
Use of Rv0222-Rv2657c-Rv1509 Fusion Protein to Improve the Accuracy of an Antibody ELISA for Extra-Pulmonary Tuberculosis in Humans

 and
and 
Abstract
:1. Introduction
2. Results
2.1. Generation of Fusion Antigens
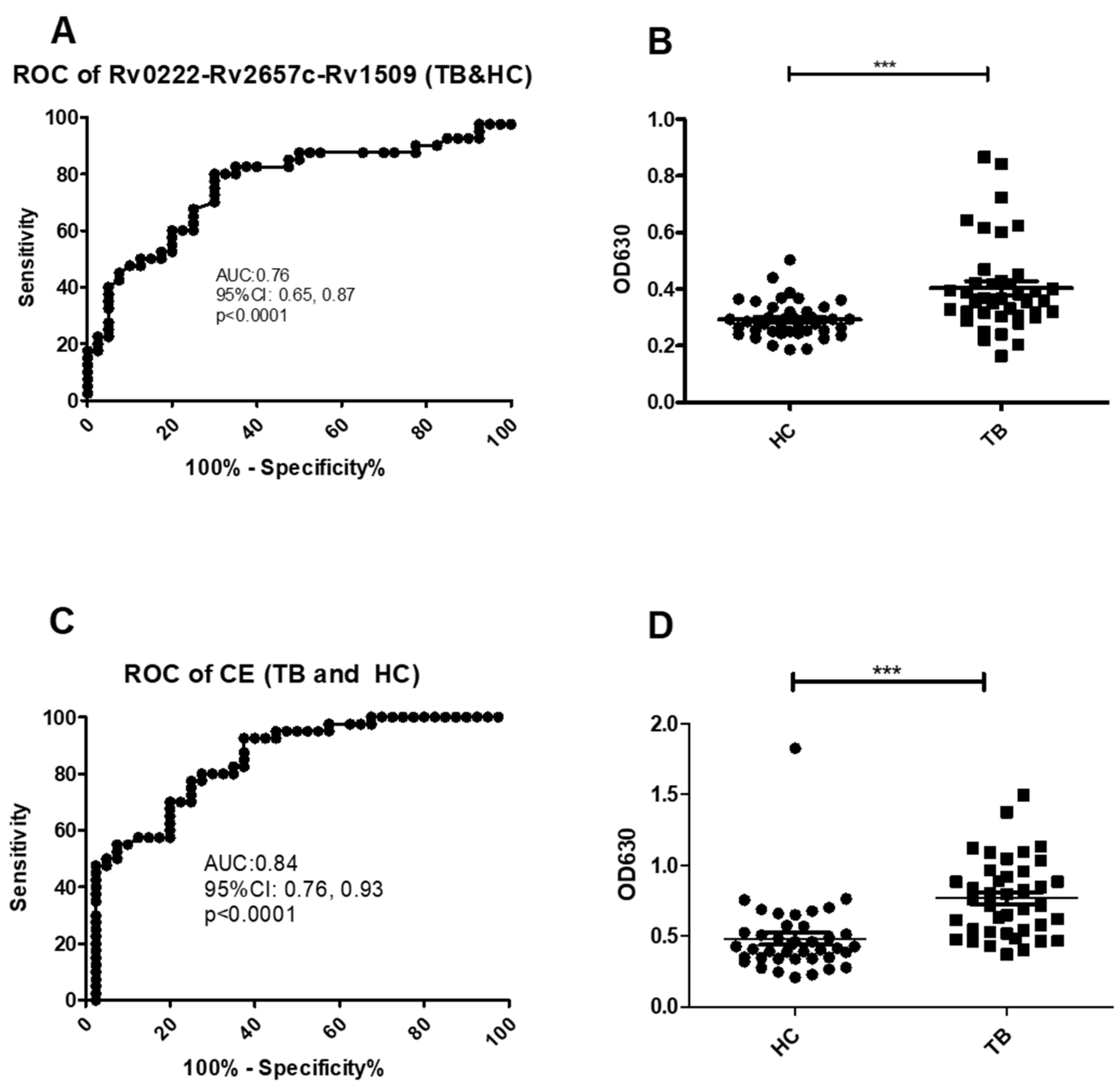
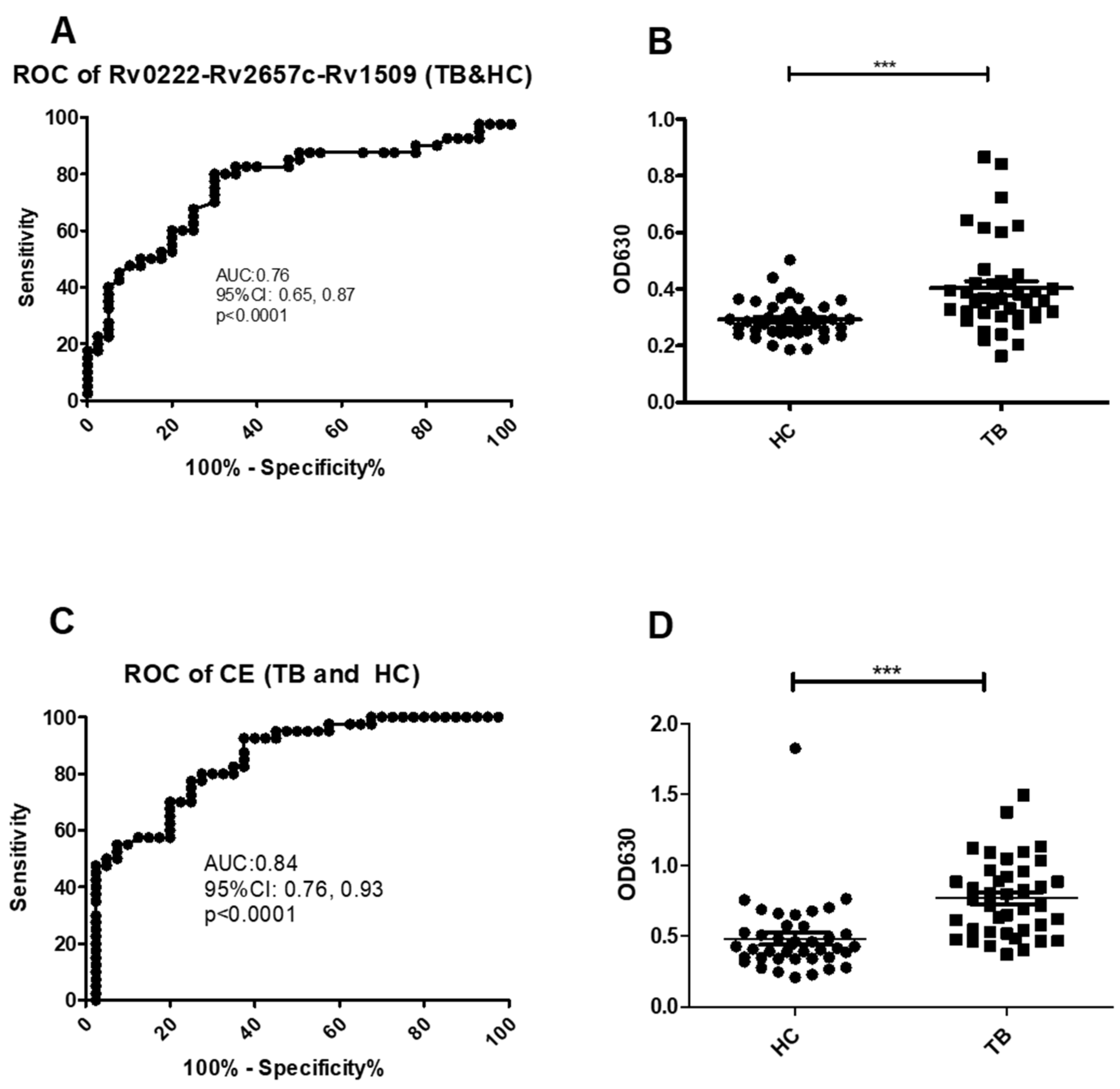
2.2. Rv0222-Rv2657c-Rv1509-iELISA for TB Diagnosis
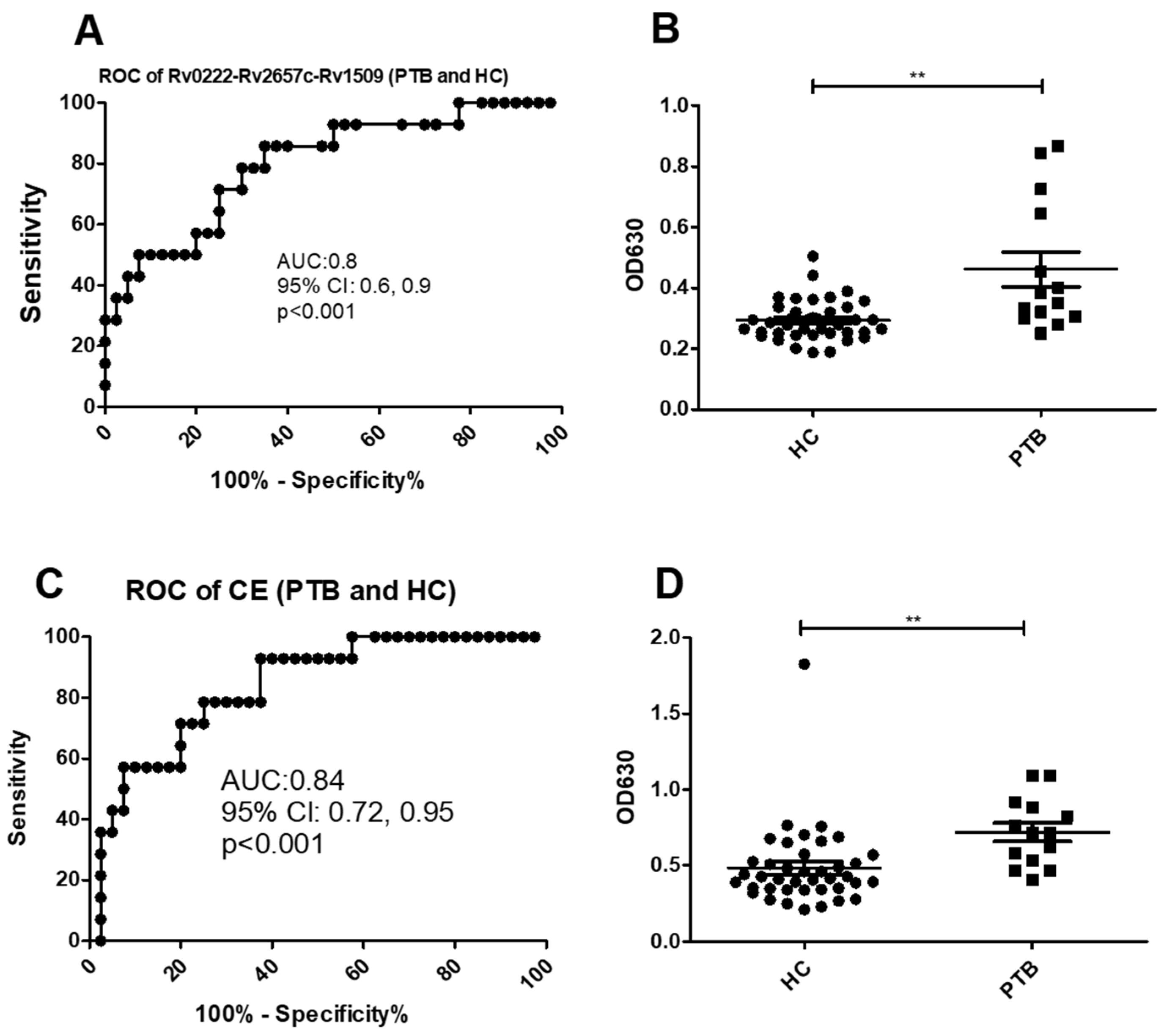
2.3. Use of the Rv0222-Rv2657c-Rv1509-iELISA to Diagnose PTB
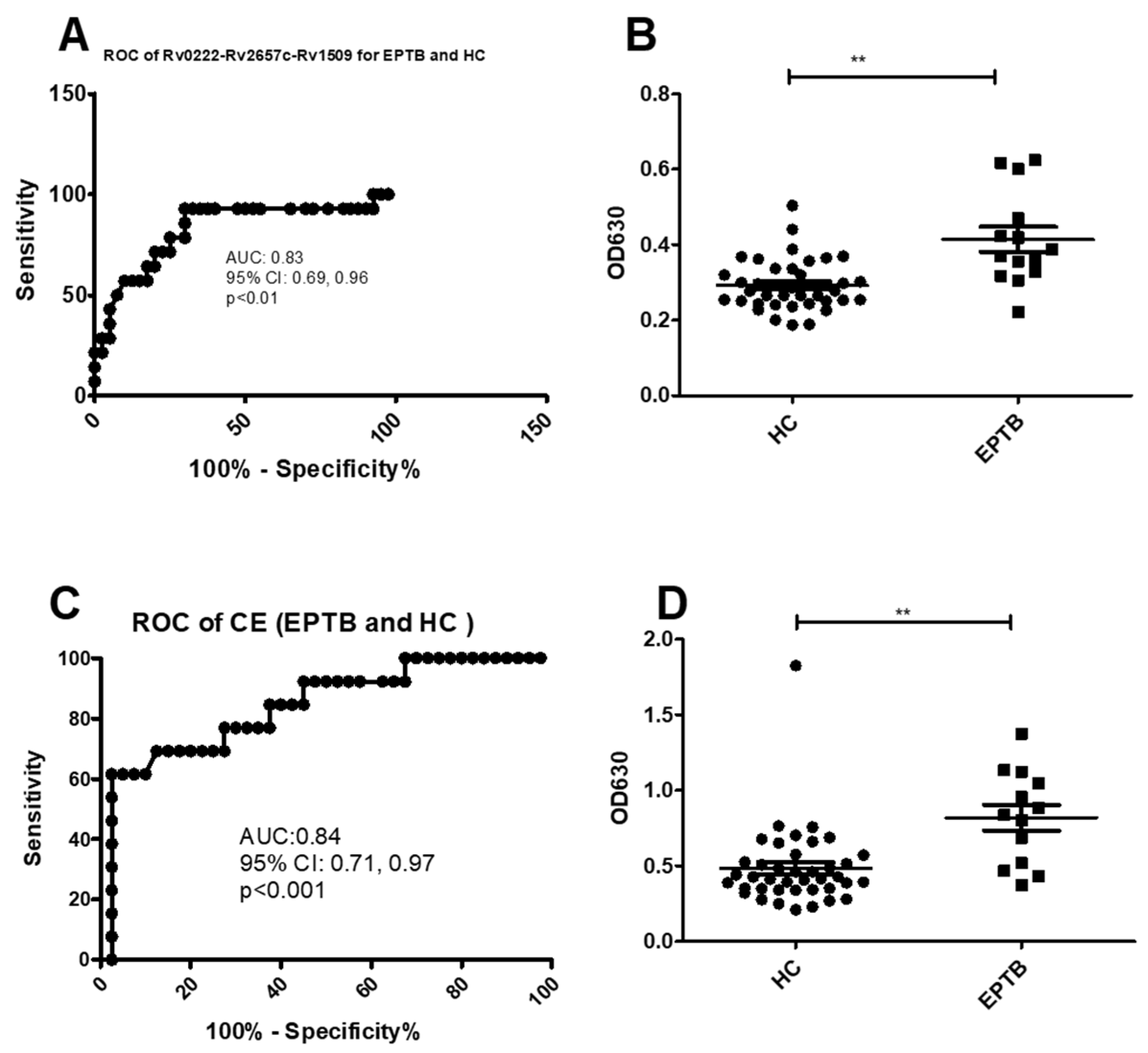
2.4. Use of the Rv0222-Rv2657c-Rv1509-iELISA to Diagnose EPTB
3. Discussion
4. Materials and Methods
4.1. Ethics Statement
4.2. Serum Samples and Patients
4.3. Cloning, Expression and Purification of Target Proteins
4.4. Indirect ELISA (iELISA)
4.5. Statistical Analyses
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global Tuberculosis Report 2019. Available online: https://www.who.int/teams/global-tuberculosis-programme/tb-reports (accessed on 12 February 2021).
- Purohit, M.; Mustafa, T. Laboratory Diagnosis of Extra-pulmonary Tuberculosis (EPTB) in Resource-constrained Setting: State of the Art, Challenges and the Need. J. Clin. Diagn. Res. 2015, 9, EE01–EE06. [Google Scholar] [CrossRef]
- Zhao, J.; Zhu, Z.; Zhang, X.; Suzuki, Y.; Chagan-Yasutan, H.; Chen, H.; Wan, Y.; Xu, J.; Ashino, Y.; Hattori, T. Evaluation of Anti-TBGL Antibody in the Diagnosis of Tuberculosis Patients in China. J. Immunol. Res. 2015, 2015, 834749. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.Y. Diagnosis and Treatment of Extrapulmonary Tuberculosis. Tuberc. Respir. Dis. 2015, 78, 47–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. XpertMTB/RIF:WHO Policy Update and Implementation Manual. Available online: http://appswhoint/iris/bitstream/handle/10665/112469/9789241506700_engpdf (accessed on 12 February 2021).
- Wang, S.; Wu, J.; Chen, J.; Gao, Y.; Zhang, S.; Zhou, Z.; Huang, H.; Shao, L.; Jin, J.; Zhang, Y.; et al. Evaluation of Mycobacterium tuberculosis -specific antibody responses for the discrimination of active and latent tuberculosis infection. Int. J. Infect. Dis. 2018, 70, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broger, T.; Roy, R.B.; Filomena, A.; Greef, C.H.; Rimmele, S.; Havumaki, J.; Danks, D.; Schneiderhan-Marra, N.; Gray, C.M.; Singh, M.; et al. Diagnostic Performance of Tuberculosis-Specific IgG Antibody Profiles in Patients with Presumptive Tuberculosis from Two Continents. Clin. Infect. Dis. 2017, 64, 947–955. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Cao, S.; Liu, Y.; Zhang, X.; Wang, W.; Li, C. Potential role for Rv2026c- and Rv2421c-specific antibody responses in diagnosing active tuberculosis. Clin. Chim. Acta 2018, 487, 369–376. [Google Scholar] [CrossRef]
- Tasbiti, A.H.; Bahrmand, A.; Shokrgozar, M.A.; Ghanaie, M.; Fateh, A.; Karimi, A.; Yari, S. Evaluation of Antigen Detection Test (Chromatographic Immunoassay): Potential to Replace the Antibody Assay Using Purified 45-kDa Protein for Rapid Diagnosis of Tuberculosis. J. Clin. Lab. Anal. 2013, 28, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Rodríguez, C.; Estrada-Chávez, C.; García-Vigil, J.; Laredo-Sánchez, F.; Halabe-Cherem, J.; Pereira-Suárez, A.; Mancilla, R. An IgG antibody response to the antigen 85 complex is associated with good outcome in Mexican Totonaca Indians with pulmonary tuberculosis. Int. J. Tuberc. Lung Dis. 2002, 6, 706–712. [Google Scholar]
- Tan, S.; Lin, N.; Huang, M.; Wang, Q.; Tan, Y.; Li, B.; Zhang, N.; Guo, T.; Cui, Y.; Chen, X.; et al. CTL immunogenicity of Rv3615c antigen and diagnostic performances of an ESAT-6/CFP-10/Rv3615c antigen cocktail for Mycobacterium tuberculosis infection. Tuberculosis 2017, 107, 5–12. [Google Scholar] [CrossRef]
- Majumdar, A.; Kamble, P.D.; Harinath, B.C. Detection of circulating free and immune-complexed antigen in pulmonary tuberculosis using cocktail of antibodies to mycobacterium tuberculosis excretory secretory antigens by peroxidase enzyme immunoassay. Indian J. Tuberc. 2010, 57, 67–74. [Google Scholar]
- Harinath, B.C.; Kumar, S.; Roy, S.S.; Hirudkar, S.; Upadhye, V.; Shende, N. A cocktail of affinity-purified antibodies reactive with diagnostically useful mycobacterial antigens ES-31, ES-43, and EST-6 for detecting the presence of Mycobacterium tuberculosis. Diagn. Microbiol. Infect. Dis. 2006, 55, 65–68. [Google Scholar] [CrossRef]
- Wang, F.; Yu, J.; Zhou, Y.; Luo, Y.; Wu, S.; Huang, M.; Yin, B.; Huang, J.; Mao, L.; Sun, Z. The Use of TB-Specific Antigen/Phytohemagglutinin Ratio for Diagnosis and Treatment Monitoring of Extrapulmonary Tuberculosis. Front. Immunol. 2018, 9, 1047. [Google Scholar] [CrossRef] [PubMed]
- Huo, Z.-Y.; Peng, L. Accuracy of the interferon-γ release assay for the diagnosis of active tuberculosis among HIV-seropositive individuals: A systematic review and meta-analysis. BMC Infect. Dis. 2016, 16, 350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gómez, A.V.; González-Martín, J.; García-Basteiro, A.L. Xpert® MTB/RIF: Utilidad en el diagnóstico de la tuberculosis y de la resistencia a la rifampicina. Med. Clín. 2017, 149, 399–405. [Google Scholar] [CrossRef] [Green Version]
- Wu, X.; Tan, G.; Gao, R.; Yao, L.; Bi, D.; Guo, Y.; Yu, F.; Fan, L. Assessment of the Xpert MTB/RIF Ultra assay on rapid diagnosis of extrapulmonary tuberculosis. Int. J. Infect. Dis. 2019, 81, 91–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, Y.; Li, R.; Shen, J.; He, L.; Li, Y.; Zhang, N.; Wu, Q.; Zhang, J.; Zheng, J.; Wang, X. Clinical effect of T-SPOT.TB test for the diagnosis of tuberculosis. BMC Infect. Dis. 2019, 19, 993–998. [Google Scholar] [CrossRef] [PubMed]
- Pottumarthy, S.; Wells, V.C.; Morris, A.J. A comparison of seven tests for serological diagnosis of tuberculosis. J. Clin. Microbiol. 2000, 8, 2227–2231. [Google Scholar] [CrossRef] [PubMed]
- Cole, S.T. Learning from the genome sequence ofMycobacterium tuberculosisH37Rv. FEBS Lett. 1999, 452, 7–10. [Google Scholar] [CrossRef] [Green Version]
- Ren, N.; Jinli, J.; Chen, Y.; Zhou, X.; Wang, J.; Ge, P.; Khan, F.A.; Zhang, L.; Hu, C.; Robertson, I.D.; et al. Identification of new diagnostic biomarkers forMycobacterium tuberculosisand the potential application in the serodiagnosis of human tuberculosis. Microb. Biotechnol. 2018, 11, 893–904. [Google Scholar] [CrossRef]
- Wu, X.; Yang, Y.; Zhang, J.; Li, B.; Liang, Y.; Zhang, C.; Dong, M. Comparison of antibody responses to seventeen antigens from Mycobacterium tuberculosis. Clin. Chim. Acta 2010, 411, 1520–1528. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.-N.; Chen, J.-P.; Chen, D.-L. Serodiagnosis Efficacy and Immunogenicity of the Fusion Protein of Mycobacterium tuberculosis Composed of the 10-Kilodalton Culture Filtrate Protein, ESAT-6, and the Extracellular Domain Fragment of PPE68. Clin. Vaccine Immunol. 2012, 19, 536–544. [Google Scholar] [CrossRef] [PubMed]
- Khurshid, S.; Afzal, M.; Khalid, R.; Khan, I.H.; Akhtar, M.W. Improving sensitivity for serodiagnosis of tuberculosis using TB16.3-echA1 fusion protein. Tuberculosis 2014, 94, 519–524. [Google Scholar] [CrossRef] [PubMed]
- Bryksin, A.; Matsumura, I. Overlap Extension PCR Cloning. Methods Mol. Biol. 2013, 1073, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.-L.; Zhou, Y.-X.; Wu, S.-M.; Pan, Q.; Xia, B.; Zhang, X.-L. CFP10 and ESAT6 aptamers as effective Mycobacterial antigen diagnostic reagents. J. Infect. 2014, 69, 569–580. [Google Scholar] [CrossRef] [PubMed]
- Yuan, K.; Liang, D.; Wu, X.-Q.; Yao, Z.-S.; Jin, D.-X.; Yang, Z.-D.; Zhang, S.-C.; Ding, J.-Y.; Jiang, X.-B.; Chen, J.-T. Diagnostic value of enzyme-linked immunospot assay using CFP10/ESAT6 fusion protein as antigen in spinal tuberculosis. Zhongguo Yi Xue Ke Xue Yuan Xue Bao 2015, 37, 44–49. [Google Scholar] [PubMed]
- Ross, T.D. Accurate confidence intervals for binomial proportion and Poisson rate estimation. Comput. Biol. Med. 2003, 33, 509–531. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antigen | Compared Group * | Sensitivity (%) (95%) | Specificity (%) (95%) |
|---|---|---|---|
| Rv0222-Rv2657c-Rv1509 | TB & HC | 80 (32/40) | 70 (28/40) |
| (64.4, 90.9) | (53.5, 83.4) | ||
| PTB & HC | 85.7 (12/14) | 70 (28/40) | |
| (57.2, 98.2) | (53.5, 83.4) | ||
| EPTB & HC | 92.8 (13/14) | 70 (28/40) | |
| (66.1, 99.8) | (53.5, 83.4) | ||
| CE | TB & HC | 77.5 (31/40) | 72.5 (29/40) |
| (61.5, 89.2) | (56.1, 85.4) | ||
| PTB & HC | 71.4 (10/14) | 80 (32/40) | |
| (41.9, 91.6) | (64.4, 90.9) | ||
| EPTB & HC | 71.4 (10/14) | 67.5 (27/40) | |
| (41.9, 91.6) | (50.9, 81.4) |
| NO. | Gender | Age | TB Form |
|---|---|---|---|
| 1 | male | 66 | PTB |
| 2 | male | 23 | PTB |
| 3 | male | 60 | PTB |
| 4 | female | 44 | PTB |
| 5 | male | 23 | PTB |
| 6 | female | 45 | PTB |
| 7 | male | 64 | PTB |
| 8 | male | 72 | PTB |
| 9 | male | 77 | PTB |
| 10 | male | 51 | PTB |
| 11 | male | 23 | PTB |
| 12 | male | 68 | PTB |
| 13 | female | 25 | PTB |
| 14 | male | 58 | PTB |
| 15 | Unknown | 31 | Unknown |
| 16 | Unknown | 59 | Unknown |
| 17 | Unknown | 31 | Unknown |
| 18 | Unknown | 37 | Unknown |
| 19 | Unknown | Unknown | Unknown |
| 20 | Unknown | Unknown | Unknown |
| 21 | Unknown | Unknown | Unknown |
| 22 | Unknown | Unknown | Unknown |
| 23 | Unknown | Unknown | Unknown |
| 24 | male | 18 | EPTB |
| 25 | female | 20 | EPTB |
| 26 | female | 78 | EPTB |
| 27 | male | 41 | EPTB |
| 28 | female | 35 | EPTB |
| 29 | male | 69 | EPTB |
| 30 | female | Unknown | EPTB |
| 31 | female | 69 | EPTB |
| 32 | female | 26 | EPTB |
| 33 | male | 53 | EPTB |
| 34 | female | 25 | EPTB |
| 35 | male | 43 | EPTB |
| 36 | male | 34 | EPTB |
| 37 | female | 23 | EPTB |
| 38 | Unknown | Unknown | Unknown |
| 39 | Unknown | Unknown | Unknown |
| 40 | Unknown | Unknown | Unknown |
| Gene | Restriction Endonuclease | Primers |
|---|---|---|
| Rv0222 | BamHI | 5′-ATA GGATCC ATGAGCAGCGAAAGCGACG-3′ 3′-AGATCCGCCTCCACCTGAACCGCCACCTCCCGCGTAGCCTTCCACCGCAGCA-5′ |
| Rv2657c | 5′-GGAGGTGGCGGTTCAGGTGGAGGCGGATCTAGTCTCGGGTGGACGGTC-3′ 3′AGATCCGCCTCCACCTGAACCGCCACCTCCCTCACTGATCGTGATGTACC-5′ | |
| Rv1509 | HindⅢ | 5′GGAGGTGGCGGTTCAGGTGGAGGCGGATCTACGGGTGAAGGTTTTGGCAA-3′ 3′GC AAGCTT CGAACGCCAGACTCCCTT-5′ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.; Ge, P.; Zhang, K.; Xiang, J.; Zhang, L.; Robertson, I.D.; Guo, A. Use of Rv0222-Rv2657c-Rv1509 Fusion Protein to Improve the Accuracy of an Antibody ELISA for Extra-Pulmonary Tuberculosis in Humans. Pathogens 2021, 10, 828. https://doi.org/10.3390/pathogens10070828
Chen Y, Ge P, Zhang K, Xiang J, Zhang L, Robertson ID, Guo A. Use of Rv0222-Rv2657c-Rv1509 Fusion Protein to Improve the Accuracy of an Antibody ELISA for Extra-Pulmonary Tuberculosis in Humans. Pathogens. 2021; 10(7):828. https://doi.org/10.3390/pathogens10070828
Chicago/Turabian StyleChen, Yingyu, Pan Ge, Kailun Zhang, Jie Xiang, Li Zhang, Ian D. Robertson, and Aizhen Guo. 2021. "Use of Rv0222-Rv2657c-Rv1509 Fusion Protein to Improve the Accuracy of an Antibody ELISA for Extra-Pulmonary Tuberculosis in Humans" Pathogens 10, no. 7: 828. https://doi.org/10.3390/pathogens10070828
APA StyleChen, Y., Ge, P., Zhang, K., Xiang, J., Zhang, L., Robertson, I. D., & Guo, A. (2021). Use of Rv0222-Rv2657c-Rv1509 Fusion Protein to Improve the Accuracy of an Antibody ELISA for Extra-Pulmonary Tuberculosis in Humans. Pathogens, 10(7), 828. https://doi.org/10.3390/pathogens10070828