
Determinants of Health-Related Quality of Life in Chronic Chikungunya Disease in Guadeloupe

 , , , and
, , , and
Abstract
:1. Introduction
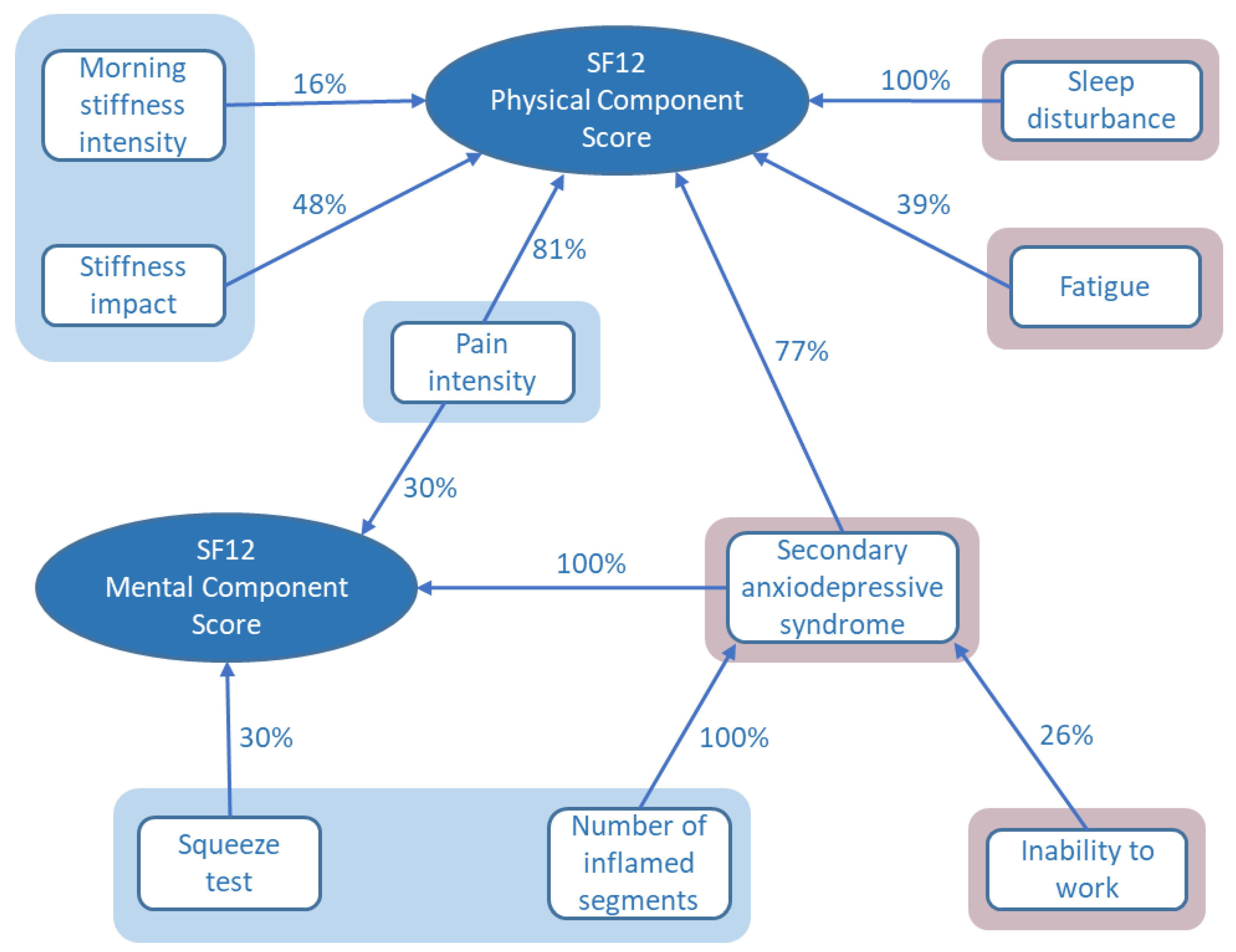
2. Results
3. Discussion
4. Materials and Methods
4.1. Study Design and Setting
4.2. Clinical Data Collection
4.3. Statistical Methods
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Staples, J.E.; Breiman, R.F.; Powers, A.M. Chikungunya fever: An epidemiological review of a re-emerging infectious disease. Clin. Infect. Dis. 2009, 49, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Suhrbier, A. Rheumatic manifestations of chikungunya: Emerging concepts and interventions. Nat. Rev. Rheumatol. 2019, 15, 597–611. [Google Scholar] [CrossRef] [PubMed]
- O’Driscoll, M.; Salje, H.; Chang, A.Y.; Watson, H. Arthralgia resolution rate following chikungunya virus infection. Int. J. Infect. Dis 2021, 112, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Simon, F.; Javelle, E.; Oliver, M.; Leparc-Goffart, I.; Marimoutou, C. Chikungunya virus infection. Curr. Infect. Dis. Rep. 2011, 13, 218–228. [Google Scholar] [CrossRef] [PubMed]
- Hickie, I.; Davenport, T.; Wakefield, D.; Vollmer-Conna, U.; Cameron, B.; Vernon, S.D.; Reeves, W.C.; Lloyd, A. Post-infective and chronic fatigue syndromes precipitated by viral and non-viral pathogens: Prospective cohort study. BMJ 2006, 333, 575. [Google Scholar] [CrossRef]
- Boaventura, P.; Macedo, S.; Ribeiro, F.; Jaconiano, S.; Soares, P. Post-COVID-19 Condition: Where Are We Now? Life 2022, 12, 517. [Google Scholar] [CrossRef]
- Elsinga, J.; Grobusch, M.P.; Tami, A.; Gerstenbluth, I.; Bailey, A. Health-related impact on quality of life and coping strategies for chikungunya: A qualitative study in Curaçao. PLoS Negl. Trop. Dis. 2017, 11, e0005987. [Google Scholar] [CrossRef]
- Marimoutou, C.; Ferraro, J.; Javelle, E.; Deparis, X.; Simon, F. Chikungunya infection: Self-reported rheumatic morbidity and impaired quality of life persist 6 years later. Clin. Microbiol. Infect. 2015, 21, 688–693. [Google Scholar] [CrossRef]
- Couzigou, B.; Criquet-Hayot, A.; Javelle, E.; Tignac, S.; Mota, E.; Rigaud, F.; Alain, A.; Troisgros, O.; Pierre-François, S.; Abel, S.; et al. Occurrence of Chronic Stage Chikungunya in the General Population of Martinique during the First 2014 Epidemic: A Prospective Epidemiological Study. Am. J. Trop. Med. Hyg. 2018, 99, 182–190. [Google Scholar] [CrossRef]
- Anwar, S.; Taslem Mourosi, J.; Khan, M.F.; Ullah, M.O.; Vanakker, O.M.; Hosen, M.J. Chikungunya outbreak in Bangladesh (2017): Clinical and hematological findings. PLoS Negl. Trop. Dis. 2020, 14, e0007466. [Google Scholar] [CrossRef]
- Schilte, C.; Staikovsky, F.; Couderc, T.; Madec, Y.; Carpentier, F.; Kassab, S.; Albert, M.L.; Lecuit, M.; Michault, A. Chikungunya virus-associated long-term arthralgia: A 36-month prospective longitudinal study. PloS Negl. Trop. Dis. 2013, 7, e2137. [Google Scholar] [CrossRef]
- Elsinga, J.; Gerstenbluth, I.; van der Ploeg, S.; Halabi, Y.; Lourents, N.T.; Burgerhof, J.G.; Van Der Veen, H.T.; Grobusch, M.P. Long-term Chikungunya Sequelae in Curaçao: Burden, Determinants, and a Novel Classification Tool. J. Infect. Dis. 2017, 216, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Gérardin, P.; Fianu, A.; Malvy, D.; Mussard, C.; Boussaïd, K.; Rollot, O.; Michault, A.; Gaüzere, B.A.; Bréart, G.; Favier, F. Perceived morbidity and community burden after a Chikungunya outbreak: The TELECHIK survey, a population-based cohort study. BMC Med. 2011, 9, 5. [Google Scholar] [CrossRef] [PubMed]
- Tritsch, S.R.; Amdur, R.; Encinales, L.; Cadena, A.; Fierbaugh, P.; Avendaño, G.; Gomez, C.A.H.; Suchowiecki, K.; Mendoza-Torres, E.; Rosales, W.; et al. Sleep disturbances are a significant predictor of chikungunya arthritis flare severity. J. Cell Immunol. 2021, 3, 191–197. [Google Scholar] [CrossRef]
- Duvignaud, A.; Fianu, A.; Bertolotti, A.; Jaubert, J.; Michault, A.; Poubeau, P.; Fred, A.; Méchain, M.; Gaüzère, B.A.; Favier, F.; et al. Rheumatism and chronic fatigue, the two facets of post-chikungunya disease: The TELECHIK cohort study on Reunion island. Epidemiol. Infect. 2018, 146, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, V.; Malaisamy, M.; Ponnaiah, M.; Kaliaperuaml, K.; Vadivoo, S.; Gupte, M.D. Impact of Chikungunya on health related quality of life Chennai, South India. PLoS ONE 2012, 7, e51519. [Google Scholar] [CrossRef]
- Soumahoro, M.K.; Gérardin, P.; Boëlle, P.Y.; Perrau, J.; Fianu, A.; Pouchot, J.; Malvy, D.; Flahault, A.; Favier, F.; Hanslik, T. Impact of Chikungunya virus infection on health status and quality of life: A retrospective cohort study. PLoS ONE 2009, 4, e7800. [Google Scholar] [CrossRef]
- Tritsch, S.R.; Encinales, L.; Pacheco, N.; Cadena, A.; Cure, C.; McMahon, E.; Watson, H.; Ramirez, A.P.; Mendoza, A.R.; Li, G.; et al. Chronic joint pain 3 years after chikungunya virus infection largely characterized by relapsing-remitting symptoms. J. Rheumatol. 2020, 47, 1267–1274. [Google Scholar] [CrossRef]
- Watson, H.; Tritsch, S.R.; Encinales, L.; Cadena, A.; Cure, C.; Ramirez, A.P.; Mendoza, A.R.; Chang, A.Y. Stiffness, pain and joint counts in chronic chikungunya disease: Relevance to disability and quality of life. Clin. Rheum. 2020, 39, 1679–1686. [Google Scholar] [CrossRef]
- Watson, H.; Nogueira-Hayd, R.L.; Rodrigues-Moreno, M.; Naveca, F.; Suchowiecki, K.; Calusi, G.; Firestein, G.S.; Simon, G.; Chang, A.Y. Tender and swollen joint counts are poorly associated with disability in chikungunya arthritis compared to rheumatoid arthritis. Sci. Rep. 2021, 11, 18578. [Google Scholar] [CrossRef]
- Luo, W.; Zeng, C.; He, H. The significance of the squeeze test to identify arthritis was underestimated or not? Ann. Rheum. Dis. 2015, 74, e60. [Google Scholar] [CrossRef] [PubMed]
- van den Bosch, W.B.; Mangnus, L.; Reijnierse, M.; Huizinga, T.W.K.; van der Helm-van Mil, A.H.M. The diagnostic accuracy of the squeeze test to identify arthritis: A cross-sectional cohort study. Ann. Rheum. Dis. 2015, 74, 1886–1889. [Google Scholar] [CrossRef] [PubMed]
- Ninla-Aesong, P.; Mitarnun, W.; Noipha, K. Long-term persistence of chikungunya virus-associated manifestations and anti-chikungunya virus antibody in Southern Thailand: 5 Years after an outbreak in 2008–2009. Viral Immunol. 2020, 33, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Morales, A.J.; Hoyos-Guapacha, K.L.; Vargas-Zapata, S.L.; Meneses-Quintero, O.M.; Gutiérrez-Segura, J.C. Would be IL-6 a missing link between chronic inflammatory rheumatism and depression after chikungunya infection? Rheumatol. Int. 2017, 37, 1149–1151. [Google Scholar] [CrossRef] [PubMed]
- Chow, A.; Her, Z.; Ong, E.K.S.; Chen, J.; Dimatatac, F.; Kwek, D.J.C.; Barkham, T.; Yang, H.; Rénia, L.; Leo, Y.S.; et al. Persistent arthralgia induced by chikungunya virus infection is associated with interleukin-6 and granulocyte macrophage colony-stimulating factor. J. Infect. Dis. 2011, 203, 149–157. [Google Scholar] [CrossRef]
- Chopra, A.; Anuradha, V.; Ghorpade, R.; Saluja, M. Acute Chikungunya and persistent musculoskeletal pain following the 2006 Indian epidemic: A 2-year prospective rural community study. Epidemiol. Infect. 2012, 140, 842–850. [Google Scholar] [CrossRef]
- Doran, C.; Elsinga, J.; Fokkema, A.; Berenschot, K.; Gerstenbluth, I.; Duits, A.; Lourents, N.; Halabi, Y.; Burgerhof, J.; Baile, A.; et al. Long-term Chikungunya sequelae and quality of life 2.5 years post-acute disease in a prospective cohort in Curaçao. PLoS Negl. Trop. Dis. 2022, 16, e0010142. [Google Scholar] [CrossRef]
- Dorléans, F.; Hoen, B.; Najioullah, F.; Herrmann-Storck, C.; Schepers, K.M.; Abel, S.; Lamaury, I.; Fagour, L.; Césaire, R.; Guyomard, S.; et al. Out-break of Chikungunya in the French Caribbean Islands of Martinique and Guadeloupe: Findings from a hospital-based surveillance system (2013–2015). Am J Trop. Med. Hyg. 2018, 98, 1819–1825. [Google Scholar] [CrossRef]
- Bouhassira, D.; Attal, N.; Alchaar, H.; Boureau, F.; Brochet, B.; Bruxelle, J.; Cunin, G.; Fermanian, J.; Ginies, P.; Grun-Overdyking, A.; et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). Pain 2005, 114, 29–36. [Google Scholar] [CrossRef]
- Gandek, B.; Ware, J.E.; Aaronson, N.K.; Apolone, G.; Bjorner, J.B.; Brazier, J.E.; Bullinger, M.; Kaasa, S.; Leplege, A.; Prieto, L.; et al. Cross-validation of item selection and scoring for the SF-12 Health Survey in nine countries: Results from the IQOLA Project. International Quality of Life Assessment. J. Clin. Epidemiol. 1998, 51, 1171–1178. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Parameter Assessed (Scale) | n | Mean ± SD | Median | IQR | Range |
|---|---|---|---|---|---|
| No. of painful segments (max 10) | 61 | 6.2 ± 2.4 | 6 | 4 | 1–10 |
| No. of stiff segments (max 10) | 60 | 4.1 ± 2.4 | 3.5 | 4 | 0–10 |
| No. of inflamed segments (max 9) | 61 | 2.2 ± 2.0 | 2 | 3 | 0–9 |
| Pain intensity (0–10) | 55 | 6.2 ± 2.4 | 7 | 3 | 0–10 |
| DN4 * (neuropathic pain) (0–10) | 51 | 4.5 ± 2.3 | 4 | 3 | 0–9 |
| Morning stiffness (0–10) | 43 | 6.9 ± 2.6 | 7 | 4 | 0–10 |
| Overall stiffness severity (0–10) | 45 | 7.6 ± 1.7 | 8 | 3 | 4–10 |
| Stiffness impact (0–10) | 44 | 7.5 ± 2.1 | 8 | 3 | 1–10 |
| Fatigue (0–100) | 46 | 57.0 ± 24.3 | 60 | 35 | 0–100 |
| SF-12 * quality of life score | 45 | PCS *: 32.3 ± 7.5 | 32.5 | 10.6 | 17.9–47.2 |
| 45 | MCS *: 34.9 ± 9.5 | 34.7 | 12.7 | 17.1–58.4 | |
| RAPID-3 * score (0–30) | 38 | 17.0 ± 7.0 | 17.4 | 8.3 | 3 −30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simon, F.; Bossy, R.; Federico, D.; Dezaunay, J.; Demoux, A.-L.; Rugard, N.; Calusi, G.; Nizzardo, A.; Watson, H.; Gane-Troplent, F. Determinants of Health-Related Quality of Life in Chronic Chikungunya Disease in Guadeloupe. Pathogens 2022, 11, 989. https://doi.org/10.3390/pathogens11090989
Simon F, Bossy R, Federico D, Dezaunay J, Demoux A-L, Rugard N, Calusi G, Nizzardo A, Watson H, Gane-Troplent F. Determinants of Health-Related Quality of Life in Chronic Chikungunya Disease in Guadeloupe. Pathogens. 2022; 11(9):989. https://doi.org/10.3390/pathogens11090989
Chicago/Turabian StyleSimon, Fabrice, Rémi Bossy, Denise Federico, Julien Dezaunay, Anne-Laurence Demoux, Nadia Rugard, Giulia Calusi, Andrea Nizzardo, Hugh Watson, and Franciane Gane-Troplent. 2022. "Determinants of Health-Related Quality of Life in Chronic Chikungunya Disease in Guadeloupe" Pathogens 11, no. 9: 989. https://doi.org/10.3390/pathogens11090989
APA StyleSimon, F., Bossy, R., Federico, D., Dezaunay, J., Demoux, A.-L., Rugard, N., Calusi, G., Nizzardo, A., Watson, H., & Gane-Troplent, F. (2022). Determinants of Health-Related Quality of Life in Chronic Chikungunya Disease in Guadeloupe. Pathogens, 11(9), 989. https://doi.org/10.3390/pathogens11090989