking status (%) | 45 (43.7) | 51 (63.7) | <0.01 | |
| Cannabis status (%) | 26 (24.5) | 22 (26.8) | 0.72 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romeo, B.; Lestra, V.; Martelli, C.; Amirouche, A.; Benyamina, A.; Hamdani, N. The Modulated Role of Toxoplasma gondii on Eosinophils in Psychiatric Disorders after Cannabis Cessation. Pathogens 2023, 12, 1333. https://doi.org/10.3390/pathogens12111333
Romeo B, Lestra V, Martelli C, Amirouche A, Benyamina A, Hamdani N. The Modulated Role of Toxoplasma gondii on Eosinophils in Psychiatric Disorders after Cannabis Cessation. Pathogens. 2023; 12(11):1333. https://doi.org/10.3390/pathogens12111333
Chicago/Turabian StyleRomeo, Bruno, Valentine Lestra, Catherine Martelli, Ammar Amirouche, Amine Benyamina, and Nora Hamdani. 2023. "The Modulated Role of Toxoplasma gondii on Eosinophils in Psychiatric Disorders after Cannabis Cessation" Pathogens 12, no. 11: 1333. https://doi.org/10.3390/pathogens12111333
APA StyleRomeo, B., Lestra, V., Martelli, C., Amirouche, A., Benyamina, A., & Hamdani, N. (2023). The Modulated Role of Toxoplasma gondii on Eosinophils in Psychiatric Disorders after Cannabis Cessation. Pathogens, 12(11), 1333. https://doi.org/10.3390/pathogens12111333