
Pneumocystis jirovecii Pneumonia after Heart Transplantation: Two Case Reports and a Review of the Literature

 ,
,  ,
, 
Abstract
:1. Introduction
2. Clinical Cases
2.1. First Case
2.2. Second Case
3. Epidemiology of PcP
3.1. Incidence of PcP
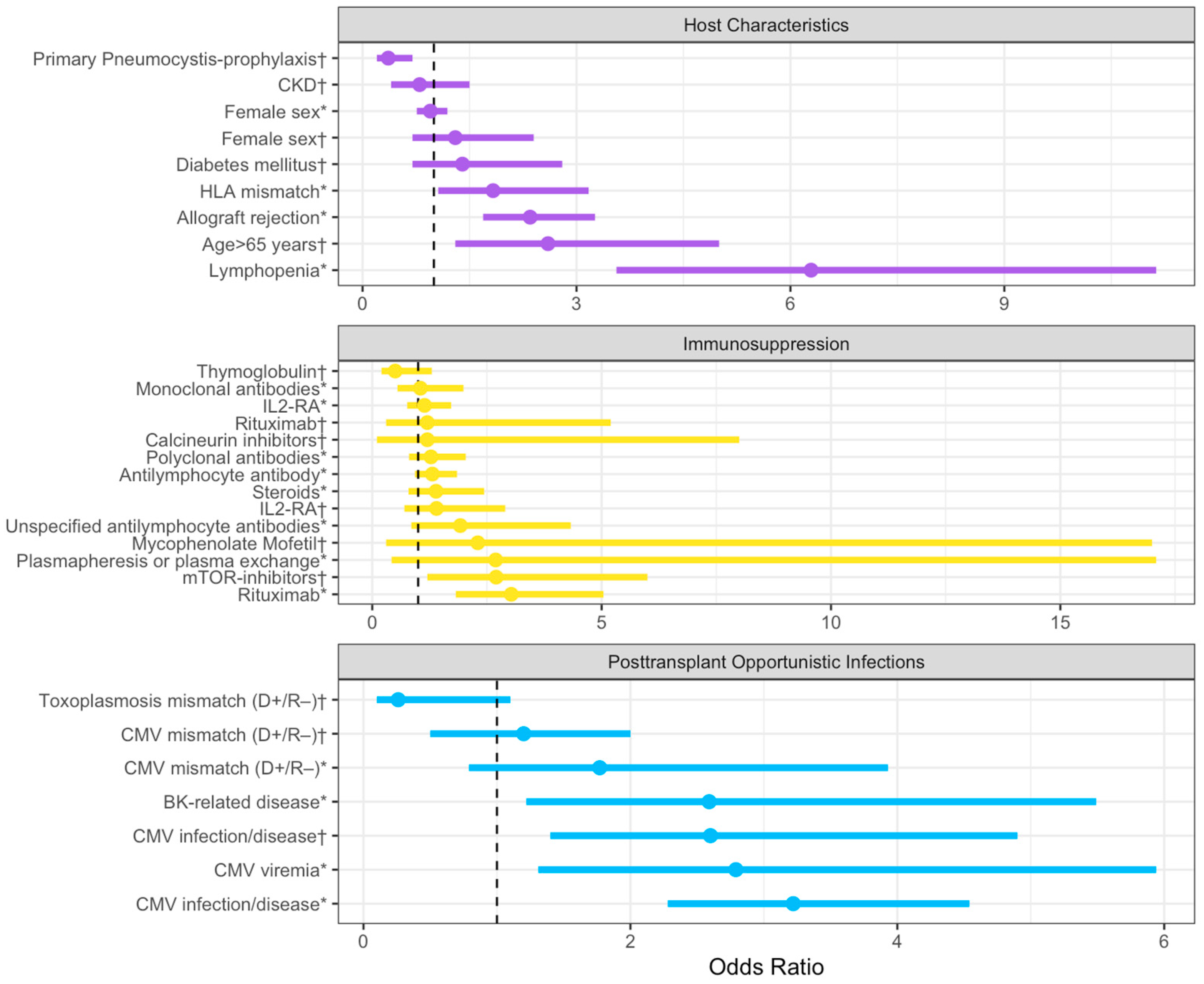
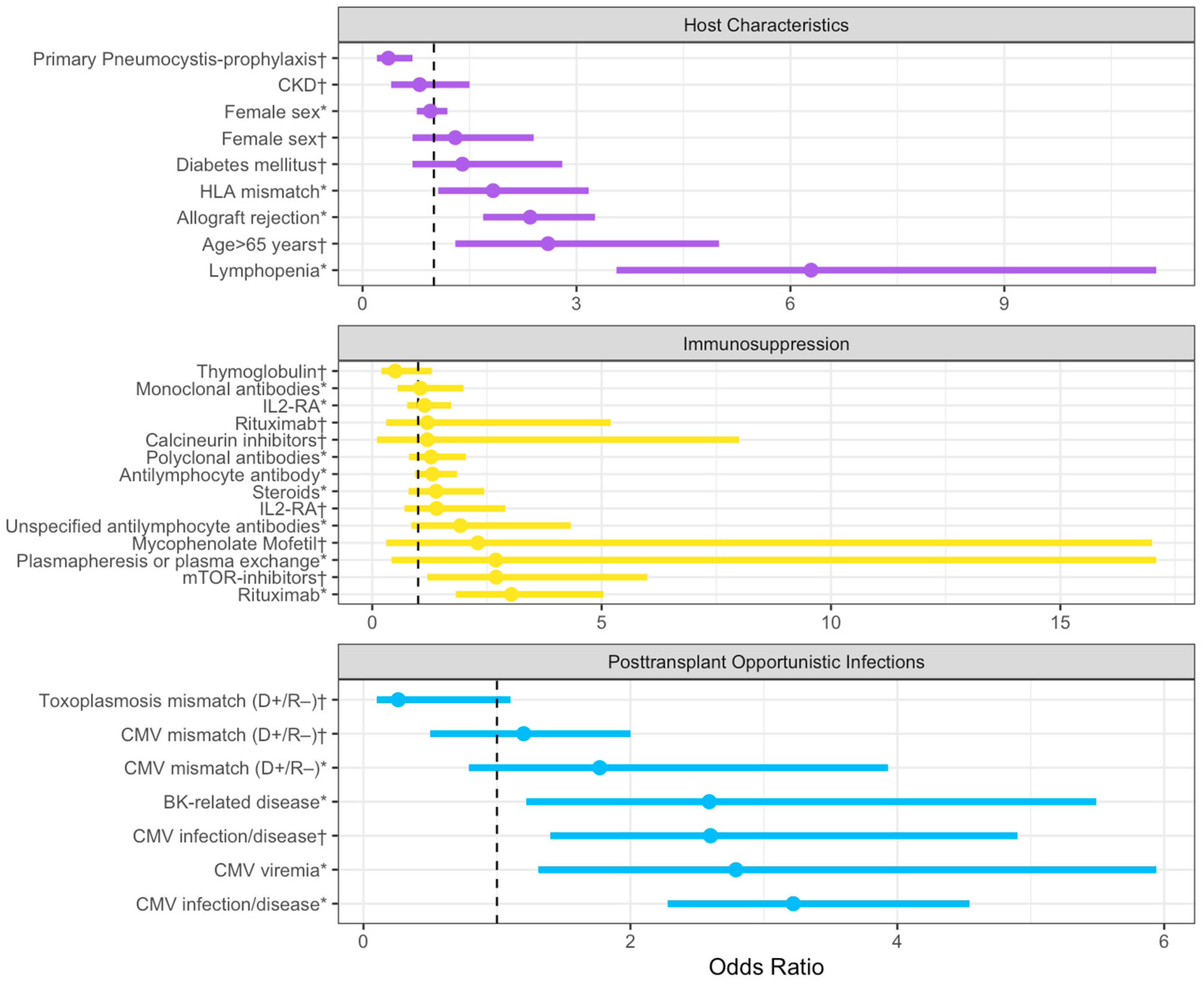
3.2. Risk Factors for PcP in HT Recipients
3.3. Viral Infection as Risk Factor for PcP
3.4. Immunosuppressive Therapies as Risk Factor for PcP
3.5. PcP Prophylaxis: State of the Art
4. Clinical Features of PcP
4.1. Clinical Manifestation and Diagnosis of PcP
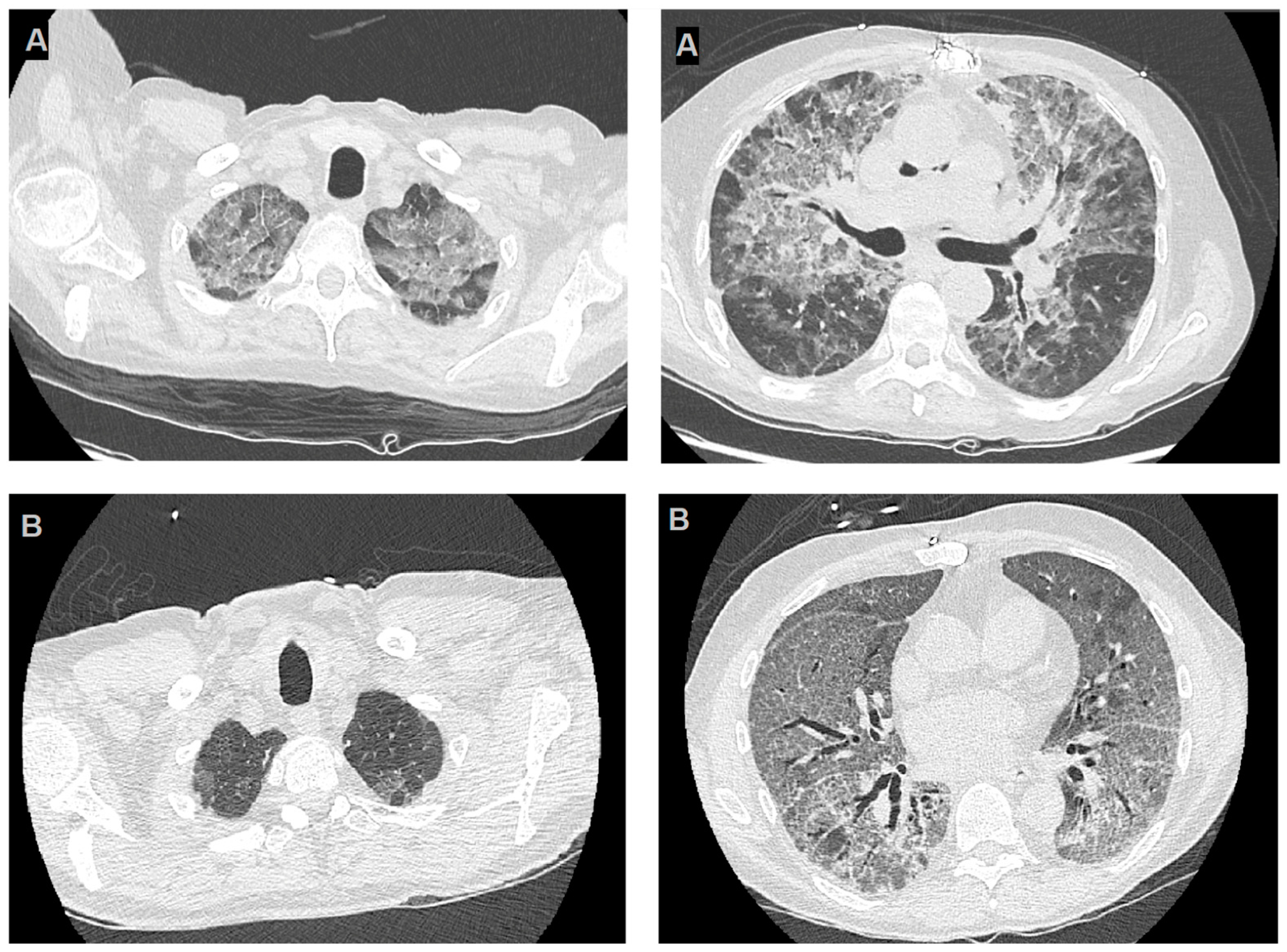
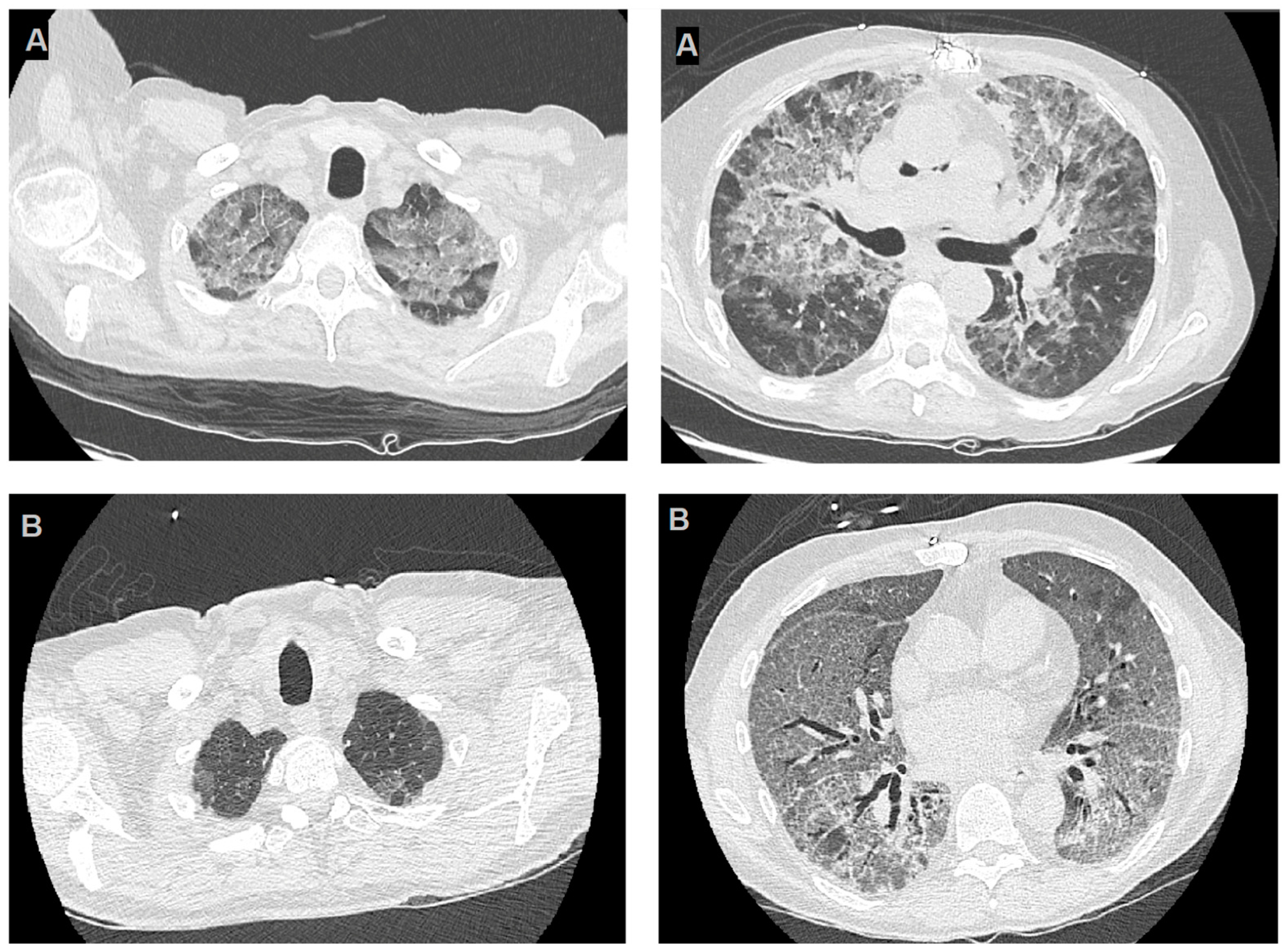
4.2. Imaging of PcP
4.3. Laboratory Testing
4.4. Microbiological Diagnosis and Diagnostic Approach of PcP in HT Recipients
4.5. Therapeutic Approach
5. Conclusions and Future Perspectives
Author Contributions
Funding
Conflicts of Interest
References
- Timsit, J.-F.; Sonneville, R.; Kalil, A.C.; Bassetti, M.; Ferrer, R.; Jaber, S.; Lanternier, F.; Luyt, C.-E.; Machado, F.; Mikulska, M.; et al. Diagnostic and Therapeutic Approach to Infectious Diseases in Solid Organ Transplant Recipients. Intensive Care Med. 2019, 45, 573–591. [Google Scholar] [CrossRef]
- Poole, D.; Skurzak, S.; Mehra, M.R. Prediction of Optimal Outcomes in Organ Transplantation. Intensive Care Med. 2019, 45, 367–370. [Google Scholar] [CrossRef]
- Grossi, P.; Farina, C.; Fiocchi, R.; Dalla Gasperina, D. Prevalence and Outcome of Invasive Fungal Infections in 1,963 Thoracic Organ Transplant Recipients: A Multicenter Retrospective Study. Italian Study Group of Fungal Infections in Thoracic Organ Transplant Recipients. Transplantation 2000, 70, 112–116. [Google Scholar]
- Iriart, X.; Challan Belval, T.; Fillaux, J.; Esposito, L.; Lavergne, R.-A.; Cardeau-Desangles, I.; Roques, O.; Del Bello, A.; Cointault, O.; Lavayssière, L.; et al. Risk Factors of Pneumocystis Pneumonia in Solid Organ Recipients in the Era of the Common Use of Posttransplantation Prophylaxis. Am. J. Transplant. 2015, 15, 190–199. [Google Scholar] [CrossRef] [PubMed]
- Nevez, G.; Totet, A.; Matos, O.; Calderon, E.J.; Miller, R.F.; Le Gal, S. It Is Still PCP That Can Stand for Pneumocystis Pneumonia: Appeal for Generalized Use of Only One Acronym. Med. Mycol. 2021, 59, 842–844. [Google Scholar] [CrossRef]
- Neofytos, D.; Hirzel, C.; Boely, E.; Lecompte, T.; Khanna, N.; Mueller, N.J.; Boggian, K.; Cusini, A.; Manuel, O.; Van Delden, C.; et al. Pneumocystis Jirovecii Pneumonia in Solid Organ Transplant Recipients: A Descriptive Analysis for the Swiss Transplant Cohort. Transpl. Infect. Dis. 2018, 20, e12984. [Google Scholar] [CrossRef]
- Neofytos, D.; Fishman, J.A.; Horn, D.; Anaissie, E.; Chang, C.-H.; Olyaei, A.; Pfaller, M.; Steinbach, W.J.; Webster, K.M.; Marr, K.A. Epidemiology and Outcome of Invasive Fungal Infections in Solid Organ Transplant Recipients: Invasive Fungal Infections in SOT. Transpl. Infect. Dis. 2010, 12, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Hosseini-Moghaddam, S.M.; Shokoohi, M.; Singh, G.; Dufresne, S.F.; Boucher, A.; Jevnikar, A.; Prasad, G.V.R.; Shoker, A.; Kabbani, D.; Hebert, M.J.; et al. A Multicenter Case-Control Study of the Effect of Acute Rejection and Cytomegalovirus Infection on Pneumocystis Pneumonia in Solid Organ Transplant Recipients. Clin. Infect. Dis. 2019, 68, 1320–1326. [Google Scholar] [CrossRef]
- Lee, H.-Y.; Choi, S.-H.; Kim, T.; Chang, J.; Kim, S.-H.; Lee, S.O.; Kim, M.-N.; Sung, H. Epidemiologic Trends and Clinical Features of Pneumocystis Jirovecii Pneumonia in Non-HIV Patients in a Tertiary-Care Hospital in Korea over a 15-Year-Period. Jpn. J. Infect. Dis. 2019, 72, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Wang, E.H.Z.; Partovi, N.; Levy, R.D.; Shapiro, R.J.; Yoshida, E.M.; Greanya, E.D. Pneumocystis Pneumonia in Solid Organ Transplant Recipients: Not yet an Infection of the Past. Transpl. Infect. Dis. 2012, 14, 519–525. [Google Scholar] [CrossRef]
- Cheng, Y.-D.; Huang, C.-H.; Gau, S.-Y.; Chung, N.-J.; Huang, S.-W.; Huang, C.-Y.; Lee, C.-Y. Risk of Pneumocystis Jirovecii Pneumonia among Solid Organ Transplant Recipients: A Population-Based Study. J. Fungi 2022, 9, 23. [Google Scholar] [CrossRef]
- Permpalung, N.; Kittipibul, V.; Mekraksakit, P.; Rattanawong, P.; Nematollahi, S.; Zhang, S.X.; Steinke, S.M. A Comprehensive Evaluation of Risk Factors for Pneumocystis Jirovecii Pneumonia in Adult Solid Organ Transplant Recipients: A Systematic Review and Meta-Analysis. Transplantation 2021, 105, 2291–2306. [Google Scholar] [CrossRef]
- Nunes, J.; Issa, N.; Dupuis, A.; Accoceberry, I.; Pedeboscq, S. Pneumocystis in the Era of Prophylaxis: Do the Guidelines Have to Change? Infection 2022, 50, 995–1000. [Google Scholar] [CrossRef]
- Korkmaz Ekren, P.; Töreyin, Z.N.; Nahid, P.; Doskaya, M.; Caner, A.; Turgay, N.; Zeytinoglu, A.; Toz, S.; Bacakoglu, F.; Guruz, Y.; et al. The Association between Cytomegalovirus Co-infection with Pneumocystis Pneumonia and Mortality in Immunocompromised non-HIV Patients. Clin. Respir. J. 2018, 12, 2590–2597. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Chen, J.; Dong, L. Supplementary Role of Immunological Indicators in the Diagnosis and Prognosis of Pneumocystis Pneumonia in Non-HIV Immunocompromised Patients. Infect. Drug Resist. 2022, 15, 4675–4683. [Google Scholar] [CrossRef]
- Duan, J.; Gao, J.; Liu, Q.; Sun, M.; Liu, Y.; Tan, Y.; Xing, L. Characteristics and Prognostic Factors of Non-HIV Immunocompromised Patients with Pneumocystis Pneumonia Diagnosed by Metagenomics Next-Generation Sequencing. Front. Med. 2022, 9, 812698. [Google Scholar] [CrossRef]
- Yu, Q.; Jia, P.; Su, L.; Zhao, H.; Que, C. Outcomes and Prognostic Factors of Non-HIV Patients with Pneumocystis Jirovecii Pneumonia and Pulmonary CMV Co-Infection: A Retrospective Cohort Study. BMC Infect. Dis. 2017, 17, 392. [Google Scholar] [CrossRef]
- Chong, W.H.; Saha, B.K.; Ananthakrishnan, R.; Chopra, A. State-of-the-Art Review of Secondary Pulmonary Infections in Patients with COVID-19 Pneumonia. Infection 2021, 49, 591–605. [Google Scholar] [CrossRef] [PubMed]
- Bhat, P.; Noval, M.; Doub, J.B.; Heil, E. Concurrent COVID-19 and Pneumocystis Jirovecii Pneumonia in a Severely Immunocompromised 25-Year-Old Patient. Int. J. Infect. Dis. 2020, 99, 119–121. [Google Scholar] [CrossRef] [PubMed]
- Merchant, E.A.; Flint, K.; Barouch, D.H.; Blair, B.M. Co-Infection with Coronavirus Disease 2019, Previously Undiagnosed Human Immunodeficiency Virus, Pneumocystis Jirovecii Pneumonia and Cytomegalovirus Pneumonitis, with Possible Immune Reconstitution Inflammatory Syndrome. IDCases 2021, 24, e01153. [Google Scholar] [CrossRef] [PubMed]
- Peng, J.; Ni, M.; Du, D.; Lu, Y.; Song, J.; Liu, W.; Shen, N.; Wang, X.; Zhu, Y.; Vallance, B.A.; et al. Successful Treatment of a Kidney Transplant Patient with COVID-19 and Late-Onset Pneumocystis Jirovecii Pneumonia. Ann. Clin. Microbiol. Antimicrob. 2021, 20, 83. [Google Scholar] [CrossRef] [PubMed]
- Viceconte, G.; Buonomo, A.R.; Lanzardo, A.; Pinchera, B.; Zappulo, E.; Scotto, R.; Schiano Moriello, N.; Vargas, M.; Iacovazzo, C.; Servillo, G.; et al. Pneumocystis Jirovecii Pneumonia in an Immunocompetent Patient Recovered from COVID-19. Infect. Dis. 2021, 53, 382–385. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Saito, A.; Kuronuma, K.; Nishikiori, H.; Chiba, H. Pneumocystis Jirovecii Pneumonia Associated with COVID-19 in Patients with Interstitial Pneumonia. Medicina 2022, 58, 1151. [Google Scholar] [CrossRef] [PubMed]
- Gentile, I.; Viceconte, G.; Lanzardo, A.; Zotta, I.; Zappulo, E.; Pinchera, B.; Scotto, R.; Schiano Moriello, N.; Foggia, M.; Giaccone, A.; et al. Pneumocystis Jirovecii Pneumonia in Non-HIV Patients Recovering from COVID-19: A Single-Center Experience. Int. J. Environ. Res. Public Health 2021, 18, 11399. [Google Scholar] [CrossRef]
- Chong, W.H.; Saha, B.K.; Chopra, A. Narrative Review of the Relationship between COVID-19 and PJP: Does It Represent Coinfection or Colonization? Infection 2021, 49, 1079–1090. [Google Scholar] [CrossRef]
- Franconi, I.; Monari, C.; Tutone, M.; Ciusa, G.; Corradi, L.; Franceschini, E.; Meschiari, M.; Puzzolante, C.; Gennari, W.; Pecorari, M.; et al. Pneumocystosis as a Complication of H1N1 Influenza a Infection in an HIV-Positive Patient on Effective cART. Open Forum Infect. Dis. 2019, 6, ofz105. [Google Scholar] [CrossRef]
- Pulcini, C.; Hasseine, L.; Mondain, V.; Baudin, G.; Roger, P.-M. Possible Pandemic HIN1 Influenza Complicated by Pneumocystis Jirovecii Pneumonia in an HIV-Infected Patient. J. Mycol. Méd. 2012, 22, 88–91. [Google Scholar] [CrossRef]
- Burke, J.; Soubani, A.O. Influenza and Pneumocystis Jirovecii Pneumonia in an Allogeneic Hematopoietic Stem Cell Transplantation Recipient: Coinfection or Superinfection? Transpl. Infect. Dis. 2018, 20, e12802. [Google Scholar] [CrossRef]
- Van Kampen, J.J.A.; Bielefeld-Buss, A.J.; Ott, A.; Maaskant, J.; Faber, H.J.; Lutisan, J.G.; Boucher, C.A.B. Case Report: Oseltamivir-Induced Resistant Pandemic Influenza A (H1N1) Virus Infection in a Patient with AIDS and Pneumocystis Jirovecii Pneumonia. J. Med. Virol. 2013, 85, 941–943. [Google Scholar] [CrossRef]
- Muramatsu, H.; Kuriyama, A.; Anzai, Y.; Ikegami, T. A Co-Infection of Varicella-Zoster Virus and Pneumocystis Jirovecii in a Non-HIV Immunocompromised Patient: A Case Report. BMC Infect. Dis. 2019, 19, 1092. [Google Scholar] [CrossRef]
- Qi, Z.; Sun, Y.; Li, J.; Wang, Y.; Lu, H.; Wang, X.; Li, Z. Severe Pulmonary Co-Infection with Varicella-Zoster Virus, Pneumocystis Jirovecii and Cytomegalovirus: A Case Report. J. Int. Med. Res. 2022, 50, 030006052110707. [Google Scholar] [CrossRef]
- Fillatre, P.; Chevrier, S.; Revest, M.; Gacouin, A.; Jouneau, S.; Leroy, H.; Robert-Gangneux, F.; Minjolle, S.; Tulzo, Y.; Tattevin, P. Human Herpes Virus Co-Infection Is Associated with Mortality in HIV-Negative Patients with Pneumocystis Jirovecii Pneumonia. Eur. J. Clin. Microbiol. Infect. Dis. 2013, 32, 189–194. [Google Scholar] [CrossRef]
- Salazar, F.; Bignell, E.; Brown, G.D.; Cook, P.C.; Warris, A. Pathogenesis of Respiratory Viral and Fungal Coinfections. Clin. Microbiol. Rev. 2022, 35, e00094-21. [Google Scholar] [CrossRef] [PubMed]
- Pan, L.; Wu, F.; Cai, Q.; Xu, Z.; Hu, H.; Tang, T.; Yue, R.; Hou, Y.; Zhang, X.; Fang, Y.; et al. Whole Genome Profiling of Lung Microbiome in Solid Organ Transplant Recipients Reveals Virus Involved Microecology May Worsen Prognosis. Front. Cell. Infect. Microbiol. 2022, 12, 863399. [Google Scholar] [CrossRef] [PubMed]
- Malpica, L.; Moll, S. Practical Approach to Monitoring and Prevention of Infectious Complications Associated with Systemic Corticosteroids, Antimetabolites, Cyclosporine, and Cyclophosphamide in Nonmalignant Hematologic Diseases. Hematology 2020, 2020, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Ghembaza, A.; Vautier, M.; Cacoub, P.; Pourcher, V.; Saadoun, D. Risk Factors and Prevention of Pneumocystis Jirovecii Pneumonia in Patients with Autoimmune and Inflammatory Diseases. Chest 2020, 158, 2323–2332. [Google Scholar] [CrossRef] [PubMed]
- Pike-Lee, T.; Syed, S.; Willis, M.A.; Li, Y. Pneumocystis Jirovecii Pneumonia in Neurologic Disorders: Is Prophylaxis Necessary? Neurol. Clin. Pract. 2021, 11, 242–248. [Google Scholar] [CrossRef]
- Sierra, C.M.; Daiya, K.C. Prophylaxis for Pneumocystis Jirovecii Pneumonia in Patients with Inflammatory Bowel Disease: A Systematic Review. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2022, 42, 858–867. [Google Scholar] [CrossRef]
- Chew, L.-C.; Maceda-Galang, L.M.; Tan, Y.K.; Chakraborty, B.; Thumboo, J. Pneumocystis Jirovecii Pneumonia in Patients with Autoimmune Disease on High-Dose Glucocorticoid. JCR J. Clin. Rheumatol. 2015, 21, 72–75. [Google Scholar] [CrossRef]
- Park, J.W.; Curtis, J.R.; Kim, M.J.; Lee, H.; Song, Y.W.; Lee, E.B. Pneumocystis Pneumonia in Patients with Rheumatic Diseases Receiving Prolonged, Non-High-Dose Steroids—Clinical Implication of Primary Prophylaxis Using Trimethoprim–Sulfamethoxazole. Arthritis Res. Ther. 2019, 21, 207. [Google Scholar] [CrossRef]
- Zhang, Y.; Zheng, Y. Pneumocystis Jirovecii Pneumonia in Mycophenolate Mofetil-Treated Patients with Connective Tissue Disease: Analysis of 17 Cases. Rheumatol. Int. 2014, 34, 1765–1771. [Google Scholar] [CrossRef]
- Neff, R.T.; Jindal, R.M.; Yoo, D.Y.; Hurst, F.P.; Agodoa, L.Y.; Abbott, K.C. Analysis of USRDS: Incidence and Risk Factors for Pneumocystis Jiroveci Pneumonia. Transplantation 2009, 88, 135–141. [Google Scholar] [CrossRef]
- Zalmanovich, A.; Ben-Ami, R.; Rahav, G.; Alon, D.; Moses, A.; Olshtain-Pops, K.; Weinberger, M.; Shitrit, P.; Katzir, M.; Gottesman, B.-S.; et al. Rituximab Identified as an Independent Risk Factor for Severe PJP: A Case-Control Study. PLoS ONE 2020, 15, e0239042. [Google Scholar] [CrossRef]
- Park, J.W.; Curtis, J.R.; Jun, K.I.; Kim, T.M.; Heo, D.S.; Ha, J.; Suh, K.-S.; Lee, K.-W.; Lee, H.; Yang, J.; et al. Primary Prophylaxis for Pneumocystis Jirovecii Pneumonia in Patients Receiving Rituximab. Chest 2022, 161, 1201–1210. [Google Scholar] [CrossRef]
- Yetmar, Z.A.; Duffy, D.; Smith, B.H.; Vikram, H.R.; Brumble, L.; Limper, A.H.; Beam, E. Risk Factors and Outcomes of Pneumocystis Pneumonia in Solid Organ Transplant Recipients: Impact of Posttransplant Lymphoproliferative Disorder. Clin. Transplant. 2023, 37, e15021. [Google Scholar] [CrossRef]
- Velleca, A.; Shullo, M.A.; Dhital, K.; Azeka, E.; Colvin, M.; DePasquale, E.; Farrero, M.; García-Guereta, L.; Jamero, G.; Khush, K.; et al. The International Society for Heart and Lung Transplantation (ISHLT) Guidelines for the Care of Heart Transplant Recipients. J. Heart Lung Transplant. 2023, 42, e1–e141. [Google Scholar] [CrossRef]
- Fishman, J.A.; Gans, H.; The AST Infectious Diseases Community of Practice. Pneumocystis Jiroveci in Solid Organ Transplantation: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13587. [Google Scholar] [CrossRef] [PubMed]
- Aggoun, D.; Bleibtreu, A.; Desiré, E.; Lecuyer, L.; Leprince, P.; Varnous, S.; Coutance, G.; Lescroart, M.; The PNC HTX STUDY GROUP. Pneumocystis Prophylaxis in French Heart Transplant Centers: A Nationwide Survey. Transpl. Infect. Dis. 2023, 25, e14053. [Google Scholar] [CrossRef]
- Fillatre, P.; Decaux, O.; Jouneau, S.; Revest, M.; Gacouin, A.; Robert-Gangneux, F.; Fresnel, A.; Guiguen, C.; Le Tulzo, Y.; Jégo, P.; et al. Incidence of Pneumocystis Jiroveci Pneumonia among Groups at Risk in HIV-Negative Patients. Am. J. Med. 2014, 127, 1242.e11–1242.e17. [Google Scholar] [CrossRef] [PubMed]
- Goto, N.; Takahashi-Nakazato, A.; Futamura, K.; Okada, M.; Yamamoto, T.; Tsujita, M.; Hiramitsu, T.; Narumi, S.; Tsuchiya, K.; Gatanaga, H.; et al. Lifelong Prophylaxis with Trimethoprim-Sulfamethoxazole for Prevention of Outbreak of Pneumocystis Jirovecii Pneumonia in Kidney Transplant Recipients. Transplant. Direct 2017, 3, e151. [Google Scholar] [CrossRef] [PubMed]
- Apostolopoulou, A.; Fishman, J.A. The Pathogenesis and Diagnosis of Pneumocystis Jiroveci Pneumonia. J. Fungi 2022, 8, 1167. [Google Scholar] [CrossRef]
- McKinnell, J.A.; Cannella, A.P.; Kunz, D.F.; Hook Rd, E.W.; Moser, S.A.; Miller, L.G.; Baddley, J.W.; Pappas, P.G. Pneumocystis Pneumonia in Hospitalized Patients: A Detailed Examination of Symptoms, Management, and Outcomes in Human Immunodeficiency Virus (HIV)-Infected and HIV-Uninfected Persons. Transpl. Infect. Dis. 2012, 14, 510–518. [Google Scholar] [CrossRef]
- Fujii, T.; Iwamoto, A.; Nakamura, T.; Iwamoto, A.; Iwamoto, A.; Iwamoto, A. Pneumocystis Pneumonia in Patients with HIV Infection: Clinical Manifestations, Laboratory Findings, and Radiological Features. J. Infect. Chemother. 2007, 13, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Hsu, J.M.; Hass, A.; Gingras, M.-A.; Chong, J.; Costiniuk, C.; Ezer, N.; Fraser, R.S.; McDonald, E.G.; Lee, T.C. Radiographic Features in Investigated for Pneumocystis Jirovecii Pneumonia: A Nested Case-Control Study. BMC Infect. Dis. 2020, 20, 492. [Google Scholar] [CrossRef]
- Vogel, M.N.; Vatlach, M.; Weissgerber, P.; Goeppert, B.; Claussen, C.D.; Hetzel, J.; Horger, M. HRCT-Features of Pneumocystis Jiroveci Pneumonia and Their Evolution before and after Treatment in Non-HIV Immunocompromised Patients. Eur. J. Radiol. 2012, 81, 1315–1320. [Google Scholar] [CrossRef]
- Cereser, L.; Dallorto, A.; Candoni, A.; Volpetti, S.; Righi, E.; Zuiani, C.; Girometti, R. Pneumocystis Jirovecii Pneumonia at Chest High-Resolution Computed Tomography (HRCT) in Non-HIV Immunocompromised Patients: Spectrum of Findings and Mimickers. Eur. J. Radiol. 2019, 116, 116–127. [Google Scholar] [CrossRef]
- Rego De Figueiredo, I.; Vieira Alves, R.; Drummond Borges, D.; Torres, M.; Lourenço, F.; Antunes, A.M.; Gruner, H.; Panarra, A. Pneumocystosis Pneumonia: A Comparison Study between HIV and Non-HIV Immunocompromised Patients. Pulmonology 2019, 25, 271–274. [Google Scholar] [CrossRef]
- Vogel, M.; Weissgerber, P.; Goeppert, B.; Hetzel, J.; Vatlach, M.; Claussen, C.; Horger, M. Accuracy of Serum LDH Elevation for the Diagnosis of Pneumocystis Jiroveci Pneumonia. Swiss Med. Wkly. 2011, 141, w13184. [Google Scholar] [CrossRef] [PubMed]
- Koo, S.; Bryar, J.M.; Page, J.H.; Baden, L.R.; Marty, F.M. Diagnostic Performance of the (1→3)-β- D -Glucan Assay for Invasive Fungal Disease. Clin. Infect. Dis. 2009, 49, 1650–1659. [Google Scholar] [CrossRef] [PubMed]
- Theel, E.S.; Doern, C.D. Point-Counterpoint: β- D -Glucan Testing Is Important for Diagnosis of Invasive Fungal Infections. J. Clin. Microbiol. 2013, 51, 3478–3483. [Google Scholar] [CrossRef]
- Sax, P.E.; Komarow, L.; Finkelman, M.A.; Grant, P.M.; Andersen, J.; Scully, E.; Powderly, W.G.; Zolopa, A.R.; The AIDS Clinical Trials Group Study A5164 Team Blood. (1->3)- -D-Glucan as a Diagnostic Test for HIV-Related Pneumocystis Jirovecii Pneumonia. Clin. Infect. Dis. 2011, 53, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Corsi-Vasquez, G.; Ostrosky-Zeichner, L.; Pilkington, E.F.; Sax, P.E. Point-Counterpoint: Should Serum β- D -Glucan Testing Be Used for the Diagnosis of Pneumocystis Jirovecii Pneumonia? J. Clin. Microbiol. 2019, 58, e01340-19. [Google Scholar] [CrossRef] [PubMed]
- Son, H.-J.; Sung, H.; Park, S.Y.; Kim, T.; Lee, H.J.; Kim, S.-M.; Chong, Y.P.; Lee, S.-O.; Choi, S.-H.; Kim, Y.S.; et al. Diagnostic Performance of the (1–3)-β-D-Glucan Assay in Patients with Pneumocystis Jirovecii Compared with Those with Candidiasis, Aspergillosis, Mucormycosis, and Tuberculosis, and Healthy Volunteers. PLoS ONE 2017, 12, e0188860. [Google Scholar] [CrossRef] [PubMed]
- Shoham, S.; Dominguez, E.A.; The AST Infectious Diseases Community of Practice. Emerging Fungal Infections in Solid Organ Transplant Recipients: Guidelines of the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13525. [Google Scholar] [CrossRef]
- Kauffman, C.; Miceli, M. Histoplasmosis and Blastomycosis in Solid Organ Transplant Recipients. J. Fungi 2015, 1, 94–106. [Google Scholar] [CrossRef]
- Krishnan, G.; Power, M.; Bariola, J.R.; Dare, R. Comparison of Indirect Fungal Diagnostic Tests in Patients with Proven Histoplasmosis. Open Forum Infect. Dis. 2022, 9, ofac609. [Google Scholar] [CrossRef]
- Nambiar, P.; Cober, E.; Johnson, L.; Brizendine, K.D. Fatal Fusarium Infection Manifesting as Osteomyelitis Following Previous Treatment with Amphotericin B in a Multi-Visceral Transplant: Case Report and Review of Fusarium Infections in Solid Organ Transplantation. Transpl. Infect. Dis. 2018, 20, e12872. [Google Scholar] [CrossRef]
- Carneiro, H.A.; Coleman, J.J.; Restrepo, A.; Mylonakis, E. Fusarium Infection in Lung Transplant Patients: Report of 6 Cases and Review of the Literature. Medicine 2011, 90, 69–80. [Google Scholar] [CrossRef]
- Sal, E.; Stemler, J.; Salmanton-García, J.; Falces-Romero, I.; Kredics, L.; Meyer, E.; Würstl, B.; Lass-Flörl, C.; Racil, Z.; Klimko, N.; et al. Invasive Trichoderma Spp. Infections: Clinical Presentation and Outcome of Cases from the Literature and the FungiScope® Registry. J. Antimicrob. Chemother. 2022, 77, 2850–2858. [Google Scholar] [CrossRef]
- Burzio, C.; Balzani, E.; Montrucchio, G.; Trompeo, A.C.; Corcione, S.; Brazzi, L. Trichoderma Spp.-Related Pneumonia: A Case Report in Heart–Lung Transplantation Recipient and a Systematic Literature Review. J. Fungi 2023, 9, 195. [Google Scholar] [CrossRef]
- Karageorgopoulos, D.E.; Qu, J.-M.; Korbila, I.P.; Zhu, Y.-G.; Vasileiou, V.A.; Falagas, M.E. Accuracy of β -D-Glucan for the Diagnosis of Pneumocystis Jirovecii Pneumonia: A Meta-Analysis. Clin. Microbiol. Infect. 2013, 19, 39–49. [Google Scholar] [CrossRef]
- Del Corpo, O.; Butler-Laporte, G.; Sheppard, D.C.; Cheng, M.P.; McDonald, E.G.; Lee, T.C. Diagnostic Accuracy of Serum (1-3)-β-D-Glucan for Pneumocystis Jirovecii Pneumonia: A Systematic Review and Meta-Analysis. Clin. Microbiol. Infect. 2020, 26, 1137–1143. [Google Scholar] [CrossRef] [PubMed]
- Esteves, F.; Calé, S.S.; Badura, R.; De Boer, M.G.; Maltez, F.; Calderón, E.J.; Van Der Reijden, T.J.; Márquez-Martín, E.; Antunes, F.; Matos, O. Diagnosis of Pneumocystis Pneumonia: Evaluation of Four Serologic Biomarkers. Clin. Microbiol. Infect. 2015, 21, 379.e1–379.e10. [Google Scholar] [CrossRef]
- Bateman, M.; Oladele, R.; Kolls, J.K. Diagnosing Pneumocystis Jirovecii Pneumonia: A Review of Current Methods and Novel Approaches. Med. Mycol. 2020, 58, 1015–1028. [Google Scholar] [CrossRef]
- Mirovsky, P.; Fishman, J.A. An Improved Method for the Prolonged Maintenance of Pneumocystis Carinii In Vitro. J. Infect. Dis. 1993, 167, 1470–1473. [Google Scholar] [CrossRef]
- Schildgen, V.; Mai, S.; Khalfaoui, S.; Lüsebrink, J.; Pieper, M.; Tillmann, R.L.; Brockmann, M.; Schildgen, O. Pneumocystis Jirovecii Can Be Productively Cultured in Differentiated CuFi-8 Airway Cells. mBio 2014, 5, e01186-14. [Google Scholar] [CrossRef] [PubMed]
- Cushion, M.T.; Tisdale-Macioce, N.; Sayson, S.G.; Porollo, A. The Persistent Challenge of Pneumocystis Growth Outside the Mammalian Lung: Past and Future Approaches. Front. Microbiol. 2021, 12, 681474. [Google Scholar] [CrossRef]
- Riebold, D.; Mahnkopf, M.; Wicht, K.; Zubiria-Barrera, C.; Heise, J.; Frank, M.; Misch, D.; Bauer, T.; Stocker, H.; Slevogt, H. Axenic Long-Term Cultivation of Pneumocystis Jirovecii. J. Fungi 2023, 9, 903. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Singh, S.; Mirdha, B.R.; Guleria, R.; Agarwal, S.K.; Mohan, A. Evaluation of Loop-Mediated Isothermal Amplification Assay for the Detection of Pneumocystis Jirovecii in Immunocompromised Patients. Mol. Biol. Int. 2015, 2015, 819091. [Google Scholar] [CrossRef]
- Huber, T.; Serr, A.; Geißdörfer, W.; Hess, C.; Lynker-Aßmus, C.; Von Loewenich, F.D.; Bogdan, C.; Held, J. Evaluation of the Amplex Eazyplex Loop-Mediated Isothermal Amplification Assay for Rapid Diagnosis of Pneumocystis Jirovecii Pneumonia. J. Clin. Microbiol. 2020, 58, e01739-20. [Google Scholar] [CrossRef]
- Scharmann, U.; Kirchhoff, L.; Schmidt, D.; Buer, J.; Steinmann, J.; Rath, P. Evaluation of a Commercial Loop-mediated Isothermal Amplification (LAMP) Assay for Rapid Detection of Pneumocystis Jirovecii. Mycoses 2020, 63, 1107–1114. [Google Scholar] [CrossRef]
- Cruciani, M.; Marcati, P.; Malena, M.; Bosco, O.; Serpelloni, G.; Mengoli, C. Meta-Analysis of Diagnostic Procedures for Pneumocystis Carinii Pneumonia in HIV-1-Infected Patients. Eur. Respir. J. 2002, 20, 982–989. [Google Scholar] [CrossRef]
- Morjaria, S.; Frame, J.; Franco-Garcia, A.; Geyer, A.; Kamboj, M.; Babady, N.E. Clinical Performance of (1,3) Beta-D Glucan for the Diagnosis of Pneumocystis Pneumonia (PCP) in Cancer Patients Tested with PCP Polymerase Chain Reaction. Clin. Infect. Dis. 2019, 69, 1303–1309. [Google Scholar] [CrossRef]
- Damiani, C.; Le Gal, S.; Da Costa, C.; Virmaux, M.; Nevez, G.; Totet, A. Combined Quantification of Pulmonary Pneumocystis Jirovecii DNA and Serum (1→3)-β- D -Glucan for Differential Diagnosis of Pneumocystis Pneumonia and Pneumocystis Colonization. J. Clin. Microbiol. 2013, 51, 3380–3388. [Google Scholar] [CrossRef]
- Matsumura, Y.; Ito, Y.; Iinuma, Y.; Yasuma, K.; Yamamoto, M.; Matsushima, A.; Nagao, M.; Takakura, S.; Ichiyama, S. Quantitative Real-Time PCR and the (1 → 3)-β-d-Glucan Assay for Differentiation between Pneumocystis Jirovecii Pneumonia and Colonization. Clin. Microbiol. Infect. 2012, 18, 591–597. [Google Scholar] [CrossRef] [PubMed]
- Veintimilla, C.; Álvarez-Uría, A.; Martín-Rabadán, P.; Valerio, M.; Machado, M.; Padilla, B.; Alonso, R.; Diez, C.; Muñoz, P.; Marín, M. Pneumocystis Jirovecii Pneumonia Diagnostic Approach: Real-Life Experience in a Tertiary Centre. J. Fungi 2023, 9, 414. [Google Scholar] [CrossRef] [PubMed]
- Lagrou, K.; Chen, S.; Masur, H.; Viscoli, C.; Decker, C.F.; Pagano, L.; Groll, A.H. Pneumocystis Jirovecii Disease: Basis for the Revised EORTC/MSGERC Invasive Fungal Disease Definitions in Individuals Without Human Immunodeficiency Virus. Clin. Infect. Dis. 2021, 72, S114–S120. [Google Scholar] [CrossRef]
- Maschmeyer, G.; Helweg-Larsen, J.; Pagano, L.; Robin, C.; Cordonnier, C.; Schellongowski, P. ECIL Guidelines for Treatment of Pneumocystis Jirovecii Pneumonia in Non-HIV-Infected Haematology Patients. J. Antimicrob. Chemother. 2016, 71, 2405–2413. [Google Scholar] [CrossRef] [PubMed]
- Ice, L.L.; Barreto, J.N.; Dao, B.D.; Wolf, R.C.; Dierkhising, R.A.; Jannetto, P.J.; Langman, L.J.; Tosh, P.K. Relationship of Sulfamethoxazole Therapeutic Drug Monitoring to Clinical Efficacy and Toxicity: A Retrospective Cohort Study. Ther. Drug Monit. 2016, 38, 319–326. [Google Scholar] [CrossRef] [PubMed]
- El-Najjar, N.; Hösl, J.; Holzmann, T.; Jantsch, J.; Gessner, A. UPLC-MS/MS Method for Therapeutic Drug Monitoring of 10 Antibiotics Used in Intensive Care Units. Drug Test. Anal. 2018, 10, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Klinker, H.; Langmann, P.; Zilly, M.; Richter, E. Drug Monitoring during the Treatment of AIDS-Associated Pneumocystis Carinii Pneumonia with Trimethoprim-Sulfamethoxazole. J. Clin. Pharm. Ther. 1998, 23, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Hammarström, H.; Krifors, A.; Athlin, S.; Friman, V.; Golestani, K.; Hällgren, A.; Otto, G.; Oweling, S.; Pauksens, K.; Kinch, A.; et al. Treatment with Reduced-Dose Trimethoprim-Sulfamethoxazole Is Effective in Mild to Moderate Pneumocystis Jirovecii Pneumonia in Patients with Hematologic Malignancies. Clin. Infect. Dis. 2023, 76, e1252–e1260. [Google Scholar] [CrossRef] [PubMed]
- Ohmura, S.; Naniwa, T.; Tamechika, S.; Miyamoto, T.; Shichi, D.; Kazawa, N.; Iwagaitsu, S.; Maeda, S.; Wada, J.; Niimi, A. Effectiveness and Safety of Lower Dose Sulfamethoxazole/Trimethoprim Therapy for Pneumocystis Jirovecii Pneumonia in Patients with Systemic Rheumatic Diseases: A Retrospective Multicenter Study. J. Infect. Chemother. 2019, 25, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Kosaka, M.; Ushiki, A.; Ikuyama, Y.; Hirai, K.; Matsuo, A.; Hachiya, T.; Hanaoka, M. A Four-Center Retrospective Study of the Efficacy and Toxicity of Low-Dose Trimethoprim-Sulfamethoxazole for the Treatment of Pneumocystis Pneumonia in Patients without HIV Infection. Antimicrob. Agents Chemother. 2017, 61, e01173-17. [Google Scholar] [CrossRef] [PubMed]
- Butler-Laporte, G.; Smyth, E.; Amar-Zifkin, A.; Cheng, M.P.; McDonald, E.G.; Lee, T.C. Low-Dose TMP-SMX in the Treatment of Pneumocystis Jirovecii Pneumonia: A Systematic Review and Meta-Analysis. Open Forum Infect. Dis. 2020, 7, ofaa112. [Google Scholar] [CrossRef]
- Haseeb, A.; Abourehab, M.A.S.; Almalki, W.A.; Almontashri, A.M.; Bajawi, S.A.; Aljoaid, A.M.; Alsahabi, B.M.; Algethamy, M.; AlQarni, A.; Iqbal, M.S.; et al. Trimethoprim-Sulfamethoxazole (Bactrim) Dose Optimization in Pneumocystis Jirovecii Pneumonia (PCP) Management: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 2833. [Google Scholar] [CrossRef]
- Sohani, Z.N.; Butler-Laporte, G.; Aw, A.; Belga, S.; Benedetti, A.; Carignan, A.; Cheng, M.P.; Coburn, B.; Costiniuk, C.T.; Ezer, N.; et al. Low-Dose Trimethoprim-Sulfamethoxazole for the Treatment of Pneumocystis Jirovecii Pneumonia (LOW-TMP): Protocol for a Phase III Randomised, Placebo-Controlled, Dose-Comparison Trial. BMJ Open 2022, 12, e053039. [Google Scholar] [CrossRef]
- Creemers-Schild, D.; Kroon, F.P.; Kuijper, E.J.; De Boer, M.G.J. Treatment of Pneumocystis Pneumonia with Intermediate-Dose and Step-down to Low-Dose Trimethoprim–Sulfamethoxazole: Lessons from an Observational Cohort Study. Infection 2016, 44, 291–299. [Google Scholar] [CrossRef]
- Choi, J.S.; Lee, S.H.; Leem, A.Y.; Song, J.H.; Kim, S.Y.; Chung, K.S.; Jung, J.Y.; Kang, Y.A.; Kim, Y.S.; Chang, J.; et al. Pneumocystis Jirovecii Pneumonia (PCP) PCR-Negative Conversion Predicts Prognosis of HIV-Negative Patients with PCP and Acute Respiratory Failure. PLoS ONE 2018, 13, e0206231. [Google Scholar] [CrossRef]
- Kim, T.; Kim, S.-H.; Park, K.-H.; Cho, O.H.; Choi, S.-H.; Jeong, J.-Y.; Woo, J.H.; Kim, Y.S.; Lee, S.-O.; Sung, H.; et al. Clindamycin-Primaquine versus Pentamidine for the Second-Line Treatment of Pneumocystis Pneumonia. J. Infect. Chemother. 2009, 15, 343–346. [Google Scholar] [CrossRef]
- Nickel, P.; Schürmann, M.; Albrecht, H.; Schindler, R.; Budde, K.; Westhoff, T.; Millward, J.; Suttorp, N.; Reinke, P.; Schürmann, D. Clindamycin–Primaquine for Pneumocystis Jiroveci Pneumonia in Renal Transplant Patients. Infection 2014, 42, 981–989. [Google Scholar] [CrossRef]
- Kovacs, J.A. Pneumocystis Carinii Pneumonia: A Comparison Between Patients with the Acquired Immunodeficiency Syndrome and Patients with Other Immunodeficiencies. Ann. Intern. Med. 1984, 100, 663. [Google Scholar] [CrossRef] [PubMed]
- Held, J.; Wagner, D. β-d-Glucan Kinetics for the Assessment of Treatment Response in Pneumocystis Jirovecii Pneumonia. Clin. Microbiol. Infect. 2011, 17, 1118–1122. [Google Scholar] [CrossRef] [PubMed]
- Utili, R.; Durante-Mangoni, E.; Basilico, C.; Mattei, A.; Ragone, E.; Grossi, P. Efficacy of Caspofungin Addition to Trimethoprim-Sulfamethoxazole Treatment for Severe Pneumocystis Pneumonia in Solid Organ Transplant Recipients. Transplantation 2007, 84, 685–688. [Google Scholar] [CrossRef]
- Toma, E.; Thorne, A.; Singer, J.; Raboud, J.; Lemieux, C.; Trottier, S.; Bergeron, M.G.; Tsoukas, C.; Falutz, J.; Lalonde, R.; et al. Clindamycin with Primaquine vs. Trimethoprim-Sulfamethoxazole Therapy for Mild and Moderately Severe Pneumocystis Carinii Pneumonia in Patients with AIDS: A Multicenter, Double-Blind, Randomized Trial (CTN 004). Clin. Infect. Dis. 1998, 27, 524–530. [Google Scholar] [CrossRef]
- Helweg-Larsen, J.; Benfield, T.; Atzori, C.; Miller, R.F. Clinical Efficacy of First- and Second-Line Treatments for HIV-Associated Pneumocystis Jirovecii Pneumonia: A Tri-Centre Cohort Study. J. Antimicrob. Chemother. 2009, 64, 1282–1290. [Google Scholar] [CrossRef] [PubMed]
- Abolghasemi, S.; Sharif-Kashani, B.; Naghashzadeh, F.; Marjani, M.; Moniri, A.; Doroudinia, A.; Tabarsi, P. Caspofungin as Salvage Therapy for Pneumocystis Pneumonia in a Heart Transplant Recipient. Tanaffos 2018, 17, 203–206. [Google Scholar]
- Lobo, M.L.; Esteves, F.; De Sousa, B.; Cardoso, F.; Cushion, M.T.; Antunes, F.; Matos, O. Therapeutic Potential of Caspofungin Combined with Trimethoprim-Sulfamethoxazole for Pneumocystis Pneumonia: A Pilot Study in Mice. PLoS ONE 2013, 8, e70619. [Google Scholar] [CrossRef] [PubMed]
- Qi, H.; Dong, D.; Liu, N.; Xu, Y.; Qi, M.; Gu, Q. Efficacy of Initial Caspofungin plus Trimethoprim/Sulfamethoxazole for Severe PCP in Patients without Human Immunodeficiency Virus Infection. BMC Infect. Dis. 2023, 23, 409. [Google Scholar] [CrossRef]
- Wu, H.-H.; Fang, S.-Y.; Chen, Y.-X.; Feng, L.-F. Treatment of Pneumocystis Jirovecii Pneumonia in Non-Human Immunodeficiency Virus-Infected Patients Using a Combination of Trimethoprim-Sulfamethoxazole and Caspofungin. World J. Clin. Cases 2022, 10, 2743–2750. [Google Scholar] [CrossRef]
- Overgaard, U.M.; Helweg-Larsen, J. Pneumocystis Jiroveci Pneumonia (PCP) in HIV-1-Negative Patients: A Retrospective Study 2002–2004. Scand. J. Infect. Dis. 2007, 39, 589–595. [Google Scholar] [CrossRef]
- Pareja, J.G.; Garland, R.; Koziel, H. Use of Adjunctive Corticosteroids in Severe Adult Non-HIV Pneumocystis Carinii Pneumonia. Chest 1998, 113, 1215–1224. [Google Scholar] [CrossRef] [PubMed]
- Kofteridis, D.P.; Valachis, A.; Velegraki, M.; Antoniou, M.; Christofaki, M.; Vrentzos, G.E.; Andrianaki, A.M.; Samonis, G. Predisposing Factors, Clinical Characteristics and Outcome of Pneumonocystis Jirovecii Pneumonia in HIV-Negative Patients. J. Infect. Chemother. 2014, 20, 412–416. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Denning, D.W. The Impact of Corticosteroids on the Outcome of Fungal Disease: A Systematic Review and Meta-Analysis. Curr. Fungal Infect. Rep. 2023, 17, 54–70. [Google Scholar] [CrossRef]
- Yang, C.-Y.; Shih, C.-J.; Yang, W.-C.; Lin, C.-C. Aggressive Immunosuppressant Reduction and Long-Term Rejection Risk in Renal Transplant Recipients with Pneumocystis Jiroveci Pneumonia. Exp. Clin. Transplant. 2012, 10, 344–349. [Google Scholar] [CrossRef]
- Shih, C.; Tarng, D.; Yang, W.; Yang, C. Immunosuppressant Dose Reduction and Long-Term Rejection Risk in Renal Transplant Recipients with Severe Bacterial Pneumonia. Singap. Med. J. 2014, 55, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Brakemeier, S.; Pfau, A.; Zukunft, B.; Budde, K.; Nickel, P. Prophylaxis and Treatment of Pneumocystis Jirovecii Pneumonia after Solid Organ Transplantation. Pharmacol. Res. 2018, 134, 61–67. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Laboratory Values: | Case 1 | Case 2 |
|---|---|---|
| WBC: | 4.79 × 109/L | 13.2 × 109/L |
| Lymphocytes: | 340 cells/mL | 530 cells/mL |
| CRP: | 220.1 mg/L | 23.2 mg/L |
| PCT: | 0.56 mcg/L | 0.02 mcg/L |
| LDH: | 541 UI/L (+4) | 315 UI/L |
| BDG: | 264.1 pg/mL (+5) | 207.7 pg/mL (+3) |
| Imaging: | Case 1 | Case 2 |
| Chest X-ray: | Diffuse alveolar-interstitial opacities, possible pulmonary oedema | Diffuse bilateral thickenings |
| RCT: | Multiple symmetrical ground-glass opacities. Apical and perihilar prevalence. | Ubiquitous ground glass thickenings. Anterior–posterior gradient. |
| Immuno-Suppresion Medications | Case 1 | Case 2 |
| Mofetil Mycophenolate | 1000 mg BID | 1500 mg BID |
| Ciclosporin | 125 mg BID | 100 mg + 75 mg daily |
| Prednisone | 10 mg daily | - |
| Current Recommendations on PcP Prophylaxis | |
|---|---|
| Universal prophylaxis is recommended for at least 6–12 months following heart transplant. | Class I, Level of Evidence B ISHLT Guidelines for the Care of Heart Transplant Recipients |
Extended prophylaxis can be considered:
| Class IIa, Level of Evidence B ISHLT Guidelines for the Care of Heart Transplant Recipients |
Prolonged prophylaxis is indicated in SOT recipients who show:
| N.A. American Society of Transplantation Infectious Diseases Community of Practice |
| Lifelong prophylaxis in SOT patients with history of PcP | N.A. |
| American Society of Transplantation Infectious Diseases Community of Practice | |
| Proposed Recommendations on PcP Prophylaxis | |
Extended prophylaxis:
| Hosseini-Moghaddam et al. [8] |
Extended prophylaxis:
| Permpalung et al. [12] |
Prolonged prophylaxis:
| Malpica et al. [35] |
| Lifelong prophylaxis in all HT recipients | Fillatre et al. [32] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burzio, C.; Balzani, E.; Corcione, S.; Montrucchio, G.; Trompeo, A.C.; Brazzi, L. Pneumocystis jirovecii Pneumonia after Heart Transplantation: Two Case Reports and a Review of the Literature. Pathogens 2023, 12, 1265. https://doi.org/10.3390/pathogens12101265
Burzio C, Balzani E, Corcione S, Montrucchio G, Trompeo AC, Brazzi L. Pneumocystis jirovecii Pneumonia after Heart Transplantation: Two Case Reports and a Review of the Literature. Pathogens. 2023; 12(10):1265. https://doi.org/10.3390/pathogens12101265
Chicago/Turabian StyleBurzio, Carlo, Eleonora Balzani, Silvia Corcione, Giorgia Montrucchio, Anna Chiara Trompeo, and Luca Brazzi. 2023. "Pneumocystis jirovecii Pneumonia after Heart Transplantation: Two Case Reports and a Review of the Literature" Pathogens 12, no. 10: 1265. https://doi.org/10.3390/pathogens12101265
APA StyleBurzio, C., Balzani, E., Corcione, S., Montrucchio, G., Trompeo, A. C., & Brazzi, L. (2023). Pneumocystis jirovecii Pneumonia after Heart Transplantation: Two Case Reports and a Review of the Literature. Pathogens, 12(10), 1265. https://doi.org/10.3390/pathogens12101265