
Potential Neurocognitive Symptoms Due to Respiratory Syncytial Virus Infection



{kind=link}
{kind=link}
Abstract
1. Introduction
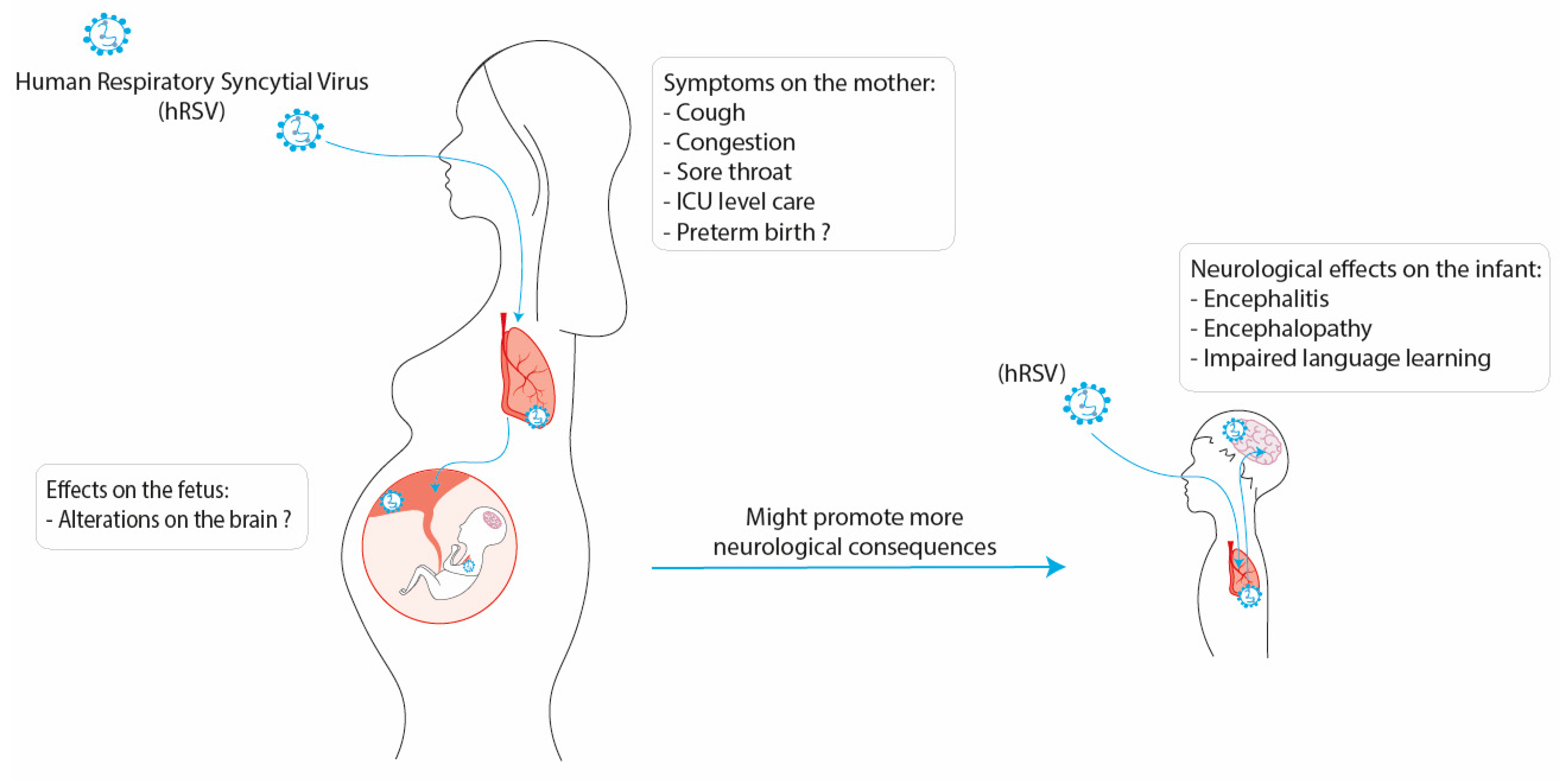
2. hRSV Infection during Pregnancy and Effects on the Newborn
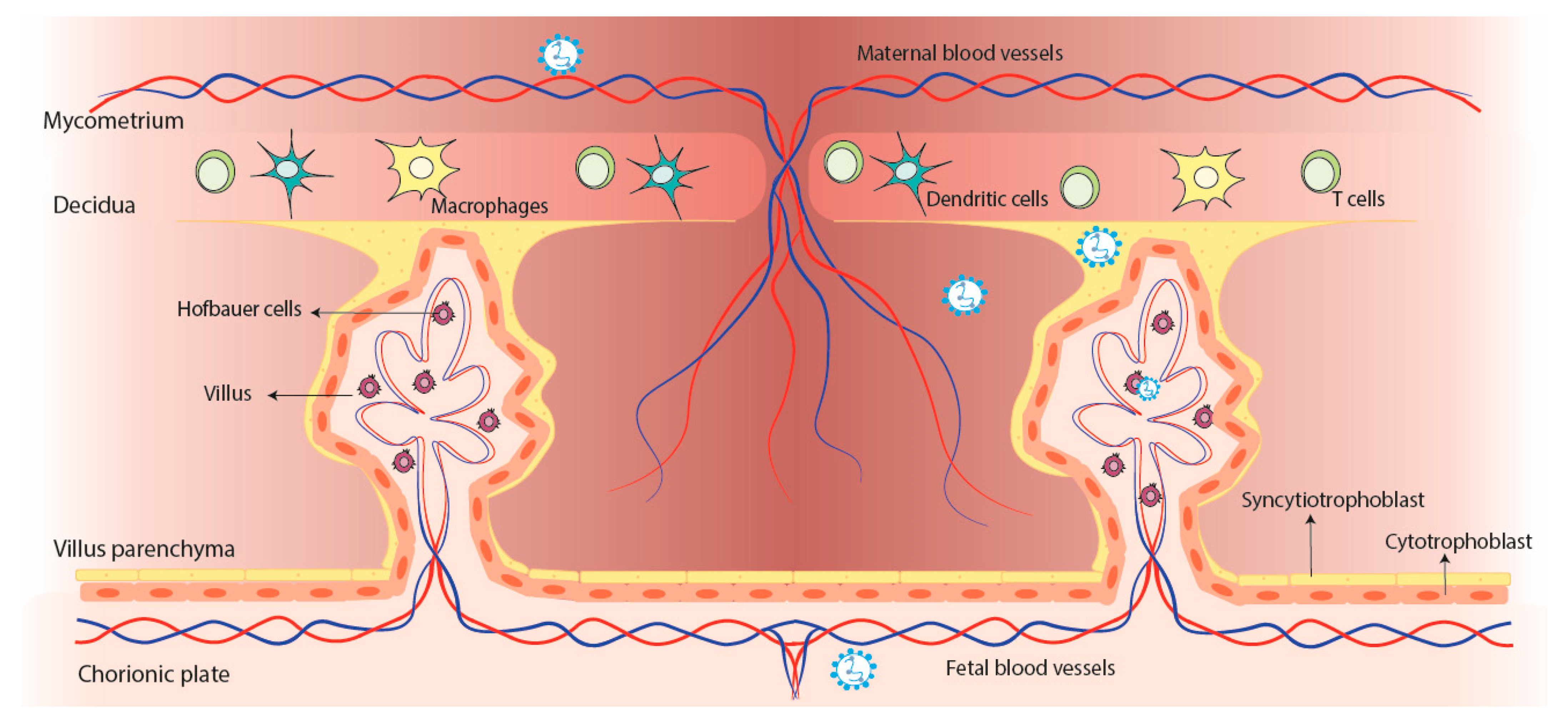
3. hRSV Infection during Gestation: Possible Impairment of Fetal Neurodevelopment?
4. Neurological Consequences due to hRSV Infection
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Barr, R.; Green, C.A.; Sande, C.J.; Drysdale, S.B. Respiratory syncytial virus: Diagnosis, prevention and management. Ther. Adv. Infect. Dis. 2019, 6, 204993611986579. [Google Scholar] [CrossRef]
- Caballero, M.T.; Polack, F.P. Respiratory syncytial virus is an “opportunistic” killer. Pediatr. Pulmonol. 2018, 53, 664–667. [Google Scholar] [CrossRef]
- Mammas, I.N.; Drysdale, S.B.; Rath, B.; Theodoridou, M.; Papaioannou, G.; Papatheodoropoulou, A.; Koutsounaki, E.; Koutsaftiki, C.; Kozanidou, E.; Achtsidis, V.; et al. Update on current views and advances on RSV infection (Review). Int. J. Mol. Med. 2020, 46, 509–520. [Google Scholar] [CrossRef] [PubMed]
- Amarasinghe, G.K.; Ayllón, M.A.; Bào, Y.; Basler, C.F.; Bavari, S.; Blasdell, K.R.; Briese, T.; Brown, P.A.; Bukreyev, A.; Balkema-Buschmann, A.; et al. Taxonomy of the order Mononegavirales: Update 2019. Arch. Virol. 2019, 164, 1967–1980. [Google Scholar] [CrossRef] [PubMed]
- Bohmwald, K.; Espinoza, J.A.; Rey-Jurado, E.; Gómez, R.S.; González, P.A.; Bueno, S.M.; Riedel, C.A.; Kalergis, A.M. Human Respiratory Syncytial Virus: Infection and Pathology. Semin. Respir. Crit. Care Med. 2016, 37, 522–537. [Google Scholar] [CrossRef]
- Andeweg, S.P.; Schepp, R.M.; van de Kassteele, J.; Mollema, L.; Berbers, G.A.M.; van Boven, M. Population-based serology reveals risk factors for RSV infection in children younger than 5 years. Sci. Rep. 2021, 11, 8953. [Google Scholar] [CrossRef] [PubMed]
- Shi, T.; McAllister, D.A.; O’Brien, K.L.; Simoes, E.A.F.; Madhi, S.A.; Gessner, B.D.; Polack, F.P.; Balsells, E.; Acacio, S.; Aguayo, C.; et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: A systematic review and modelling study. Lancet 2017, 390, 946–958. [Google Scholar] [CrossRef]
- Kazakova, A.; Kakkola, L.; Päkkilä, H.; Teros-Jaakkola, T.; Soukka, T.; Peltola, V.; Waris, M.; Julkunen, I. Serological Array-in-Well Multiplex Assay Reveals a High Rate of Respiratory Virus Infections and Reinfections in Young Children. mSphere 2019, 4, e00447-19. [Google Scholar] [CrossRef]
- Hervé, P.L.; Deloizy, C.; Descamps, D.; Rameix-Welti, M.A.; Fix, J.; McLellan, J.S.; Eléouët, J.F.; Riffault, S. RSV N-nanorings fused to palivizumab-targeted neutralizing epitope as a nanoparticle RSV vaccine. Nanomed. Nanotechnol. Biol. Med. 2017, 13, 411–420. [Google Scholar] [CrossRef]
- Opek, M.W.; Yeshayahu, Y.; Glatman-Freedman, A.; Kaufman, Z.; Sorek, N.; Brosh-Nissimov, T. Delayed respiratory syncytial virus epidemic in children after relaxation of COVID-19 physical distancing measures, Ashdod, Israel, 2021. Eurosurveillance 2021, 26, 2100706. [Google Scholar] [CrossRef]
- Agha, R.; Avner, J.R. Delayed Seasonal RSV Surge Observed During the COVID-19 Pandemic. Pediatrics 2021, 148, e2021052089. [Google Scholar] [CrossRef]
- Foley, D.A.; Yeoh, D.K.; Minney-Smith, C.A.; Martin, A.C.; Mace, A.O.; Sikazwe, C.T.; Le, H.; Levy, A.; Moore, H.C.; Blyth, C.C. The Interseasonal Resurgence of Respiratory Syncytial Virus in Australian Children Following the Reduction of Coronavirus Disease 2019–Related Public Health Measures. Clin. Infect. Dis. 2021, 73, e2829–e2830. [Google Scholar] [CrossRef]
- Ujiie, M.; Tsuzuki, S.; Nakamoto, T.; Iwamoto, N. Resurgence of Respiratory Syncytial Virus Infections during COVID-19 Pandemic, Tokyo, Japan. Emerg. Infect. Dis. 2021, 27, 2969–2970. [Google Scholar] [CrossRef]
- Kalergis, A.M.; Soto, J.A.; Gálvez, N.M.S.; Andrade, C.A.; Fernandez, A.; Bohmwald, K.; Bueno, S.M. Pharmacological management of human respiratory syncytial virus infection. Expert Opin. Pharmacother. 2020, 21, 2293–2303. [Google Scholar] [CrossRef] [PubMed]
- Mac, S.; Sumner, A.; Duchesne-Belanger, S.; Stirling, R.; Tunis, M.; Sander, B. Cost-effectiveness of Palivizumab for Respiratory Syncytial Virus: A systematic review. Pediatrics 2019, 143, e20184064. [Google Scholar] [CrossRef] [PubMed]
- Andrade, C.A.; Pacheco, G.A.; Gálvez, N.M.S.; Soto, J.A.; Bueno, S.M.; Kalergis, A.M. Innate immune components that regulate the pathogenesis and resolution of hRSV and hMPV infections. Viruses 2020, 12, 637. [Google Scholar] [CrossRef] [PubMed]
- Bohmwald, K.; Soto, J.A.J.A.; Andrade-Parra, C.; Fernández-Fierro, A.; Espinoza, J.A.J.A.; Ríos, M.; Eugenin, E.A.E.A.E.A.; González, P.A.P.A.; Opazo, M.C.M.C.; Riedel, C.A.; et al. Lung pathology due to hRSV infection impairs blood–brain barrier permeability enabling astrocyte infection and a long-lasting inflammation in the CNS. Brain. Behav. Immun. 2021, 91, 159–171. [Google Scholar] [CrossRef]
- Velázquez-Cervantes, M.A.; Martínez-Castillo, M.; González-García, L.D.; Vargas-Pavía, T.A.; Martínez-Salazar, M.G.; Mancilla-Herrera, I.; León-Reyes, G.; García-Cordero, J.; Helguera-Repetto, A.C.; León-Juárez, M. The BeWo cell line derived from a human placental choriocarcinoma is permissive for respiratory syncytial virus infection. Virus Genes 2019, 55, 406–410. [Google Scholar] [CrossRef] [PubMed]
- Bohmwald, K.; Gálvez, N.M.S.; Ríos, M.; Kalergis, A.M. Neurologic Alterations Due to Respiratory Virus Infections. Front. Cell. Neurosci. 2018, 12, 386. [Google Scholar] [CrossRef]
- Park, A.; Suh, S.I.; Son, G.R.; Lee, Y.H.; Seo, H.S.; Eun, B.L.; Lee, N.J.; Seol, H.Y. Respiratory syncytial virus-related encephalitis: Magnetic resonance imaging findings with diffusion-weighted study. Neuroradiology 2014, 56, 163–168. [Google Scholar] [CrossRef]
- Xu, L.; Gao, H.; Zeng, J.; Liu, J.; Lu, C.; Guan, X.; Qian, S.; Xie, Z. A fatal case associated with respiratory syncytial virus infection in a young child. BMC Infect. Dis. 2018, 18, 217. [Google Scholar] [CrossRef]
- Regan, A.K.; Klein, N.P.; Langley, G.; Drews, S.J.; Buchan, S.; Ball, S.; Kwong, J.C.; Naleway, A.; Thompson, M.; Wyant, B.E.; et al. Respiratory Syncytial Virus Hospitalization During Pregnancy in 4 High-income Countries, 2010–2016. Clin. Infect. Dis. 2018, 67, 1915–1918. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, S.M.; Dotters-Katz, S.; Heine, R.P.; Grotegut, C.A.; Swamy, G.K. Maternal Effects of Respiratory Syncytial Virus Infection during Pregnancy. Emerg. Infect. Dis. 2015, 21, 1951. [Google Scholar] [CrossRef] [PubMed]
- Piedimonte, G.; Walton, C.; Samsell, L. Vertical Transmission of Respiratory Syncytial Virus Modulates Pre- and Postnatal Innervation and Reactivity of Rat Airways. PLoS ONE 2013, 8, e61309. [Google Scholar] [CrossRef] [PubMed]
- Althouse, B.M.; Flasche, S.; Toizumi, M.; Thi Nguyen, H.-A.; Minh Vo, H.; Nhat Le, M.; Hashizume, M.; Ariyoshi, K.; Duc Anh, D.; Rodgers, G.L.; et al. Differences in clinical severity of respiratory viral infections in hospitalized children. Sci. Rep. 2021, 11, 1–11. [Google Scholar] [CrossRef]
- Lee, N.; Smith, S.; Zelyas, N.; Klarenbach, S.; Zapernick, L.; Bekking, C.; So, H.; Yip, L.; Tipples, G.; Taylor, G.; et al. Burden of noninfluenza respiratory viral infections in adults admitted to hospital: Analysis of a multiyear Canadian surveillance cohort from 2 centres. CMAJ 2021, 193, E439–E446. [Google Scholar] [CrossRef]
- Suleiman-Martos, N.; Caballero-Vázquez, A.; Gómez-Urquiza, J.L.; Albendín-García, L.; Romero-Béjar, J.L.; Cañadas-De la Fuente, G.A. Prevalence and risk factors of respiratory syncytial virus in children under 5 years of age in the who european region: A systematic review and meta-analysis. J. Pers. Med. 2021, 11, 416. [Google Scholar] [CrossRef]
- Uyeki, T.M. High-risk Groups for Influenza Complications. J. Am. Med. Assoc. 2020, 324, 2334. [Google Scholar] [CrossRef]
- Supak, D.; Pethő, B.; Cseh, R.; Lintner, B.; Acs, N. Pregnancy complications and birth outcomes in pregnant women with viral infections: A population-based study. Authorea Prepr. 2020. [Google Scholar] [CrossRef]
- Liong, S.; Oseghale, O.; To, E.E.; Brassington, K.; Erlich, J.R.; Luong, R.; Liong, F.; Brooks, R.; Martin, C.; O’Toole, S.; et al. Influenza A virus causes maternal and fetal pathology via innate and adaptive vascular inflammation in mice. Proc. Natl. Acad. Sci. USA 2020, 117, 24964–24973. [Google Scholar] [CrossRef]
- Moreno, J.L.; Kurita, M.; Holloway, T.; López, J.; Cadagan, R.; Martínez-Sobrido, L.; García-Sastre, A.; González-Maeso, J. Maternal influenza viral infection causes schizophrenia-like alterations of 5-HT2Aand mGlu2 receptors in the adult offspring. J. Neurosci. 2011, 31, 1863–1872. [Google Scholar] [CrossRef]
- Shi, L.; Fatemi, S.H.; Sidwell, R.W.; Patterson, P.H. Maternal Influenza Infection Causes Marked Behavioral and Pharmacological Changes in the Offspring. J. Neurosci. 2003, 23, 297–302. [Google Scholar] [CrossRef]
- Lafond, K.E.; Porter, R.M.; Whaley, M.J.; Suizan, Z.; Ran, Z.; Aleem, M.A.; Thapa, B.; Sar, B.; Proschle, V.S.; Peng, Z.; et al. Global burden of influenza-associated lower respiratory tract infections and hospitalizations among adults: A systematic review and meta-analysis. PLoS Med. 2021, 18, e1003550. [Google Scholar] [CrossRef]
- Englund, J.A.; Chu, H.Y. Respiratory Virus Infection During Pregnancy: Does It Matter? J. Infect. Dis. 2018, 218, 512–515. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Tong, L.; Li, M.; Wang, Y.; Li, L.; Yang, D.; Zhang, Y.; Chen, Z. Recurrent Wheezing and Asthma After Respiratory Syncytial Virus Bronchiolitis. Front. Pediatr. 2021, 9, 543. [Google Scholar] [CrossRef]
- Hause, A.M.; Avadhanula, V.; Maccato, M.L.; Pinell, P.M.; Bond, N.; Santarcangelo, P.; Ferlic-Stark, L.; Munoz, F.M.; Piedra, P.A. A Cross-sectional Surveillance Study of the Frequency and Etiology of Acute Respiratory Illness Among Pregnant Women. J. Infect. Dis. 2018, 218, 528–535. [Google Scholar] [CrossRef]
- Hause, A.M.; Avadhanula, V.; Maccato, M.L.; Pinell, P.M.; Bond, N.; Santarcangelo, P.; Ferlic-Stark, L.; Ye, X.; Iwuchukwu, O.; Maurer, L.; et al. Clinical characteristics and outcomes of respiratory syncytial virus infection in pregnant women. Vaccine 2019, 37, 3464–3471. [Google Scholar] [CrossRef] [PubMed]
- Madhi, S.A.; Cutland, C.L.; Downs, S.; Jones, S.; van Niekerk, N.; Simoes, E.A.F.; Nunes, M.C. Burden of Respiratory Syncytial Virus Infection in South African Human Immunodeficiency Virus (HIV)-Infected and HIV-Uninfected Pregnant and Postpartum Women: A Longitudinal Cohort Study. Clin. Infect. Dis. 2018, 66, 1658–1665. [Google Scholar] [CrossRef] [PubMed]
- Chu, H.Y.; Katz, J.; Tielsch, J.; Khatry, S.K.; Shrestha, L.; LeClerq, S.C.; Magaret, A.; Kuypers, J.; Steinhoff, M.C.; Englund, J.A.; et al. Clinical Presentation and Birth Outcomes Associated with Respiratory Syncytial Virus Infection in Pregnancy. PLoS ONE 2016, 11, 0152015. [Google Scholar] [CrossRef] [PubMed]
- Manti, S.; Cuppari, C.; Lanzafame, A.; Salpietro, C.; Betta, P.; Leonardi, S.; Perez, M.K.; Piedimonte, G. Detection of respiratory syncytial virus (RSV) at birth in a newborn with respiratory distress. Pediatr. Pulmonol. 2017, 52, E81–E84. [Google Scholar] [CrossRef] [PubMed]
- Manti, S.; Esper, F.; Alejandro-Rodriguez, M.; Leonardi, S.; Betta, P.; Cuppari, C.; Lanzafame, A.; Worley, S.; Salpietro, C.; Perez, M.K.; et al. Respiratory syncytial virus seropositivity at birth is associated with adverse neonatal respiratory outcomes. Pediatr. Pulmonol. 2020, 55, 3074–3079. [Google Scholar] [CrossRef] [PubMed]
- Bokun, V.; Moore, J.J.; Moore, R.; Smallcombe, C.C.; Harford, T.J.; Rezaee, F.; Esper, F.; Piedimonte, G. Respiratory syncytial virus exhibits differential tropism for distinct human placental cell types with Hofbauer cells acting as a permissive reservoir for infection. PLoS ONE 2019, 14, e0225767. [Google Scholar] [CrossRef] [PubMed]
- Piedimonte, G.; Perez, M.K. Alternative mechanisms for respiratory syncytial virus (RSV) infection and persistence: Could RSV be transmitted through the placenta and persist into developing fetal lungs? Curr. Opin. Pharmacol. 2014, 16, 82–88. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Brown, P.M.; Harford, T.J.; Agrawal, V.; Yen-Lieberman, B.; Rezaee, F.; Piedimonte, G. Prenatal Exposure to Respiratory Syncytial Virus Alters Postnatal Immunity and Airway Smooth Muscle Contractility during Early-Life Reinfections. PLoS ONE 2017, 12, e0168786. [Google Scholar] [CrossRef]
- Piedimonte, G.; Harford, T.J. Effects of maternal−fetal transmission of viruses and other environmental agents on lung development. Pediatr. Res. 2020, 87, 420–426. [Google Scholar] [CrossRef]
- Tortorolo, L.; Langer, A.; Polidori, G.; Vento, G.; Stampachiacchere, B.; Aloe, L.; Piedimonte, G. Neurotrophin overexpression in lower airways of infants with respiratory syncytial virus infection. Am. J. Respir. Crit. Care Med. 2005, 172, 233–237. [Google Scholar] [CrossRef]
- PIEDIMONTE, G. Contribution of neuroimmune mechanisms to airway inflammation and remodeling during and after respiratory syncytial virus infection. Pediatr. Infect. Dis. J. 2003, 22, S66–S75. [Google Scholar] [CrossRef]
- Goeden, N.; Velasquez, J.; Arnold, K.A.; Chan, Y.; Lund, B.T.; Anderson, G.M.; Bonnin, A. Maternal inflammation disrupts fetal neurodevelopment via increased placental output of serotonin to the fetal brain. J. Neurosci. 2016, 36, 6041–6049. [Google Scholar] [CrossRef]
- Parboosing, R.; Bao, Y.; Shen, L.; Schaefer, C.A.; Brown, A.S. Gestational influenza and bipolar disorder in adult offspring. JAMA Psychiatry 2013, 70, 677–685. [Google Scholar] [CrossRef]
- Bohmwald, K.; Andrade, C.A.; Kalergis, A.M. Contribution of Pro-Inflammatory Molecules Induced by Respiratory Virus Infections to Neurological Disorders. Pharmaceuticals 2021, 14, 340. [Google Scholar] [CrossRef]
- Minakova, E.; Warner, B.B. Maternal immune activation, central nervous system development and behavioral phenotypes. Birth Defects Res. 2018, 110, 1539–1550. [Google Scholar] [CrossRef] [PubMed]
- Ozaki, K.; Kato, D.; Ikegami, A.; Hashimoto, A.; Sugio, S.; Guo, Z.; Shibushita, M.; Tatematsu, T.; Haruwaka, K.; Moorhouse, A.J.; et al. Maternal immune activation induces sustained changes in fetal microglia motility. Sci. Rep. 2020, 10, 1–19. [Google Scholar] [CrossRef]
- Quagliato, L.A.; de Matos, U.; Nardi, A.E. Maternal immune activation generates anxiety in offspring: A translational meta-analysis. Transl. Psychiatry 2021, 11, 1–6. [Google Scholar] [CrossRef]
- Aguilar-Valles, A.; Rodrigue, B.; Matta-Camacho, E. Maternal Immune Activation and the Development of Dopaminergic Neurotransmission of the Offspring: Relevance for Schizophrenia and Other Psychoses. Front. Psychiatry 2020, 11, 852. [Google Scholar] [CrossRef] [PubMed]
- Luchicchi, A.; Lecca, S.; Melis, M.; De Felice, M.; Cadeddu, F.; Frau, R.; Muntoni, A.L.; Fadda, P.; Devoto, P.; Pistis, M. Maternal Immune Activation Disrupts Dopamine System in the Offspring. Int. J. Neuropsychopharmacol. 2016, 19, 1–10. [Google Scholar] [CrossRef]
- Reisinger, S.N.; Kong, E.; Khan, D.; Schulz, S.; Ronovsky, M.; Berger, S.; Horvath, O.; Cabatic, M.; Berger, A.; Pollak, D.D. Maternal immune activation epigenetically regulates hippocampal serotonin transporter levels. Neurobiol. Stress 2016, 4, 34–43. [Google Scholar] [CrossRef]
- Estes, M.L.; McAllister, A.K. Maternal immune activation: Implications for neuropsychiatric disorders. Science 2016, 353, 772–777. [Google Scholar] [CrossRef] [PubMed]
- Parker-Athill, E.C.; Tan, J. Maternal Immune Activation and Autism Spectrum Disorder: Interleukin-6 Signaling as a Key Mechanistic Pathway. Neurosignals 2010, 18, 113–128. [Google Scholar] [CrossRef]
- Winter, C.; Djodari-Irani, A.; Sohr, R.; Morgenstern, R.; Feldon, J.; Juckel, G.; Meyer, U. Prenatal immune activation leads to multiple changes in basal neurotransmitter levels in the adult brain: Implications for brain disorders of neurodevelopmental origin such as schizophrenia. Int. J. Neuropsychopharmacol. 2009, 12, 513–524. [Google Scholar] [CrossRef]
- Meyer, U.; Nyffeler, M.; Schwendener, S.; Knuesel, I.; Yee, B.K.; Feldon, J. Relative Prenatal and Postnatal Maternal Contributions to Schizophrenia-Related Neurochemical Dysfunction after In Utero Immune Challenge. Neuropsychopharmacology 2007, 33, 441–456. [Google Scholar] [CrossRef]
- Meyer, U.; Engler, A.; Weber, L.; Schedlowski, M.; Feldon, J. Preliminary evidence for a modulation of fetal dopaminergic development by maternal immune activation during pregnancy. Neuroscience 2008, 154, 701–709. [Google Scholar] [CrossRef]
- Weber-Stadlbauer, U.; Richetto, J.; Zwamborn, R.A.J.; Slieker, R.C.; Meyer, U. Transgenerational modification of dopaminergic dysfunctions induced by maternal immune activation. Neuropsychopharmacology 2020, 46, 404–412. [Google Scholar] [CrossRef]
- MacDowell, K.S.; Munarriz-Cuezva, E.; Meana, J.J.; Leza, J.C.; Ortega, J.E. Paliperidone Reversion of Maternal Immune Activation-Induced Changes on Brain Serotonin and Kynurenine Pathways. Front. Pharmacol. 2021, 12, 1183. [Google Scholar] [CrossRef]
- Holloway, T.; Moreno, J.L.; Umali, A.; Rayannavar, V.; Hodes, G.E.; Russo, S.J.; González-Maeso, J. Prenatal Stress Induces Schizophrenia-Like Alterations of Serotonin 2A and Metabotropic Glutamate 2 Receptors in the Adult Offspring: Role of Maternal Immune System. J. Neurosci. 2013, 33, 1088–1098. [Google Scholar] [CrossRef]
- Nakagawa, K.; Yoshino, H.; Ogawa, Y.; Yamamuro, K.; Kimoto, S.; Noriyama, Y.; Makinodan, M.; Yamashita, M.; Saito, Y.; Kishimoto, T. Maternal Immune Activation Affects Hippocampal Excitatory and Inhibitory Synaptic Transmission in Offspring From an Early Developmental Period to Adulthood. Front. Cell. Neurosci. 2020, 14, 241. [Google Scholar] [CrossRef]
- Arrode-Brusés, G.; Brusés, J.L. Maternal immune activation by poly(I:C) induces expression of cytokines IL-1β and IL-13, chemokine MCP-1 and colony stimulating factor VEGF in fetal mouse brain. J. Neuroinflammation 2012, 9, 1–16. [Google Scholar] [CrossRef]
- Paraschivescu, C.; Barbosa, S.; Lorivel, T.; Glaichenhaus, N.; Davidovicid, L.; Davidovic, L. Cytokine changes associated with the maternal immune activation (mia) model of autism: A penalized regression approach. PLoS ONE 2020, 15, e0231609. [Google Scholar] [CrossRef]
- Pendyala, G.; Chou, S.; Jung, Y.; Coiro, P.; Spartz, E.; Padmashri, R.; Li, M.; Dunaevsky, A. Maternal Immune Activation Causes Behavioral Impairments and Altered Cerebellar Cytokine and Synaptic Protein Expression. Neuropsychopharmacology 2017, 42, 1435–1446. [Google Scholar] [CrossRef] [PubMed]
- Somerville, L.K.; Basile, K.; Dwyer, D.E.; Kok, J. The Impact of Influenza Virus Infection in Pregnancy. Future Microbiol. 2018, 13, 263–274. [Google Scholar] [CrossRef] [PubMed]
- Antonson, A.M.; Kenney, A.D.; Chen, H.J.; Corps, K.N.; Yount, J.S.; Gur, T.L. Moderately pathogenic maternal influenza A virus infection disrupts placental integrity but spares the fetal brain. Brain Behav. Immun. 2021, 96. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, H.; Walendy-Gnirß, K.; Tekin-Bubenheim, N.; Kouassi, N.M.; Ben-Batalla, I.; Berenbrok, N.; Wolff, M.; dos Reis, V.P.; Zickler, M.; Scholl, L.; et al. Offspring born to influenza A virus infected pregnant mice have increased susceptibility to viral and bacterial infections in early life. Nat. Commun. 2021, 12, 1–14. [Google Scholar] [CrossRef]
- Gozde Kanmaz, H.; Erdeve, O.; Suna Oǧz, S.; Uras, N.; Çelen, Ş.; Korukluoglu, G.; Zergeroglu, S.; Kara, A.; Dilmen, U. Placental transmission of novel pandemic influenza a virus. Fetal Pediatr. Pathol. 2011, 30, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Vásquez, R.D.; Chávez, V.M.; Gamio, I.E.; Muñoz, R.I.; Polar, M.F.; Montalvo, R.; Ticona, E. Probable vertical transmission of the influenza virus a (H1N1): Apropos of a case. Rev. Peru. Med. Exp. Salud Publica 2010, 27, 466–469. [Google Scholar] [CrossRef]
- Picone, O.; Bernabe-Dupont, C.; Vauloup-Fellous, C.; Castel, C.; Cordier, A.G.; Guillet, M.; Grangeot-Keros, L.; Boileau, P.; Benachi, A.; Frydman, R. Un possible cas de transmission in utero du virus de la grippe A (H1N1). J. Gynecol. Obstet. Biol. Reprod. 2011, 40, 473–475. [Google Scholar] [CrossRef]
- Smith, S.E.P.; Li, J.; Garbett, K.; Mirnics, K.; Patterson, P.H. Maternal Immune Activation Alters Fetal Brain Development through Interleukin-6. J. Neurosci. 2007, 27, 10695–10702. [Google Scholar] [CrossRef] [PubMed]
- Landreau, F.; Galeano, P.; Caltana, L.R.; Masciotra, L.; Chertcoff, A.; Pontoriero, A.; Baumeister, E.; Amoroso, M.; Brusco, H.A.; Tous, M.I.; et al. Effects of Two Commonly Found Strains of Influenza A Virus on Developing Dopaminergic Neurons, in Relation to the Pathophysiology of Schizophrenia. PLoS ONE 2012, 7, e51068. [Google Scholar] [CrossRef]
- Zeafley, J. Neurological, Electroencephalographic, and Virological Findings in Febrile Children Ages at Admission, and Sex Incidence Age at Time of Group A Group B Group C Group D Admission (28 cases) (25 cases) (18 cases) (7 cases). Arch. Dis. Child. 1970, 45, 611. [Google Scholar] [CrossRef]
- Bohmwald, K.; Espinoza, J.A.; González, P.A.; Bueno, S.M.; Riedel, C.A.; Kalergis, A.M. Central nervous system alterations caused by infection with the human respiratory syncytial virus. Rev. Med. Virol. 2014. [Google Scholar] [CrossRef] [PubMed]
- Tison-Chambellan, C.; Cheuret, E.; Cances, C.; Karsenty, C.; Le Camus, C.; Sevely, A.; Chaix, Y. Rhombencéphalite liée au virus respiratoire syncytial chez un garçon de 7 ans. Arch. Pediatr. 2013, 20, 657–660. [Google Scholar] [CrossRef]
- Moriyama, K.; Takahashi, Y.; Shiihara, T. Another case of respiratory syncytial virus-related limbic encephalitis. Neuroradiology 2014, 56, 435–436. [Google Scholar] [CrossRef]
- Millichap, J.J.; Wainwright, M.S. Neurological complications of respiratory syncytial virus infection: Case series and review of literature. J. Child Neurol. 2009, 24, 1499–1503. [Google Scholar] [CrossRef] [PubMed]
- Kawashima, H.; Ioi, H.; Ushio, M.; Yamanaka, G.; Matsumoto, S.; Nakayama, T. Cerebrospinal fluid analysis in children with seizures from respiratory syncytial virus infection. Scand. J. Infect. Dis. 2009, 41, 228–231. [Google Scholar] [CrossRef] [PubMed]
- Otake, Y.; Yamagata, T.; Morimoto, Y.; Imi, M.; Mori, M.; Aihara, T.; Ichiyama, T.; Momoi, M.Y. Elevated CSF IL-6 in a patient with respiratory syncytial virus encephalopathy. Brain Dev. 2007, 29, 117–120. [Google Scholar] [CrossRef] [PubMed]
- Saravanos, G.L.; King, C.L.; Deng, L.; Dinsmore, N.; Ramos, I.; Takashima, M.; Crawford, N.; Clark, J.E.; Dale, R.C.; Jones, C.A.; et al. Respiratory Syncytial Virus–Associated Neurologic Complications in Children: A Systematic Review and Aggregated Case Series. J. Pediatr. 2021, 239, 39–49.e9. [Google Scholar] [CrossRef]
- Picone, S.; Mondì, V.; Di Palma, F.; Martini, L.; Paolillo, P. Neonatal Encephalopathy and SIADH during RSV Infection. Am. J. Perinatol. 2019, 36, S106–S109. [Google Scholar] [CrossRef]
- Van den Pol, A.N. van den Viral infection leading to brain dysfunction: More prevalent than appreciated? Neuron 2009, 64, 17. [Google Scholar] [CrossRef] [PubMed]
- Peña, M.; Jara, C.; Flores, J.C.; Hoyos-Bachiloglu, R.; Iturriaga, C.; Medina, M.; Carcey, J.; Espinoza, J.; Bohmwald, K.; Kalergis, A.M.; et al. Severe respiratory disease caused by human respiratory syncytial virus impairs language learning during early infancy. Sci. Rep. 2020, 10, 22356. [Google Scholar] [CrossRef]
- Bird, C.M.; Burgess, N. The hippocampus and memory: Insights from spatial processing. Nat. Rev. Neurosci. 2008, 9, 182–194. [Google Scholar] [CrossRef]
- Miyamoto, K.; Fujisawa, M.; Tsuboi, T.; Hirao, J.I.; Sugita, K.; Arisaka, O.; Hozumi, H.; Kuwashima, S.; Tsuboi, T. Systemic inflammatory response syndrome and prolonged hypoperfusion lesions in an infant with respiratory syncytial virus encephalopathy. J. Infect. Chemother. 2013, 19, 978–982. [Google Scholar] [CrossRef] [PubMed]
- Bogaerts, L.; Szmalec, A.; Hachmann, W.M.; Page, M.P.A.; Duyck, W. Linking memory and language: Evidence for a serial-order learning impairment in dyslexia. Res. Dev. Disabil. 2015, 43–44, 106–122. [Google Scholar] [CrossRef] [PubMed]
- Espinoza, J.A.; Bohmwald, K.; Cespedes, P.F.; Gomez, R.S.; Riquelme, S.A.; Cortes, C.M.; Valenzuela, J.A.; Sandoval, R.A.; Pancetti, F.C.; Bueno, S.M.; et al. Impaired learning resulting from Respiratory Syncytial Virus infection. Proc. Natl. Acad. Sci. USA 2013, 11, 9112–9117. [Google Scholar] [CrossRef]
- Kumar, A. Long-term potentiation at CA3-CA1 hippocampal synapses with special emphasis on aging, disease, and stress. Front. Aging Neurosci. 2011, 3, 1–20. [Google Scholar] [CrossRef]
- Hause, A.M.; Panagiotakopoulos, L.; Weintraub, E.S.; Sy, L.S.; Glenn, S.C.; Tseng, H.-F.; McNeil, M.M. Adverse Outcomes in Pregnant Women Hospitalized With Respiratory Syncytial Virus Infection: A Case Series. Clin. Infect. Dis. 2021, 72, 138–140. [Google Scholar] [CrossRef]
- Brown, A.S.; Meyer, U. Maternal Immune Activation and Neuropsychiatric Illness: A Translational Research Perspective. Am. J. Psychiatry 2018, 175, 1073–1083. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Smith, S.E.P.; Malkova, N.; Tse, D.; Su, Y.; Patterson, P.H. Activation of the maternal immune system alters cerebellar development in the offspring. Brain Behav. Immun. 2009, 23, 116–123. [Google Scholar] [CrossRef]
- Eisenhut, M. Extrapulmonary manifestations of severe respiratory syncytial virus infection--a systematic review. Crit. Care 2006, 10, R107. [Google Scholar] [CrossRef] [PubMed]
- Reisinger, S.; Khan, D.; Kong, E.; Berger, A.; Pollak, A.; Pollak, D.D. The Poly(I:C)-induced maternal immune activation model in preclinical neuropsychiatric drug discovery. Pharmacol. Ther. 2015, 149, 213–226. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, Y.; Suyama, K.; Go, H.; Hosoya, M. Clinical manifestations of respiratory syncytial virus-associated encephalopathy in Fukushima, Japan. Pediatr. Int. 2019, 61, 802–806. [Google Scholar] [CrossRef]
- Jiang, Y.; Patel, C.D.; Manivanh, R.; North, B.; Backes, I.M.; Posner, D.A.; Gilli, F.; Pachner, A.R.; Nguyen, L.N.; Leib, D.A. Maternal antiviral immunoglobulin accumulates in neural tissue of neonates to prevent HSV neurological disease. MBio 2017, 8, e00678-17. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andrade, C.A.; Kalergis, A.M.; Bohmwald, K. Potential Neurocognitive Symptoms Due to Respiratory Syncytial Virus Infection. Pathogens 2022, 11, 47. https://doi.org/10.3390/pathogens11010047
Andrade CA, Kalergis AM, Bohmwald K. Potential Neurocognitive Symptoms Due to Respiratory Syncytial Virus Infection. Pathogens. 2022; 11(1):47. https://doi.org/10.3390/pathogens11010047
Chicago/Turabian StyleAndrade, Catalina A., Alexis M. Kalergis, and Karen Bohmwald. 2022. "Potential Neurocognitive Symptoms Due to Respiratory Syncytial Virus Infection" Pathogens 11, no. 1: 47. https://doi.org/10.3390/pathogens11010047
APA StyleAndrade, C. A., Kalergis, A. M., & Bohmwald, K. (2022). Potential Neurocognitive Symptoms Due to Respiratory Syncytial Virus Infection. Pathogens, 11(1), 47. https://doi.org/10.3390/pathogens11010047